ABOS Part I Orthopaedic Spine Review: Spondylolisthesis, Disc Herniation & Cauda Equina Syndrome | Part 22305
Key Takeaway
This ABOS Part I comprehensive review module offers 20 advanced orthopedic MCQs mirroring ABOS Part I and AAOS OITE exams. It covers spondylolisthesis classifications, diagnosis, and management, including surgical indications and complications. Also discussed are disc prolapse types, nerve root anatomy, and urgent management of Cauda Equina Syndrome.
ABOS Part I Orthopaedic Spine Review: Spondylolisthesis, Disc Herniation & Cauda Equina Syndrome | Part 22305
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 14-year-old competitive gymnast presents with insidious onset low back pain exacerbated by extension and hyperextension activities. Physical examination reveals hamstring tightness and a palpable step-off at L5. AP and lateral radiographs of the lumbar spine show a defect in the pars interarticularis at L5 with an anterior translation of L5 on S1. Which of the following is the most appropriate classification for this condition?
Explanation
Correct Answer: B
The patient's age, activity (gymnast), pars defect, and anterior translation are classic for an isthmic spondylolisthesis. Wiltse-Newman classification Type II isthmic is characterized by a lesion in the pars interarticularis. Given the insidious onset and high-impact repetitive extension activities, it's most likely a stress fracture (lytic) rather than an acute traumatic fracture (Type IV) or congenital dysplastic anomaly (Type I). Degenerative (Type III) is typically seen in older adults, and pathologic (Type V) is due to bone disease.
Question 2
Which of the following Meyerding grades of spondylolisthesis indicates a slip of 50-75% of the vertebral body's width?
Explanation
Correct Answer: C
The Meyerding classification system grades spondylolisthesis based on the percentage of anterior displacement of the superior vertebral body over the inferior one. Grade I is 0-25%, Grade II is 25-50%, Grade III is 50-75%, Grade IV is 75-100%, and Grade V (spondyloptosis) is complete displacement (>100%). Therefore, 50-75% displacement corresponds to Grade III.
Question 3
A 55-year-old female presents with a long history of low back pain and bilateral leg pain, worse with standing and walking, relieved by sitting or leaning forward. Radiographs show L4-L5 degenerative spondylolisthesis (Grade I) with associated spinal stenosis. She has failed 6 months of comprehensive conservative management including physical therapy, NSAIDs, and epidural steroid injections. Neurological exam reveals mild quadriceps weakness (4+/5) bilaterally but no frank motor deficit. What is the most appropriate next step in management?
Explanation
Correct Answer: C
For symptomatic degenerative spondylolisthesis with spinal stenosis that has failed conservative management, surgical intervention is often indicated. The Spine Patient Outcomes Research Trial (SPORT) demonstrated superior outcomes for surgical treatment compared to non-operative care in patients with degenerative spondylolisthesis and stenosis. While decompression alone can address stenosis, studies like SPORT have shown that adding fusion to decompression significantly improves outcomes and reduces reoperation rates for degenerative spondylolisthesis, especially in the presence of instability or significant back pain. Quadriceps weakness suggests L4 nerve root compression, making decompression necessary. Anterior fusion alone does not address the posterior decompression requirement. TLIF typically includes decompression. The best option combining decompression and stabilization is decompression with instrumented posterolateral fusion.
Question 4
Which type of spondylolisthesis is most commonly associated with a sacral spina bifida occulta and a trapezoidal L5 vertebral body?
Explanation
Correct Answer: A
Type I, or Dysplastic Spondylolisthesis, is a congenital anomaly characterized by malformed sacral facets, an elongated pars, and a trapezoidal L5 vertebral body, often associated with sacral spina bifida occulta. This morphology leads to an inherent instability that predisposes to anterior slippage. The other types have different underlying etiologies.
Question 5
A 30-year-old male with chronic L5-S1 isthmic spondylolisthesis (Grade II) complains of persistent low back pain and bilateral S1 radiculopathy despite 9 months of conservative treatment. On examination, he has bilateral hamstring tightness and a positive straight leg raise test at 45 degrees. Which of the following imaging modalities is most crucial for evaluating potential nerve root compression and planning surgical decompression?
