ABOS Part I Review: Tibia Fractures, IM Nailing & Compartment Syndrome Management | Part 22231

Key Takeaway
Tibia fracture management involves accurate classification (Gustilo-Anderson, Tscherne, AO/OTA), appropriate imaging like CT scans for intra-articular extension, and surgical stabilization, often with intramedullary nailing. Critical considerations include preventing and managing complications such as acute compartment syndrome, vascular injury, and non-union, with specific techniques like blocking screws and suprapatellar approaches.
ABOS Part I Review: Tibia Fractures, IM Nailing & Compartment Syndrome Management | Part 22231
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 28-year-old male presents to the emergency department after a high-energy motor vehicle collision, sustaining a closed midshaft diaphyseal tibia fracture. He is hemodynamically stable, and initial neurovascular examination is intact. Given the epidemiology and anatomical considerations of high-energy tibia fractures, which of the following statements is most accurate?
Explanation
Correct Answer: D
Explanation:
The case states that high-energy mechanisms are frequently associated with comminution, segmental defects, significant soft tissue compromise, and a higher propensity for open fractures (up to 30-40% in some series). It also notes a bimodal distribution, affecting young, active males involved in high-energy trauma. This directly supports option D.
- Option A is incorrect: While elderly individuals are affected by lower-energy falls, the bimodal distribution includes young, active males involved in high-energy trauma, which is the context of this question. The overall incidence is 16.9 per 100,000 person-years, but high-energy mechanisms are distinct.
- Option B is incorrect: The main blood supply to the tibial diaphysis is primarily from the nutrient artery (a branch of the posterior tibial artery). While periosteal vessels contribute, especially after trauma or reaming, the nutrient artery is the primary supply, and damage to it in high-energy injuries can impair healing.
- Option C is incorrect: The case explicitly states, 'The tibia has a precarious soft tissue envelope, particularly on its anteromedial surface, where it is largely subcutaneous.' This limited soft tissue coverage predisposes to open fractures and wound healing complications.
- Option E is incorrect: The case states, 'The tibia is the primary weight-bearing bone of the lower leg.' The fibula runs parallel and provides stability to the ankle joint, but is not the primary weight-bearing bone. While its integrity affects load sharing and rotational stability, its primary biomechanical importance is at the ankle and knee, not as the primary weight-bearer for the lower leg.
Question 2
A 35-year-old construction worker sustains a high-energy closed midshaft tibia fracture after a fall from scaffolding. On presentation, he complains of severe pain, especially with passive dorsiflexion of the toes. His leg is tense to palpation, and sensation in the first web space is diminished. Which of the following neurovascular structures is most likely compromised in this scenario, and what is the immediate management?
Explanation
Correct Answer: C
Explanation:
The clinical presentation of severe pain with passive stretch, tense compartment, and diminished sensation in the first web space (which is innervated by the deep peroneal nerve) are classic signs of acute compartment syndrome in the anterior compartment. The deep peroneal nerve and anterior tibial artery run in the anterior compartment. The case explicitly states that compartment syndrome is a surgical emergency requiring emergent fasciotomy.
- Option A is incorrect: The superficial peroneal nerve innervates the dorsum of the foot (except the first web space) and runs in the lateral compartment. While it can be injured, the specific symptoms point more strongly to the anterior compartment. Emergent surgical exploration for nerve repair is not the immediate management for compartment syndrome.
- Option B is incorrect: The posterior tibial artery runs in the deep posterior compartment. While vascular injury is a concern in high-energy trauma, the symptoms described are more indicative of compartment syndrome than a direct arterial transection, and emergent fasciotomy takes precedence over diagnostic imaging if compartment syndrome is clinically evident.
- Option D is incorrect: The tibial nerve runs in the deep posterior compartment. While nerve injury can occur, the constellation of symptoms (pain with passive stretch, tense compartment, specific sensory deficit) points to compartment syndrome, which requires immediate surgical intervention, not just observation.
- Option E is incorrect: The peroneal artery runs in the deep posterior compartment. Similar to option B, while vascular injury is a risk, the immediate concern with these symptoms is compartment syndrome, which requires fasciotomy, not just provisional fixation and vascular repair (unless a definitive vascular injury is confirmed and contributing to ischemia, which is not the primary presentation here).
Question 3
A 62-year-old male presents with a Gustilo-Anderson Type IIIA open midshaft tibia fracture after being struck by a car. He has multiple other injuries, including a closed head injury and a pelvic fracture, but is hemodynamically stable after initial resuscitation. Based on the case guidelines, what is the most appropriate initial management strategy for his tibia fracture?
