Pediatric Orthopaedics, Hand Surgery, Spine Trauma Review for ABOS Part I | Part 22303

Key Takeaway
This comprehensive module prepares candidates for the ABOS Part I and AAOS OITE exams. It covers pediatric orthopaedics, including fractures, scoliosis, and nonaccidental trauma. Key topics in hand surgery (digital nerve/artery repair) and spine trauma (SCIWORA, ATLS principles) are thoroughly reviewed for board success.
Pediatric Orthopaedics, Hand Surgery, Spine Trauma Review for ABOS Part I | Part 22303
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 7-year-old male presents to the emergency department after falling from a tree, sustaining a Gartland Type III supracondylar humerus fracture with posteromedial displacement. Initial neurovascular examination reveals a warm, well-perfused hand with good capillary refill, but no palpable radial pulse. There are no acute neurological deficits. After successful closed reduction and percutaneous pinning with lateral-entry K-wires, the radial pulse remains non-palpable, but the hand remains warm, pink, and well-perfused with normal sensation and motor function. What is the most appropriate next step in management?
Explanation
Correct Answer: C
The patient presents with a 'pulseless pink' hand after reduction and pinning of a supracondylar humerus fracture. The case text explicitly discusses the controversy surrounding this scenario. While a 'pulseless pale' hand is an absolute surgical emergency requiring immediate exploration, a 'pulseless pink' hand (where the hand remains warm, well-perfused, and neurologically intact despite an absent pulse) allows for a period of observation. The text states: 'More recent literature... suggests that if the hand remains warm and well-perfused with normal capillary refill and no neurological deficit after successful closed reduction and pinning, observation for pulse return may be appropriate, with exploration reserved for signs of ischemia or evolving neurological deficits. The key is strict observation.'
- Option A (Immediate surgical exploration of the brachial artery): This would be the correct step for a 'pulseless pale' hand where perfusion is compromised, or if observation of a 'pulseless pink' hand fails and signs of ischemia develop. It is not the immediate next step for a stable 'pulseless pink' hand.
- Option B (Urgent angiography to delineate the vascular injury): Angiography is typically considered if observation fails and vascular injury is suspected, or if there's a need for precise mapping before exploration. It's not the immediate first step after a stable reduction in a 'pulseless pink' scenario.
- Option C (Observation for 1-2 hours with strict neurovascular monitoring): This aligns directly with the current understanding and guidelines for a 'pulseless pink' hand after successful reduction and stabilization. The goal is to monitor for spontaneous return of the pulse or any signs of evolving ischemia or neurological compromise.
- Option D (Removal of K-wires and re-reduction of the fracture): The fracture is stated to be successfully reduced and pinned. Re-reduction is indicated if the reduction is lost or if the initial reduction was inadequate and contributing to the vascular issue. In this scenario, the reduction is stable, and the pulselessness is likely due to spasm or intimal injury, not persistent compression from the fracture itself.
- Option E (Application of a long arm cast and discharge with close follow-up): Discharging a patient with a non-palpable radial pulse, even if the hand is pink and warm, without a period of close observation in a monitored setting, is unsafe and could lead to missed evolving ischemia.
Question 2
A 9-year-old child presents with a Gartland Type III supracondylar humerus fracture, displaced posteromedially. During closed reduction, which of the following maneuvers is most critical for correcting the rotational component of this specific fracture pattern?
Explanation
Correct Answer: C
The case text details the specific reduction maneuvers for supracondylar humerus fractures: 'Correction of Rotation: This is crucial. For posteromedial displacement, pronate the forearm. For posterolateral displacement, supinate the forearm. The common type III extension fracture with posteromedial displacement often requires pronation to disengage the radial column.'
- Option A (Applying valgus stress to the elbow): Valgus stress is used to correct varus angulation, not primarily rotational deformity.
- Option B (Maintaining the forearm in supination): Supination is indicated for posterolateral displacement, not posteromedial.
- Option C (Pronating the forearm): This is the correct maneuver for posteromedial displacement, as described in the text, to help disengage the radial column and correct rotation.
- Option D (Applying varus stress to the elbow): Varus stress is used to correct valgus angulation, not primarily rotational deformity.
- Option E (Hyperflexing the elbow beyond 120 degrees): While flexion is a critical part of the reduction maneuver to bring the olecranon into the fossa, hyperflexion beyond 110 degrees can risk neurovascular compression, especially if the reduction is not complete, and is not the primary maneuver for correcting rotation.
Question 3
A 6-year-old child sustains a complete, dorsally angulated distal radius fracture. Radiographs show 25 degrees of dorsal angulation and 5 mm of shortening. The child is right-hand dominant. Based on the principles of pediatric fracture management, what is the most appropriate initial management strategy?
Explanation
Correct Answer: C
The case text highlights the significant remodeling potential in younger children for distal radius fractures. It states: 'Acceptable angulation varies significantly with age. For distal radius, 20-25 degrees of dorsal angulation is often acceptable in children under 10, decreasing to 10-15 degrees in adolescents. Rotational deformity is poorly tolerated at any age. Shortening up to 1 cm can remodel.' This 6-year-old falls within the age group where 25 degrees of dorsal angulation and 5 mm of shortening are generally acceptable after closed reduction and casting.
- Option A (Immediate open reduction and internal fixation with a plate): ORIF is rarely indicated for isolated distal radius fractures in children, typically reserved for open fractures, highly comminuted articular fractures, or irreducibility with soft tissue interposition. This fracture does not meet those criteria.
- Option B (Closed reduction and percutaneous K-wire fixation): K-wire fixation is indicated for unstable fractures after reduction, large metaphyseal-diaphyseal angle, or significant displacement in older children that cannot be maintained in a cast. While this fracture is complete and displaced, the angulation and shortening are within acceptable limits for a 6-year-old after closed reduction and casting, making K-wires potentially overtreatment initially.
- Option C (Closed reduction and long arm cast application): Given the acceptable angulation and shortening for a 6-year-old, closed reduction followed by immobilization in a cast (often a short arm cast for distal radius, but a long arm cast might be chosen for initial stability or surgeon preference) is the most appropriate initial management. The text mentions 'The majority of pediatric fractures are managed non-operatively.'
- Option D (Observation with a short arm splint due to excellent remodeling potential): While remodeling potential is excellent, a complete, dorsally angulated fracture requires reduction to achieve acceptable alignment and prevent malunion, even if minor. Observation without reduction is not appropriate for a displaced complete fracture.
- Option E (Elastic stable intramedullary nailing (ESIN)): ESINs are typically used for unstable forearm shaft fractures, significantly displaced distal radius fractures, comminuted patterns, and in older children/adolescents, especially when K-wires might not provide sufficient stability or for diaphyseal fractures. For a simple complete distal radius fracture within acceptable parameters for a 6-year-old, it's generally not the first-line treatment.
Question 4
A 12-year-old adolescent sustains a Salter-Harris Type III fracture of the distal radial physis. Radiographs confirm intra-articular involvement and 2 mm of displacement. The patient is skeletally immature with significant remaining growth. What is the most critical aspect of management for this specific physeal injury?
Explanation
Correct Answer: C
The case text explicitly addresses the management of Salter-Harris Type III and IV fractures: 'Specific Physeal Injuries: Salter-Harris type III and IV fractures, particularly intra-articular ones, require anatomical reduction to prevent growth arrest and articular incongruity.' A 12-year-old with significant remaining growth makes this even more critical.
- Option A (Immobilization in a short arm cast for 6 weeks): While immobilization is necessary, simply casting without anatomical reduction for a displaced SH Type III fracture is insufficient and will likely lead to complications.
- Option B (Aggressive physical therapy to prevent stiffness): Rehabilitation is important post-fixation, but aggressive physical therapy is not the critical initial management for a displaced intra-articular physeal fracture and can even be detrimental if the fracture is not anatomically reduced and stable.
- Option C (Anatomical reduction to prevent growth arrest and articular incongruity): This is the most critical aspect. SH Type III fractures involve the epiphysis and articular surface. Any displacement can lead to a step-off in the joint, causing premature arthritis, and can also damage the growth plate, leading to angular deformity or limb length discrepancy. Anatomical reduction, often requiring surgical intervention, is paramount.
- Option D (Observation for spontaneous remodeling of the displacement): Remodeling potential is limited for intra-articular displacement and for older children/adolescents. Furthermore, rotational deformities and articular step-offs remodel poorly at any age.
- Option E (Percutaneous pinning with pins crossing the physis for maximum stability): While pinning might be part of the surgical management to achieve and maintain anatomical reduction, pins crossing the physis should generally be avoided if possible, or placed in a way that minimizes damage (e.g., smooth pins, removed timely). The primary goal is anatomical reduction, and the method of fixation is secondary to that goal.