Explanation
Correct Answer: C
While plain radiographs define the slip, and CT can better visualize bony stenosis, MRI is superior for evaluating soft tissue structures, including nerve roots, discs, and the spinal cord, and identifying nerve root compression by hypertrophic soft tissue, disc herniation, or foraminal stenosis, which is critical for surgical planning in patients with radiculopathy. EMG assesses nerve function but isn't an imaging modality for structural compression.
Question 6
What is the primary role of an oblique radiograph in the workup of spondylolisthesis?
Explanation
Correct Answer: B
Oblique radiographs are specifically used to visualize the pars interarticularis, which appears as the 'neck' of the 'Scottie dog.' A defect or fracture in the pars ('collar on the Scottie dog') is indicative of an isthmic spondylolysis or spondylolisthesis. Other views (AP/Lateral) are better for alignment, slip percentage, and disc space evaluation.
Question 7
In a pediatric patient with spondylolysis (pars defect without slip) who is asymptomatic, what is the recommended management?
Explanation
Correct Answer: C
For asymptomatic spondylolysis without slip, the primary recommendation is observation with activity as tolerated. Most pars defects remain stable and asymptomatic. Surgical intervention is reserved for symptomatic, failed conservative cases. Bracing or activity restriction might be considered for symptomatic spondylolysis to promote healing, but not for asymptomatic lesions. Physical therapy is more relevant for symptomatic individuals.
Question 8
A 68-year-old male with a history of hypertension and diabetes presents with progressively worsening low back pain and L4-L5 neurogenic claudication. He has a Grade I degenerative spondylolisthesis at L4-L5. His pain is 7/10 on the VAS. He has tried epidural steroid injections, NSAIDs, and physical therapy for 9 months with no sustained relief. What is the strongest indicator for surgical intervention in this patient?
Explanation
Correct Answer: C
The strongest indicator for surgical intervention in symptomatic degenerative spondylolisthesis is the failure of a prolonged course of conservative management combined with persistent severe symptoms (pain, neurological deficits) impacting quality of life. While neurogenic claudication itself is a symptom, its persistence despite non-operative efforts is the key factor. The grade of slip alone isn't an indication for surgery, nor are comorbidities unless they contraindicate surgery. Age is a factor for surgical risk but not an indication for surgery.
Question 9
What is the most common neurological complication following reduction of a high-grade spondylolisthesis?
Explanation
Correct Answer: B
The L5 nerve root is most vulnerable during the reduction of a high-grade L5-S1 spondylolisthesis. This is due to its course over the sacral ala and the potential for stretch injury during the reduction maneuver, especially with attempts to correct lumbosacral kyphosis. While other nerve injuries can occur, L5 radiculopathy/palsy is the most frequently reported neurological complication.
Question 10
Which of the following describes the anatomical defect in Type IIB isthmic spondylolisthesis?
Explanation
Correct Answer: A
Wiltse-Newman Type II isthmic spondylolisthesis is subdivided: Type IIA is a lytic (stress) fracture of the pars, Type IIB is an elongated but intact pars (often a healed stress fracture with elongation), and Type IIC is an acute fracture of the pars. Therefore, Type IIB specifically refers to an elongated pars without a clear lytic defect.
Question 11
A 37-year-old male presents with back and left lower limb pain, suspected 'slipped disc'. During the initial evaluation, which of the following findings would be the MOST concerning red flag, necessitating immediate further investigation for a serious spinal pathology?
Explanation
Correct Answer: D
The case explicitly lists 'Urinary retention', 'Faecal incontinence', 'Saddle area numbness and loss of anal tone', and 'Widespread neurological signs' as characteristics of Cauda Equina Syndrome (CES). The importance of detecting CES early is highlighted, with early intervention (< 24 hours) shown to improve outcome. Acute onset of urinary retention and saddle anesthesia are hallmark symptoms of CES, representing a surgical emergency requiring immediate investigation and intervention. Options A, B, C, and E are typical signs and symptoms of radiculopathy, which, while requiring appropriate management, do not represent the same level of immediate neurological emergency as CES.