Explanation
Correct Answer: C
Explanation:
The case explicitly states, 'For Gustilo I, II, IIIA fractures, thorough surgical debridement of all contaminated and devitalized tissue is paramount. Pulsatile lavage. Repeat debridement ('second look') after 24-48 hours may be necessary.' It also highlights 'Damage Control Orthopedics (DCO): For unstable polytrauma patients or those with severe soft tissue swelling/compromise, provisional external fixation is performed first. Definitive fixation (usually IM nailing) is delayed until the patient is physiologically stable and soft tissue swelling has subsided (typically 5-10 days, but can be longer).' Given the Gustilo IIIA open fracture and polytrauma status, emergent debridement and provisional external fixation are the most appropriate initial steps.
- Option A is incorrect: While early total care (ETC) is an option for isolated closed fractures, for open fractures, especially in polytrauma patients, the priority is debridement and provisional stabilization (DCO) to manage contamination and systemic inflammatory response, delaying definitive internal fixation.
- Option B is incorrect: Non-operative management is generally reserved for non-displaced or minimally displaced closed fractures, which is rare in high-energy trauma, and is absolutely contraindicated for open fractures.
- Option D is incorrect: While plate osteosynthesis can be used in some open fractures, it is not the primary initial management for a Gustilo IIIA fracture, which requires debridement and often provisional external fixation first. Autogenous bone grafting is typically delayed until soft tissue healing is complete or for non-unions.
- Option E is incorrect: Delaying all surgical intervention for an open fracture is contraindicated. Emergent debridement is critical to reduce infection risk.
Question 4
A 40-year-old male presents with a high-energy midshaft tibia fracture. Pre-operative planning is underway. The trauma surgeon notes a concern for potential intra-articular extension at the knee, as well as significant comminution not fully appreciated on plain radiographs. Which imaging modality is most appropriate to address these specific concerns?
Explanation
Correct Answer: C
Explanation:
The case states that a CT scan is 'Useful for identifying subtle intra-articular extension at the knee or ankle, which can influence fixation strategy' and for 'Detailed assessment of comminution, bone loss, and fracture geometry.' This directly addresses both concerns mentioned in the vignette.
- Option A is incorrect: ABI is used to assess vascular status, not fracture morphology or intra-articular extension.
- Option B is incorrect: MRI is rarely indicated acutely for fracture assessment but may be useful for ligamentous injury assessment at the knee/ankle if suspected post-reduction. It is not the primary modality for bone detail or comminution in the acute setting.
- Option D is incorrect: Conventional angiography is indicated if there is suspicion of vascular injury, not for assessing intra-articular extension or comminution.
- Option E is incorrect: While oblique views on plain radiographs can provide more information than AP/lateral views, they are still limited in assessing subtle intra-articular extension or complex comminution compared to a CT scan.
Question 5
During intramedullary nailing of a midshaft tibia fracture, the surgeon is preparing the entry point. The image below demonstrates a common approach for proximal tibial entry. Which of the following statements accurately describes a key consideration for this step?

Explanation
Correct Answer: C
Explanation:
The case states, 'The choice of entry point is critical to avoid malalignment (especially apex anterior/posterior deformity or valgus/varus) and iatrogenic injury.' It further specifies, 'Once the entry point is identified on the proximal tibia (usually medial to the lateral tibial spine and lateral to the medial tibial spine, aligning with the intercondylar notch), an awl or drill is used to open the cortex. The goal is to align with the central axis of the medullary canal in both AP and lateral planes.' This directly supports option C.
- Option A is incorrect: The entry point is usually medial to the lateral tibial spine and lateral to the medial tibial spine, aligning with the intercondylar notch, not lateral to the lateral tibial spine. Splitting the patellar tendon centrally or paratendinously is a common approach.
- Option B is incorrect: While suprapatellar nailing is a technique that may reduce anterior knee pain, the case describes it as 'a more recent technique' and does not state it is preferred in all cases. Patellar ligament splitting is also a common approach.
- Option D is incorrect: Entry point preparation (opening the cortex) always precedes reaming. Reaming is the sequential enlargement of the medullary canal after the entry point is established.
- Option E is incorrect: The entry point is made on the proximal tibia, typically through or adjacent to the patellar tendon, not through the medial collateral ligament, which is a knee stabilizer.
Question 6
A 50-year-old male with a closed, comminuted midshaft tibia fracture is undergoing intramedullary nailing. The surgeon is debating between reamed and unreamed nailing. The patient has no other significant comorbidities, and soft tissue swelling is minimal. Based on the case, which approach is generally preferred for this type of fracture in this patient, and why?
Explanation
Correct Answer: B
Explanation:
The case states, 'Reamed intramedullary nailing is the gold standard for diaphyseal tibia fractures due to superior union rates, lower reoperation rates, and faster time to union compared to plating or casting for most patterns.' Under 'Reamed Nailing,' it lists advantages: 'Maximizes nail-to-bone contact, allowing for a larger diameter and stiffer nail, which provides greater rotational and bending stability. Enhances primary callus formation.' This aligns with the scenario of a closed, comminuted fracture in a healthy patient where stability and union are paramount.
- Option A is incorrect: While unreamed nailing does preserve endosteal blood supply and has a lower risk of fat embolism, the case indicates that reamed nailing is generally preferred for closed fractures due to superior stability and union rates.