Question 5
A 10-year-old male presents with a severely displaced forearm shaft fracture involving both the radius and ulna. He complains of severe pain, disproportionate to the injury, and pain with passive extension of his fingers. On examination, his forearm is tense and swollen, and he has paresthesia in the median nerve distribution. Radial and ulnar pulses are palpable, and capillary refill is brisk. What is the most appropriate immediate management?
Explanation
Correct Answer: D
The patient's symptoms (pain out of proportion, pain with passive stretch of fingers, paresthesia, tense compartments) are classic signs of impending or manifest compartment syndrome, as detailed in the case text under 'Complications & Management'. The text states: 'Compartment Syndrome: Pain out of proportion to injury, pain with passive stretch, paresthesia, tense compartments, weakness. (Pulselessness, pallor are late signs). Salvage Strategy: Emergency! Immediate four-compartment fasciotomy of the forearm.'
- Option A (Elevation of the limb and close observation): While elevation is part of general fracture management, it is insufficient and dangerous for compartment syndrome, which requires immediate surgical intervention. Close observation will lead to irreversible muscle and nerve damage.
- Option B (Administration of intravenous opioids and muscle relaxants): Pain medication might mask the critical symptom of pain out of proportion and delay diagnosis, which is detrimental in compartment syndrome. Muscle relaxants are not indicated.
- Option C (Urgent closed reduction and casting): While the fracture needs reduction, attempting closed reduction and casting in the presence of compartment syndrome symptoms can worsen the condition by increasing pressure within the already compromised compartments. The compartment syndrome must be addressed first.
- Option D (Immediate four-compartment fasciotomy of the forearm): This is the definitive and emergency treatment for compartment syndrome to relieve pressure and prevent irreversible tissue damage.
- Option E (CT scan of the forearm to assess soft tissue injury): Imaging like CT is not indicated for the acute diagnosis and management of compartment syndrome. Clinical diagnosis and immediate surgical intervention are paramount.
Question 6
During percutaneous pinning of a Gartland Type III supracondylar humerus fracture, the surgeon opts for a medial and lateral crossed pin configuration. Which of the following is the most critical step to minimize the risk of iatrogenic ulnar nerve injury during medial pin placement?
Explanation
Correct Answer: C
The case text specifically addresses the risk of ulnar nerve injury with medial pinning: 'Medial and Lateral Crossed Pins: Offers theoretically greater stability, but carries a higher risk of iatrogenic ulnar nerve injury. Ulnar Nerve Protection: The elbow must be fully extended to move the ulnar nerve posteriorly, away from the medial epicondyle. Alternatively, a small incision can be made to palpate and protect the ulnar nerve directly (mini-open technique).'
- Option A (Inserting the medial pin with the elbow in 90 degrees of flexion): This is incorrect. Flexing the elbow brings the ulnar nerve anteriorly, making it more vulnerable to injury during medial pin placement. The text states the elbow should be fully extended to move the nerve posteriorly.
- Option B (Using a smaller diameter K-wire for the medial pin): While appropriate K-wire size is important, using a smaller diameter wire does not inherently protect the ulnar nerve from direct injury if its path is in the nerve's trajectory.
- Option C (Performing a mini-open technique to palpate and protect the ulnar nerve): This is a direct and effective method of ulnar nerve protection, as described in the text. It allows for direct visualization or palpation of the nerve, moving it out of the path of the K-wire.
- Option D (Inserting the medial pin from a more anterior entry point): This might actually increase the risk of ulnar nerve injury, as the nerve courses posteriorly to the medial epicondyle but can be more anterior with elbow flexion. A posterior entry point with elbow extension is generally safer, or direct protection.
- Option E (Ensuring the lateral pin is placed first to stabilize the fracture): While stabilizing the fracture with lateral pins first is a common practice, it does not directly protect the ulnar nerve during subsequent medial pin placement.
Question 7
A 4-year-old child presents with an isolated, non-displaced greenstick fracture of the distal radius. The interosseous membrane is intact. Which of the following statements regarding this injury and its management is most accurate?
Explanation
Correct Answer: C
The question asks for the most accurate statement regarding a greenstick distal radius fracture in a 4-year-old, drawing on various sections of the text.
- Option A (The strong interosseous membrane dictates that this isolated fracture implies high-energy trauma): The text states: 'The strong interosseous membrane dictates that isolated shaft fractures are rare, implying high-energy trauma if present.' This statement refers to shaft fractures, not distal radius fractures. Distal radius fractures are very common and often isolated, not necessarily implying high-energy trauma.
- Option B (Rotational deformities remodel well in this age group): The text explicitly states: 'Rotational deformities remodel poorly, regardless of age.' This makes the statement inaccurate.
- Option C (The thick periosteum often hinges dorsally, aiding in reduction but requiring careful assessment of stability): The text states under 'Distal Radius & Ulna': 'The thick periosteum often hinges dorsally, allowing for closed reduction but requiring careful assessment of stability.' This is an accurate statement and a key characteristic of pediatric distal radius fractures.
- Option D (This fracture pattern typically requires percutaneous K-wire fixation due to inherent instability): Greenstick fractures are described as 'inherently stable fracture patterns that typically heal well with immobilization' in the 'Non-Operative Indications' section. K-wire fixation is generally not required for non-displaced greenstick fractures.
- Option E (Aggressive passive stretching should be initiated early in rehabilitation to prevent stiffness): The 'Post-Operative Rehabilitation Protocols' section, particularly for SCHF, warns: 'Avoid forceful passive stretching or manipulation of the elbow joint, as this can increase the risk of heterotopic ossification and myositis ossificans.' This principle generally applies to pediatric fractures, favoring gentle active range of motion.
Question 8
A 14-year-old male sustains a displaced, comminuted distal radius fracture. He is skeletally mature. After closed reduction, the fracture remains unstable and significantly displaced. Which of the following fixation methods would be most appropriate for this patient, considering his age and fracture pattern?
Explanation
Correct Answer: D
The patient is a 14-year-old male with a displaced, comminuted, and unstable distal radius fracture. While K-wires and ESINs are options for pediatric fractures, the combination of age (older adolescent, closer to skeletal maturity), comminution, and instability makes ORIF with a plate a strong consideration, especially if anatomical reduction and stable fixation are difficult to achieve otherwise.
- Option A (Long arm cast immobilization without fixation): Given the fracture is unstable and significantly displaced after reduction, casting alone is unlikely to maintain an acceptable reduction, especially in an older adolescent with less remodeling potential.
- Option B (Percutaneous K-wire fixation): K-wires are a common and effective method for unstable distal radius fractures. However, for a comminuted fracture in an older adolescent, K-wires might not provide sufficient stability, and maintaining reduction could be challenging.
- Option C (Elastic stable intramedullary nailing (ESIN)): ESINs are primarily used for unstable forearm shaft fractures and some significantly displaced distal radius fractures, particularly in younger children or adolescents. While an option, for a comminuted fracture, a plate might offer more rigid and anatomical fixation.
- Option D (Open reduction and internal fixation with a small pediatric plate): The text states under 'Distal Radius Fracture - Open Reduction Internal Fixation (ORIF)': 'Indications: Very rare for isolated distal radius fractures; primarily for open fractures, highly comminuted articular fractures, or irreducibility with soft tissue interposition. Fixation: Small pediatric plates and screws or K-wires.' While rare for isolated distal radius fractures, a comminuted and unstable fracture in an older adolescent (closer to adult bone) is a stronger indication for ORIF with a plate to achieve and maintain anatomical reduction, especially if closed methods fail. This provides the most rigid fixation for a comminuted pattern.
- Option E (Observation with a short arm splint): This is inappropriate for a displaced, unstable fracture that requires reduction and stabilization.
Question 9
A 5-year-old child is recovering from a successfully pinned Gartland Type II supracondylar humerus fracture. K-wires were removed at 3 weeks post-operatively. Which of the following is the most appropriate recommendation for the initial phase of rehabilitation?
Explanation
Correct Answer: B
The 'Post-Operative Rehabilitation Protocols' section for Supracondylar Humerus Fracture (Pinned) states: 'After pin removal, a posterior splint may be used for comfort, but active range of motion of the elbow and wrist is immediately encouraged. Crucial: Avoid forceful passive stretching or manipulation of the elbow joint, as this can increase the risk of heterotopic ossification and myositis ossificans. Gravity-assisted gentle flexion/extension exercises.'
- Option A (Initiate aggressive passive stretching of the elbow to regain full extension): This is explicitly warned against in the text due to the risk of heterotopic ossification and myositis ossificans.
