ABOS Part I Orthopedic Review: Hand & Ankle Trauma, Osteoarthritis, Physeal Fractures | Part 22159
Key Takeaway
This ABOS Part I review module covers key orthopedic topics: diagnosis and management of erosive osteoarthritis (PIP, thumb CMC), surgical interventions like arthrodesis and trapeziectomy, and the pathophysiology, diagnosis, and surgical fixation of complex distal tibial triplane fractures in adolescents. It emphasizes rehabilitation and long-term care strategies for these conditions.
ABOS Part I Orthopedic Review: Hand & Ankle Trauma, Osteoarthritis, Physeal Fractures | Part 22159
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 52-year-old female presents with a 2-year history of progressive pain, stiffness, and swelling in her bilateral index finger PIP joints. She reports acute flares of inflammation and notes that her mother had similar hand deformities. Radiographs are obtained, one of which is shown below.
Based on the clinical presentation and radiographic findings, which of the following statements regarding her condition is most accurate?

Explanation
Correct Answer: C
The clinical vignette describes a middle-aged woman with progressive pain, stiffness, swelling, acute inflammatory flares, and a familial history of hand deformities, affecting the PIP joints. The provided radiograph (Figure 1) clearly demonstrates the classic 'gull-wing' deformity with central erosion and peripheral osteophytes, which is pathognomonic for erosive osteoarthritis (EOA). The case content explicitly states that EOA predominantly affects middle-aged and older women, with a female-to-male ratio ranging from 5:1 to 12:1, and a familial predisposition has been suggested. Therefore, statement C is the most accurate.
Incorrect Options:
- A: While EOA has an inflammatory component and can mimic seronegative inflammatory arthritis, the specific radiographic 'gull-wing' deformity and the typical demographic (middle-aged women, familial history) are more characteristic of EOA than rheumatoid arthritis (RA). RA typically presents with symmetrical polyarthritis, often involving MCP and wrist joints, and characteristic marginal erosions, not central 'gull-wing' erosions.
- B: The 'pencil-in-cup' deformity is characteristic of psoriatic arthritis, where the proximal phalanx head erodes into the middle phalanx base. The image clearly shows a central erosion of the middle phalanx base with peripheral osteophytes, creating a 'gull-wing' appearance, not a 'pencil-in-cup' deformity.
- D: The case describes a progressive condition, but immediate surgical arthroplasty is not the primary treatment for this stage. Management of EOA follows a staged approach, starting with non-operative measures (NSAIDs, splinting, injections, therapy) for early disease and acute flares. Surgical intervention is reserved for persistent severe pain, progressive joint destruction, or significant functional loss refractory to conservative care.
- E: While classic osteoarthritis (OA) involves cartilage loss and osteophyte formation, the characteristic central erosion and 'gull-wing' deformity are specific to erosive osteoarthritis, which has a distinct inflammatory component leading to more aggressive joint destruction. Classic OA typically presents with joint space narrowing, subchondral sclerosis, and osteophytes, but not usually central erosions of this nature.
Question 2
A 60-year-old female with erosive osteoarthritis of the index finger PIP joint presents with increasing pain and a fixed flexion contracture of 40 degrees, significantly impairing her ability to perform fine motor tasks. Non-operative management over 6 months, including NSAIDs, splinting, and hand therapy, has failed to provide adequate relief. Surgical intervention is planned. Considering the surgical anatomy of the PIP joint, which of the following structures is primarily responsible for preventing hyperextension and provides significant volar stability?
Explanation
Correct Answer: C
The case content explicitly states that the 'Volar Plate' is a strong, fibrocartilaginous structure located on the volar aspect of the joint that prevents hyperextension and provides significant volar stability. Its paired check-rein ligaments anchor it to the proximal phalanx.
Incorrect Options:
- A: True collateral ligaments originate dorsal to the axis of rotation and are taut in flexion, contributing significantly to mediolateral stability, particularly at 30-45 degrees of flexion. They do not primarily prevent hyperextension.
- B: Accessory collateral ligaments originate volarly to the true collaterals and insert into the volar plate. They are taut in extension and relaxed in flexion, but their primary role is to reinforce the volar plate and contribute to overall stability, not solely prevent hyperextension as the main structure. The volar plate itself is the primary hyperextension block.
- D: The central slip of the extensor digitorum communis tendon inserts onto the dorsal base of the middle phalanx and directly extends the PIP joint. It has no role in preventing hyperextension or providing volar stability.
- E: The oblique retinacular ligament courses volarly to the PIP axis, connecting the flexor sheath to the terminal extensor tendon, and plays a role in coordinating DIP and PIP motion, but it is not a primary stabilizer against hyperextension of the PIP joint.
Question 3
A 58-year-old woman with a long history of erosive osteoarthritis of the index finger PIP joint presents with severe, unremitting pain and a progressive 'gull-wing' deformity. Radiographs confirm advanced joint space narrowing, central subchondral collapse, and significant osteophyte formation. She has failed all conservative treatments. The biomechanical changes in EOA, particularly the central collapse, disrupt normal joint congruity and alter load distribution. Which of the following best describes the primary consequence of this central collapse and altered load distribution in the index finger PIP joint?
Explanation
Correct Answer: C
The case content explains that in EOA, the inflammatory process leads to active chondrolysis and subchondral bone erosion, often centrally, resulting in the characteristic 'gull-wing' deformity. This central collapse disrupts the normal joint congruity and alters load distribution. The biomechanics section states: 'The index finger PIP joint's role in forceful pinch and grip exacerbates these changes, leading to increased pain, stiffness, deformity (e.g., flexion contracture, lateral deviation), and functional disability.' Therefore, exacerbated pain, stiffness, and functional disability are the primary consequences.
Incorrect Options:
- A: While osteophyte formation is a compensatory response, it restricts motion and contributes to pain through impingement, rather than increasing overall joint stability in a functional sense, especially when central collapse is present. The overall effect is instability and dysfunction.
- B: Disrupted articular surface contact due to central collapse and osteophytes typically leads to restricted range of motion and stiffness, not enhanced motion.
- D: The case states that 'The intrinsic muscles can become imbalanced, further contributing to progressive deformity,' which would negatively impact pinch strength and function, not improve it.
- E: The central collapse and altered load distribution, coupled with the inflammatory process, make the joint more susceptible to further deformity and destruction, not less.
Question 4
A 65-year-old right-hand dominant woman presents with severe, persistent pain in her left index finger PIP joint due to erosive osteoarthritis. She has a 35-degree fixed flexion contracture and significant lateral deviation, making it difficult to hold objects and perform daily tasks. She has undergone 9 months of non-operative treatment, including NSAIDs, corticosteroid injections, and extensive hand therapy, with no significant improvement. Radiographs show advanced joint space narrowing, subchondral collapse, and large osteophytes. Which of the following is the most appropriate indication for surgical intervention in this patient?