- Option C is incorrect: Unreamed nailing is indeed preferred for Gustilo II and IIIA open fractures to avoid spreading contamination, but the patient in the vignette has a closed fracture.
- Option D is incorrect: The case mentions that anterior knee pain is a common complication of IM nailing, but it does not state that reamed nailing specifically is associated with lower rates of anterior knee pain. In fact, suprapatellar nailing techniques are discussed as potentially reducing this incidence, not reaming itself.
- Option E is incorrect: The case does not suggest that unreamed nailing is less technically demanding or faster. The choice between reamed and unreamed is based on biomechanical and biological considerations, not ease of performance.
Question 7
A 22-year-old male presents with a high-energy midshaft tibia fracture with significant comminution and a wide medullary canal, making stable reduction challenging. The surgeon decides to use an adjunct technique to improve alignment and prevent malreduction during intramedullary nailing. The image below illustrates a technique that could be employed in this situation. Which of the following adjuncts is most appropriate for this scenario?

Explanation
Correct Answer: C
Explanation:
The case states, 'Blocking screws (Poller Screws): Small cortical screws placed adjacent to the IM nail track to guide the nail into the correct position, preventing malalignment in specific planes (e.g., apex anterior/posterior, valgus/varus). Especially useful for metadiaphyseal fractures or wide medullary canals.' This directly matches the clinical scenario of a wide medullary canal and challenging reduction.
- Option A is incorrect: The case states, 'Cerclage Wires: Rarely used for midshaft diaphyseal fractures due to disruption of periosteal blood supply, but may be considered for large butterfly fragments that are difficult to reduce or stabilize. Use sparingly and with caution.' This suggests they are not the most appropriate primary adjunct for general comminution and wide canals.
- Option B is incorrect: Bone grafting is typically used for bone loss, delayed union, or non-union, often delayed until soft tissue healing is complete. It is not an adjunct for achieving acute reduction and alignment during IM nailing.
- Option D is incorrect: A temporary external fixator can assist with reduction, but it is typically used for provisional stabilization in damage control orthopedics or severe open fractures, not as a definitive fixation method in this context, nor is it the specific adjunct for guiding the nail in a wide canal.
- Option E is incorrect: Plate osteosynthesis is an alternative fixation method, not an adjunct to IM nailing, and is generally a secondary option for midshaft diaphyseal tibia fractures.
Question 8
A 48-year-old male undergoes intramedullary nailing for a high-energy closed midshaft tibia fracture. Post-operatively, he develops increasing pain, swelling, and paresthesia in the foot. On examination, his foot is cool, and pedal pulses are diminished. Which of the following is the most critical early complication to rule out, and what is its immediate management?
Explanation
Correct Answer: D
Explanation:
The symptoms of increasing pain, swelling, paresthesia, a cool foot, and diminished pedal pulses are highly suggestive of acute vascular compromise (e.g., laceration, transection, or thrombosis of major arteries). The case lists 'Vascular Injury' as an early complication, describing it as 'Laceration, transection, or thrombosis of major arteries (anterior/posterior tibial, peroneal). Presents as pulselessness, pallor, cold extremity.' The management is 'Emergent vascular surgery consultation and repair (bypass or primary repair).' While compartment syndrome can present similarly, the diminished pulses and cool extremity strongly point to a primary vascular injury requiring immediate repair to prevent limb loss.
- Option A is incorrect: DVT typically presents with swelling and pain, but usually not with a cool extremity or diminished pulses, which are signs of arterial insufficiency.
- Option B is incorrect: FES presents with a triad of respiratory insufficiency, neurological dysfunction, and petechial rash, not primarily with localized limb ischemia.
- Option C is incorrect: While acute compartment syndrome is a critical early complication, the presence of diminished pulses and a cool extremity makes vascular injury a more immediate and limb-threatening concern that must be addressed first. Compartment syndrome can be secondary to vascular injury, but the primary issue here is arterial flow.
- Option E is incorrect: Infection is a later complication unless it's an open fracture, and its acute presentation would not typically include a cool extremity and diminished pulses.
Question 9
A 30-year-old male undergoes intramedullary nailing for a high-energy midshaft tibia fracture. Six months post-operatively, he complains of persistent pain around the knee, particularly with kneeling and stair climbing. Radiographs confirm union of the fracture, and the image below shows a typical final IM nail construct. What is the most likely diagnosis for his persistent knee pain, and what is the recommended management?
Explanation
Correct Answer: C
Explanation:
The case specifically addresses 'Anterior Knee Pain Post-IM Nailing' as a common late complication, stating, 'Up to 50% of patients experience anterior knee pain after IM nailing of the tibia.' It describes the etiology as multifactorial and the management as 'While common, hardware removal for symptomatic pain is often effective, but should be delayed until complete union.' The vignette describes persistent knee pain after confirmed union, which is characteristic of this complication.