- Option B (Encourage gentle active range of motion (AROM) exercises for the elbow and wrist): This is the correct and recommended approach for early rehabilitation after pin removal, as it helps restore motion without the risks associated with passive stretching.
- Option C (Begin immediate weight-bearing activities to strengthen the arm): Weight-bearing and strengthening exercises are part of a later phase of rehabilitation (4-8+ weeks), not immediately after pin removal.
- Option D (Maintain strict immobilization in a cast for an additional 3 weeks): K-wires are typically removed when early callus formation is evident (around 3-4 weeks), and at that point, active motion is encouraged, not continued strict immobilization.
- Option E (Refer for immediate occupational therapy focusing on fine motor skills): While occupational therapy may be beneficial, the immediate focus after pin removal for an elbow fracture is on regaining elbow and wrist range of motion, not primarily fine motor skills, unless there are specific neurological deficits.
Question 10
A 3-year-old child presents with a suspected non-displaced lateral condyle fracture of the humerus. Plain radiographs are equivocal due to the largely cartilaginous nature of the distal humerus at this age. What is the most appropriate next imaging modality to confirm the diagnosis and guide management?
Explanation
Correct Answer: B
The case text discusses imaging modalities: 'Computed Tomography (CT): Reserved for complex intra-articular fractures (e.g., lateral condyle, capitellum), multi-fragmentary fractures, or when precise anatomical detail is needed for surgical planning. Not routinely used due to radiation exposure.' In a 3-year-old, the lateral condyle is largely cartilaginous, making plain radiographs difficult to interpret for non-displaced fractures. CT provides superior bony detail to confirm the fracture and assess displacement, which is crucial for lateral condyle fractures due to their high risk of nonunion and growth disturbance if not anatomically reduced.
- Option A (Magnetic Resonance Imaging (MRI)): MRI is primarily for soft tissue injuries, ligamentous damage, or avascular necrosis. While it can show cartilage, CT is generally preferred for acute bony detail, especially for fracture assessment.
- Option B (Computed Tomography (CT) scan): This is the most appropriate choice. CT provides excellent bony detail, which is essential for diagnosing subtle or non-displaced intra-articular fractures like lateral condyle fractures in young children where much of the bone is still cartilage and not visible on plain X-rays.
- Option C (Stress views of the elbow): Stress views are rarely indicated in acute trauma and are primarily for assessing ligamentous stability, not for diagnosing a bony fracture.
- Option D (Repeat plain radiographs in 1 week): While sometimes used for subtle fractures (e.g., scaphoid), waiting a week for a potentially displaced intra-articular fracture like a lateral condyle fracture can delay definitive treatment and worsen prognosis.
- Option E (Arteriography): Arteriography is indicated for suspected vascular injury (e.g., pulseless pale hand where reduction fails), not for diagnosing a bony fracture.
Question 11
A 10-year-old patient presents with a malunion of a forearm shaft fracture, exhibiting 20 degrees of angulation in the sagittal plane and 15 degrees of rotational deformity. The fracture occurred 6 months ago and has healed. Based on the remodeling potential described in the case, what is the most important consideration for surgical correction?
Explanation
Correct Answer: B
The case text provides clear guidance on remodeling potential: 'Remodeling potential is significant, especially in younger children, but rotational deformities remodel poorly. Rotational deformities remodel poorly, regardless of age. Angulatory deformities remodel best when in the plane of motion of the joint and closer to the physis.'
- Option A (The sagittal plane angulation will remodel completely over time, requiring no intervention): While sagittal plane angulation remodels well, 20 degrees in a 10-year-old (an older child) might not remodel completely, especially if it's a shaft fracture (further from the physis). The statement 'completely' is too absolute.
- Option B (The rotational deformity will remodel poorly and is the primary indication for corrective osteotomy): This is accurate. The text explicitly states that rotational deformities remodel poorly regardless of age. Therefore, a 15-degree rotational deformity is a significant concern and a strong indication for surgical correction (osteotomy) if it causes functional impairment or severe cosmetic deformity.
- Option C (Both angulation and rotation will remodel significantly due to the patient's age): This is incorrect. While angulation might remodel to some extent, rotational deformities remodel poorly.
- Option D (Surgical correction is contraindicated as the fracture has already healed): This is incorrect. Corrective osteotomy is a standard procedure for symptomatic malunions after fracture healing, especially for deformities that do not remodel.
- Option E (The distance from the physis is the sole determinant of remodeling potential): This is incorrect. While distance from the physis is a factor, age and the plane of deformity (sagittal vs. coronal) are also critical, and rotational deformities remodel poorly irrespective of these factors.
Question 12
A 32-year-old right-hand dominant carpenter sustains a clean laceration to the volar aspect of his left ring finger at the level of the proximal phalanx. Examination reveals complete loss of sensation on the ulnar side of the ring finger and a positive Allen's test for the ulnar digital artery of that digit. Doppler ultrasound confirms absent flow in the ulnar proper digital artery. The flexor tendons are intact. Given the surgical anatomy described in the case, which of the following statements best describes the typical anatomical relationship of the proper digital nerve and artery at the mid-phalanx level?
Explanation
Correct Answer: C
The case explicitly states under 'Surgical Anatomy & Biomechanics' that 'Distally, their relationship with the arteries can vary, but generally, the nerve is more superficial and closer to the skin than the artery, especially in the mid-phalanx.' This makes the nerve more vulnerable to superficial lacerations at this level.
- Option A is incorrect because while the relationship can vary, the nerve is generally more superficial, not deep and dorsal, at the mid-phalanx. At the DIP joint level, they typically lie dorsally to the digital artery, but this is not the mid-phalanx.
- Option B is incorrect because the nerve is generally more superficial than the artery at the mid-phalanx, not the artery being more superficial. Both are volar to the flexor tendon sheath, but the relative depth differs.
- Option D is incorrect as the case notes that the relationship 'can vary' distally, and specifically states that at the DIP joint level, the nerve typically lies dorsally to the digital artery, contradicting a consistent volar relationship.
- Option E is incorrect because the case states the neurovascular bundles are 'encased in a delicate fibrofatty sheath within the digital canal, lying volar to the flexor tendon sheath,' not within the sheath itself.
Question 13
A 28-year-old patient presents with a 1.5 cm laceration to the radial aspect of the left index finger, sustained 48 hours prior. Examination reveals complete loss of sensation on the radial side of the index finger, with a positive Tinel's sign at the injury site. The digit is well-perfused. Surgical exploration confirms a complete transection of the radial proper digital nerve of the index finger with a 5 mm gap after minimal debridement. Based on the case's guidelines for nerve repair, what is the most appropriate initial surgical management?
Explanation
Correct Answer: C
The case states under 'Indications for Surgical Intervention' that 'Acute Repair: Indicated for clean lacerations identified within 72 hours, ideally within 24 hours.' The patient presents within 48 hours, making acute primary repair appropriate. For nerve repair technique, the case states 'Epineurial Repair: This is the most common technique for proper digital nerves... The goal is to align the nerve without rotation and achieve precise coaptation of the fascicular bundles.' A 5 mm gap after minimal debridement is generally manageable with direct, tension-free epineurial repair, especially with gentle mobilization, and does not typically necessitate grafting or conduits which are reserved for larger gaps (>1 cm).
- Option A is incorrect because secondary repair is for missed injuries or failed primary repairs (after 3 weeks), and a 5 mm gap is usually amenable to direct repair, not requiring a graft unless significant tension is present after mobilization.
- Option B is incorrect because delayed primary repair is for conditions preventing immediate repair, which is not the case here (48 hours is within the acute window). Conduits are typically considered for smaller gaps, but direct repair is preferred if tension-free.
- Option D is incorrect as a complete transection of a proper digital nerve requires surgical repair to optimize functional recovery; observation for spontaneous regeneration is not indicated for complete transections.
- Option E is incorrect because excision and relocation are management strategies for painful neuromas, not for acute nerve transections where the goal is to restore continuity and function.
Question 14
A 55-year-old diabetic patient presents to the emergency department 10 hours after sustaining a severe crush injury to his left small finger. The digit is pale, cold, and has absent capillary refill. Doppler signals are absent over both proper digital arteries. Radiographs show a comminuted fracture of the proximal phalanx. Given the patient's presentation and the information in the case, what is the most critical immediate surgical priority?
Explanation
Correct Answer: C
The case explicitly states under 'Combined Injuries' that 'In cases of combined digital nerve and artery injury, vascular repair takes precedence if the digit is ischemic. Restoring blood flow is critical for tissue viability.' The patient presents with clear signs of critical digital ischemia (pale, cold, absent capillary refill, absent Doppler signals) 10 hours post-injury, which is beyond the 'golden period' for warm ischemia (6-8 hours) but still within a window where revascularization can salvage the digit. Therefore, immediate revascularization is the paramount priority to prevent irreversible tissue damage and potential necrosis.