Question 12
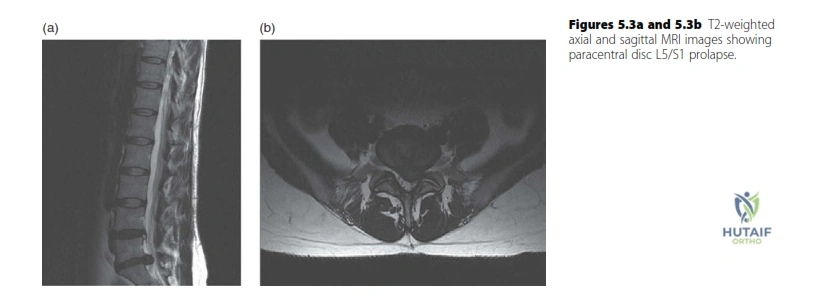
A 37-year-old male presents with left lower limb radiculopathy. An MRI is performed. Review the provided T2-weighted MRI scan of the lumbar spine.
Based on the image and the case description, what is the most likely diagnosis and affected nerve root?
Explanation
Correct Answer: C
The case explicitly states that the MRI shows 'a paracentral disc prolapse at the L5/S1 level'. The background knowledge section on 'Exiting nerve roots in the cervical and lumbar spine' further clarifies that for a common 'paracentral' disc prolapse at the L5/S1 level, it is the S1 'traversing' nerve root that is most commonly compressed. Therefore, an L5/S1 paracentral disc prolapse affecting the S1 nerve root is the most accurate diagnosis based on the provided information.
Question 13
A 37-year-old male is diagnosed with a left L5/S1 paracentral disc prolapse. Based on the expected S1 nerve root compression, which combination of physical exam findings is most consistent with this diagnosis?

Explanation
Correct Answer: C
The candidate's expected findings for an L5/S1 disc prolapse are explicitly stated: 'I would expect the pain, paraesthesia and numbness to be in an S1 distribution (posterior calf, heel and lateral border of the foot) on the left. There may be an associated subjective decreased sensation in the same distribution, a decreased ankle jerk on that side...' The S1 nerve root primarily innervates the muscles responsible for ankle plantarflexion and mediates the Achilles reflex (ankle jerk). Sensory distribution for S1 includes the posterior calf, heel, and lateral border of the foot. Therefore, weakness in ankle plantarflexion, numbness over the lateral foot/heel, and a diminished Achilles reflex are the classic findings for S1 radiculopathy.
Question 14
A 45-year-old patient presents with acute low back pain and bilateral leg weakness. To definitively diagnose Cauda Equina Syndrome, which of the following clinical findings is considered a hallmark symptom?
Explanation
Correct Answer: D
The case explicitly lists 'Urinary retention' and 'Faecal incontinence' as key characteristics of Cauda Equina Syndrome. These symptoms, along with saddle area numbness and loss of anal tone, are considered hallmark signs of CES, indicating significant compression of the sacral nerve roots. While options A, B, C, and E can be present in various spinal pathologies, including severe radiculopathy, new onset urinary retention or overflow incontinence is a critical red flag that mandates immediate investigation for CES.
Question 15
A 50-year-old patient presents with a 12-hour history of saddle anesthesia, new-onset urinary retention, and progressive bilateral lower extremity weakness. An MRI confirms a large acute disc prolapse causing Cauda Equina Syndrome. What is the most appropriate immediate management strategy?
Explanation
Correct Answer: C
The case emphasizes the critical importance of timely intervention for Cauda Equina Syndrome, stating: 'The importance of detecting cauda equina syndrome early is that early intervention (< 24 hours) has been shown to improve outcome.' Given the acute onset of hallmark CES symptoms (saddle anesthesia, urinary retention, bilateral weakness) and MRI confirmation, urgent surgical decompression is indicated to prevent permanent neurological deficits. Options A, B, D, and E represent conservative or delayed management strategies that are inappropriate and potentially harmful in the setting of acute CES.
