ABOS Part I & AAOS OITE Orthopedic Surgery Review: Knee ACL, Meniscus, & Hand Flexor Tendon Repair | Part 22221
Key Takeaway
This ABOS Part I & AAOS OITE orthopedic review module covers critical topics in knee and hand surgery. It details ACL reconstruction, meniscal repair, and flexor tendon repair, including surgical techniques, graft choices, rehabilitation protocols, and management of complications. It's designed for comprehensive exam preparation.
ABOS Part I & AAOS OITE Orthopedic Surgery Review: Knee ACL, Meniscus, & Hand Flexor Tendon Repair | Part 22221
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 22-year-old collegiate soccer player presents with acute right knee pain and instability after a non-contact pivoting injury. Clinical examination reveals a Grade III Lachman test, a high-grade pivot shift, and mild gapping with valgus stress at 30 degrees of flexion. Plain radiographs show a subtle avulsion fracture from the lateral aspect of the proximal tibia. Which of the following statements best describes the significance of the radiographic finding and its associated injury?
Explanation
Correct Answer: B
The case explicitly states that a subtle, small elliptic avulsion fracture arising from the lateral aspect of the proximal tibia, just distal to the articular surface, was identified on plain radiographs. This finding is known as a Segond fracture. It represents an avulsion of the anterolateral capsule and anterolateral ligament (ALL) and is considered pathognomonic for an anterior cruciate ligament (ACL) tear. Its presence indicates a higher degree of anterolateral rotatory instability, which aligns with the clinical finding of a high-grade pivot shift.
- Option A is incorrect because a Segond fracture is pathognomonic for an ACL rupture, not a PCL rupture, and indicates anterolateral, not posterolateral, instability.
- Option C is incorrect because an arcuate fracture involves the fibular head and is associated with avulsion of the fibular collateral ligament or popliteus tendon, indicating posterolateral corner injury, which is distinct from the described lateral tibial plateau avulsion.
- Option D is incorrect because a tibial spine avulsion fracture involves the intercondylar eminence of the tibia and is a different type of bony ACL injury, not the lateral tibial plateau avulsion described.
- Option E is incorrect because while it is a fracture of the lateral tibial plateau region, its specific morphology (avulsion) and location are characteristic of a Segond fracture, which is strongly associated with rotational and valgus mechanisms leading to ACL injury, rather than a direct impact.
Question 2
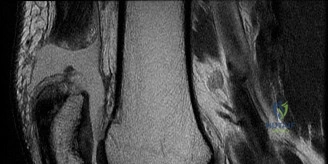
Following the initial clinical assessment, an MRI of the right knee was obtained. Review the provided sagittal T2-weighted image.
Which of the following findings is most accurately depicted in this image and is consistent with the patient's presentation?
Explanation
Correct Answer: C
The provided sagittal T2-weighted MRI image, combined with the case description, clearly demonstrates a complete rupture of the anterior cruciate ligament (ACL). The ligament fibers are discontinuous, edematous, and appear amorphous, consistent with the 'empty notch sign' mentioned in the text. Furthermore, the image shows areas of hyperintensity (bone bruising) in the middle portion of the lateral femoral condyle and the posterior aspect of the lateral tibial plateau, which are characteristic osteochondral impaction injuries resulting from the pivot-shift mechanism. This aligns perfectly with the patient's mechanism of injury and clinical findings.
- Option A is incorrect because the case explicitly states that the posterior drawer test and posterior sag sign were negative, confirming an intact posterior cruciate ligament (PCL). The image does not show PCL rupture.
- Option B is incorrect because the case states the lateral meniscus appeared intact, and the medial meniscus had a longitudinal vertical tear in the posterior horn, not a bucket-handle tear of the lateral meniscus.
- Option D is incorrect because the case describes a Grade I to II sprain of the superficial medial collateral ligament (sMCL), not a Grade III sprain with significant gapping. While MCL injury is present, this option overstates its severity and is not the primary finding highlighted by the image in the context of the ACL rupture.
- Option E is incorrect because the case states no gross fractures of the patella were identified on X-rays, and the MRI primarily shows ACL rupture and bone bruising, not a patellar osteochondral fracture.
Question 3
Given the patient's age, activity level, and the presence of a high-grade pivot shift with a Segond fracture, the surgical team decided to augment the intra-articular ACL reconstruction with a Lateral Extra-articular Tenodesis (LET). Which of the following best describes the technique for the modified Lemaire LET performed in this case?
Explanation
Correct Answer: B
The case explicitly details the technique for the modified Lemaire lateral extra-articular tenodesis: 'A 1-centimeter wide by 8-centimeter long strip of the posterior third of the iliotibial band was harvested, leaving its distal attachment at Gerdy's tubercle intact. The proximal end was whipstitched. The femoral attachment site was identified slightly proximal and posterior to the lateral epicondyle. A guide pin was placed, and a small socket was drilled. The iliotibial band strip was passed deep to the fibular collateral ligament. With the knee held in 30 degrees of flexion and neutral rotation, the graft was tensioned and secured into the femoral socket using a 6-millimeter bioabsorbable interference screw.'
- Option A is incorrect as it describes using the semitendinosus and an incorrect fixation pattern for a Lemaire.
- Option C is incorrect as it describes a more extensive and less common ITB tenodesis, not the modified Lemaire.
- Option D is incorrect as it describes an ALL reconstruction using a synthetic graft, which is not what was performed in this case.
- Option E is incorrect as it describes using the biceps femoris tendon and an incorrect passage relative to the LCL.
Question 4
The patient's postoperative rehabilitation protocol includes specific restrictions due to the combined ACL reconstruction and meniscal repair. In Phase I (Weeks 0 to 4), what is the most critical initial weight-bearing and range of motion restriction, and what is its primary rationale?
Explanation
Correct Answer: C
The case explicitly states the Phase I rehabilitation goals: 'The primary goals in the immediate postoperative phase are to control inflammation, protect the graft and meniscal repair, and restore terminal extension.' It further specifies: 'Due to the all-inside repair of the posterior horn of the medial meniscus, weight-bearing was restricted. The patient was allowed touch-down weight-bearing with crutches with the brace locked in full extension. Passive and active-assisted range of motion was initiated early but restricted to 0 to 90 degrees for the first four weeks to prevent excessive shear stress on the healing meniscus.' The primary rationale for these restrictions is to protect the delicate meniscal repair during its initial healing phase, as excessive load or motion can disrupt the repair.