- Option A is incorrect because while the fracture needs addressing, it is secondary to restoring blood flow in an ischemic digit.
- Option B is incorrect because nerve repair, even delayed primary, is secondary to establishing vascularity. Debridement is important but must be followed by revascularization.
- Option D is incorrect as neuroma management is for chronic painful conditions, not acute ischemic emergencies.
- Option E is incorrect because observation for 24 hours in an ischemic digit would lead to irreversible necrosis. Immediate intervention is required.
Question 15
A 40-year-old construction worker undergoes surgical repair of a complete transection of the radial proper digital nerve of his middle finger, sustained from a sharp saw blade 24 hours prior. During the procedure, a 1.5 cm nerve gap is identified after minimal debridement and gentle mobilization. The surgeon determines a tension-free direct repair is not possible. Based on the case's guidelines, what is the most appropriate next step for nerve reconstruction?
Explanation
Correct Answer: C
The case states under 'Nerve Grafting' that 'If a significant gap (typically >1 cm) exists after mobilization and tension-free repair is not possible, an autologous nerve graft is indicated.' A 1.5 cm gap falls into this category. The 'Key Literature & Guidelines' section further reinforces this: 'For nerve gaps, autologous nerve grafting (e.g., sural nerve... ) remains the most reliable method for bridging larger defects. Meta-analyses and systematic reviews generally show superior outcomes for autografts compared to nerve conduits for gaps >1 cm.'
- Option A is incorrect because the case emphasizes 'tension-free' repair. A tensioned repair leads to poor outcomes due to ischemia and scar formation.
- Option B is incorrect because while conduits can be used, the case indicates they are primarily for 'smaller gaps (<1 cm)' and that autografts are generally superior for gaps >1 cm.
- Option D is incorrect as excision and relocation are for painful neuromas, not for bridging an acute nerve gap to restore continuity.
- Option E is incorrect because delaying repair for 6-8 weeks would lead to further nerve retraction and scar formation, making reconstruction more difficult and potentially compromising outcomes. Acute management with grafting is preferred.
Question 16
A 60-year-old patient undergoes microvascular repair of a transected proper digital artery in the ring finger following a replantation attempt. Post-operatively, 4 hours later, the digit becomes cool, pale, and capillary refill is sluggish at 4 seconds. Doppler signals are significantly diminished. The nursing staff immediately notifies the surgeon. Based on the case's discussion of complications, what is the most appropriate immediate management step?
Explanation
Correct Answer: D
The case describes 'Thrombosis of Arterial Repair' as a 'surgical emergency.' It states: 'Signs include a cool, pale, or cyanotic digit, sluggish capillary refill, and absent Doppler signals. Immediate re-exploration is warranted. The anastomosis is opened, any thrombus is removed (thrombectomy), and the anastomosis is revised after ensuring healthy vessel ends.' The patient's symptoms are classic for arterial thrombosis, requiring urgent surgical intervention.
- Option A is incorrect because antibiotics are for infection, and elevation might worsen perfusion in an already compromised digit.
- Option B is incorrect because while topical papaverine can help with vasospasm, the signs here (cool, pale, sluggish refill, diminished Doppler) are more indicative of thrombosis, which requires surgical intervention, not just observation.
- Option C is incorrect because while systemic anticoagulation and antiplatelet agents are often used post-operatively to prevent re-thrombosis, they are not the primary immediate treatment for an acute, established thrombosis that is compromising digital viability. Surgical revision is paramount.
- Option E is incorrect because a sympathetic block is primarily for vasospasm, but the clinical picture here strongly suggests thrombosis, which is a mechanical obstruction requiring surgical correction.
Question 17
A 48-year-old patient is recovering from a repair of a complete transection of the ulnar proper digital nerve of the small finger. Three weeks post-operatively, the patient complains of severe hypersensitivity and shooting pain in the small finger, particularly when touching the scar. Examination reveals a positive Tinel's sign at the repair site and significant allodynia. Conservative management with NSAIDs and topical analgesics has provided minimal relief. According to the case, which of the following is a recognized surgical option for managing this complication?
Explanation
Correct Answer: B
The patient's symptoms (severe hypersensitivity, shooting pain, positive Tinel's, allodynia, and failure of conservative management) are highly suggestive of a painful traumatic neuroma. The case, under 'Neuroma Excision and Management,' lists several surgical options: 'For symptomatic neuromas, surgical options include: ... Excision and Relocation: The neuroma is excised, and the nerve end is transposed into a well-vascularized, soft tissue bed (e.g., muscle, bone tunnel) away from external pressure.' This directly addresses the described complication.
- Option A is incorrect because revision neurorrhaphy with a conduit is for nerve gaps or failed repairs, not specifically for a painful neuroma where the goal is to manage the nerve stump.
- Option C is incorrect as systemic corticosteroids are not a primary treatment for painful neuromas and carry significant side effects.
- Option D is incorrect because while desensitization is part of rehabilitation, a dynamic splint is for motion, and this patient's severe pain and allodynia suggest a more aggressive approach is needed after conservative failure.
- Option E is incorrect as severe, debilitating pain and allodynia are not a 'normal part of nerve regeneration' and warrant intervention, especially after conservative measures fail.
Question 18
A 22-year-old musician undergoes repair of a complete transection of the radial proper digital nerve of the middle finger. Post-operatively, the hand therapist initiates rehabilitation. Based on the case's post-operative protocols, what is the primary goal of the initial immobilization phase (first 3-4 weeks)?
Explanation
Correct Answer: C
The case, under 'Post-Operative Rehabilitation Protocols - Initial Immobilization & Protection,' clearly states the goal: 'Protect the nerve and/or artery repair from tension and external forces, control edema, and manage pain.' It also specifies splinting to minimize tension on the repaired nerve.
- Option A is incorrect because full active range of motion is a later goal, not during the initial immobilization phase where protection is paramount.
- Option B is incorrect as aggressive strengthening is part of the later stages of rehabilitation, after initial healing and controlled motion have been established.
- Option D is incorrect because advanced sensory re-education (graphesthesia, stereognosis) is for later stages, after protective sensation returns and basic discrimination is achieved.
- Option E is incorrect because while cold intolerance is a common complication, its prevention is not the primary goal of initial immobilization. Desensitization is part of early sensory re-education, but the main focus of the initial phase is protection.
Question 19
A 35-year-old patient underwent repair of a proper digital nerve laceration 18 months ago. Despite diligent hand therapy, the patient reports persistent difficulty distinguishing textures and identifying objects without visual input, with a static two-point discrimination (2PD) of 12 mm in the affected fingertip. The patient also complains of significant cold intolerance. Based on the 'Key Literature & Guidelines' section of the case, which statement best reflects the expected long-term outcomes for digital nerve repair?
Explanation
Correct Answer: B
The 'Key Literature & Guidelines' section explicitly states under 'Outcomes of Nerve Repair': 'Achieving "excellent" sensory recovery (2PD < 6mm) is challenging and occurs in only 20-50% of repairs. "Good" recovery (2PD 6-15mm, protective sensation) is more common and represents a functionally acceptable outcome.' It also highlights: 'The literature consistently highlights the high incidence of cold intolerance following digital nerve injuries, regardless of the quality of nerve repair, with rates ranging from 30-70%.' The patient's 2PD of 12 mm falls within the 'good' recovery range, and persistent cold intolerance is a known, common complication.
- Option A is incorrect because excellent sensory recovery is challenging and cold intolerance is common, not rare.
- Option C is incorrect because complete return to normal sensation is rare, and cold intolerance often persists, not resolving spontaneously. Recovery can take 12-18 months or longer.
- Option D is incorrect because a 2PD of 12 mm is considered 'good' recovery and does not automatically mandate revision surgery, especially after 18 months.
- Option E is incorrect because while significant recovery occurs in the first 6-12 months, nerve regeneration and sensory re-education can continue to yield improvements for 12-18 months or even longer.
Question 20
A 50-year-old patient presents with a 2 cm laceration to the volar aspect of the thumb, sustained 3 days ago. Examination reveals complete loss of sensation on the radial side of the thumb. The common digital nerves arise from the median and ulnar nerves in the palm. Based on the anatomical description in the case, which nerve is primarily responsible for the sensory innervation of the radial side of the thumb?