Explanation
Correct Answer: D
The case content's 'Operative Indications' section clearly states that surgical intervention is considered when non-operative measures fail to provide adequate relief from pain, or when significant functional impairment or deformity develops. Specific indications include 'Persistent severe pain: Localized to the PIP joint, refractory to conservative management' and 'Significant loss of function: Inability to perform activities of daily living (ADLs) or occupational tasks due to stiffness, weakness, or pain' and 'Fixed deformity: Such as a significant flexion contracture (>30 degrees), lateral deviation, or rotational deformity that impairs function and cannot be corrected by therapy.' This patient's presentation of severe, persistent pain, 35-degree fixed flexion contracture, significant lateral deviation, and failure of 9 months of conservative treatment perfectly aligns with these operative indications.
Incorrect Options:
- A, B, C: These describe scenarios that fall under 'Non-Operative Indications' in the case content, where initial management focuses on pain control, reduction of inflammation, and preservation of function, without immediate need for surgery.
- E: While patient preference is a factor, if a patient with severe symptoms and failed conservative treatment still wishes to avoid surgery, it would be a contraindication to surgery based on their choice, not an indication for surgery. The question asks for an indication for surgical intervention.
Question 5
A 55-year-old carpenter with severe erosive osteoarthritis of the index finger PIP joint, refractory to conservative treatment, elects for surgical arthrodesis to achieve a stable, pain-free joint for his demanding profession. During the procedure, after preparing the articular surfaces, the surgeon aims to achieve the optimal fusion angle for the index finger PIP joint. Which of the following angles is generally considered most appropriate for fusion of the index finger PIP joint to facilitate optimal object manipulation, pinch, and grip?

Explanation
Correct Answer: C
The 'Detailed Surgical Approach / Technique' section, under 'Arthrodesis of the PIP Joint,' states: 'The index PIP joint is typically fused in 30-45 degrees of flexion. This angle allows for optimal object manipulation, pinch, and grip without interfering with adjacent digits. For the index finger, a slightly more extended position (30-35 degrees) may be preferred to facilitate lateral pinch.' The image (Figure 2) shows a dorsal mini-fragment plate used for rigid fixation, which is a common method for achieving this desired fusion angle.
Incorrect Options:
- A & B: Fusion at 0-20 degrees of flexion would make it difficult to form a functional grip or pinch, as the finger would be too straight to conform to objects.
- D & E: Fusion at 50-80 degrees of flexion would result in a finger that is too flexed, potentially interfering with adjacent digits, making it difficult to extend the finger for object release, and hindering effective pinch and grip.
Question 6
A 48-year-old pianist with erosive osteoarthritis of the index finger PIP joint desires to preserve motion and opts for pyrocarbon arthroplasty. During the surgical procedure, after exposing the joint, the surgeon begins preparing the bone. Which of the following steps is most critical for the successful implantation of a pyrocarbon PIP joint prosthesis?
Explanation
Correct Answer: B
The 'Detailed Surgical Approach / Technique' section, under 'Pyrocarbon Arthroplasty Surgical Approach,' emphasizes: 'Precise bone cuts are critical for pyrocarbon implants. Using an oscillating saw and specific cutting guides provided by the implant system: Resect the proximal phalanx head, preserving the collateral ligament origins. Resect the middle phalanx base, preserving the volar plate and collateral ligament insertions.' This precision is essential for proper implant fit, stability, and kinematics.
Incorrect Options:
- A: Collateral ligaments are crucial for joint stability. The case states that pyrocarbon implants 'require precise bone cuts and good collateral ligament integrity.' Extensive resection would lead to instability and implant failure.
- C: While medullary canals are reamed, aggressive reaming to accommodate oversized stems is incorrect. Reaming should be precise to fit the implant stems without compromising bone stock or causing iatrogenic fracture.
- D: For arthroplasty, the articular cartilage is removed to expose bleeding cancellous bone, allowing for direct bone-to-implant contact and integration, not to leave a thin layer of cartilage.
- E: The extensor mechanism (including the central slip) is meticulously repaired after arthrodesis or arthroplasty to restore function and prevent extensor lag. Leaving it unrepaired would lead to significant functional deficit.
Question 7
A 70-year-old female undergoes arthrodesis of her index finger PIP joint for severe erosive osteoarthritis. Six months post-operatively, she continues to experience localized pain at the fusion site, and radiographs show persistent lucency at the bone-bone interface with no evidence of bridging bone. She has been compliant with her post-operative rehabilitation protocol. What is the most likely complication and its primary surgical salvage strategy?
Explanation
Correct Answer: C
The clinical scenario describes persistent pain and radiographic lucency at the fusion site 6 months post-arthrodesis, indicating a failure of the bones to unite. This is the definition of a non-union. The 'Complications & Management' section explicitly lists 'Non-Union' as a complication of arthrodesis (5-20% incidence). For management, it states: 'Surgical: Revision arthrodesis with bone grafting (autograft or allograft), more rigid internal fixation (e.g., plate and screws), re-preparation of bone ends.' This aligns perfectly with option C.
Incorrect Options:
- A: While infection is a complication, the description of persistent lucency at the bone-bone interface is more indicative of a non-union than an active infection, which would typically present with signs of inflammation, drainage, or systemic symptoms.
- B: Implant fracture is a complication of arthroplasty, not arthrodesis. Revision arthroplasty would not be the salvage for a failed arthrodesis.
- D: CRPS is a possibility after any hand surgery, but the specific radiographic finding of persistent lucency at the fusion site points more directly to a non-union.
- E: Malunion implies that the bones have fused, but in an incorrect alignment. Here, the problem is a lack of fusion (non-union), not fusion in a wrong position.
Question 8
A 62-year-old patient underwent silicone arthroplasty of the index finger PIP joint for erosive osteoarthritis 3 years ago. She now presents with increasing pain, instability, and a palpable click in the joint. Radiographs show evidence of implant fracture and subluxation. She is a high-demand individual who relies heavily on her index finger for pinch and grip. What is the most common and reliable salvage strategy for this failed PIP arthroplasty, especially for the index finger?
Explanation
Correct Answer: D
The 'Complications & Management' section, under 'Salvage Strategies' for 'Failed Arthroplasty (Instability, Fracture, Infection),' states: 'The most common and reliable salvage for a failed PIP arthroplasty, especially for the index finger, is conversion to arthrodesis. This provides stability and pain relief at the cost of motion.' The patient's high demand for pinch and grip further supports arthrodesis, as stability is prioritized for the index finger.
Incorrect Options:
- A: Revision silicone arthroplasty is generally not recommended for failed silicone implants, especially in high-demand joints like the index finger, due to the inherent limitations and high failure rates of silicone prostheses under significant load.
- B: While conversion to pyrocarbon arthroplasty may be considered in select cases if bone stock allows, the case content notes it 'carries higher risks' and that arthrodesis is 'the most common and reliable salvage,' particularly for the index finger where stability is paramount.
- C: Collateral ligament reconstruction alone would not address the implant fracture and subluxation, and would likely be insufficient to restore stability in a failed arthroplasty.
- E: Long-term corticosteroid injections and activity modification are conservative measures that have already failed in the initial treatment and are unlikely to salvage a mechanically failed arthroplasty with implant fracture and subluxation.