Question 16
A 62-year-old patient presents with symptoms consistent with an L4/L5 paracentral disc prolapse. Based on the typical anatomical relationships described in the case, which nerve root is most commonly affected by this type of disc herniation?
Explanation
Correct Answer: C
The 'Exiting nerve roots in the cervical and lumbar spine' section explicitly clarifies the anatomical relationship: 'The knowledge that the L4 nerve root exits the spinal canal below the L4 pedicle may (incorrectly) lead the candidate to expect the L4 nerve root to be compressed when a disc prolapse occurs below the L4 vertebra in the L4/5 interspace. It is best to think of this nerve root as ‘already having left the canal’ and therefore it is the L5 ‘traversing’ nerve root that is most commonly compressed by the common ‘paracentral’ disc prolapse. ... Thus an L4/5 disc prolapse commonly affects the L5 nerve root.'
Question 17
A 48-year-old patient presents with right arm pain and weakness. MRI reveals a disc prolapse at the C5/C6 level. According to the anatomical principles outlined in the case, which nerve root is most likely compressed?
Explanation
Correct Answer: C
The 'Exiting nerve roots in the cervical and lumbar spine' section details the unique nomenclature in the cervical spine: 'In the cervical spine, a prolapsed disc typically affects the exiting nerve root at that level (there is no traversing nerve root because the roots leave the spinal cord and exit the canal almost horizontally). But there is a nomenclature change in the cervical spine. Because the C6 nerve root exits above (not below) the C6 vertebra this double change means a prolapsed cervical disc at the C5/C6 level most commonly affects the C6 nerve root.'
Question 18
A patient's MRI report describes a disc herniation where the displaced disc material has a narrow 'neck' at its base but remains in continuity with the parent disc. According to the nomenclature provided, how would this specific type of disc herniation be classified?
Explanation
Correct Answer: C
The 'Nomenclature' section defines different types of disc herniation. It states: 'A focal disc herniation may be described as a protrusion or extrusion. An extruded disc has a narrow ‘neck’ at its base. Extruded disc material is sequestrated if it is no longer in continuity with the disc.' The description in the question, 'displaced disc material has a narrow 'neck' at its base but remains in continuity with the parent disc,' perfectly matches the definition of an extrusion.
Question 19
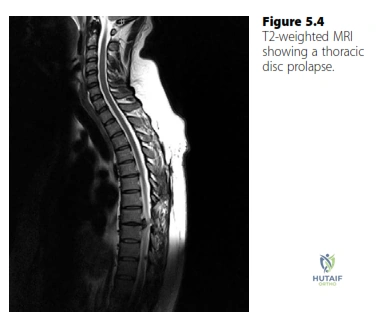
A 55-year-old patient presents with progressive upper extremity weakness, gait disturbance, and thoracic back pain. MRI reveals a calcified thoracic disc prolapse at T8/T9 causing spinal cord compression. Based on the case information, what is the recommended surgical approach for this condition?
Explanation
Correct Answer: C
The 'Disc prolapse background knowledge' section specifically addresses thoracic disc prolapse: 'A thoracic disc prolapse (rare) will typically present with symptoms and signs of spinal cord compression associated with thoracic back pain... The discs are usually calcified and require decompression from the front. Treatment therefore is via a thoracotomy and partial vertebrectomy.' This indicates that an anterior approach via thoracotomy and partial vertebrectomy is the standard surgical treatment for thoracic disc prolapse causing spinal cord compression.
Question 20
A 37-year-old male with a left L5/S1 paracentral disc prolapse causing S1 radiculopathy has been managed conservatively for 8 weeks with physical therapy and NSAIDs. His symptoms have shown minimal improvement, and he continues to experience significant pain and functional limitation. What is the most appropriate next step in his management?