- Option A is incorrect because full weight-bearing is contraindicated with a meniscal repair in the early phase.
- Option B is incorrect because unrestricted range of motion would jeopardize the meniscal repair.
- Option D is incorrect because full weight-bearing and an unlocked brace are too aggressive for the initial phase of a meniscal repair.
- Option E is incorrect because locking the brace at 30 degrees of flexion would promote a flexion contracture and is not standard for ACL/meniscal repair. The ROM restriction is also not optimal.
Question 5
The patient's primary goal is to return to elite-level competitive soccer. Considering his age, activity level, and the presence of a repairable medial meniscal tear, what was the most appropriate graft choice for his ACL reconstruction, and what is its key advantage in this scenario?
Explanation
Correct Answer: C
The case clearly states: 'The decision was made to proceed with a Bone-Patellar Tendon-Bone (BTB) autograft. The BTB autograft is often considered the gold standard for high-demand cutting athletes. Its primary biomechanical advantage lies in the rigid bone-to-bone healing within the femoral and tibial tunnels, which allows for faster incorporation (typically 6 to 8 weeks) compared to soft tissue healing (10 to 12 weeks). Furthermore, the structural properties of the central third of the patellar tendon closely match those of the native anterior cruciate ligament.'
- Option A is incorrect because while hamstring autografts have less anterior knee pain, the case notes they 'have been associated with a slightly higher rate of graft elongation and residual laxity in elite athletes,' making BTB preferred for this high-demand patient.
- Option B is incorrect because the case explicitly states: 'For a young, elite collegiate soccer player, allograft tissue is generally contraindicated due to significantly higher failure rates (up to three to four times higher) compared to autografts in the under-25 demographic.'
- Option D is incorrect because while quadriceps tendon is a good alternative, BTB was specifically chosen in this case due to the surgeon's experience and robust outcomes in elite soccer players.
- Option E is incorrect because synthetic grafts are generally not recommended for primary ACL reconstruction due to high failure rates and concerns about synovitis and long-term outcomes.
Question 6
During the arthroscopic portion of the surgery, the medial meniscus was addressed. Review the provided arthroscopic image.
Based on the image and the case description, what type of meniscal tear was identified, and what repair technique was utilized?
Explanation
Correct Answer: D
The case description states: 'Attention was turned to the medial meniscus. Probing confirmed a 1.5-centimeter longitudinal vertical tear in the posterior horn, situated in the vascularized red-white zone. The tear was unstable, easily displacing anteriorly into the joint space. An all-inside meniscal repair technique was selected. The meniscal edges and the adjacent synovium were aggressively rasped using an arthroscopic rasp and shaver to stimulate a bleeding bed and promote a healing response. Two all-inside meniscal repair devices (suture anchors) were deployed sequentially, capturing the superior and inferior leaflets of the meniscus and reducing the tear anatomically.'
- Option A is incorrect because the tear was in the medial meniscus, not lateral, and was repaired, not partially meniscectomized.
- Option B is incorrect because it was a longitudinal vertical tear, not a horizontal cleavage tear, and an all-inside technique was used.
- Option C is incorrect because it was a longitudinal vertical tear, not described as complex, and not a root tear.
- Option E is incorrect because it was a longitudinal vertical tear, not a bucket-handle tear, and an all-inside technique was used.
Question 7
The timing of ACL reconstruction is crucial to optimize outcomes and minimize complications. In this case, surgery was scheduled for four weeks post-injury. What was the primary rationale for delaying the surgical intervention, and how was the concomitant Grade II MCL sprain managed during this period?
Explanation
Correct Answer: B
The case explicitly addresses the timing of surgery: 'Historically, acute reconstruction within the first few days of injury was associated with a high incidence of postoperative joint stiffness. Current evidence-based protocols advocate for a period of "pre-habilitation." The patient was placed in a hinged knee brace and initiated on a strict physical therapy regimen aimed at resolving the acute effusion, restoring normal gait mechanics, and achieving full, symmetric range of motion, particularly terminal extension. Surgery was scheduled for four weeks post-injury, at which point his knee was quiet, the effusion had resolved, and he had regained full extension and 125 degrees of flexion. The concomitant Grade II medial collateral ligament sprain was managed non-operatively during this waiting period. Grade I and II medial collateral ligament injuries have excellent healing potential with bracing and rarely require surgical intervention, even in the setting of anterior cruciate ligament reconstruction.'
- Option A is incorrect because spontaneous healing of a complete ACL rupture is rare, and the goal was pre-habilitation, not avoiding surgery.
- Option C is incorrect because Grade I/II MCL sprains are typically managed non-operatively, not with staged surgical repair.
- Option D is incorrect because while effusion resolution is a goal, full weight-bearing is not necessarily achieved or required before surgery, especially with a meniscal tear.
- Option E is incorrect because additional imaging was not the primary reason for delay, and the MCL was managed non-operatively.
Question 8
During the surgical procedure, anatomic femoral tunnel placement is critical for successful ACL reconstruction. Which of the following describes the approach and key anatomical landmark used for femoral tunnel creation in this case?
Explanation
Correct Answer: B
The case details the femoral tunnel preparation: 'To achieve independent and anatomic femoral tunnel placement, an accessory anteromedial portal was utilized. The knee was hyperflexed to 120 degrees. A guide pin was placed in the center of the native footprint on the medial wall of the lateral femoral condyle, specifically mentioning the lateral bifurcate ridge and the lateral intercondylar ridge (resident's ridge) as landmarks. A 10-millimeter reamer was used to drill the femoral socket to a depth of 25 millimeters.'
- Option A is incorrect because transtibial drilling often leads to a more vertical femoral tunnel, which is non-anatomic and can compromise rotational stability. The case specifies an accessory anteromedial portal.
- Option C is incorrect because the femoral tunnel is placed on the lateral femoral condyle for ACL reconstruction, not the medial.
- Option D is incorrect because the anterolateral portal is typically used for visualization, and the knee is hyperflexed for anatomic femoral tunnel drilling, not full extension.
- Option E is incorrect because the posteromedial portal is used for posterior compartment pathology or PCL reconstruction, not ACL femoral tunnel placement.