Question 9
A 50-year-old patient undergoes arthrodesis of the index finger PIP joint for severe erosive osteoarthritis. Post-operatively, a dorsal splint is applied, maintaining the fused PIP joint in 35 degrees of flexion. Which of the following is the most appropriate initial post-operative rehabilitation instruction for this patient during the first 4-6 weeks?
Explanation
Correct Answer: C
The 'Post-Operative Rehabilitation Protocols' section, under 'Following PIP Arthrodesis,' states for 'Immobilization (0-6 weeks)': 'Strictly avoid any active or passive motion at the fused PIP joint.' It also states for 'Early Mobilization (0-6 weeks)': 'Active and passive range of motion exercises for the MCP and DIP joints of the operated finger, as well as the adjacent fingers, are encouraged immediately to prevent stiffness.' This aligns perfectly with option C.
Incorrect Options:
- A & B: Initiating active/passive ROM or strengthening for the fused PIP joint immediately would jeopardize the fusion site and risk non-union. The goal is rigid immobilization of the PIP joint.
- D: While wound care is important, removing the splint daily for full PIP ROM exercises would compromise the fusion. The splint is typically worn continuously until early fusion is evident.
- E: Dynamic extension splinting is typically used after arthroplasty to assist with extension and prevent flexion contractures, where motion is desired. For arthrodesis, the goal is fusion, and the joint is immobilized in a static position.
Question 10
A 59-year-old female presents with severe pain and deformity of her index finger PIP joint due to erosive osteoarthritis. She is a retired librarian and prioritizes a stable, pain-free joint for activities like reading and light gardening. Radiographs show significant joint destruction. After a thorough discussion of options, the surgeon recommends arthrodesis. According to the current consensus and literature, which of the following statements best supports the choice of arthrodesis for the index finger PIP joint in this patient?
Explanation
Correct Answer: C
The 'Summary of Key Literature / Guidelines' section, under 'Current Consensus,' states: 'For severe, painful, and deforming EOA of the index finger PIP joint refractory to conservative management: 1. Arthrodesis remains a highly reliable option, especially for patients prioritizing stability, pain relief, and strength for pinch and grip. It is generally the preferred option for the index finger PIP joint among many hand surgeons.' This directly supports the choice of arthrodesis for this patient who prioritizes stability and pain relief for her activities.
Incorrect Options:
- A: The literature review indicates that arthrodesis consistently reports high fusion rates and excellent pain relief, while arthroplasty outcomes for the index finger PIP can be less predictable, with concerns regarding implant durability and reoperation rates, especially for silicone.
- B: Silicone arthroplasty is generally less favored for the index PIP due to higher failure rates in this high-demand digit, as stated in the literature review.
- D: While pyrocarbon arthroplasty is a viable alternative, it is not universally recommended. The consensus emphasizes that the decision must be individualized, and arthrodesis is often preferred for the index finger.
- E: The literature review states that arthrodesis consistently reports high fusion rates (85-95%) and excellent pain relief, making this statement incorrect. While non-union is a known complication, its rates are generally manageable, and arthrodesis is considered highly reliable.
Question 11
A 45-year-old female presents with acute, severe pain and swelling in her index finger PIP joint, diagnosed with an acute flare of erosive osteoarthritis. Radiographs show early joint space narrowing and minimal osteophyte formation, without significant erosions or collapse. She has no fixed deformity and good range of motion. Which of the following is the most appropriate initial management strategy?
Explanation
Correct Answer: C
The 'Indications & Contraindications' section, under 'Non-Operative Indications,' lists 'Early disease: Minimal joint destruction, mild to moderate pain, preserved range of motion, and absence of significant deformity' and 'Acute flares: Intense pain and swelling during inflammatory episodes' as indications for non-operative management. The 'Summary of Key Literature / Guidelines' further supports this, stating: 'First-line treatment generally involves NSAIDs for pain and inflammation, activity modification, splinting for support and pain relief during flares, and hand therapy to maintain range of motion and strength. Intra-articular corticosteroid injections can provide temporary relief during acute inflammatory episodes.' This patient's presentation of an acute flare with early disease and preserved function aligns perfectly with this conservative approach.
Incorrect Options:
- A & B: Immediate surgical intervention (arthrodesis or arthroplasty) is reserved for failed conservative management, significant functional impairment, or advanced deformity/destruction, none of which are present in this early stage acute flare.
- D: Long-term systemic immunosuppressive therapy is typically reserved for systemic inflammatory arthropathies like rheumatoid arthritis or psoriatic arthritis, not generally for EOA, which is primarily managed locally and symptomatically.
- E: While psychological support can be beneficial for chronic pain, it is not the primary initial management for an acute inflammatory flare of EOA.
Question 12
A 55-year-old female presents with insidious onset of pain at the base of her right thumb, exacerbated by pinch and grasp. She reports similar, milder symptoms in her left thumb. Her mother also suffered from "thumb arthritis." Which of the following is the most accurate statement regarding the epidemiology and risk factors for this condition?
Explanation
Correct Answer: C
The case states: "Epidemiological studies estimate its prevalence to be between 16% and 25% in the general adult population, with a notable increase with age, affecting over 30% of women and 10% of men over 50 years. Women are disproportionately affected..." This directly supports option C.
Option A is incorrect as the prevalence is higher in women. Option B is incorrect; the case lists generalized ligamentous laxity as a risk factor, not a protective factor. Option D is incorrect; the case explicitly states, "Repetitive thumb use... are also implicated" as risk factors for thumb CMC OA. Option E is incorrect; prior trauma is a risk factor for developing CMC OA, but it is not listed as an absolute contraindication to surgical management, although it might influence the choice of procedure or prognosis.
Question 13
A 62-year-old right-hand dominant female presents with chronic pain at the base of her right thumb, worse with opening jars and turning keys. On examination, she has tenderness over the CMC joint, a positive grind test, and a visible dorsal prominence at the thumb base. Her MCP joint appears hyperextended. Which of the following physical exam findings is most indicative of advanced thumb CMC OA with associated deformity?
Explanation
Correct Answer: C
The case describes the progression of thumb CMC OA leading to "eventual deformity, including the classic 'shoulder sign' due to subluxation of the first metacarpal on the trapezium, and adduction contracture of the thumb metacarpal leading to secondary hyperextension of the metacarpophalangeal (MCP) joint (Z-deformity)." A reduced first web space is a direct consequence of adduction contracture, and compensatory MCP hyperextension completes the Z-deformity, which is a hallmark of advanced disease.
Option A (Positive Finkelstein's test) is primarily indicative of De Quervain's tenosynovitis, although it can sometimes elicit pain at the CMC joint if significant inflammatory synovitis is present; it is not the most indicative sign of advanced deformity. Option B (Pain with resisted wrist extension) suggests extensor carpi radialis or ulnaris pathology. Option D (Tenderness over the scaphoid tubercle) points towards scaphoid pathology. Option E (Pain with resisted thumb IP joint flexion) suggests flexor pollicis longus pathology. None of these are as specific to advanced CMC OA deformity as the Z-deformity.