Explanation
Correct Answer: B
The candidate's proposed treatment plan for a lumbar disc prolapse states: 'Initially conservatively as the natural history of most lumbar disc prolapses is that they resolve with time. If it has not resolved after 6–12 weeks of conservative management I would offer the patient microdiscectomy.' Given that the patient has undergone 8 weeks of conservative management with minimal improvement, he falls within the 6-12 week window where surgical intervention (microdiscectomy) would be offered. While epidural steroid injections (Option E) are a common non-surgical intervention, the case specifically outlines microdiscectomy as the next step after 6-12 weeks of failed conservative management. Continuing conservative management for another 6 months (Option A) would be excessively prolonged given the persistent symptoms. Options C and D are not the primary next steps in this scenario.
Question 21
A 45-year-old male presents with acute back pain, bilateral leg radiculopathy, and urinary difficulties. Post-void residual (PVR) volume is measured via ultrasound. What PVR value is generally accepted as the threshold with the highest specificity to prompt urgent MRI for suspected cauda equina syndrome?
Explanation
Question 22
A 50-year-old male presents with acute onset right anterior thigh pain and weakness in knee extension. An MRI of the lumbar spine reveals a far lateral disc herniation at L4-L5. Which nerve root is most likely compressed?
Explanation
Question 23
A 62-year-old female presents with neurogenic claudication. Radiographs demonstrate an L4-L5 Grade I degenerative spondylolisthesis. Which of the following anatomic characteristics is most strongly associated with the development of this condition?
Explanation
Question 24
An 11-year-old girl is diagnosed with a high-grade dysplastic spondylolisthesis at L5-S1. Which of the following radiographic parameters is the most reliable predictor for further slip progression?
Explanation
Question 25
A 35-year-old male is referred after a lumbar MRI, obtained for an isolated and self-limiting episode of back pain 3 months ago, revealed a large right-sided L5-S1 paracentral disc herniation. The patient is currently completely asymptomatic with normal strength, sensation, and reflexes. What is the most appropriate next step in management?
Explanation
Question 26
A 16-year-old male presents with severe lower back pain and an L5-S1 Grade IV isthmic spondylolisthesis. During a surgical reduction and fusion, which neurologic structure is at the highest risk of stretch injury?
Explanation
Question 27
A 48-year-old male presents with new-onset saddle anesthesia, bilateral lower extremity weakness, and urinary incontinence that began 12 hours ago. He is diagnosed with cauda equina syndrome. For the highest likelihood of significant bladder function recovery, decompression should ideally be performed within what timeframe from symptom onset?
Explanation
Question 28
A 35-year-old female presents with saddle anesthesia, bilateral leg weakness, and urinary incontinence. On examination, she exhibits hyperreflexia in the patellar and Achilles tendons, a positive Babinski sign bilaterally, and decreased anal sphincter tone. Which of the following is the most likely diagnosis?
Explanation
Question 29
A 42-year-old man presents with acute onset of bilateral lower extremity weakness, saddle anesthesia, and urinary retention following a heavy lifting injury. A post-void residual volume is >300 mL. MRI confirms a massive central L4-L5 disc extrusion compressing the cauda equina. Which of the following is the single most important prognostic factor for the return of his normal bowel and bladder function following emergent decompression?
Explanation
Question 30
A 16-year-old male with a high-grade L5-S1 isthmic spondylolisthesis is evaluated for surgical intervention. Radiographic assessment reveals a high pelvic incidence (PI). Which of the following accurately describes the relationship between pelvic incidence and high-grade spondylolisthesis?
Explanation
Question 31
A 45-year-old man presents with acute, severe left-sided anterior thigh pain and weakness in knee extension. Physical examination reveals a diminished left patellar reflex. MRI of the lumbar spine reveals a far lateral (extraforaminal) disc herniation at the L3-L4 level. Which nerve root is most likely compressed?
Explanation
Question 32
According to the Wiltse classification of spondylolisthesis, which of the following mechanisms correctly defines a Type IV (Traumatic) spondylolisthesis?
Explanation
Question 33
A 38-year-old woman presents with right lower extremity pain and weakness. Examination reveals weakness in right ankle dorsiflexion, great toe extension, and ankle inversion. Sensation is decreased over the dorsum of the foot. Which of the following pathologies is most likely responsible for her symptoms?