Explanation
Correct Answer: B
The 'Surgical Anatomy & Biomechanics' section states: 'Each digit, excluding the thumb and the radial aspect of the index finger which have specific innervation from the median nerve, typically receives two proper digital nerves and two proper digital arteries.' This indicates that the thumb's innervation is somewhat distinct. Specifically, the radial side of the thumb is innervated by a proper digital nerve that branches directly from the median nerve, not via a common digital nerve that then bifurcates for the thumb. The median nerve gives rise to three common digital nerves, but the thumb's innervation is mentioned as a specific exception.
- Option A is incorrect because the ulnar nerve primarily innervates the small finger and the ulnar side of the ring finger.
- Option B is correct as per the case's specific exclusion for the thumb's innervation.
- Option C is incorrect because while the radial nerve innervates the dorsum of the hand and some dorsal digits, its contribution to the volar aspect of the thumb is not described as primary for the proper digital nerve.
- Option D is incorrect because the case implies a direct innervation for the thumb from the median nerve, rather than through a common digital nerve that then bifurcates, which is the pattern for other digits.
- Option E is incorrect as the ulnar nerve does not innervate the radial side of the thumb.
Question 21
A 42-year-old patient is undergoing surgical repair of a proper digital nerve laceration in the middle finger. The surgeon is preparing for the repair under an operating microscope. According to the surgical technique described in the case, which of the following is the most appropriate suture material and technique for a primary epineurial repair of a proper digital nerve?
Explanation
Correct Answer: C
The 'Surgical Technique - Nerve Repair' section, under 'Repair Technique - Epineurial Repair,' states: 'Using 9-0 or 10-0 non-absorbable monofilament nylon sutures, 3-6 sutures are placed through the epineurium to approximate the nerve ends meticulously.' This directly matches option C.
- Option A is incorrect because 4-0 sutures are too large for digital nerve repair, and absorbable sutures are not typically used for primary nerve repair where long-term coaptation is desired.
- Option B is incorrect because 7-0 sutures are generally too large for proper digital nerves, and a running locked technique is not the standard for epineurial repair, which typically uses interrupted sutures for precise alignment.
- Option D is incorrect because 11-0 sutures might be too fine for epineurial repair (more common for fascicular repair, which is rarely indicated for digital nerves), and absorbable sutures are not preferred. Group fascicular repair is also rarely indicated for digital nerves.
- Option E is incorrect because heavy braided silk sutures are too traumatic and reactive for delicate nerve repair, and a mattress technique is not the standard for epineurial coaptation.
Question 22
A 29-year-old patient is 6 weeks post-operative from a combined repair of a proper digital nerve and artery in the index finger. The hand therapist is progressing the rehabilitation protocol. Which of the following activities is most appropriate to introduce during the early mobilization and sensory re-education phase, as described in the case?
Explanation
Correct Answer: C
The 'Post-Operative Rehabilitation Protocols - Early Mobilization & Sensory Re-education' section states: 'Gentle, controlled active flexion and extension exercises for all digital joints are initiated to promote tendon gliding and prevent joint stiffness. Exercises are performed within pain-free limits.' This is a key component of the early mobilization phase.
- Option A is incorrect because aggressive grip strengthening is part of the later stages of rehabilitation, not the early mobilization phase, where protection of the repair is still critical.
- Option B is incorrect because advanced sensory re-education, such as stereognosis and graphesthesia, is introduced in later stages, after basic protective sensation and discrimination have returned.
- Option D is incorrect because unrestricted return to heavy activities is only considered in the final stages of rehabilitation, after full strength, endurance, and refined sensation have been achieved, which can take 12-18 months or longer for nerve injuries.
- Option E is incorrect because continuous static splinting is typically for the initial immobilization phase (3-4 weeks) to protect the repair. In the early mobilization phase, the splint may be discontinued or transitioned to allow controlled motion.
Question 23
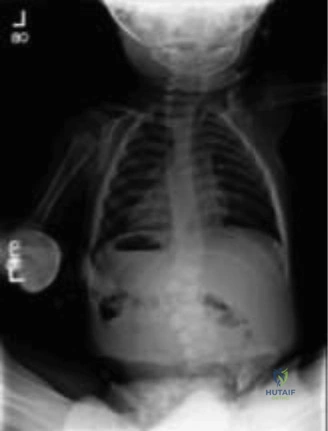
A 3-month-old boy is brought to the ER by his grandmother, who noticed his thigh was swollen, and he cried with leg movement during diaper changes. He is not voluntarily moving the affected leg. An X-ray is obtained as shown below:
What is your immediate primary concern, even before meeting the patient and family?
Explanation
Correct Answer: C
The correct answer is Nonaccidental Trauma (NAT). The case describes a femur fracture in a nonambulatory child less than 1 year of age. It is a critical teaching point that approximately 80% of femur fractures in nonambulatory children are due to nonaccidental trauma (child abuse). This high index of suspicion mandates that NAT be the immediate primary concern.
Option A (Compartment syndrome) is incorrect. While compartment syndrome is a serious complication of fractures, it is quite rare in the thigh after a femur fracture, especially in infants, and is not the most likely initial concern in this specific clinical scenario, although it should be assessed during the physical examination.
Option B (Birth trauma) is incorrect. The child is 3 months old. If the fracture had occurred at birth, it would likely be healed with a robust callus formation by this point, which is not suggested by the acute presentation.
Option D (Osteogenesis imperfecta) is incorrect. Osteogenesis imperfecta (OI) is a genetic disorder causing brittle bones and is certainly a differential diagnosis to consider in a child with unexplained fractures. However, nonaccidental trauma is statistically more common and must be ruled out first. If there is concern for OI based on history and examination, a work-up can be included as part of the overall evaluation of potential nonaccidental trauma.
Option E (Sepsis with osteomyelitis) is incorrect. While osteomyelitis can present with pain and swelling, the X-ray clearly shows a fracture, making infection a less likely primary diagnosis for the acute presentation of a swollen, painful, non-moving leg with a visible fracture.
Question 24
Following your initial evaluation of the 3-month-old boy with a femur fracture, a skeletal survey is performed due to high suspicion for nonaccidental trauma. The survey reveals a both-bone forearm fracture with callus formation, distal tibia corner fractures, and posteromedial rib fractures in various stages of healing.
Among the findings from the skeletal survey, which fracture types are considered most specific for nonaccidental trauma?
Explanation
Correct Answer: D
The correct answer is the rib fractures (particularly posteromedial) and corner fractures. The teaching case explicitly states that fractures with the highest specificity for nonaccidental trauma (NAT) are corner fractures, rib fractures (especially posteromedial rib fractures), scapular fractures, sternal fractures, and spinous process fractures.
Option A (The femur fracture, given the child's nonambulatory status) is incorrect. While a femur fracture in a nonambulatory child is highly concerning for NAT (as discussed in Q1), long-bone shaft fractures (like a femur shaft fracture) generally have low specificity for abuse when considered in isolation. The context of the child's age and non-ambulatory status elevates suspicion, but the fracture type itself is not among the 'most specific'.
Option B (Multiple fractures in different stages of healing) is incorrect. Multiple fractures and fractures in different stages of healing are indeed highly concerning for NAT and fall under 'moderate specificity' for abuse. However, they are not considered 'most specific' when compared to corner or posteromedial rib fractures.
Option C (The both-bone forearm fracture with callus formation) is incorrect. Similar to the femur fracture, long-bone shaft fractures (like a forearm fracture) have low specificity for abuse on their own. The presence of callus indicates an older injury, which is concerning in the context of NAT, but the fracture type itself is not 'most specific'.
Option E (Vertebral body fractures and transphyseal separations) is incorrect. Vertebral body fractures and transphyseal separations are listed as having 'moderate specificity' for abuse, not the highest specificity.
Question 25
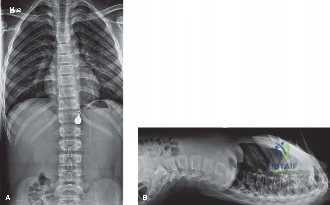
A 10-year-old premenarchal girl presents with a chief complaint of 'scoliosis'. A PA full spine X-ray, shown below, was performed after a positive forward-bend test. Her curve measures 48 degrees, and she is hyperkyphotic on the lateral X-ray. No neurologic abnormalities, spondylolysis, or spondylolisthesis are detected on physical exam.
What is the most appropriate next step in her evaluation and treatment?

Explanation
Correct Answer: E
The correct answer is to order an MRI of the cervical, thoracic, and lumbar spine. This patient, a 10-year-old premenarchal girl, has a large scoliotic curve (48 degrees) with onset before age 10, classifying it as juvenile scoliosis. It is estimated that approximately 20% of children with juvenile scoliosis (onset 3–10 years old) have an intraspinal anomaly. Therefore, obtaining an MRI of the entire spine is crucial to look for conditions such as Chiari malformation, syringomyelia (syrinx), tethered cord, or spinal cord tumors. To thoroughly evaluate for these potential underlying diagnoses, the entire neural axis, including the base of the brain and cervical spine, must be imaged.