- Option A is incorrect: Non-union implies failure of fracture healing, but the vignette states radiographs confirm union.
- Option B is incorrect: Malunion implies the fracture healed in an unacceptable position, which is not indicated by the symptoms of knee pain after union.
- Option D is incorrect: Hardware failure would typically be associated with pain at the fracture site or loss of reduction, and the radiographs confirm union, making hardware failure less likely to be the primary cause of isolated anterior knee pain.
- Option E is incorrect: CRPS is a complex pain syndrome with distinct features (e.g., allodynia, trophic changes) not fully described in the vignette, and while possible, anterior knee pain post-IM nailing is a much more common and specific diagnosis in this context.
Question 10
A 55-year-old female with a high-energy midshaft tibia fracture treated with reamed intramedullary nailing is 8 weeks post-operative. Radiographs show early callus formation, and she has good pain control. According to the post-operative rehabilitation protocols, what is the most appropriate progression for her weight-bearing status at this stage?
Explanation
Correct Answer: C
Explanation:
The case's 'Phase 2 Early Mobilization & Progressive Loading (Weeks 6-12)' section states, 'Weight Bearing: Progress from NWB/TDWB to PWB/WBAT as radiological signs of healing (early callus formation) become evident and pain allows. Regular follow-up radiographs (every 4-6 weeks) guide progression.' The patient is 8 weeks post-op with early callus, fitting this phase.
- Option A is incorrect: Continuing strict NWB until full cortical bridging is too conservative for this stage, especially with early callus formation and good pain control.
- Option B is incorrect: Initiating FWBAT immediately is too aggressive. FWBAT is typically achieved later, once clinical and radiographic union are confirmed (Phase 3).
- Option D is incorrect: Plyometric exercises are part of 'Phase 3 Advanced Strengthening & Return to Activity (Weeks 12+)' and are too aggressive for 8 weeks post-op.
- Option E is incorrect: Removing all assistive devices and encouraging independent ambulation is part of later stages of rehabilitation (Phase 3), after significant progression in strength and confidence.
Question 11
A 70-year-old male with a history of smoking and peripheral vascular disease sustains a high-energy Gustilo-Anderson Type IIIA open midshaft tibia fracture. He undergoes emergent debridement and provisional external fixation. Based on the summary of key literature and guidelines, which of the following statements regarding his definitive management and potential complications is most accurate?
Explanation
Correct Answer: C
Explanation:
The 'Summary of Key Literature / Guidelines' section states, 'Exchange nailing is a highly effective treatment for aseptic hypertrophic non-unions.' This is a well-established principle in orthopedic trauma.
- Option A is incorrect: While unreamed nailing is often favored for Gustilo IIIA/B open fractures to minimize infection spread and preserve endosteal blood supply, the case states that 'Reamed nailing generally results in higher union rates and stronger constructs than unreamed nailing, particularly in closed and Gustilo I/II open fractures.' For Gustilo IIIA/B, the choice is more nuanced, and unreamed is chosen for infection control, not necessarily for maximizing stability and union rates compared to reamed nailing in general. Reamed nailing is the gold standard for diaphyseal tibia fractures overall, but unreamed has specific indications for open fractures.
- Option B is incorrect: The case states, 'For Gustilo IIIB/IIIC fractures, early definitive soft tissue coverage (within 7 days) by plastic surgery has been shown to reduce infection rates and improve outcomes.' Therefore, delaying beyond 7 days would increase, not reduce, infection rates.
- Option D is incorrect: The case states, 'Prophylactic grafting for highly comminuted open fractures is controversial but may be considered for large segmental defects.' It is not routinely indicated.
- Option E is incorrect: The case states, 'For polytrauma patients or those with severe soft tissue swelling, provisional external fixation followed by delayed definitive internal fixation (typically within 5-10 days) is supported by evidence to reduce systemic inflammatory response and improve outcomes ('early appropriate care').' This is Damage Control Orthopedics (DCO), which is often preferred for open fractures, especially in polytrauma patients, over Early Total Care (ETC).
Question 12
A 38-year-old male presents with a high-energy proximal tibial diaphyseal fracture. His medical history includes Type 2 Diabetes Mellitus (HbA1c 6.8%) and a 15 pack-year smoking history.
Considering these comorbidities, which of the following is the MOST significant anticipated complication directly related to the patient's biological healing cascade and perioperative risk?
Explanation
Correct Answer: C
The case explicitly states that the patient's Type 2 Diabetes Mellitus and 15 pack-year smoking history significantly elevate the risk of delayed union, nonunion, and surgical site infection. Diabetes inherently alters bone microarchitecture and impairs cellular responses to trauma, while smoking induces profound peripheral vasoconstriction and tissue hypoxia. These factors directly compromise the biological healing cascade. While other complications listed are possible in trauma patients, delayed union or nonunion is the most directly and significantly impacted by the patient's specific comorbidities as described in the case.