Question 9
A 22-year-old collegiate soccer player presents with acute right knee pain, swelling, and instability following a non-contact pivoting injury. Clinical examination reveals a Grade III Lachman test, a high-grade pivot shift, and mild gapping with valgus stress at 30 degrees of flexion. MRI confirms a complete ACL rupture, a Grade II MCL sprain, and a repairable medial meniscal tear. Which of the following statements regarding the management of the concomitant Grade II MCL sprain is most accurate in this clinical scenario?
Explanation
Correct Answer: B
The case explicitly states: 'The concomitant Grade II medial collateral ligament sprain was managed non-operatively during this waiting period. Grade I and II medial collateral ligament injuries have excellent healing potential with bracing and rarely require surgical intervention, even in the setting of anterior cruciate ligament reconstruction.' This is a well-established principle in orthopedic sports medicine.
- Option A is incorrect because Grade I and II MCL sprains rarely require surgical repair.
- Option C is incorrect because surgical reconstruction with allograft is not indicated for a Grade II MCL sprain.
- Option D is incorrect because a Grade II MCL sprain is not a contraindication to ACL reconstruction, though timing may be influenced by associated injuries. The patient was allowed touch-down weight-bearing, not prolonged non-weight-bearing.
- Option E is incorrect because while a hinged brace is used, locking it at 30 degrees of flexion is not standard for MCL healing and would promote a flexion contracture. The brace was locked in full extension for ambulation in this case.
Question 10
The patient's clinical presentation, including a high-grade pivot shift and a Segond fracture, strongly suggested profound anterolateral rotatory instability. This finding significantly influenced the surgical decision-making process. What is the primary rationale for adding a Lateral Extra-articular Tenodesis (LET) to the primary ACL reconstruction in this specific patient?
Explanation
Correct Answer: C
The case clearly states the rationale for adding a LET: 'Given the presence of a high-grade pivot shift and a radiographic Segond fracture indicating anterolateral complex injury, the addition of a Lateral Extra-articular Tenodesis (LET) or Anterolateral Ligament (ALL) reconstruction was strongly considered. Recent biomechanical and clinical outcome studies, including the STABILITY trial, have demonstrated that adding a LET to a primary anterior cruciate ligament reconstruction in young, high-risk patients significantly reduces the risk of graft rupture and persistent rotatory laxity.'
- Option A is incorrect because LET primarily addresses anterolateral rotatory instability, not posterior tibial translation (which is related to PCL function).
- Option B is incorrect because LET is for rotatory knee instability, not patellar instability. The case also states no evidence of patellar apprehension or instability.
- Option D is incorrect because LET addresses lateral-sided rotatory instability, not medial collateral ligament healing or valgus instability.
- Option E is incorrect because LET is a ligamentous procedure, not directly for meniscal tears. The lateral meniscus was intact in this patient.
Question 11
The patient's history includes a sudden deceleration with a pivoting motion on a planted foot, followed by a valgus collapse of the knee, and he reported hearing a distinct 'pop.' This mechanism is highly characteristic of an ACL rupture. Which of the following statements accurately describes the biomechanical cascade leading to this injury?
Explanation
Correct Answer: B
The case provides a detailed description of the biomechanical cascade: 'The biomechanical cascade typically involves the athlete attempting to change direction rapidly. The foot becomes fixed to the playing surface... As the athlete decelerates and internally rotates the femur over a fixed, externally rotated tibia, a significant valgus moment is applied to the knee joint. This complex loading pattern overwhelms the tensile capacity of the anterior cruciate ligament, often resulting in mid-substance rupture...'
- Option A is incorrect because it describes external rotation of the femur over an internally rotated tibia and a varus moment, which is not the classic ACL mechanism described.
- Option C is incorrect because a direct blow causing hyperextension is a different mechanism, often associated with PCL or multiligamentous injuries, but not the primary non-contact pivoting mechanism.
- Option D is incorrect because a fall onto a flexed knee with the foot plantarflexed is the classic mechanism for a posterior cruciate ligament (PCL) injury.
- Option E is incorrect because this describes a degenerative process, whereas the patient experienced an acute, traumatic injury.
Question 12
A 28-year-old right-hand dominant carpenter sustains a laceration to his left ring finger while using a power saw. On examination, he is unable to actively flex his DIP joint, and his PIP joint flexion is significantly weakened compared to his uninjured digits. Sensation is intact. Radiographs show no bony injury. He is scheduled for surgical repair within 24 hours. Based on the provided case information, which of the following statements regarding his injury and initial management is MOST accurate?
Explanation
Correct Answer: C
Explanation:
The patient's inability to actively flex the DIP joint indicates a laceration of the Flexor Digitorum Profundus (FDP) tendon, as the FDP is solely responsible for DIP flexion. Weakened PIP joint flexion, despite some residual motion, suggests involvement of the Flexor Digitorum Superficialis (FDS) tendon, which is the primary flexor of the PIP joint. The ring finger is a common site for flexor tendon injuries. Given both FDP and FDS involvement, the injury is most likely in Zone II (from the A1 pulley to the FDS insertion), also known as "No Man's Land."
- Option C is correct: The case explicitly states that the A2 and A4 pulleys are considered biomechanically most critical for maintaining function, and their disruption can lead to significant bowstringing. It also notes that in Zone II, if both FDS and FDP are lacerated, repair of both tendons is generally recommended, especially if more than 50% of the FDS slips are involved, provided it does not add significant bulk.
- Option A is incorrect: Zone I involves only the FDP, distal to the FDS insertion. Since both FDS and FDP appear to be involved (DIP and PIP flexion deficits), the injury is more consistent with Zone II.
- Option B is incorrect: While preventing rerupture is a goal, the case emphasizes that post-operative rehabilitation involves controlled motion protocols (e.g., Duran, Kleinert, or Early Active Motion) to minimize adhesion formation, not strict immobilization for 6 weeks, which would lead to severe stiffness.
- Option D is incorrect: The case states that the typical critical threshold for a secure repair, allowing early active mobilization protocols, is considered to be greater than 45-50 Newtons (N) of tensile strength. 20 N is insufficient for early active motion.
- Option E is incorrect: The Brunner zig-zag incision is described as the most common and preferred approach for flexor tendon repairs in the digits because it crosses flexion creases obliquely, preventing scar contracture, and allows adequate exposure while protecting neurovascular structures with careful dissection. It is not contraindicated.