Explanation
Question 34
During the surgical reduction of a Grade V spondylolisthesis (spondyloptosis) at L5-S1 in a pediatric patient, neuromonitoring alerts the surgeon to impending nerve injury. Which of the following nerve roots is at the highest risk of iatrogenic stretch injury during this specific reduction maneuver?
Explanation
Question 35
A 55-year-old female presents with neurogenic claudication. Review the provided representative imaging.
In classical degenerative spondylolisthesis at this typical level, which of the following anatomic factors is most strongly predictive of progression?
Explanation
Question 36
A 10-year-old girl is diagnosed with a dysplastic (Wiltse Type I) spondylolisthesis at L5-S1. Compared to patients with an isthmic (Wiltse Type II) spondylolisthesis, this patient is at a significantly higher risk for which of the following complications?
Explanation
Question 37
A 40-year-old man presents with a massive, sequestrated lumbar disc herniation causing severe unilateral radiculopathy. He opts for conservative management. Over the next six months, his symptoms completely resolve, and a repeat MRI shows nearly complete resorption of the disc fragment. Which of the following mechanisms is primarily responsible for the spontaneous resorption of sequestrated disc fragments?
Explanation
Question 38
Which of the following proteoglycan and structural changes is most characteristic of intervertebral disc degeneration contributing to age-related herniation?
Explanation
Question 39
A 13-year-old male with a known Grade III L5-S1 isthmic spondylolisthesis presents with an altered gait. On examination, he walks with a characteristic waddling motion, maintaining his hips and knees in flexion with a flattened lumbar lordosis. This classic clinical presentation is referred to as:
Explanation
Question 40
A 65-year-old female undergoes a decompressive laminectomy for L4-L5 degenerative spondylolisthesis. During the procedure, an incidental durotomy occurs. The surgeon successfully achieves a primary, watertight suture repair. What is the most appropriate postoperative management regarding mobilization?
Explanation
Question 41
A 32-year-old male undergoes an L5-S1 microdiscectomy for a paracentral disc herniation. Six months later, he presents with recurrent, severe S1 radiculopathy. MRI confirms a recurrent disc herniation at the same level and side. Flexion-extension radiographs show no instability. After failing 12 weeks of conservative care, what is the most appropriate surgical intervention?
Explanation
Question 42
The SPORT (Spine Patient Outcomes Research Trial) evaluated operative versus nonoperative treatment for degenerative spondylolisthesis. Based on the long-term results of this trial, which of the following statements is true?
Explanation
Question 43
A 50-year-old diabetic patient presents with back pain and a high-grade fever. MRI reveals an epidural abscess with significant bony destruction at L3-L4 resulting in anterior translation of L3 on L4. According to the Wiltse classification, this type of spondylolisthesis is categorized as:
Explanation
Question 44
In evaluating a patient with suspected cauda equina syndrome, bladder ultrasound is performed. What minimum post-void residual (PVR) volume is generally considered highly sensitive and specific for the diagnosis of cauda equina syndrome in the setting of acute back pain and radiculopathy?
Explanation
Question 45
An 18-year-old gymnast complains of chronic low back pain exacerbated by extension. Radiographs show a Grade I isthmic spondylolisthesis at L5-S1. The slip angle is measured to assess the risk of progression. How is the slip angle (sagittal roll) correctly measured on a lateral radiograph?
Explanation
Question 46
A 60-year-old male undergoes a bilateral L4-L5 laminectomy and medial facetectomy for central stenosis. Postoperatively, he develops progressive mechanical back pain, and a repeat radiograph at 6 months reveals a new Grade II forward slip of L4 on L5. To minimize the risk of this iatrogenic (Wiltse Type VI) spondylolisthesis, resection of the pars interarticularis should not exceed what percentage?
Explanation
Question 47
Which specific parasympathetic nerve roots are primarily compressed in a central L4-L5 massive disc extrusion, leading to the loss of detrusor muscle tone and resultant urinary retention in Cauda Equina Syndrome?