Question 13
The patient's right lower extremity exhibits gross clinical deformity, significant non-pitting edema, and ecchymosis. The skin integrity is closed, but there is deep muscle contusion and moderate to severe abrasion. The compartments are tense but compressible. Pain with passive stretch of the ischemic muscles is noted but not deemed disproportionate.
Based on these findings, what is the most appropriate Tscherne classification for the closed soft tissue injury, and what is the critical diagnostic threshold for acute compartment syndrome in this patient?
Explanation
Correct Answer: C
The case describes the soft tissue envelope as exhibiting signs of severe contusion, deep muscle contusion, and moderate to severe abrasion, which is explicitly stated as consistent with a Tscherne Grade 2 closed soft tissue injury. Regarding acute compartment syndrome, the case specifies that a Delta P calculation (diastolic blood pressure minus intracompartmental pressure) of less than 30 mmHg would serve as the absolute indication for emergent four-compartment fasciotomies. Therefore, option C accurately reflects both the Tscherne classification and the critical diagnostic threshold for compartment syndrome as detailed in the case.
Question 14
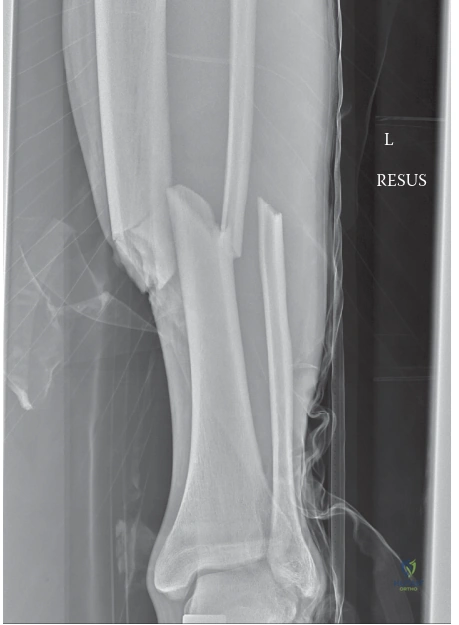
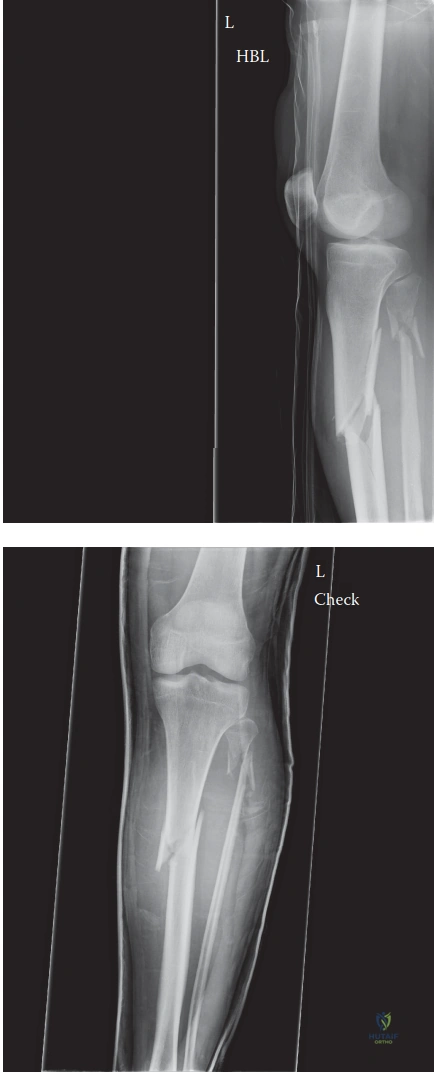
Review the provided radiograph of the patient's right lower extremity.
Based on the case and the provided image, which of the following best describes the fracture pattern and associated deformity?
Explanation
Correct Answer: C
The case explicitly states: 'Radiographic analysis of the right lower extremity revealed a severely displaced, comminuted fracture of the proximal third of the tibial diaphysis. The fracture pattern exhibited a dominant oblique configuration with a large, laterally displaced butterfly fragment... with significant apex anterior (procurvatum) and apex lateral (valgus) angulation.' The provided image clearly demonstrates these features, showing a fracture in the proximal third of the tibia with multiple fragments (comminuted), an oblique component, and the characteristic apex anterior and valgus angulation. Options A, B, D, and E describe different fracture locations, patterns, or severities that are inconsistent with both the image and the detailed description in the case.
Question 15
The patient's proximal tibial diaphyseal fracture exhibits significant apex anterior (procurvatum) and apex lateral (valgus) angulation.
Which of the following anatomical structures is primarily responsible for the apex anterior (procurvatum) deformity observed in proximal third tibial fractures?