Question 13
A 35-year-old construction worker presents to the emergency department 4 weeks after sustaining a deep laceration to his dominant index finger. He initially delayed seeking medical attention due to personal reasons. On examination, he has a complete loss of active flexion at both the PIP and DIP joints of the index finger. The wound is clean and well-healed. Passive range of motion is significantly limited due to stiffness. Based on the case, what is the MOST appropriate management strategy for this patient?
Explanation
Correct Answer: C
Explanation:
The patient presents 4 weeks post-injury with complete loss of active flexion and significant passive stiffness. The case states that "Prolonged Delay: Beyond 3-4 weeks, significant tendon retraction, muscle contracture, and fibrosis can make primary repair impossible without excessive tension. Tendon grafting or two-stage reconstruction using a Hunter rod (silastic implant) may be necessary."
- Option C is correct: Given the 4-week delay and likely significant tendon retraction and fibrosis, a primary repair is unlikely to be feasible without excessive tension, which would lead to repair failure. A staged flexor tendon reconstruction using a Hunter rod (silastic implant) is the most appropriate approach for chronic tears with significant retraction and fibrosis, as outlined in the Indications & Contraindications table.
- Option A is incorrect: Immediate primary repair is indicated for acute lacerations (within 7-10 days, or up to 3 weeks for delayed primary repair). At 4 weeks, the conditions for primary repair are typically no longer met.
- Option B is incorrect: Delayed primary repair is generally feasible up to 3 weeks. Beyond this, the challenges of retraction and fibrosis make it less viable.
- Option D is incorrect: While hand therapy is crucial post-operatively, it cannot restore tendon continuity. Attempting aggressive passive range of motion without addressing the tendon laceration would be ineffective and potentially harmful.
- Option E is incorrect: Excision of the A2 and A4 pulleys is generally avoided as they are critical for preventing bowstringing. While some pulley incision may be necessary for access during acute repair, complete excision is not a standard approach, especially not to facilitate a repair that is already likely contraindicated due to delay.
Question 14
A 50-year-old patient undergoes flexor tendon repair in Zone II of the middle finger. Intraoperatively, the surgeon notes that both the FDS and FDP tendons are completely lacerated. After meticulous repair of both tendons, the surgeon is concerned about potential bulk at the repair site compromising gliding. According to the case, which of the following is a valid consideration in this specific scenario?
Explanation
Correct Answer: B
Explanation:
The case discusses specific considerations for Zone II injuries, particularly regarding FDS repair when both tendons are lacerated. It states: "If both FDS and FDP are lacerated, repair of both tendons is generally recommended, especially if more than 50% of the FDS slips are involved. However, if the FDS repair adds significant bulk or impedes FDP gliding, one slip of the FDS can be excised to reduce bulk, or in some cases, the FDS may be excised entirely if the FDP is fully functional and its gliding needs to be prioritized. Current evidence often favors repair of both if technically feasible without excessive bulk."
- Option B is correct: This option directly aligns with the case's guidance for managing bulk in Zone II when both FDS and FDP are lacerated. Excising one slip of the FDS can reduce bulk while still providing some FDS function.
- Option A is incorrect: Excising the FDP entirely would result in a complete loss of DIP flexion, which is a critical function. The case suggests FDS excision if FDP gliding needs to be prioritized, not FDP excision.
- Option C is incorrect: Tenodesis of FDS to FDP is not a standard primary repair technique described in the case for acute lacerations.
- Option D is incorrect: Leaving both tendons unrepaired is not an appropriate primary management strategy for acute lacerations. A staged reconstruction is reserved for chronic cases or failed primary repairs.
- Option E is incorrect: The case strongly emphasizes the preservation of A2 and A4 pulleys due to their biomechanical importance. Complete excision would lead to significant bowstringing and loss of mechanical advantage, which is a major complication.
Question 15
A 42-year-old chef undergoes repair of a complete flexor digitorum profundus (FDP) laceration in Zone I of his small finger. Post-operatively, he is placed in a dorsal blocking splint and begins a controlled passive motion (Duran) protocol. Which of the following statements accurately describes a key principle or characteristic of the Duran protocol as outlined in the case?
Explanation
Correct Answer: C
Explanation:
The case provides a clear description of the Duran protocol under the "Post-Operative Rehabilitation Protocols" section.
- Option C is correct: The case states: "Duran Protocol (Controlled Passive Motion): Description: Passive flexion and extension of the DIP and PIP joints within the limits of the dorsal blocking splint, typically 10 repetitions, 4-5 times per day. The patient uses the uninjured hand to passively flex and extend the injured digit's IP joints. No active muscle contraction of the repaired tendon."
- Option A is incorrect: This describes a key feature of the Kleinert protocol, not Duran.
- Option B is incorrect: The Duran protocol is a controlled passive motion protocol, meaning there is "No active muscle contraction of the repaired tendon." Active contraction is characteristic of Early Active Motion protocols.
- Option D is incorrect: The case notes that Early Active Motion (EAM) protocols historically had slightly higher rerupture rates, but modern EAM protocols, when applied to adequately strong repairs, show comparable rerupture rates to passive protocols. Duran, being a passive protocol, is generally considered to have a lower immediate rerupture risk compared to early active protocols, though it carries a higher risk of stiffness if not performed diligently.
- Option E is incorrect: The protective phase, which includes the Duran protocol, aims to protect the repair and minimize adhesions. Full active range of motion is a gradual process achieved over weeks to months, not within the first week.
Question 16
A 22-year-old college athlete sustains a complete laceration of the FDP tendon in Zone I of his long finger. During surgical repair, the surgeon plans to use a multi-strand core suture technique to maximize tensile strength and allow for early active mobilization. Which of the following core suture techniques, as described in the case, is known for providing high tensile strength and resistance to gapping, often favored for early active motion protocols?

Explanation
Correct Answer: C
Explanation:
The question asks about core suture techniques known for high tensile strength, suitable for early active motion. The provided image also depicts a multi-strand core suture repair.