Option A (Order laboratory tests including a CBC, ANA, and HLA-B27) is incorrect. While a CBC might be considered before potential surgical intervention, ANA and HLA-B27 are not typically indicated in the routine work-up of idiopathic or juvenile scoliosis unless there are specific clinical signs suggestive of inflammatory or rheumatologic conditions, which are not mentioned here.
Option B (Order a bone density scan) is incorrect. A bone density scan is not a necessary part of the routine work-up for juvenile scoliosis. It may be considered in selected patients with specific concerns about underlying bone density issues, but not as a primary next step here.
Option C (Prescribe a brace) is incorrect. For a curve of 48 degrees, bracing is generally not considered effective, and surgical intervention is often indicated. Even if the curve were smaller and bracing was a consideration, an MRI would still be necessary for a child with juvenile scoliosis to rule out intraspinal anomalies before initiating treatment.
Option D (Order an MRI of the thoracic and lumbar spine) is incorrect. While an MRI is the correct imaging modality, it must include the cervical spine and base of the brain to adequately evaluate for Chiari malformation and other potential intraspinal anomalies that can affect the entire neural axis. Limiting the MRI to only the thoracic and lumbar spine would be an incomplete evaluation.
Question 26
A 3-year-old boy presents with his parents, who have noticed his spine 'looks crooked' over the last year and appears to be worsening. On examination, you confirm a spinal curvature and order X-rays, which are shown below.
Based on the X-ray findings, what is the most appropriate diagnosis for this child's spinal condition?
Explanation
Correct Answer: C
The correct answer is Congenital scoliosis. The X-ray clearly demonstrates a hemivertebra in the lumbar spine. Congenital scoliosis is defined by structural abnormalities of the vertebrae that are present at birth, such as hemivertebrae, wedge vertebrae, or unilateral bars. These anomalies lead to an imbalance in spinal growth and result in a curvature.
Option A (Infantile scoliosis) is incorrect. Infantile scoliosis is typically diagnosed in children from birth to 3 years of age, but it refers to a curve without an underlying structural vertebral anomaly (i.e., idiopathic). This child has a clear structural anomaly.
Option B (Juvenile scoliosis) is incorrect. Juvenile scoliosis is diagnosed in children aged 3 to 10 years, but it also refers to idiopathic curves without underlying vertebral malformations.
Option D (Idiopathic scoliosis) is incorrect. Idiopathic scoliosis is a diagnosis of exclusion, meaning there is no identifiable cause for the spinal curvature. This child has a clear congenital vertebral anomaly (hemivertebra) as the cause.
Option E (A positional curve) is incorrect. A positional curve (or non-structural curve) is typically flexible and corrects with changes in position or bending. The presence of a hemivertebra indicates a fixed, structural abnormality, not merely a positional curve.
Question 27
In the context of congenital scoliosis, various vertebral anomalies can occur, leading to different rates of curve progression. Understanding these differences is crucial for prognosis and management.
What is the correct order of congenital vertebral anomaly types, from most likely to result in progressive scoliosis to least likely to progress?
Explanation
Correct Answer: E
The correct answer is Unilateral bar with contralateral hemivertebra, unilateral bar, hemivertebra, wedge vertebra, block vertebra. This order reflects the increasing severity and likelihood of curve progression in congenital scoliosis due to the imbalance in growth potential.
- Unilateral bar with contralateral hemivertebra: This is the most severe anomaly, as the unilateral bar acts as a tether on one side, preventing growth, while the contralateral hemivertebra provides an extra growth center on the opposite side. This combination creates a significant growth imbalance, leading to rapid and severe progression.
- Unilateral bar: A unilateral bar tethers growth on one side of the spine, leading to progressive curvature as the contralateral side continues to grow normally.
- Hemivertebra: A hemivertebra is a wedge-shaped vertebra that provides an extra growth center on one side, causing a curve. While it can lead to significant progression, it is generally less aggressive than a unilateral bar or a unilateral bar with a contralateral hemivertebra. The case mentions an average 2-5 degree progression per year for a hemivertebra.
- Wedge vertebra: A wedge vertebra is a partially formed vertebra that is narrower on one side, contributing to a curve but typically with less severe progression than a hemivertebra.
- Block vertebra: Block vertebrae occur when two or more vertebrae are fused together. While they represent a congenital anomaly, they typically do not cause significant scoliosis because there is no differential growth potential to drive a progressive curve.
Question 28
A 15-year-old male is brought to the emergency department after an ATV accident where the vehicle rolled over multiple times. He reports inability to move or feel his legs. On arrival, his GCS is 15, he has a left wrist deformity, blood pressure 105/68, heart rate 102, respiratory rate 26, and SpO2 98% on room air. He is in a hard cervical collar and appears in no acute distress.
According to Advanced Trauma Life Support (ATLS) principles, what is your immediate next action?
Explanation
Correct Answer: D
The correct answer is evaluation of lungs with a stethoscope. This question tests the fundamental principles of Advanced Trauma Life Support (ATLS). Regardless of other injuries, the primary survey (ABCDEs) must always be completed first. The 'B' in ABCDE stands for Breathing and Ventilation. Auscultating the lungs with a stethoscope is a critical component of assessing breathing and ventilation to ensure adequate air entry and rule out life-threatening conditions such as pneumothorax or hemothorax, which could be present after a high-energy trauma like an ATV rollover.
Option A (Immediate CT scan of cervical, thoracic, and lumbar spine) is incorrect. While imaging of the spine is crucial given the patient's neurological deficit, it comes after the primary survey and stabilization of life-threatening conditions. Imaging is part of the secondary survey.
Option B (Exchange of hard cervical collar for a Miami-J collar) is incorrect. The type of cervical collar is a secondary concern. The priority is to maintain spinal immobilization and assess vital functions, not to change the specific type of collar at this immediate stage.
Option C (Neurosurgical consultation) is incorrect. While a neurosurgical consultation will be necessary, it is not the immediate next action. The orthopedic surgeon (or trauma team leader) must first complete the primary survey and stabilize the patient before initiating specialty consultations.
Option E (Obtain radiographs of the left wrist to evaluate for fracture) is incorrect. Evaluation and management of musculoskeletal injuries like a wrist deformity are part of the secondary survey, after the primary survey has been completed and life-threatening conditions addressed.
Question 29
Following the primary survey, a detailed physical examination of the 15-year-old male reveals sensation is not intact distal to the umbilicus, no sensation around the rectum, and no voluntary rectal tone. He has 5/5 strength in bilateral upper extremities and 0/5 strength in all key muscles of the bilateral lower extremities. When his glans penis is squeezed during a simultaneous digital rectal examination, the muscles surrounding his rectum contract around your finger.
What is the neurophysiological pathway by which the bulbocavernosus reflex (BCR) works?
Explanation
Correct Answer: E
The correct answer is Dorsal penile nerve → afferent pudendal nerve fibers → sacral plexus → efferent pudendal nerve fibers → perineal muscle. The bulbocavernosus reflex (BCR) is a polysynaptic reflex that involves the S2-S4 sacral segments of the spinal cord. The afferent limb of the reflex is carried by the dorsal penile nerve (a branch of the pudendal nerve) to the sacral plexus. The efferent limb, which causes contraction of the bulbocavernosus and external anal sphincter muscles, is carried by the efferent fibers of the pudendal nerve from the sacral plexus to the perineal muscles.
The presence of an intact BCR in a patient with a suspected spinal cord injury is crucial because it indicates that the patient is NOT in spinal shock, and therefore, the neurological deficit observed is likely to be the final deficit. Spinal shock is characterized by a temporary loss of spinal cord function and reflex activity below the level of injury, including an absent BCR.
The other options describe incorrect or partially incorrect pathways involving different nerves (genitofemoral, obturator, ilioinguinal) or an incorrect order of afferent/efferent signaling.
Question 30
Based on the physical examination findings of the 15-year-old male (sensation not intact distal to the umbilicus, no sensation around the rectum, no voluntary rectal tone, 0/5 strength in bilateral lower extremities, and an intact bulbocavernosus reflex), what would be the patient’s classification according to the American Spinal Injury Association (ASIA) impairment scale?
Explanation
Correct Answer: A
The correct answer is ASIA Impairment Scale (AIS) A. The patient presents with complete motor and sensory loss below the level of the umbilicus, including the sacral segments S4-5 (no sensation around the rectum and no voluntary rectal tone). According to the ASIA classification:
- AIS A (Complete): No sensory or motor function is preserved in the sacral segments S4–5. This perfectly matches the patient's presentation.