Question 14
A 48-year-old male presents with early thumb CMC OA. During a discussion about the biomechanics of the joint, the surgeon emphasizes the role of a specific ligament in preventing dorsoradial subluxation of the first metacarpal. Which ligament is the surgeon most likely referring to as the primary static stabilizer against this subluxation?
Explanation
Correct Answer: D
The case explicitly states under "Ligamentous Stabilizers": "Anterior Oblique Ligament (AOL) / Beak Ligament: Considered the most crucial ligament for resisting dorsoradial subluxation of the metacarpal. ...Degeneration and laxity of this ligament are central to the pathogenesis of thumb CMC OA."
Option A (Ulnar Collateral Ligament) provides stability against radial deviation. Option B (Posterior Oblique Ligament) provides dorsal stability but is not considered the primary resistor of dorsoradial subluxation. Option C (Radial Collateral Ligament) provides stability against ulnar deviation. Option E (Intermetacarpal Ligaments) provide static stability and resist axial loading and proximal migration, but not primarily dorsoradial subluxation of the first metacarpal on the trapezium.
Question 15
A 58-year-old female with long-standing thumb CMC OA is noted to have a "shoulder sign" on clinical examination and radiographs showing significant dorsoradial subluxation of the first metacarpal on the trapezium. This subluxation is a key event in the progression of her arthritis. Which of the following statements best describes the biomechanical consequence of this subluxation?
Explanation
Correct Answer: C
Under "Biomechanics of OA Progression," the case details: "1. AOL Laxity/Degeneration: Weakening of the AOL... leads to increased dorsoradial subluxation of the first metacarpal on the trapezium during pinch and grasp. 2. Increased Shear Stress: The altered kinematics result in non-physiological loading patterns, causing high shear and compressive forces on the remaining cartilage."
Option A is incorrect; the subluxation leads to increased shear forces. Option B is partially correct in that compressive forces increase, but the primary issue is the non-physiological loading patterns involving both shear and compression, leading to cartilage erosion, not primarily osteophyte formation as the initial consequence. Option D is incorrect; subluxation destabilizes the joint and leads to incongruent contact, not increased stable contact. Option E is incorrect; subluxation and the resulting adduction contracture limit the web space and impair opposition, leading to the Z-deformity.
Question 16
A 70-year-old patient presents with severe thumb pain. Radiographs reveal significant joint space narrowing, subchondral sclerosis, and osteophyte formation at the thumb CMC joint. There is also evidence of early degenerative changes at the scaphotrapeziotrapezoid (STT) joint. According to the Eaton and Littler classification system, what stage of CMC arthritis does this presentation most likely represent?
Explanation
Correct Answer: D
The Eaton and Littler classification system is described in the case: "Eaton and Littler's classification system, ranging from Stage I (pre-arthritic, joint space widening) to Stage IV (pancarpal arthritis with significant destruction), is commonly used to grade radiographic severity." The presence of "early degenerative changes at the scaphotrapeziotrapezoid (STT) joint" in addition to severe CMC changes is the key indicator for Stage IV, as it signifies involvement beyond the primary CMC joint, often referred to as pancarpal arthritis.
Stage I involves pre-arthritic changes or joint space widening. Stage II involves mild joint space narrowing and osteophytes. Stage III involves significant joint space narrowing, subluxation, osteophyte formation, and subchondral sclerosis, but typically without symptomatic STT involvement or pancarpal arthritis.
Question 17
A 52-year-old painter presents with mild to moderate pain at the base of his dominant thumb, exacerbated by fine brushwork. Radiographs show Eaton-Littler Stage II changes. He has tried NSAIDs with some relief. Which of the following non-operative interventions is most appropriate as the next step in his management, specifically targeting joint stabilization and pain reduction during activity?
Explanation
Correct Answer: D
The patient presents with mild to moderate pain and Eaton-Littler Stage II changes, indicating early to moderate disease. The case states that non-operative management is first-line for such patients. Among the non-operative options, "Orthotics/Splinting: Custom or off-the-shelf splints (e.g., thumb spica splints) to immobilize or support the joint, reducing pain and stabilizing subluxation. Nighttime splinting is common." This directly addresses joint stabilization and pain reduction during activity, which is crucial for a painter.
Option A and E (surgical interventions) are premature given the mild-to-moderate symptoms and Stage II disease. Option B (oral corticosteroids) is not a standard long-term management for chronic OA. Option C (intra-articular corticosteroid injection) can provide temporary pain relief but does not offer continuous joint stabilization during activity as effectively as a splint, and repeated injections carry risks.
Question 18
A 68-year-old female with Eaton-Littler Stage III thumb CMC arthritis has failed 6 months of conservative management, including splinting, NSAIDs, and two corticosteroid injections. She reports debilitating pain and significant functional impairment. She is a well-controlled diabetic (HbA1c 6.5%) and a non-smoker. Which of the following factors would be a relative contraindication to proceeding with surgical intervention (e.g., LRTI)?
Explanation
Correct Answer: D
The case lists "Significant Arthritis in Adjacent Joints: Severe arthritis in the scaphotrapeziotrapezoid (STT) joint or other wrist joints may necessitate a broader surgical approach or influence choice of procedure" as a relative contraindication. While not an absolute contraindication, it complicates the surgical plan for an isolated CMC procedure.
Options A, B, and E (failure of non-operative management, Eaton-Littler Stage III disease, and debilitating pain/functional impairment) are all strong indications for surgical intervention, as outlined in the case. Option C (well-controlled diabetes) is not a contraindication; uncontrolled diabetes would be a relative or absolute contraindication, but an HbA1c of 6.5% is considered well-controlled and generally acceptable for elective surgery.
Question 19
A surgeon is performing a trapeziectomy with LRTI for advanced thumb CMC arthritis. After excising the trapezium, the next step involves preparing the FCR tendon for reconstruction. Referring to the provided image and the case description, which statement accurately describes the FCR tendon harvest for a standard LRTI?

Explanation
Correct Answer: B
Under "Detailed Surgical Approach / Technique Trapeziectomy with LRTI - FCR Tendon Harvest," the case states: "A slip of the FCR tendon, approximately one-third to one-half of its width, and about 8-10 cm long, is harvested from its radial aspect. The slip is proximally based and distally released from its insertion..." The image visually supports the concept of a tendon slip being used for reconstruction.
Option A is incorrect; while the entire FCR can be used, the standard LRTI often uses a slip, and it's used for both suspension and interposition, not just interposition. Option C is incorrect; the slip is proximally based, not distally, and while the scaphoid can be an anchoring point in some variations, it's not the primary method described for the slip passage itself. Option D is incorrect; the FCR is typically used for both components. Option E is incorrect; the slip is harvested from the radial aspect, and preserving a portion of the FCR (as opposed to the entire tendon) is what helps maintain some wrist flexion function, not harvesting from a specific aspect to preserve it.
Question 20
A patient undergoes trapeziectomy with LRTI. Six months post-operatively, they report persistent pain on the radial aspect of the wrist, particularly with axial loading, and radiographs show some proximal migration of the first metacarpal towards the scaphoid. This is causing impingement. Which of the following complications is most likely occurring, and what is a potential salvage strategy?