- Option C is correct: The case explicitly states under "Core Suture Techniques" that "Doble-Modified Kessler (4-strand): Two modified Kessler sutures placed 90 degrees apart. This significantly increases strength." It also mentions that modern techniques typically involve 4- to 6-strand repairs, and that a 4- to 6-strand core suture combined with an epitendinous repair is a prerequisite for successful early active motion protocols, achieving strengths of 45-70 N.
- Option A is incorrect: The Modified Kessler (2-strand) is described as "Historically popular, but often insufficient for early active motion without significant gapping."
- Option B is incorrect: The Pennington (2-strand) is also described as a 2-strand technique with "similar limitations" to the modified Kessler.
- Option D is incorrect: An epitendinous suture is applied after the core suture and primarily smooths the repair site and adds 10-50% to tensile strength, but it is not the primary core suture responsible for the majority of tensile strength.
- Option E is incorrect: A single horizontal mattress suture is a basic suture pattern and would not provide the multi-strand strength required for early active motion protocols.
Question 17
A 60-year-old diabetic patient undergoes flexor tendon repair of the ring finger. Three weeks post-operatively, he presents with increasing pain, swelling, redness, and purulent discharge from the surgical site. He also has limited active and passive range of motion. Based on the case, what is the MOST appropriate initial management for this complication?
Explanation
Correct Answer: C
Explanation:
The patient's symptoms (increasing pain, swelling, redness, purulent discharge) are classic signs of a deep surgical site infection. The case addresses "Infection" as a complication.
- Option C is correct: The case states under "Complications & Management" for deep/purulent infection: "Surgical debridement, IV antibiotics, wound culture, possible tendon debridement/excision (leading to reconstruction)." This aggressive approach is necessary to control the infection and prevent further damage to the tendon and surrounding tissues.
- Option A is incorrect: Aggressive hand therapy would be contraindicated in the presence of an active infection, as it could worsen inflammation, spread the infection, and potentially lead to rerupture due to compromised tissue strength.
- Option B is incorrect: While antibiotics are necessary, oral antibiotics alone are often insufficient for deep or purulent infections following tendon repair. Surgical debridement is crucial to remove infected tissue and foreign material (suture).
- Option D is incorrect: While rerupture is a possible complication, the primary signs here point to infection. Re-repairing an infected tendon is highly likely to fail and worsen the infection. The infection must be controlled first.
- Option E is incorrect: A dynamic traction splint is part of rehabilitation for tendon gliding, but it is not appropriate in the setting of an acute infection.
Question 18
A 25-year-old factory worker sustains a complete laceration of the FDP tendon in Zone I of his index finger. During the surgical repair, after placing a 4-strand core suture, the surgeon proceeds to apply an epitendinous suture. According to the case, what is the primary purpose of this epitendinous suture?
Explanation
Correct Answer: C
Explanation:
The case clearly outlines the purpose of the epitendinous suture under "Tendon Repair Principles."
- Option C is correct: The case states: "Epitendinous Suture: Purpose: Smoothes the repair site, reducing friction and adhesion formation. Adds 10-50% to the tensile strength of the repair, depending on the technique. Closes the tendon sheath, preventing the core suture from catching on surrounding tissues."
- Option A is incorrect: The core suture is responsible for the majority of the repair's tensile strength and resistance to gapping, not the epitendinous suture.
- Option B is incorrect: The epitendinous suture is applied at the repair site in the digit, not to prevent muscle contracture in the forearm.
- Option D is incorrect: The fibro-osseous pulley system is a separate anatomical structure. While pulleys may be incised for access and sometimes repaired, the epitendinous suture's role is not to re-establish the pulley system itself.
- Option E is incorrect: This describes a function related to dynamic traction protocols (like Kleinert) and is not the primary purpose of the epitendinous suture.
Question 19
A 30-year-old patient undergoes flexor tendon repair of the middle finger in Zone II. Post-operatively, the hand therapist initiates an Early Active Motion (EAM) protocol. Which of the following is a key characteristic or advantage of EAM protocols, as highlighted in the case, compared to controlled passive motion protocols?
Explanation
Correct Answer: C
Explanation:
The case discusses the advantages and characteristics of Early Active Motion (EAM) protocols in the "Post-Operative Rehabilitation Protocols" section.
- Option C is correct: The case states: "Early Active Motion (EAM) Protocols... Rationale: Active muscle contraction leads to greater tendon excursion, theoretically reducing adhesions more effectively and leading to faster return of active range of motion." It also mentions that EAM protocols generally demonstrate superior outcomes in terms of active ROM and quicker return to function compared to CPM.
- Option A is incorrect: The case notes: "While some early EAM protocols had slightly higher rerupture rates historically, modern EAM protocols, when applied to adequately strong repairs, show comparable rerupture rates to passive protocols." So, a significantly higher rate is not accurate for modern EAM.
- Option B is incorrect: EAM protocols involve controlled motion, not strict continuous immobilization. Immobilization is characteristic of older, less effective protocols or for very tenuous repairs.
- Option D is incorrect: EAM protocols require a strong repair (e.g., 4-6 strand core suture with epitendinous repair) with tensile strength typically greater than 45-50 N, not weak repairs.
- Option E is incorrect: This describes controlled passive motion (CPM) protocols like Duran, not EAM. EAM involves controlled active muscle contraction.
Question 20
A 48-year-old patient presents with a "jersey finger" injury, where he forcibly hyperextended his ring finger while grabbing an opponent's jersey, resulting in an avulsion of the FDP tendon from its insertion. This injury is classified as a Zone I flexor tendon injury. According to the case, what is a common method for repairing this specific type of injury?
Explanation
Correct Answer: B
Explanation:
The case specifically addresses Zone I injuries, including FDP avulsions (jersey finger), under "Specific Considerations by Zone."
- Option B is correct: The case states: "Zone I (FDP Avulsions): Often involve a bony fragment (e.g., 'jersey finger'). Repair involves reattaching the FDP to the distal phalanx (e.g., using a pull-out suture technique through the nail plate, suture anchors, or direct repair if a large bony fragment is present)."
- Option A is incorrect: Primary repair of FDP to FDS is not the standard for a Zone I FDP avulsion. The FDS inserts more proximally on the middle phalanx.
- Option C is incorrect: Excision of the FDP would result in permanent loss of DIP flexion, which is not the goal of treatment.
- Option D is incorrect: A two-stage reconstruction using a Hunter rod is typically reserved for chronic, irreparable tears or failed primary repairs, not acute avulsions.