Explanation
Correct Answer: C
The case specifically addresses the deforming forces in proximal third tibial fractures: 'This specific deformity pattern is classic for proximal third tibial fractures and is driven by the unopposed pull of the extensor mechanism (quadriceps via the patellar tendon) on the proximal fragment, drawing it into extension, while the pes anserinus and iliotibial band exert variable varus/valgus and rotational forces.' The extensor mechanism, primarily through the patellar tendon, pulls the proximal fragment anteriorly, creating the apex anterior (procurvatum) deformity. The other options are either not the primary deforming force for procurvatum or contribute more to other deformities (e.g., pes anserinus and iliotibial band for varus/valgus).
Question 16
Following plain radiographs, a dedicated computed tomography (CT) scan of the right knee and proximal tibia with fine axial cuts and multiplanar reconstructions was ordered for this patient.
What is the MOST critical reason for obtaining a CT scan in a high-energy proximal third tibial shaft fracture, even if plain radiographs appear to show an extra-articular injury?
Explanation
Correct Answer: C
The case emphasizes the importance of the CT scan: 'While plain radiographs provide the macroscopic architecture of the diaphyseal injury, they are notoriously insensitive for detecting occult intra-articular extension into the tibial plateau. Literature indicates that up to 20% to 30% of high-energy proximal third tibial shaft fractures possess an unrecognized coronal or sagittal split propagating into the articular surface. The presence of an intra-articular component drastically alters the surgical algorithm...' Therefore, the primary and most critical reason for the CT scan in this context is to rule out occult intra-articular extension, which would fundamentally change the surgical approach. While templating (E) is a benefit, it's not the most critical reason for the CT in terms of altering the fundamental treatment strategy for an articular injury.
Question 17
The patient has a closed, comminuted proximal third tibial diaphyseal fracture (AO/OTA 42-B3, Tscherne Grade 2) and a history of Type 2 Diabetes and smoking. Surgical stabilization is indicated.
Considering the patient's fracture characteristics and comorbidities, which surgical fixation method is generally considered the gold standard and offers the most biomechanical advantages for this specific injury, while mitigating risks associated with his medical history?
Explanation
Correct Answer: D
The case explicitly states: 'Intramedullary Nailing (IMN) remains the gold standard for tibial diaphyseal fractures. It is a load-sharing device that preserves the extraosseous blood supply, offers superior biomechanical stability against bending and torsional forces, and allows for earlier weight-bearing.' It also discusses the disadvantages of plating (MIPPO or ORIF with plates) in this context, noting that 'plating the tibia, particularly on the subcutaneous anteromedial surface, requires significant soft tissue stripping... and introduces bulky hardware under a traumatized soft tissue envelope, significantly increasing the risk of wound dehiscence and deep infection.' This risk is particularly relevant for a diabetic, smoking patient with impaired healing. Non-operative management (A) is contraindicated for this high-energy, displaced fracture, and external fixation (B) is generally reserved for damage control or severe open fractures, not definitive treatment in a stable, closed injury.
Question 18
The surgical plan for this patient involves a Suprapatellar Intramedullary Nailing technique.
What is the primary biomechanical advantage of utilizing a suprapatellar approach for intramedullary nailing of a proximal tibial diaphyseal fracture, compared to a traditional infrapatellar approach?
Explanation
Correct Answer: C
The case highlights the key advantage of the suprapatellar approach: 'The critical advantage of the suprapatellar approach is patient positioning. The limb is positioned with the knee in a semi-extended posture, resting on a sterile bump at approximately 15 to 20 degrees of flexion. This semi-extended position dramatically reduces the tension on the extensor mechanism, neutralizing the primary deforming force that causes procurvatum.' This directly addresses the common challenge of apex anterior deformity in proximal tibial nailing. Options A, B, D, and E are incorrect; distal interlocking is not inherently easier, blocking screws are still often necessary, direct visualization of the fracture is not achieved, and it does not significantly reduce the risk of compartment syndrome compared to other approaches.
Question 19
During the intramedullary nailing of this patient's proximal tibial fracture, blocking screws (Poller screws) were strategically placed in the proximal fragment.
To prevent the classic apex anterior (procurvatum) and valgus malalignment, where should the blocking screws be placed in the proximal fragment relative to the anticipated nail trajectory?
Explanation
Correct Answer: B
The case provides precise guidance on blocking screw placement: 'To prevent the classic valgus and procurvatum deformity, two blocking screws were placed in the proximal fragment. One screw was placed in the posterior half of the proximal fragment (viewed laterally) to block the nail from translating posteriorly, thereby preventing procurvatum. A second screw was placed in the lateral half of the proximal fragment (viewed on AP) to prevent the nail from translating laterally, thereby preventing valgus.' Blocking screws are placed on the concave side of the deformity to guide the nail centrally. For procurvatum (apex anterior), the nail tends to go posterior, so a posterior screw blocks this. For valgus (apex lateral), the nail tends to go lateral, so a lateral screw blocks this.
Question 20
During the intramedullary nailing procedure, sequential flexible reaming was performed.
What is a recognized benefit of sequential flexible reaming during intramedullary nailing of a tibial diaphyseal fracture?