Explanation
Correct Answer: C
The patient's symptoms (persistent pain on the radial aspect of the wrist, worse with axial loading, and radiographic evidence of proximal metacarpal migration causing impingement) are classic for pillar pain, specifically due to proximal metacarpal subsidence. The case lists "Pillar Pain (Radioscaphoid Impingement)" and "Proximal Metacarpal Subsidence" as complications. For management of pillar pain, it suggests "radial styloidectomy or revision trapeziectomy if residual fragments." For symptomatic/severe subsidence, it suggests "Revision surgery with more robust suspension plasty, intermetacarpal arthrodesis, or implant arthroplasty." Option C accurately combines the complication and appropriate salvage strategies.
Option A (Radial sensory nerve injury) would typically present with neuropathic pain, dysesthesia, or neuroma, not primarily axial loading pain and radiographic impingement. Option B (CRPS) is a diffuse, disproportionate pain syndrome with autonomic features, not typically localized to mechanical impingement. Option D (FCR tendon donor site rupture) would cause pain at the FCR tendon, not necessarily radial wrist impingement. Option E (Adduction contracture) would present with limited web space and impaired opposition, not primarily radial pillar pain with axial loading.
Question 21
Following a trapeziectomy with LRTI, a patient is in the early post-operative phase (0-4 weeks). Which of the following is the most appropriate rehabilitation instruction for this phase?
Explanation
Correct Answer: C
Under "Post-Operative Rehabilitation Protocols - Phase I: Immobilization and Protection (0-4/6 Weeks)," the case states: "Immobilization: ...Thumb spica splint or cast, typically immobilizing the wrist in slight extension, the thumb CMC joint in neutral to slight palmar abduction and slight pronation... Gentle Exercises (Non-Operated Digits): Encourage active range of motion (AROM) of the fingers and IP joint of the thumb to prevent stiffness and maintain circulation." This instruction is critical for protecting the fresh reconstruction.
Option A (immediate active CMC ROM) is too aggressive and risks disrupting the tendon reconstruction. Option B (progressive resistance exercises) is appropriate for later phases (Phase III and IV), not immediately post-op. Option D (forceful passive stretching) is contraindicated in the early phase due to the risk of compromising the surgical repair. Option E (heat therapy) is generally avoided in the immediate post-operative period as it can increase swelling and inflammation; cryotherapy is preferred.
Question 22
A 14-year-old male, Tanner Stage IV, presents with a complex distal tibial physeal fracture after a soccer injury. His history includes seven years of single-sport specialization, training 18+ hours/week, and recent vague, deep-seated distal tibial pain. Which of the following statements best describes the most likely underlying pathophysiology contributing to this patient's acute injury?
Explanation
Correct Answer: C
The case explicitly states that the patient's history of single-sport specialization, high training volume, and prodromal symptoms (vague, deep-seated pain in the distal tibia) strongly suggest a pre-existing stress reaction or stress fracture of the distal tibial metaphysis. This chronic microtrauma disrupts normal bone remodeling, leading to microscopic trabecular failure and structural compromise. When a sudden, high-energy torsional force is applied to this already weakened bone, it fails catastrophically, often involving the partially closed physis, as seen in this complex triplane fracture. This highlights the long-term impact of single-sport specialization and inadequate recovery.
Option A is incorrect because Tanner Stage IV indicates partial physeal closure, specifically the transitional period where the physis is uniquely vulnerable to these types of fractures (Tillaux and triplane). Complete closure would make a physeal fracture impossible. Option B is incorrect as the mechanism described is a twisting sensation with a planted foot, characteristic of an external rotation injury, not a direct impact. Option D is incorrect; while avulsion fractures of the anterior inferior tibiofibular ligament (Chaput tubercle) are seen in this age group (Tillaux fracture), the underlying pathophysiology of chronic stress reaction due to specialization is a more fundamental contributing factor to the complexity of this specific injury. Option E is incorrect; while a 'pop' can occur with ligamentous injuries, the severe pain, rapid swelling, and inability to bear weight, especially in the context of prodromal symptoms and the described mechanism, are highly suggestive of a significant bony injury, which was confirmed to be a complex physeal fracture.
Question 23
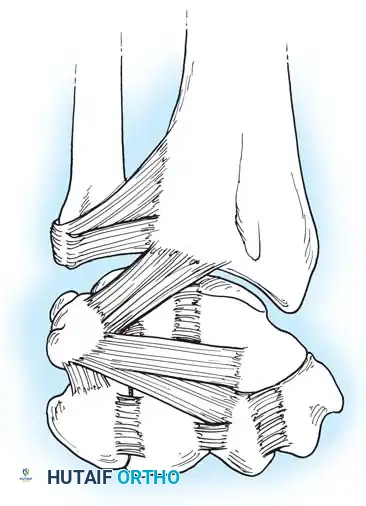
A 14-year-old male presents to the ED after a soccer injury. On examination, you note significant diffuse edema, moderate ecchymosis, and a subtle deformity with the foot in slight external rotation. Palpation reveals marked tenderness circumferentially around the distal tibia and fibula, maximal over the distal tibial metaphysis, physis, and epiphysis. Distal pulses are palpable and strong.
Given these findings and the provided image, which of the following is the most appropriate next step in the immediate management of this patient?

Explanation
Correct Answer: C
The most appropriate immediate next step for any acute ankle injury with suspected fracture is to obtain standard orthogonal radiographs (anteroposterior, lateral, and mortise views) of the ankle. These initial diagnostic modalities are crucial for identifying the presence of a fracture, assessing its general morphology, and guiding further management. The clinical findings of significant edema, ecchymosis, deformity, and marked tenderness are highly indicative of a fracture, making radiographic evaluation mandatory.
Option A is incorrect because applying a cast and discharging without definitive diagnosis and assessment of displacement is inappropriate and could lead to missed significant injury or inadequate treatment. Option B is incorrect; formal stress testing or stress radiographs are typically deferred in the acute setting due to severe pain and are not the initial diagnostic step. Gross instability was appreciated, but formal stress testing is usually done after initial imaging and often under anesthesia if surgery is planned. Option D is incorrect; while compartment syndrome is a serious concern, the case states distal pulses were palpable and strong, and there were no signs of impending compartment syndrome. Therefore, emergent fasciotomy is not indicated at this stage. Prophylactic antibiotics are given preoperatively, not as an immediate ED step without a confirmed open fracture. Option E is incorrect; attempting a closed reduction without full radiographic assessment, including potentially a CT scan, is premature and could be harmful, especially given the complex nature of these transitional fractures where soft tissue interposition is common.
Question 24
A 14-year-old male, Tanner Stage IV, sustains a distal tibial physeal fracture. The distal tibial physis contributes approximately 45% of the total longitudinal growth of the tibia. Understanding the chronological and spatial sequence of physeal closure is critical for managing such injuries. Which of the following statements accurately describes the typical pattern of distal tibial physeal closure?

Explanation
Correct Answer: B
The case explicitly states that the closure pattern of the distal tibial physis is highly predictable and asymmetric. It initiates in the central portion (often referred to as Kump bump) and proceeds medially. The lateral and anterolateral portions of the physis are the final segments to fuse. This asymmetrical closure creates a unique biomechanical vulnerability during the transitional period, leading to fracture patterns like the juvenile Tillaux and triplane fractures.