- Option E is incorrect: The A2 pulley is located on the proximal phalanx, and repairing the FDP to it would not restore DIP joint function.
Question 21
A 33-year-old patient undergoes flexor tendon repair of the small finger. Post-operatively, the surgeon and hand therapist decide to implement a Kleinert protocol. Which of the following is a characteristic feature of the Kleinert protocol, as described in the case?
Explanation
Correct Answer: B
Explanation:
The case provides a clear description of the Kleinert protocol under the "Post-Operative Rehabilitation Protocols" section.
- Option B is correct: The case states: "Kleinart Protocol (Controlled Passive Motion with Dynamic Traction): Description: Utilizes a dynamic traction system (rubber band attached to the fingernail and a wrist strap) to passively flex the digits into the palm. The patient actively extends the digits against the resistance of the rubber band to the limits of the dorsal blocking splint."
- Option A is incorrect: This describes a synergistic wrist motion exercise, which is part of some Early Active Motion (EAM) protocols, not Kleinert.
- Option C is incorrect: This describes a "place and hold" exercise, which is also part of some EAM protocols, not Kleinert.
- Option D is incorrect: The Kleinert protocol is a controlled motion protocol, not strict immobilization.
- Option E is incorrect: While Kleinert is a passive motion protocol, it still requires a reasonably strong repair. The case does not specify a very low tensile strength requirement for Kleinert; rather, it emphasizes that EAM protocols require strong repairs (45-50 N).
Question 22
A 29-year-old patient presents with a complete flexor digitorum profundus (FDP) laceration in Zone II of the ring finger. During pre-operative planning, the surgeon emphasizes the importance of a bloodless field and precise visualization. Which of the following equipment is highlighted in the case as critical for precise tendon identification, suture placement, and neurovascular repair?
Explanation
Correct Answer: C
Explanation:
The case details the necessary equipment for flexor tendon repair under "Pre-Operative Planning & Patient Positioning."
- Option C is correct: The case states: "Equipment: Loupe magnification (2.5x to 4.5x) is critical for precise tendon identification, suture placement, and neurovascular repair."
- Option A is incorrect: Large bone-holding clamps are typically used in fracture fixation, not for delicate flexor tendon repair.
- Option B is incorrect: While headlights provide light, the case specifically emphasizes the critical need for magnification for precision, implying standard headlights alone are insufficient.
- Option D is incorrect: A pneumatic tourniquet is used, but it is applied to the upper arm for a bloodless field in hand surgery, not the lower extremity.
- Option E is incorrect: The case specifies: "Non-absorbable monofilament sutures (e.g., 3-0, 4-0, 5-0 Prolene or Ethibond) for core repair," not absorbable sutures.
Question 23
A 24-year-old male is 3 months status post anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. He complains of an inability to fully extend his knee and anterior knee pain during walking. Lateral extension radiographs demonstrate that the tibial tunnel is positioned entirely anterior to the intersection of Blumensaat's line and the tibial plateau. What is the most likely consequence of this tunnel malposition?
Explanation
Question 24
An 8-year-old boy (Tanner stage 1) sustains a complete mid-substance ACL tear. Conservative management fails, and he exhibits recurrent instability. What is the most appropriate surgical technique to minimize the risk of growth arrest?
Explanation
Question 25
When comparing bone-patellar tendon-bone (BTB) autografts to quadrupled hamstring autografts for ACL reconstruction, which of the following is an established biological or biomechanical advantage of the BTB graft?
Explanation
Question 26
The anterior cruciate ligament consists of two functionally distinct bundles. The anteromedial (AM) bundle is most responsible for resisting anterior tibial translation at which of the following degrees of knee flexion?
Explanation
Question 27
A 45-year-old female experiences acute posterior medial knee pain after squatting to lift a heavy box. MRI reveals a complete posterior root tear of the medial meniscus. Biomechanically, this injury most closely mimics the contact pressures of which of the following conditions?
Explanation
Question 28
A 28-year-old carpenter lacerates the volar aspect of his index finger at the level of the proximal phalanx, transecting both the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons. According to the Verdan classification, which zone of flexor tendon injury does this represent?
Explanation
Question 29
During a flexor tendon repair in Zone II, careful preservation or reconstruction of the flexor sheath is attempted. Which two annular pulleys are the most critical to preserve to prevent bowstringing and mechanical disadvantage?
Explanation
Question 30
When performing a primary repair of a lacerated flexor tendon, which factor is the strongest predictor of the initial tensile strength of the repair?
Explanation
Question 31
Following a 4-strand core repair with a running epitendinous suture for a Zone II FDP laceration, the surgeon prescribes a post-operative rehabilitation protocol. Which of the following is the most widely accepted modern approach to prevent adhesions while protecting the repair?
Explanation
Question 32
The medial meniscus is injured more frequently than the lateral meniscus. This is largely attributed to its decreased mobility. Which anatomical structure firmly anchors the medial meniscus, limiting its excursion during knee motion?
Explanation
Question 33
A 22-year-old athlete returns to the clinic 6 months following a successful ACL reconstruction. She complains of an audible "clunk" and a 10-degree block to terminal extension. MRI demonstrates a nodular mass anterior to the ACL graft in the intercondylar notch. What is the most likely diagnosis?
Explanation
Question 34
A 24-year-old rugby player injures his ring finger while grabbing an opponent's jersey. He cannot actively flex the distal interphalangeal (DIP) joint. Radiographs show a large bony avulsion fragment volar to the DIP joint. According to the Leddy and Packer classification, what type of FDP avulsion injury is this?
Explanation
Question 35
During arthroscopic repair of a meniscal tear in the avascular "white-white" zone, the surgeon elects to perform an abrasion of the intercondylar notch (trephination/notch microfracture). What is the primary biological rationale for this adjunct procedure?
Explanation
Question 36
Flexor tendons within the digital synovial sheaths of the hand rely on specific mechanisms for nutrition and healing. Which of the following accurately describes their primary mode of nutritional supply?
Explanation
Question 37
During the femoral tunnel preparation for ACL reconstruction, the surgeon identifies the lateral intercondylar ridge (resident's ridge). What is the critical anatomical significance of this landmark when placing the femoral tunnel?