- AIS B (Sensory incomplete): Sensory but not motor function is preserved below the neurological level and includes the sacral segments S4–5 (light touch or pin prick at S4–5 or deep anal pressure) AND no motor function is preserved more than three levels below the motor level on either side of the body. This patient has no S4-5 sensation.
- AIS C (Motor incomplete): Motor function is preserved below the neurological level, and more than half of key muscle functions below the neurological level of injury (NLI) have a muscle grade less than 3 (Grades 0–2). This patient has no motor function below the NLI.
- AIS D (Motor incomplete): Motor function is preserved below the neurological level, and at least half (half or more) of key muscle functions below the NLI have a muscle grade >3. This patient has no motor function below the NLI.
- AIS E (Normal): If sensation and motor function as tested with the ISNCSCI are graded as normal in all segments, and the patient had prior deficits, then the AIS grade is E. Someone without an initial SCI does not receive an AIS grade. This patient clearly has deficits.
Therefore, the complete absence of sensory and motor function in the sacral segments S4-5 classifies this patient as AIS A.
Question 31
Plain radiographs of the 15-year-old male's spine are obtained following his ATV accident, as shown below. Despite his complete motor and sensory loss below the umbilicus, these radiographs show no evidence of any fractures or displacements.
Given the clinical presentation and the radiographic findings, what is the next step in management to definitively diagnose the patient's condition?
Explanation
Correct Answer: B
The correct answer is to obtain an MRI without contrast of the thoracic and lumbar spine. The patient's clinical picture strongly points toward a spinal cord injury (complete motor and sensory loss), yet the plain radiographs show no evidence of fractures or displacements. This scenario is characteristic of Spinal Cord Injury Without Radiographic Abnormality (SCIWORA). To definitively diagnose SCIWORA and evaluate the spinal cord itself, as well as its surrounding ligaments, an MRI is the gold standard. MRI provides detailed information about soft tissues, including the spinal cord, intervertebral discs, and ligaments, which cannot be adequately visualized on plain radiographs or standard CT scans.
Option A (Obtain a CT scan of the thoracic and lumbar spine) is incorrect. A standard CT scan provides excellent bony detail but offers limited information about the spinal cord itself or ligamentous injuries unless a CT myelogram is performed, which is not the initial diagnostic choice for SCIWORA.
Option C (Obtain bending radiographs to observe for instability of the thoracolumbar spine) is incorrect. Obtaining bending radiographs in a patient with a suspected spinal cord injury and potential instability (even if not visible on static films) is contraindicated and could worsen the neurological deficit. The spine should be kept immobilized until stability is confirmed.
Option D (Obtain electromyogram and nerve conduction studies of the patient’s bilateral lower extremities) is incorrect. EMG and nerve conduction studies are used to evaluate peripheral nerve function and muscle integrity, typically for chronic conditions or specific neuropathies. They are not indicated for the acute diagnosis of a spinal cord injury.
Option E (Administer high-dose corticosteroids immediately) is incorrect. While corticosteroids were historically used for acute spinal cord injury, current evidence does not support their routine use, and they are associated with significant side effects. Their administration is not a diagnostic step.
Question 32
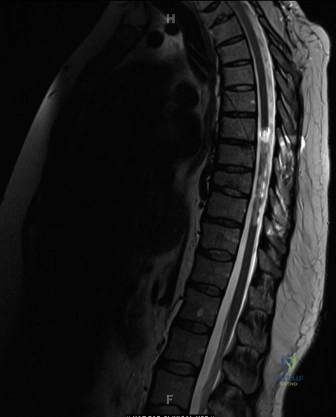
An MRI is obtained for the 15-year-old male with suspected SCIWORA, and a sagittal view is displayed below. The MRI confirms a spinal cord injury without radiographic abnormality.
Given the findings on MRI and the diagnosis of SCIWORA, what is the best predictor of long-term neurologic outcome in this condition?
Explanation
Correct Answer: D
The correct answer is neurologic status at time of presentation. For patients with SCIWORA, the most significant predictor of long-term neurologic outcome is their neurologic status at the time of initial presentation. Patients with complete lesions (like this patient, classified as ASIA A) very rarely improve, while those with incomplete but severe spinal cord lesions may improve but often not to pre-injury levels. The extent of the initial neurological deficit is paramount in determining the prognosis.
It's important to note a nuance mentioned in the case: in the subset of patients with only minor edema or hemorrhage on MRI, the MRI findings themselves have been shown to be a better predictor of long-term outcome than neurologic status at presentation. However, for the general SCIWORA population, and especially for those with significant deficits (as implied by the image showing clear cord signal changes and the patient's ASIA A status), the initial clinical neurological status remains the primary predictor.
Option A (Age at the time of injury) is incorrect. While age can influence recovery potential in some contexts, it is not the best predictor of long-term neurologic outcome in SCIWORA compared to the initial neurologic status.
Option B (Sex) is incorrect. There is no evidence to suggest that sex is a significant predictor of long-term neurologic outcome in SCIWORA.
Option C (Mechanism of injury) is incorrect. While the mechanism of injury (e.g., high-energy trauma) can indicate the potential for severe injury, it is not as direct a predictor of long-term neurologic outcome as the actual neurological deficit observed.
Option E (Socioeconomic status) is incorrect. Socioeconomic status can affect access to rehabilitation and long-term care, but it is not a direct predictor of the inherent neurologic recovery potential after SCIWORA.
Question 33
A 5-year-old child sustains a displaced lateral condyle fracture of the humerus. Which of the following is the most common long-term complication if this fracture goes on to a delayed union or nonunion?
Explanation
Question 34
When utilizing the Ponseti method for the correction of idiopathic clubfoot, what is the first deformity that must be addressed during the casting sequence?
Explanation
Question 35
A 24-year-old male sustains a proximal pole scaphoid fracture. Operative fixation is planned. Which of the following describes the most appropriate surgical approach and rationale?
Explanation
Question 36
During a fasciectomy for severe Dupuytren's contracture, the surgeon dissects out the spiral cord. The spiral cord displaces the neurovascular bundle in which direction?
Explanation
Question 37
A 12-year-old is involved in a high-speed motor vehicle collision while wearing a lap-belt only. Radiographs reveal a bony Chance fracture of L2. Which of the following associated injuries has the highest incidence in this patient?
Explanation
Question 38
A 35-year-old male presents with severe neck pain and right upper extremity weakness following a diving accident. Imaging reveals a right-sided unilateral facet dislocation at C5-C6. Which of the following neurological deficits is most likely present?
Explanation
Question 39
A 6-month-old female with developmental dysplasia of the hip (DDH) has failed 6 weeks of treatment in a Pavlik harness, with persistent dislocation of the left hip. What is the most appropriate next step in management?
Explanation
Question 40
A 42-year-old carpenter presents with the inability to make an "A-OK" sign with his right hand, instead demonstrating a flattened pinch. Sensation in the hand is completely normal. Compression of which of the following nerves is the most likely cause?
Explanation
Question 41
An 84-year-old male with severe baseline COPD sustains a Type II odontoid fracture after a ground-level fall. He is neurologically intact. Which of the following treatments provides the lowest morbidity and mortality for this specific patient?
Explanation
Question 42
A 14-year-old male sustains an isolated juvenile Tillaux fracture of the right ankle. Which of the following ligaments is responsible for avulsing the fracture fragment?
Explanation
Question 43
A 28-year-old skier presents with a painful, swollen thumb after falling on an outstretched hand with the pole in his palm. MRI confirms a complete rupture of the ulnar collateral ligament (UCL) of the thumb MCP joint with a Stener lesion. What anatomical structure is interposed in a Stener lesion?
Explanation
Question 44
A 70-year-old male with pre-existing cervical spondylosis presents after a hyperextension injury. He exhibits marked motor weakness in his upper extremities, particularly his hands, with relative sparing of his lower extremities. What is the most likely diagnosis?
Explanation
Question 45
A 12-year-old obese boy presents with acute left groin pain and an inability to bear weight after a minor twisting injury. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Which of the following defines this as an "unstable" SCFE?
Explanation
Question 46
During a Zone II flexor tendon repair, the surgeon adds a running epitendinous suture to the core suture construct. What is the primary biomechanical benefit of adding this epitendinous suture?
Explanation
Question 47
A 25-year-old female presents after a fall from 10 feet. CT reveals an L1 burst fracture with 15 degrees of focal kyphosis and 30% canal compromise. She has normal neurological function, and MRI confirms the posterior ligamentous complex (PLC) is completely intact. According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the most appropriate management?
Explanation
Question 48
A 6-year-old boy is diagnosed with Legg-Calvé-Perthes disease. According to the modified lateral pillar classification (Herring), which of the following radiographic findings indicates the worst prognosis (Group C)?