Option A is incorrect as it reverses the correct closure pattern. Option C is incorrect because the closure is distinctly asymmetrical, not symmetrical. Option D is incorrect as the primary description focuses on medial-to-lateral and central-to-peripheral progression, not posterior-to-anterior. Option E is incorrect; the distal tibial physis typically begins to close around age 14-15 in males, corresponding precisely with Tanner Stage IV development, making physeal fractures, particularly transitional ones, common in this stage.
Question 25
The patient's injury mechanism involved an external rotation force on a planted foot. This mechanism, combined with the asymmetrical physeal closure, predisposes adolescents to specific fracture patterns. Considering the provided image, which depicts a complex multi-planar fracture, what is the most accurate description of the typical fracture lines in a triplane fracture?
Explanation
Correct Answer: C
The case specifically describes the biomechanics of a triplane fracture: 'The fracture line propagates through the epiphysis in the sagittal plane, travels along the open physis in the axial plane, and exits through the posterior metaphysis in the coronal plane.' This multi-planar nature is what gives the triplane fracture its name and makes it complex to diagnose and treat.
Option A describes a simpler fracture pattern, not a triplane. Option B incorrectly describes the planes of exit for the metaphyseal and epiphyseal components. Option D describes a metaphyseal fracture, which is distinct from a triplane fracture involving the physis and epiphysis. Option E describes a different injury altogether, although medial malleolus fractures can occur with external rotation, it's not the defining characteristic of a triplane fracture.
Question 26
Following initial radiographs for the 14-year-old male with a suspected complex distal tibial physeal fracture, the plain films are inconclusive regarding the exact extent of articular displacement. The patient's clinical presentation and mechanism of injury are highly suggestive of a triplane fracture.
Based on the case, what is the most appropriate next imaging modality for definitive preoperative planning?

Explanation
Correct Answer: C
The case explicitly states: 'A high-resolution Computed Tomography scan with sagittal, coronal, and three-dimensional reconstructions is mandatory for all suspected triplane and Tillaux fractures. The CT scan allows the orthopedic surgeon to precisely map the fracture lines, quantify the articular step-off, identify the presence of intercalary articular fragments, and plan the exact trajectory for internal fixation.' Plain films frequently underestimate the degree of articular displacement and the number of fracture fragments in these complex, multi-planar injuries.
Option A is incorrect because stress views are not the primary method for assessing articular displacement in complex physeal fractures and are often limited by pain. Option B, MRI, is excellent for soft tissue and cartilage assessment but is not the primary modality for detailed bony architecture and fracture mapping in the acute setting for surgical planning of these specific fractures. Option D, bone scintigraphy, is used for stress fractures but not for acute, complex intra-articular fracture planning. Option E, arthrography, is an invasive procedure not indicated for routine preoperative planning of these fractures.
Question 27
A 14-year-old male presents with a triplane fracture of the distal tibia. Preoperative CT scan reveals 3 mm of articular step-off and a displaced metaphyseal fragment. The primary goal of management is anatomic restoration of the articular surface. Based on the provided guidelines, what is the most appropriate management strategy?
Explanation
Correct Answer: C
The case clearly states the operative decision-making criteria: 'Operative intervention is strictly indicated when there is unacceptable displacement of the articular surface. The universally accepted threshold for surgical intervention in intra-articular fractures of the weight-bearing distal tibia is greater than two millimeters of displacement or step-off.' With 3 mm of articular step-off, this patient unequivocally meets the criteria for immediate open reduction and internal fixation (ORIF) to prevent post-traumatic osteoarthritis.
Option A is incorrect because non-operative management is reserved for undisplaced fractures or those with less than 2 mm of displacement. Option B is partially correct in that closed reduction may be attempted, but with 3mm of displacement, the likelihood of successful anatomic closed reduction is low, and the guidelines indicate that if displacement is >2mm, ORIF is indicated. The table also states 'Failed Closed Reduction -> Operative ORIF'. Given the initial displacement, proceeding directly to ORIF is the most appropriate and definitive management. Option D, external fixation, is typically reserved for open fractures, highly comminuted fractures, or those with significant soft tissue compromise, which are not described here. Option E, percutaneous pinning without open reduction, is less likely to achieve anatomic reduction of a complex triplane fracture with 3mm of articular step-off and is generally not recommended for displaced intra-articular fractures.
Question 28
During open reduction and internal fixation of the patient's triplane fracture via an anterolateral approach, the surgeon encounters difficulty achieving anatomic reduction of the anterolateral epiphyseal fragment despite adequate exposure. What is the most common impediment to closed and open reduction in these types of fractures?
Explanation
Correct Answer: D
The case explicitly states: 'The fracture edges are often covered with interposed periosteum, which is the most common impediment to closed reduction. This periosteum must be carefully elevated and retracted to expose the raw cancellous bone of the fracture site.' This soft tissue interposition is a frequent reason for failed closed reduction and requires meticulous surgical technique during open reduction.
Option A, significant comminution, can make reduction challenging but is not described as the 'most common impediment' in the text. Option B, interposition of the anterior inferior tibiofibular ligament, can occur, particularly in Tillaux fractures, but the text highlights periosteum as the most common impediment. Option C, excessive fracture hematoma, must be irrigated and debrided for visualization, but it is not the primary mechanical block to reduction. Option E, premature physeal closure, is a complication that occurs after healing, not an impediment to acute reduction.
Question 29
Following successful reduction of the triplane fracture, the surgeon proceeds with internal fixation using partially threaded cannulated screws. The patient is Tanner Stage IV and nearing skeletal maturity. When placing the screws for definitive fixation, which principle is most critical to prioritize in this specific patient?
Explanation
Correct Answer: C
The case states: 'If the patient is Tanner Stage IV and nearing skeletal maturity, the risk of clinically significant growth arrest from crossing the physis with a smooth screw shaft is negligible compared to the catastrophic risk of articular incongruity.' Therefore, prioritizing anatomic articular congruity is paramount in this age group, even if it necessitates crossing the physis with a smooth screw shaft, as the risk of growth arrest is low and the risk of post-traumatic arthritis from incongruity is high.
Option A is incorrect because, while generally desirable, in older adolescents nearing skeletal maturity, the risk-benefit analysis shifts, and articular congruity takes precedence over strictly avoiding physeal violation. Option B is incorrect; partially threaded screws are typically used to achieve lag compression across the fracture fragments, and fully threaded screws might not provide the desired compression. Option D is incorrect; K-wires are used for provisional fixation, but definitive fixation for displaced intra-articular fractures typically requires screws for stable compression. Option E is incorrect; screw placement trajectory is dictated by fracture morphology and optimal fixation, not solely by nerve avoidance, although nerve protection is always critical during the approach.
Question 30
Despite meticulous surgical technique for the triplane fracture, the patient is at risk for several postoperative complications. Which of the following complications is considered the most dreaded in pediatric distal tibial physeal fractures, particularly if not anatomically reduced?