Explanation
Question 48
A 45-year-old male presents with acute severe left leg pain. MRI demonstrates a far lateral (extraforaminal) disc herniation at the L3-L4 level. Which nerve root is most likely compressed by this specific herniation?
Explanation
Question 49
Which of the following best summarizes the findings of the Spine Patient Outcomes Research Trial (SPORT) regarding the treatment of degenerative spondylolisthesis?
Explanation
Question 50
A 38-year-old patient with a known massive L4-L5 central disc herniation presents to the emergency department. Which of the following clinical findings has the highest negative predictive value for Cauda Equina Syndrome?
Explanation
Question 51
A 22-year-old male presents with back pain and is diagnosed with an L5-S1 isthmic spondylolisthesis. Which spinopelvic parameter is typically abnormally increased in this population, predisposing them to elevated lumbosacral shear forces?
Explanation
Question 52
A 40-year-old man presents with acute L5 radiculopathy from a paracentral disc extrusion. He opts for conservative management and his symptoms resolve over 6 months. By what primary mechanism does the herniated disc material resorb?
Explanation
Question 53
When performing a Wiltse paraspinal muscle-splitting approach for a far lateral L4-L5 disc herniation, the deep dissection plane is developed between which two muscles?
Explanation
Question 54
Dysplastic (Type I) spondylolisthesis is characterized by congenital deficiency of the superior sacral facet or L5 inferior facet. Which of the following radiographic findings is most characteristic of high-grade dysplastic spondylolisthesis?
Explanation
Question 55
A 45-year-old male presents with acute severe back pain, bilateral sciatica, and new-onset urinary retention. Imaging confirms a massive L4-L5 central disc extrusion. What is the most appropriate next step in management?
Explanation
Question 56
A patient with an L4-L5 paracentral disc herniation will most likely exhibit weakness in which of the following movements during a physical examination?
Explanation
Question 57
A 35-year-old female underwent a successful L5-S1 microdiscectomy 6 months ago but now presents with recurrent, severe S1 radiculopathy. MRI with contrast confirms a recurrent disc herniation at the same level. What is the expected recurrence rate after a primary lumbar microdiscectomy?
Explanation
Question 58
Which of the following anatomic and biomechanical changes is most directly responsible for the development of degenerative (Wiltse Type III) spondylolisthesis?
Explanation
Question 59
A 50-year-old presents with progressive myelopathy and is found to have a large, calcified central disc herniation at T8-T9. Which of the following surgical approaches is universally CONTRAINDICATED?
Explanation
Question 60
A 10-year-old female gymnast is diagnosed with a Grade II L5-S1 isthmic spondylolisthesis. Which of the following is the most significant radiographic risk factor for further anterior progression of her slip?
Explanation
Question 61
A 19-year-old college football lineman presents with chronic mechanical low back pain. Radiographs show a Grade I L5-S1 isthmic spondylolisthesis. Which diagnostic test is most useful to confirm that the pars defect is the primary source of his pain prior to performing a direct pars repair?
Explanation
Question 62
A 45-year-old male presents with severe lower back pain, bilateral lower extremity weakness, and perineal numbness. A post-void residual (PVR) bladder volume is measured. Which of the following PVR volumes is most strongly indicative of cauda equina syndrome?
Explanation
Question 63
A 52-year-old male presents with acute severe left leg pain. Physical examination reveals weakness in left ankle dorsiflexion and great toe extension, but normal ankle plantarflexion. He has numbness over the dorsal web space between the first and second toes. Which of the following disc herniations is most likely responsible?
Explanation
Question 64
Which of the following anatomic factors has been most strongly correlated with the development of degenerative spondylolisthesis at the L4-L5 level?
Explanation
Question 65
A 16-year-old high school football lineman complains of chronic low back pain. Radiographs demonstrate an isthmic spondylolisthesis. Advanced imaging reveals an elongated, but intact, pars interarticularis without a frank fracture. According to the Wiltse classification, which subtype does this represent?
Explanation
Question 66
A 40-year-old male has an MRI demonstrating a lumbar disc herniation. He elects for nonoperative management. Based on the natural history of lumbar disc herniations, which morphologic type has the highest rate of spontaneous resorption?