Explanation
Correct Answer: C
The case states: 'Sequential flexible reaming was performed in 0.5-millimeter increments. Reaming generates autologous bone graft (osteogenic reamings) that is deposited at the fracture site, promoting secondary bone healing.' This is a well-known biological advantage of reamed nailing. Reaming does not directly reduce the fracture (A), it can actually increase the risk of fat embolization (B), it allows for a larger diameter nail (D), and fluoroscopic guidance is still essential (E).
Question 21
Following intramedullary nailing for the proximal tibial diaphyseal fracture, the patient is in the immediate postoperative period.
What is the MOST critical immediate postoperative concern that requires extreme vigilance and hourly monitoring in this patient?
Explanation
Correct Answer: D
The case explicitly states: 'The immediate postoperative period requires extreme vigilance for the development of delayed acute compartment syndrome. The trauma of reaming and nail insertion introduces additional volume and inflammatory mediators into the closed fascial spaces. The patient was admitted to the orthopedic trauma unit with strict instructions for hourly neurovascular and compartment checks for the first 24 hours.' While DVT, SSI, delayed union, and hardware failure are all potential complications, delayed acute compartment syndrome is the most immediate, life-threatening, and limb-threatening complication requiring hourly monitoring in the immediate postoperative period, as emphasized in the case.
Question 22
A 28-year-old male presents to the trauma center after a high-energy motor vehicle collision, sustaining an open right tibial diaphyseal fracture. Despite initial hemodynamic stability and palpable distal pulses, he develops excruciating, unremitting pain in his right lower leg, rated 10/10 on the VAS, unresponsive to high-dose opioids. Clinical examination reveals a tense, 'wood-hard' anterior compartment. Which of the following is the MOST sensitive and specific clinical finding for diagnosing acute compartment syndrome in this patient?
Explanation
Correct Answer: C
Explanation:
The most sensitive and specific clinical finding for diagnosing acute compartment syndrome (ACS) is severe pain with passive stretch of the muscles within the affected compartment, which is disproportionate to the injury and unrelieved by analgesia. In this case, passive plantarflexion of the ankle and passive flexion of the great toe selectively stretch the muscles of the anterior compartment (tibialis anterior, extensor hallucis longus, extensor digitorum longus), eliciting excruciating pain. This is a hallmark sign of ACS.
- A. Absence of distal pulses (dorsalis pedis and posterior tibial): Pulselessness is a very late and unreliable sign of ACS. Peripheral pulses are often maintained until intra-compartmental pressure exceeds systolic arterial pressure, which signifies irreversible damage. The case explicitly states that distal pulses remained robust and palpable, highlighting this pitfall.
- B. Pallor and poikilothermia of the affected limb: These are classic signs of acute arterial occlusion/ischemia, not typically ACS. In ACS, the limb is often warm due to the hyperemic response of early tissue distress, and pallor is not a primary feature until very late stages.
- D. Paresthesia in the distribution of the superficial peroneal nerve: While sensory changes (paresthesia, diminished two-point discrimination) are important signs of nerve ischemia in ACS, they are generally considered less sensitive and specific than pain with passive stretch, and often represent a more advanced stage of nerve compromise. The case describes this as altered sensation progressing to early paresthesia, indicating it's an evolving sign.
- E. Gross deformity and crepitus at the fracture site: Gross deformity and crepitus are expected findings with a displaced tibial fracture. They are indicative of the fracture itself, not specifically acute compartment syndrome. While the fracture is the inciting event, these findings do not differentiate between a simple fracture and one complicated by ACS.
Question 23
The patient's clinical presentation, including escalating pain, tense compartments, and severe pain with passive stretch, led to a clinical diagnosis of acute compartment syndrome. Given the high-energy mechanism and open fracture, which of the following conditions would be the MOST critical to differentiate from acute compartment syndrome, and what specific finding in this case helped rule it out?
Explanation
Correct Answer: C
Explanation:
In the setting of high-energy trauma to an extremity, acute arterial occlusion is a limb-threatening emergency that must be rapidly differentiated from acute compartment syndrome. Both can present with severe pain and potential neurological deficits. However, the case explicitly states that the dorsalis pedis and posterior tibial pulses remained robust and palpable, and capillary refill was brisk (<2 seconds). This strongly rules out a major arterial occlusion as the primary pathology.
- A. Deep Vein Thrombosis (DVT); absence of Homan's sign: DVT typically presents with generalized swelling, dull aching pain, and erythema, usually developing over a longer period (hours to days) than the acute timeline of this injury. While Homan's sign is unreliable, the acute onset and localized compartment tenseness are inconsistent with DVT.
- B. Necrotizing Fasciitis; absence of crepitus and systemic toxicity: Necrotizing fasciitis is a severe soft tissue infection. While it causes severe pain, it is typically accompanied by systemic signs of sepsis (fever, tachycardia), crepitus (indicating gas-forming organisms), and hemorrhagic bullae, which were not present in this acute setting.