Explanation
Correct Answer: C
The case explicitly states: 'The most dreaded complication is premature physeal closure leading to angular deformity or leg length discrepancy.' While the risk is mitigated in older adolescents, precise anatomical reduction of the physis minimizes the formation of a transphyseal bony bar. This complication can have significant long-term functional and cosmetic consequences for a growing child.
Option A, hardware prominence, is a frequent complaint (30-40% incidence) often requiring secondary surgery, but it is generally not considered 'dreaded' in the same way as growth arrest. Option B, superficial wound infection, has a low incidence (less than 2%) and is typically manageable. Option D, DVT, is rare in pediatric trauma patients. Option E, neurological deficit, while serious, is also a rare complication with careful surgical technique and is not specifically highlighted as the 'most dreaded' in the context of physeal fractures compared to growth disturbances.
Question 31
The patient successfully undergoes ORIF for his triplane fracture. During the rehabilitation phase, the orthopedic surgeon emphasizes the importance of addressing the underlying etiology of the injury. Beyond the phased weight-bearing and functional recovery, what is the most critical long-term recommendation for this patient, given his history?
Explanation
Correct Answer: C
The case emphasizes: 'A critical component of the rehabilitation phase for this specific patient population is addressing the underlying etiology of the injury: single-sport specialization. ...the patient must be counseled to incorporate at least three months of off-season rest or participation in a different sport annually to allow for adequate skeletal remodeling and to mitigate the risk of future stress-related catastrophic failures.'
Option A is incorrect; immediate high-intensity strength training upon cast removal could overload the healing bone and is not part of a phased recovery. Option B is incorrect; return to competitive soccer is typically permitted between three and five months postoperatively, contingent upon full recovery, not just pain subsidence, and without addressing the underlying specialization issue, recurrence is likely. Option D is incorrect; focusing solely on sport-specific training perpetuates the problem of single-sport specialization and increases the risk of overuse injuries. Option E is incorrect; hardware removal is typically elective and performed after complete radiographic consolidation, usually 6-12 months postoperatively, not at 3 months, and it does not address the underlying etiology of the injury.
Question 32
A 14-year-old boy sustains an ankle injury while sliding into a base. Radiographs reveal a fracture of the anterolateral aspect of the distal tibia epiphysis. Which of the following ligaments is responsible for the avulsion of this bony fragment?
Explanation
Question 33
A 10-year-old boy crushes his long finger in a door. Examination shows a laceration through the nail bed and the proximal nail plate sits superficial to the eponychial fold. Radiographs show a displaced Salter-Harris I fracture of the distal phalanx. What is the most appropriate definitive management?
Explanation
Question 34
A 13-year-old girl sustains an ankle fracture. Radiographs show a fracture line in the sagittal plane on the AP view and in the coronal plane on the lateral view. What Salter-Harris classification does this fracture pattern functionally represent?
Explanation
Question 35
A 62-year-old woman presents with severe pain at the base of her thumb. Radiographs demonstrate advanced trapeziometacarpal joint space narrowing, subchondral sclerosis, and a 3 mm radial subluxation of the metacarpal base, but the scaphotrapezial joint is completely spared. What is the Eaton-Littler stage of her thumb arthritis?
Explanation
Question 36
A 25-year-old man sustains a closed intra-articular fracture of the base of the thumb metacarpal with a single volar-ulnar fragment. Which of the following muscles is primarily responsible for the proximal and dorsal displacement of the metacarpal shaft?
Explanation
Question 37
According to the Lauge-Hansen classification, which of the following is the first structure injured in a Supination-External Rotation (SER) ankle fracture?
Explanation
Question 38
A 45-year-old man presents with post-traumatic ankle osteoarthritis following a malreduced lateral malleolus fracture. Biomechanical studies have shown that a lateral shift of the talus by 1 mm decreases the tibiotalar contact area by approximately what percentage?
Explanation
Question 39
A 22-year-old rugby player presents unable to actively flex the DIP joint of his ring finger after grabbing an opponent's jersey. Radiographs reveal a bony avulsion fragment located at the level of the proximal interphalangeal (PIP) joint. According to the Leddy and Packer classification, what type of injury is this?
Explanation
Question 40
A 9-year-old child sustains a Salter-Harris IV fracture of the medial malleolus. Which of the following is the most significant long-term complication uniquely associated with this specific injury pattern?
Explanation
Question 41
A 55-year-old woman presents with a painful, translucent mass over the dorsum of her right index finger DIP joint. Radiographs confirm severe osteoarthritis with a prominent dorsal osteophyte. What is the most critical surgical step to minimize the recurrence of this mass after excision?
Explanation
Question 42
A 35-year-old man presents with chronic wrist pain and a history of an untreated scaphoid waist fracture 10 years ago. Radiographs reveal scaphoid nonunion with radioscaphoid joint space narrowing, but the radiolunate joint is spared. What is the primary biomechanical reason the radiolunate joint is typically spared in a SNAC (Scaphoid Nonunion Advanced Collapse) wrist?
Explanation
Question 43
A 40-year-old sustains an ankle fracture-dislocation. Closed reduction in the emergency department is unsuccessful. CT scan reveals the proximal fibular fragment is entrapped behind the posterior tubercle of the distal tibia. What is this specific injury pattern called?
Explanation
Question 44
When utilizing an anterolateral surgical approach for the open reduction and internal fixation of a severe pilon fracture, which of the following neurologic structures is at greatest risk of iatrogenic injury?
Explanation
Question 45
A 30-year-old basketball player presents with a drooping long finger DIP joint. Radiographs show a dorsal avulsion fracture involving 45% of the articular surface of the distal phalanx with associated volar subluxation of the joint. What is the most appropriate management?
Explanation
Question 46
A 25-year-old male sustains a thumb injury during a fist fight. Radiographs reveal a two-part fracture of the base of the first metacarpal with the shaft displaced proximally and radially. Which of the following structures is primarily responsible for holding the volar ulnar base fragment in its anatomic position?
Explanation
Question 47
A 13-year-old girl presents with ankle pain after a twisting injury. Radiographs reveal a fracture of the anterolateral aspect of the distal tibial epiphysis. What is the normal sequence of closure of the distal tibial physis that predisposes her to this specific injury pattern?
Explanation
Question 48
A 65-year-old female presents with severe pain at the base of her thumb. Radiographs demonstrate advanced joint space narrowing and osteophytes at the trapeziometacarpal joint, as well as narrowing of the scaphotrapezialtrapezoid (STT) joint. According to the Eaton-Littler classification, what stage is her basal joint osteoarthritis?
Explanation
Question 49
A 28-year-old rugby player presents with an inability to actively flex the distal interphalangeal (DIP) joint of his ring finger after grabbing an opponent's jersey. The flexor digitorum profundus (FDP) tendon has retracted into the palm. Within what timeframe must this injury ideally be repaired to avoid tendon necrosis and fixed retraction?
Explanation
Question 50
A 45-year-old male is evaluated in the emergency department following a fall from a height. He sustained a severely comminuted pilon fracture with massive soft tissue swelling and hemorrhagic fracture blisters. The decision is made to place a spanning external fixator. What is the primary rationale for this staged approach ('span, scan, and plan')?