Explanation
Question 49
A newborn is evaluated for a unilateral absent thumb and marked radial deviation of the wrist. Radiographs confirm radial longitudinal deficiency (radial clubhand). Which of the following tests is most critical to perform before any surgical intervention?
Explanation
Question 50
A 22-year-old male presents with tetraplegia following a C5 burst fracture. He is flaccid, areflexic, and lacks perianal sensation. Which of the following clinical signs marks the end of the spinal shock phase?
Explanation
Question 51
A 3-year-old child weighing 14 kg sustains an isolated, closed, diaphyseal spiral fracture of the femur after a twisting fall. What is the gold standard initial treatment?
Explanation
Question 52
According to the Mayfield progressive stages of perilunate instability, what is the final stage (Stage IV) of the injury progression?
Explanation
Question 53
A 13-year-old male with a BMI of 35 presents with chronic left knee pain and an obligate external rotation of the hip during active flexion. An AP pelvis radiograph confirms a stable slipped capital femoral epiphysis (SCFE). Which of the following describes the most appropriate surgical intervention?
Explanation
Question 54
A 24-year-old male falls on an outstretched hand and sustains a fracture through the proximal pole of the scaphoid. This region of the scaphoid is at the highest risk for avascular necrosis due to its blood supply. Which artery provides the primary vascular contribution to the proximal pole?
Explanation
Question 55
A 30-year-old male falls from a ladder, sustaining an L1 burst fracture. CT shows 40% canal compromise. He is neurologically intact. MRI demonstrates an intact posterior ligamentous complex (PLC). According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the most appropriate management?
Explanation
Question 56
A 7-month-old female is referred for a persistently dislocated left hip after 6 weeks of unsuccessful Pavlik harness treatment. Radiographs confirm a laterally displaced and superiorly migrated proximal femur. What is the most appropriate next step in management?
Explanation
Question 57
A 22-year-old rugby player presents with an inability to actively flex the DIP joint of his right ring finger after a tackle. Radiographs reveal a large bony avulsion fragment at the volar base of the distal phalanx that is retracted to the level of the DIP joint. What is the Leddy-Packer classification and optimal timing for repair?
Explanation
Question 58
An 80-year-old female sustains a low-energy fall from a standing height. CT of the cervical spine reveals a Type II odontoid fracture with 2 mm of posterior displacement. She is neurologically intact. Which of the following is the most appropriate initial management?
Explanation
Question 59
A 6-year-old male is diagnosed with Legg-Calve-Perthes disease. Radiographs show involvement of the entire epiphysis, but the lateral pillar maintains greater than 50% of its height. Which of the following is the most important prognostic factor for the development of late degenerative joint disease in this patient?
Explanation
Question 60
A 5-year-old boy falls and sustains a lateral condyle humerus fracture. Radiographs reveal 3 mm of displacement of the fracture fragment. What is the most appropriate management?
Explanation
Question 61
A 25-year-old rugby player presents with an inability to actively flex the distal interphalangeal (DIP) joint of his ring finger. Palpation reveals a tender mass in the palm. Radiographs are negative. Within what time frame must surgical intervention be performed to allow for direct repair of the tendon to the distal phalanx?
Explanation
Question 62
A 30-year-old male is brought in obtunded following a severe motor vehicle collision. CT of the cervical spine demonstrates a right-sided unilateral C5-C6 facet dislocation. What is the most appropriate next step in management of the cervical spine injury?
Explanation
Question 63
An infant is brought to the clinic for management of idiopathic clubfoot. According to the Ponseti method, the initial serial casting should primarily aim to correct which of the following deformities?
Explanation
Question 64
A 45-year-old male presents with chronic wrist pain and a history of a remote scaphoid fracture. Radiographs demonstrate a scaphoid nonunion with radioscaphoid arthritis, but the capitolunate joint is spared. Which of the following is the most appropriate surgical treatment?
Explanation
Question 65
A 22-year-old male falls from a height and sustains an L1 burst fracture. He is neurologically intact. MRI demonstrates definitive rupture of the posterior ligamentous complex (PLC). According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is his total score and recommended management?
Explanation
Question 66
A 13-year-old obese male presents with a 4-week history of left knee pain and a limp. On examination, flexion of the left hip results in obligate external rotation. Radiographs confirm a slipped capital femoral epiphysis (SCFE). The slippage occurs through which zone of the physis?
Explanation
Question 67
During a ligament reconstruction and tendon interposition (LRTI) procedure for thumb carpometacarpal (CMC) arthritis, the flexor carpi radialis (FCR) tendon is commonly utilized. The primary goal of the ligament reconstruction portion of this procedure is to recreate the function of which of the following ligaments?
Explanation
Question 68
An 82-year-old female presents with severe neck pain following a ground-level fall. Imaging reveals a Type II odontoid fracture with 3 mm of posterior displacement. She is neurologically intact but has severe medical comorbidities (ASA class IV). What is the most appropriate management?
Explanation
Question 69
A 14-year-old male sustains an ankle injury while skateboarding. Radiographs demonstrate a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis (Tillaux fracture). Which of the following ligaments is responsible for the avulsion of this fracture fragment?
Explanation
Question 70
A 65-year-old female presents with severe, long-standing carpal tunnel syndrome and marked thenar atrophy. Which of the following muscles is most likely atrophied, reflecting profound median nerve denervation?
Explanation
Question 71
A 65-year-old male with underlying cervical spondylosis sustains a hyperextension injury to his neck in a rear-end collision. He presents with profound bilateral upper extremity motor weakness but retains ability to move his legs. What is the most likely pathological mechanism of this specific spinal cord injury syndrome?
Explanation
Question 72
A 6-year-old boy is diagnosed with Legg-Calve-Perthes disease. Radiographs reveal fragmentation of the femoral head with the lateral pillar maintaining 60% of its original height. According to the Herring Lateral Pillar Classification, what is the classification and typical prognosis?
Explanation
Question 73
A 12-month-old infant is brought in for surgical evaluation of simple, complete syndactyly of the long and ring fingers. When planning the surgical release, what is the primary reconstructive technique utilized to create the new web space and prevent web creep?
Explanation
Question 74
A 13-year-old obese male presents with acute left groin pain and an inability to bear weight on the affected extremity, even with the use of crutches. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Which of the following factors most strongly predicts the development of avascular necrosis (AVN) in this patient?
Explanation
Question 75
A 28-year-old carpenter sustains a deep laceration to the volar aspect of his index finger in Zone II. During surgical exploration and repair of the flexor digitorum profundus (FDP) and superficialis (FDS) tendons, maintaining the integrity of the flexor pulley system is critical. Which of the following pulley combinations is most essential to preserve in order to prevent bowstringing of the flexor tendons?
Explanation
Question 76
An 82-year-old male with a history of COPD and osteoporosis sustains a Type II odontoid fracture after a ground-level fall. He complains of severe neck pain but remains neurologically intact. When considering treatment, which of the following management options is associated with the highest risk of mortality and severe complications in this specific patient demographic?
Explanation
Question 77
A 6-week-old female is currently being treated with a Pavlik harness for developmental dysplasia of the hip (DDH). The parents bring her to the clinic noting a decrease in spontaneous movement of the affected leg over the past two days. On examination, the infant lacks active knee extension, though ankle and toe movements are normal. What is the most likely cause of this clinical finding?
Explanation
Question 78
A 16-year-old male is brought to the emergency department after a high-speed motor vehicle collision where he was a restrained rear-seat passenger wearing a lap belt. Radiographs and CT imaging reveal a flexion-distraction injury of the lumbar spine (Chance fracture).
Which of the following associated injuries must be most aggressively ruled out in this patient?
Explanation
Question 79
A 24-year-old male presents with radial-sided wrist pain after a fall on an outstretched hand. Imaging confirms a displaced proximal pole fracture of the scaphoid. What anatomical characteristic of the scaphoid's blood supply places the proximal pole at the highest risk for avascular necrosis (AVN)?
Explanation
Question 80
A 5-year-old child sustains a displaced lateral condyle fracture of the humerus that goes unrecognized for 6 weeks, resulting in an established nonunion. If left untreated into adulthood, what is the most likely long-term complication associated with this specific nonunion?
Explanation
Question 81
A 65-year-old male with pre-existing cervical spondylotic stenosis falls forward and strikes his chin on a table, sustaining a severe hyperextension injury to his neck. He arrives at the trauma bay with significant bilateral motor weakness that is noticeably more profound in his upper extremities than his lower extremities, particularly affecting his hands. Proprioception and perianal sensation remain largely intact. What is the most likely diagnosis?
Explanation
None