Explanation
Question 38
Radial tears of the meniscus are known to cause rapid progression of knee osteoarthritis compared to simple longitudinal tears. This is primarily because a complete radial tear directly abolishes which meniscal function?
Explanation
Question 39
The origin of the lumbrical muscles from the flexor digitorum profundus (FDP) tendons serves as the functional anatomic boundary between which two flexor tendon zones in the hand?
Explanation
Question 40
A 16-year-old athlete undergoes an all-inside meniscal repair for a longitudinal peripheral tear in the red-red zone. Which of the following suture configurations is biomechanically strongest because it captures the primary collagen fiber orientation of the meniscus?
Explanation
Question 41
A patient presents with a swollen, erythematous, and exquisitely painful knee 3 weeks after an uncomplicated ACL reconstruction with a hamstring autograft. Joint aspiration yields a white blood cell count of 85,000 cells/mcL with 90% polymorphonuclear leukocytes. What is the most appropriate initial management?
Explanation
Question 42
Following a primary flexor tendon repair in the hand, the healing process goes through inflammatory, fibroblastic, and remodeling phases. At what post-operative timeframe is the repaired tendon statistically at its weakest, increasing the risk of spontaneous rupture?
Explanation
Question 43
Which bundle of the anterior cruciate ligament (ACL) is primarily responsible for rotational stability and is tightest when the knee is in extension?
Explanation
Question 44
A 30-year-old carpenter lacerates his index finger volar surface at the level of the proximal phalanx, cutting both the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP). Which zone of flexor tendon injury does this represent, and what is its historical designation?
Explanation
Question 45
A 50-year-old female experiences a pop in the back of her knee while squatting. MRI reveals a complete radial tear adjacent to the posterior horn medial meniscus root. Biomechanically, if left untreated, this injury is most equivalent to which of the following?
Explanation
Question 46
Following an ACL reconstruction, a patient complains of recurrent knee giving way. On exam, the Lachman test is grade I with a firm endpoint, but the pivot shift is grade III. Radiographs show the femoral tunnel positioned at the 12 o'clock position in the intercondylar notch. What is the primary cause of this patient's instability?
Explanation
Question 47
During a Zone II flexor tendon repair, the surgeon opts for a 4-strand core suture technique instead of a traditional 2-strand technique. What is the primary biomechanical advantage of increasing the number of core suture strands?
Explanation
Question 48
During arthroscopy for an acute ACL tear, the surgeon evaluates the posterior horn of the medial meniscus and suspects a tear of the meniscocapsular junction. What is the most appropriate approach to optimally view and treat this 'ramp lesion'?
Explanation
Question 49
When performing a wide exposure for a delayed flexor tendon repair in the hand, which of the following annular pulleys are considered the most critical biomechanically to preserve or reconstruct to prevent tendon bowstringing?
Explanation
Question 50
A 9-year-old male (Tanner stage 1) sustains a midsubstance ACL rupture. The family desires surgical intervention due to recurrent instability. Which surgical technique is most appropriate to minimize the risk of growth arrest?
Explanation
Question 51
The healing potential of a meniscus tear is largely dependent on its blood supply. Which of the following vascular structures are the primary source of blood supply to the peripheral aspect of the menisci?
Explanation
Question 52
Following a 4-strand Zone II flexor tendon repair, the patient is started on an early active motion rehabilitation protocol. Compared to static immobilization, early active motion has been shown to result in which of the following?
Explanation
Question 53
A 25-year-old male is undergoing primary ACL reconstruction. He is an avid deep-squat weightlifter and sprinter. If a quadrupled hamstring autograft is chosen over a bone-patellar tendon-bone autograft, he is at the highest risk for which of the following specific post-operative deficits?
Explanation
Question 54
A 21-year-old rugby player presents with an inability to actively flex the distal interphalangeal joint of his ring finger after grabbing an opponent's jersey. Examination reveals a tender mass in the palm. According to the Leddy-Packer classification, what is the recommended timeframe for surgical intervention for this specific injury pattern?
Explanation
Question 55
A 6-year-old child presents with a painless, palpable, and audible 'clunk' on the lateral side of the knee during terminal extension. An MRI confirms a lateral discoid meniscus. If the Wrisberg variant is present, which of the following anatomic structures is characteristically absent?
Explanation
Question 56
Two weeks after an uncomplicated hamstring autograft ACL reconstruction, a patient presents with an acute effusion, severe knee pain, and a fever of 101.5°F. Aspiration yields purulent fluid with a WBC count of 85,000/µL. What is the most appropriate initial surgical management?
Explanation
Question 57
The flexor tendons of the hand receive their nutrition through both synovial diffusion and a direct vascular supply. Which structures carry the direct segmental blood supply to the flexor digitorum superficialis and profundus tendons within the digital sheath?
Explanation
Question 58
A 30-year-old carpenter sustains a volar laceration over the proximal phalanx of his ring finger, resulting in an inability to actively flex the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. He is scheduled for primary flexor tendon repair. This injury occurred in which of the following flexor tendon zones?
Explanation
Question 59
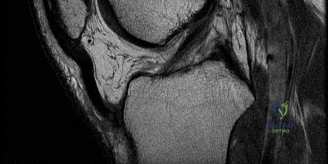
A 23-year-old skier sustains a twisting injury to his knee. MRI demonstrates the bone bruise pattern shown.
What is the primary mechanism of injury associated with this classic bone bruise pattern?
Explanation
Question 60
Which of the following flexor tendon repair techniques provides the greatest ultimate tensile strength to allow for early active motion protocols?
Explanation
Question 61
A 55-year-old male feels a pop in the posterior aspect of his knee while deep squatting. An MRI reveals the finding typically associated with the image below.
If this specific medial meniscal lesion is left untreated, what is the primary biomechanical consequence?
Explanation
Question 62
During an inside-out repair of a posterior horn tear of the medial meniscus, which of the following neurologic structures is at greatest risk of iatrogenic injury?
Explanation
Question 63
A 28-year-old female presents with recurrent instability 2 years post-ACL reconstruction. Imaging shows a vertical femoral tunnel positioned anterior to the native footprint.
What is the most likely clinical consequence of this specific femoral tunnel malposition?
Explanation
Question 64
A 21-year-old collegiate rugby player sustains an avulsion of the flexor digitorum profundus (FDP) of his ring finger (Jersey finger). Radiographs reveal a large bony fragment retracted to the level of the proximal interphalangeal (PIP) joint. This represents which type of Leddy-Packer injury?