Explanation
Question 51
A 60-year-old woman complains of a painful bump on the dorsal aspect of her index finger DIP joint. Examination reveals a translucent nodule and grooving of the adjacent nail bed. Which of the following is the most critical surgical step to prevent recurrence if operative excision is chosen?
Explanation
Question 52
A 14-year-old boy presents after an ankle injury. Radiographs show a fracture line extending vertically through the epiphysis on the AP view, and extending posteriorly through the metaphysis on the lateral view. Which Salter-Harris classification functionally describes this fracture?
Explanation
Question 53
A 32-year-old man presents with a painful, swollen PIP joint after a sports injury. Examination reveals a volar PIP dislocation. Which of the following complications is most likely if the primary injured structure is not properly treated?
Explanation
Question 54
A 22-year-old athlete sustains a rotational ankle injury. Radiographs show a fracture of the proximal third of the fibula and widening of the medial clear space. What structure is highly at risk during surgical approach or from the injury itself in this specific fracture pattern?
Explanation
Question 55
A 55-year-old male with end-stage post-traumatic ankle osteoarthritis is undergoing an ankle arthrodesis. To optimize his postoperative gait, what is the ideal position for fusing the tibiotalar joint?
Explanation
Question 56
Which of the following physical examination tests is considered most accurate for intraoperative evaluation of syndesmotic instability following internal fixation of a lateral malleolus fracture?
Explanation
Question 57
A 35-year-old manual laborer presents with progressive wrist pain 5 years after an untreated scaphoid fracture. Radiographs show scaphoid nonunion advanced collapse (SNAC). The radiocarpal joint shows radioscaphoid arthritis, and there is narrowing of the capitolunate joint. However, the radiolunate joint is spared. Why is the radiolunate joint typically preserved in advanced SNAC and SLAC wrists?
Explanation
Question 58
A 25-year-old male sustains a proximal phalanx shaft fracture of the middle finger with apex volar angulation. Which two muscle groups are primarily responsible for creating this characteristic deformity?
Explanation
Question 59
A 58-year-old woman presents with severe hand pain. Radiographs demonstrate central erosions of the PIP and DIP joints with a characteristic 'gull-wing' appearance. Rheumatoid factor and anti-CCP antibodies are negative. What cytokine is most strongly implicated in the pathogenesis of the cartilage destruction in this condition?
Explanation
Question 60
A 9-year-old boy sustains a severe crush injury to his distal femoral physis (Salter-Harris V). Two years later, he is noted to have a significant leg length discrepancy and angular deformity due to a physeal bar. Which of the following is an absolute contraindication to physeal bar resection?
Explanation
Question 61
A 40-year-old female experiences an inversion injury to her ankle. Radiographs show a transverse fracture of the lateral malleolus at the level of the joint line, and a vertical fracture of the medial malleolus. According to the Lauge-Hansen classification, what is the mechanism of injury?
Explanation
Question 62
In a patient presenting with an irreducible fracture-dislocation of the ankle, radiographs show the fibula displaced behind the posterior tubercle of the tibia. Attempts at closed reduction in the emergency department are unsuccessful. What is this specific injury pattern called?
Explanation
Question 63
A 10-year-old falls on an outstretched hand, sustaining a Salter-Harris II fracture of the distal radius. According to the standard biomechanics of this injury pattern, where does the periosteum typically remain intact?
Explanation
Question 64
During surgical repair of an acute ankle syndesmotic disruption, the surgeon identifies the most important ligamentous stabilizer of the distal tibiofibular joint, which contributes to over 40% of its ultimate strength. Which ligament is this?
Explanation
Question 65
A 24-year-old male is diagnosed with a stage III perilunate dislocation according to Mayfield's classification. Which intercarpal ligamentous connection or joint is disrupted at this stage?
Explanation
Question 66
A 14-year-old boy presents with ankle pain after an external rotation injury sustained while playing soccer. Radiographs reveal a Salter-Harris III fracture of the anterolateral distal tibia. Which of the following structures is biomechanically responsible for avulsing this fracture fragment?
Explanation
Question 67
A 28-year-old male presents with severe pain at the base of his right thumb after punching a wall. Radiographs reveal a 3-part, Y-shaped intra-articular fracture of the first metacarpal base. During surgical planning for this Rolando fracture, understanding the deforming forces is critical. Which of the following deforming forces is correctly paired with the displacement of the first metacarpal shaft fragment?
Explanation
Question 68
A 45-year-old male sustains an ankle injury during a fall. Radiographs show widening of the medial clear space and a proximal fibular fracture, but no lateral malleolus fracture at the ankle level. According to the Lauge-Hansen Pronation-External Rotation (PER) classification, which of the following structures is injured last in the sequence?
Explanation
Question 69
A 13-year-old boy presents with severe right ankle pain following an external rotation injury while playing soccer. CT imaging reveals an epiphyseal fracture of the distal tibia. The fracture pattern appears as a sagittal fracture line on the AP view and a coronal fracture line on the lateral view. How is this specific fracture pattern categorized according to the Salter-Harris (SH) classification on these distinct imaging planes?
Explanation
Question 70
A 65-year-old female with advanced osteoarthritis of her right middle finger DIP joint presents with a painful, transilluminating dorsal nodule over the joint and grooving of her fingernail. Aspiration and corticosteroid injection have failed. She is scheduled for surgical excision. To minimize the risk of recurrence, which of the following steps is most critical during the surgical procedure?
Explanation
Question 71
A 35-year-old male falls 15 feet from a ladder, sustaining a closed, severely comminuted tibial pilon fracture. On presentation, his ankle exhibits massive soft tissue swelling and multiple fracture blisters. What is the most appropriate initial management for this patient to minimize catastrophic soft tissue complications?
Explanation
Question 72
A 14-year-old female presents after an acute ankle twisting injury. Radiographs show a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis, with 3 mm of displacement. Which of the following ligaments is primarily responsible for avulsing this fracture fragment?
Explanation
Question 73
A 24-year-old male complains of deep radial-sided wrist pain 3 months after falling onto an outstretched hand. Initial radiographs at the time of injury were read as normal. Current MRI shows a displaced scaphoid proximal pole fracture with signs of avascular necrosis. The vulnerability of the proximal pole to ischemia is due to its retrograde blood supply, which primarily arises from branches entering the scaphoid at which location?
Explanation
Question 74
A 58-year-old male with end-stage post-traumatic ankle osteoarthritis complains of daily, severe pain that limits his ambulation. He elects to undergo an open ankle arthrodesis. To ensure the most energy-efficient gait and to limit the breakdown of adjacent hindfoot joints, what is the optimal position for the tibiotalar fusion?
Explanation
Question 75
A 6-year-old girl sustained a distal femoral Salter-Harris II fracture 18 months ago. Recent scanograms demonstrate a 2.5 cm leg length discrepancy and 15 degrees of progressive valgus deformity. An MRI maps an osseous physeal bar occupying 40% of the cross-sectional area of the central physis. What is the most appropriate definitive management for this patient?
Explanation
None