Explanation
Question 67
A 35-year-old male presents with severe right leg pain radiating to the plantar aspect of his foot. On examination, he has an absent Achilles reflex and 4/5 strength in ankle plantarflexion. A paracentral disc herniation at which level is the most likely cause?
Explanation
Question 68
A 12-year-old female undergoes surgical reduction and instrumented fusion for a Meyerding Grade IV isthmic spondylolisthesis at L5-S1. Postoperatively, she exhibits new-onset weakness in foot dorsiflexion and great toe extension. Which nerve root is most commonly injured during the reduction maneuver for a high-grade slip?
Explanation
Question 69
In the evaluation of spinopelvic parameters for a patient with adult spinal deformity and spondylolisthesis, which of the following equations accurately defines Pelvic Incidence (PI)?
Explanation
Question 70
A patient with a massive central L4-L5 disc herniation develops acute urinary retention, fecal incontinence, and saddle anesthesia. Compression of which specific nerve roots is primarily responsible for the saddle anesthesia?
Explanation
Question 71
Based on the results of the Spine Patient Outcomes Research Trial (SPORT) regarding degenerative spondylolisthesis, which of the following statements is true regarding outcomes at the 4-year follow-up?
Explanation
Question 72
A 48-year-old female presents to the emergency department with acute onset of bilateral sciatica, severe perianal numbness, and loss of bowel control following a heavy lifting event. MRI confirms a massive central L5-S1 disc extrusion. To optimize the potential for full neurologic recovery of sphincter function, surgical decompression should ideally be performed within what maximum time frame from symptom onset?
Explanation
Question 73
A 35-year-old male undergoes a successful primary L4-L5 microdiscectomy for a herniated disc. He asks about the risk of recurrence. What is the generally accepted rate of recurrent disc herniation at the same level following a primary lumbar microdiscectomy?
Explanation
Question 74
During a wide lumbar laminectomy and medial facetectomy for severe central and lateral recess stenosis at L4-L5, excessive resection of the pars interarticularis can lead to iatrogenic spondylolisthesis. Biomechanical instability is most likely to occur if the bilateral pars resection exceeds what percentage?
Explanation
Question 75
A 65-year-old male with neurogenic claudication is found to have an L4-L5 degenerative spondylolisthesis. Which of the following findings on dynamic flexion-extension radiographs is the most widely accepted threshold to define dynamic instability, thereby strongly supporting the addition of fusion to a surgical decompression?
Explanation
Question 76
Dysplastic (Wiltse Type I) spondylolisthesis is characterized by congenital abnormalities of the upper sacrum or the neural arch of L5. Which of the following associated findings is most highly correlated with this specific subtype?
Explanation
Question 77
According to the Wiltse classification, Type IV (Traumatic) spondylolisthesis is characterized by an acute fracture involving which specific anatomical structure?
Explanation
Question 78
A 45-year-old male presents with left anterior thigh pain and weakness in left knee extension. His left patellar reflex is symmetrically diminished compared to the right. MRI reveals a far-lateral disc herniation. At which lumbar level is this far-lateral herniation most likely located?
Explanation
Question 79
A 20-year-old collegiate gymnast complains of isolated, persistent mechanical low back pain. Radiographs and CT show a bilateral L5 pars defect without spondylolisthesis. After 9 months of conservative care, surgery is considered. Which diagnostic test is most appropriate to confirm that the pars defects are the primary pain generators before performing a direct pars repair?
Explanation
Question 80
A 14-year-old soccer player presents with a 4-week history of focal lower back pain exacerbated by extension. Plain radiographs (AP, lateral, and obliques) of the lumbar spine are completely normal. Which of the following is the most sensitive imaging modality to detect an early, acute pars interarticularis stress reaction in this patient?
Explanation
Question 81
When evaluating a patient with suspected cauda equina syndrome, checking the bulbocavernosus reflex is part of the neurologic exam. Which of the following spinal segments mediates this reflex?
Explanation
None