Explanation
Question 65
When performing a clinical examination for a suspected isolated flexor digitorum superficialis (FDS) laceration in the middle finger, the examiner holds the index, ring, and small fingers in full extension. What is the biomechanical rationale for this maneuver?
Explanation
Question 66
Which of the following intrinsic anatomical risk factors is most strongly associated with an increased incidence of non-contact ACL tears in female athletes?
Explanation
Question 67
A 10-year-old male with wide-open physes sustains a mid-substance ACL tear. The family opts for surgical intervention. Which of the following surgical techniques is most appropriate to minimize the risk of growth arrest?
Explanation
Question 68
Following a Zone II flexor tendon repair, what is the primary source of nutrition for the tendon during the initial stages of healing?
Explanation
Question 69
A 16-year-old athlete undergoes an arthroscopic partial meniscectomy for a symptomatic discoid lateral meniscus. The surgeon notes that the posterior horn lacks meniscotibial attachments and is hypermobile. Which variant of a discoid meniscus does this represent?
Explanation
Question 70
A patient with long-standing Rheumatoid Arthritis presents with an inability to actively flex the interphalangeal joint of the thumb. History reveals a sudden loss of function without preceding trauma. What is the most likely etiology of this tendon rupture (Mannerfelt syndrome)?
Explanation
Question 71
During acute ACL reconstruction, the surgeon evaluates the menisci. A peripheral longitudinal tear at the meniscocapsular junction of the posterior horn of the medial meniscus is suspected but not clearly visualized from the standard anterolateral viewing portal. What is the best step to evaluate this lesion?
Explanation
Question 72
A 25-year-old male is 3 weeks post-operative from an ACL reconstruction with bone-patellar tendon-bone autograft. He presents with worsening knee pain, swelling, erythema, and a fever of 101.5°F. Joint aspiration yields a leukocyte count of 65,000 cells/mm3 with 90% neutrophils. What is the most appropriate initial management?
Explanation
Question 73
Biomechanical studies of the digital flexor tendon pulleys have demonstrated that preserving or repairing certain pulleys is critical to prevent clinically significant bowstringing. Which two pulleys are deemed most critical in this regard?
Explanation
Question 74
Which of the following blood vessels provides the primary arterial supply to the peripheral 10-30% of the medial and lateral menisci?
Explanation
Question 75
When counseling a patient on graft choices for primary ACL reconstruction, you discuss the morbidity of bone-patellar tendon-bone (BTB) autograft compared to hamstring autograft. Which of the following is significantly more common with BTB autograft?
Explanation
Question 76
A surgeon is performing an ACL reconstruction using an anteromedial portal technique for femoral tunnel drilling. To minimize the risk of a critically short femoral tunnel or posterior wall blowout, at what degree of knee flexion should the knee ideally be positioned during drilling?
Explanation
Question 77
A patient presents with a laceration isolated to the flexor digitorum profundus (FDP) tendon in Zone I of the index finger. If primary repair is performed utilizing an early active mobilization protocol, what complication is statistically most common?
Explanation
Question 78
A 16-year-old female gymnast is undergoing ACL reconstruction. If a bone-patellar tendon-bone allograft is chosen instead of a bone-patellar tendon-bone autograft, what is the most likely biomechanical or clinical consequence?
Explanation
Question 79
During an ACL reconstruction, the surgeon evaluates the native footprints. The native anterior cruciate ligament consists of two distinct bundles. The anteromedial (AM) bundle is best described by which of the following kinematic characteristics?
Explanation
Question 80
A 24-year-old male presents 4 months after an uncomplicated hamstring autograft ACL reconstruction complaining of a painful inability to fully extend his knee. Clinical examination reveals a palpable clunk at terminal extension. What is the most likely etiology of his limited extension?
Explanation
Question 81
A 55-year-old female sustains a medial meniscus posterior root tear while squatting. Biomechanically, how does this specific injury alter knee joint loading?
Explanation
Question 82
Which of the following best describes the vascular supply of the adult meniscus, which fundamentally determines the healing potential of surgical meniscal repairs?
Explanation
Question 83
A 10-year-old boy presents with a painful popping sensation in his lateral knee. MRI demonstrates a Wrisberg variant discoid lateral meniscus. What specific anatomical deficiency defines this variant?
Explanation
Question 84
A 28-year-old carpenter sustains a deep laceration to the volar aspect of his index finger precisely at the level of the proximal interphalangeal (PIP) joint, severing both the FDS and FDP tendons. In which flexor tendon zone did this injury occur?
Explanation
Question 85
During the surgical exploration and repair of a Zone II flexor tendon laceration, the surgeon must be meticulous in preserving or reconstructing the pulley system to prevent bowstringing. Which of the following pairs of annular pulleys are biomechanically most critical to preserve?
Explanation
Question 86
When performing a primary flexor tendon repair in the hand, the tensile strength of the repair site is most directly proportional to which of the following technical factors?
Explanation
Question 87
Review the provided sagittal MRI <br/><br/>. In the setting of an acute non-contact pivoting injury resulting in an ACL rupture, which specific pattern of secondary trabecular microfractures (bone bruises) is classically observed on MRI?
Explanation
Question 88
A 9-year-old boy (Tanner stage 1) with widely open physes sustains a complete ACL tear. He experiences recurrent giving-way episodes despite bracing and physical therapy. If surgical reconstruction is selected, which technique is most appropriate to minimize the risk of iatrogenic growth arrest?
Explanation
Question 89
During an arthroscopic ACL reconstruction, the surgeon probes the posterior aspect of the medial compartment and identifies a 'ramp lesion'. This pathology represents a tear involving which of the following specific structures?
Explanation
Question 90
Following a multi-strand Zone II flexor tendon repair, modern postoperative rehabilitation often employs early active motion protocols. What is the primary physiological and clinical advantage of early active mobilization over prolonged strict immobilization?
Explanation
Question 91
A patient presents with a volar laceration to the hand. To isolate and test the integrity of the Flexor Digitorum Superficialis (FDS) of the ring finger, the examiner holds all other digits in full extension and asks the patient to flex the ring finger at the PIP joint. What anatomical principle makes this test valid?
Explanation
None