- D. Severe Fracture Pain; pain unresponsive to high-dose opioids and disproportionate to injury: While severe fracture pain is a differential, the key differentiating factor from ACS is that fracture pain is usually proportional to the injury and improves with immobilization and analgesia. The patient's pain was 'excruciating, unremitting,' '10/10 on the VAS,' and 'completely unrelieved' by high-dose opioids, which strongly points away from isolated fracture pain and towards ACS. However, this option describes a finding that confirms ACS rather than ruling out a critical differential.
- E. Peripheral Neuropathy; intact light touch sensation in multiple nerve distributions: Peripheral neuropathy is a chronic condition and not an acute traumatic differential. While nerve injury can occur with trauma, the initial intact sensation followed by rapid deterioration points to an acute ischemic process, not a pre-existing neuropathy.
Question 24
Given the patient's clear clinical signs of acute compartment syndrome, the decision was made to proceed directly to surgery without intra-compartmental pressure monitoring. However, in an equivocal case, such as an obtunded or polytraumatized patient, pressure monitoring would be indicated. Which of the following pressure measurements is the MOST reliable indicator for emergent fasciotomy?
Explanation
Correct Answer: C
Explanation:
The most reliable indicator for emergent fasciotomy, especially in equivocal cases or non-communicative patients, is the differential pressure (Delta P). Delta P is calculated as Diastolic Blood Pressure (DBP) minus the Intra-compartmental Pressure (ICP). A Delta P of less than 30 mmHg signifies inadequate tissue perfusion and is a widely accepted threshold for emergent fasciotomy. This metric accounts for the patient's systemic blood pressure, which is crucial because a hypotensive patient with a relatively low absolute compartment pressure can still be ischemic, while a hypertensive patient with a higher absolute compartment pressure might maintain adequate perfusion.
- A. Absolute intra-compartmental pressure greater than 30 mmHg: While often cited, relying solely on an absolute pressure threshold is a known pitfall. A patient with a DBP of 100 mmHg and an ICP of 35 mmHg (ΔP = 65 mmHg) may not require fasciotomy, whereas a patient with a DBP of 50 mmHg and an ICP of 25 mmHg (ΔP = 25 mmHg) is critically ischemic and requires intervention.
- B. Absolute intra-compartmental pressure greater than 40 mmHg: Similar to option A, this absolute threshold does not account for the patient's systemic blood pressure and is therefore less reliable than the Delta P.
- D. A Delta P (Systolic Blood Pressure - Intra-compartmental Pressure) less than 30 mmHg: While the concept of a differential pressure is correct, the standard and most widely accepted calculation for Delta P in the context of ACS uses Diastolic Blood Pressure, not Systolic Blood Pressure, as it more accurately reflects the pressure gradient for capillary perfusion.
- E. A Delta P (Mean Arterial Pressure - Intra-compartmental Pressure) less than 40 mmHg: While Mean Arterial Pressure (MAP) is a measure of overall perfusion, the established and validated threshold for Delta P in ACS specifically uses Diastolic Blood Pressure.
Question 25
The patient underwent emergent dual-incision four-compartment fasciotomy and unreamed intramedullary nailing. The case highlights the critical time sensitivity of acute compartment syndrome. Skeletal muscle can tolerate ischemia for approximately 4 hours without permanent damage. Between 4 and 8 hours, irreversible myonecrosis and peripheral nerve damage begin to occur. Beyond 8 hours, the damage is essentially complete. What is the primary cellular mechanism underlying irreversible damage in acute compartment syndrome?
Explanation
Correct Answer: B
Explanation:
The primary cellular mechanism underlying irreversible damage in acute compartment syndrome is the failure of the ATP-dependent Na+/K+ pump. As intra-compartmental pressure rises, it compromises capillary perfusion, leading to tissue ischemia and cellular hypoxia. Without adequate oxygen, cells cannot produce sufficient ATP through oxidative phosphorylation. The Na+/K+ pump, which actively transports sodium out of the cell and potassium into the cell, is highly ATP-dependent. Its failure leads to an accumulation of sodium and water inside the cell, causing intracellular swelling. This swelling further exacerbates the intra-compartmental pressure in a vicious cycle, ultimately leading to cell membrane rupture and myonecrosis.
- A. Excessive calcium influx leading to muscle hypercontracture and rigor mortis: While calcium dysregulation (influx of calcium) does occur in ischemic cells and contributes to muscle damage and hypercontracture, it is a downstream effect of the initial energy failure and membrane dysfunction, not the primary initiating mechanism of irreversible damage.
- C. Accumulation of lactic acid causing severe acidosis and enzyme denaturation: Lactic acid accumulation and acidosis are consequences of anaerobic metabolism during ischemia. While acidosis contributes to cellular dysfunction, the fundamental irreversible damage stems from the failure of ion pumps and subsequent cellular swelling and membrane integrity loss.
- D. Direct mechanical compression of muscle fibers leading to necrosis: While there is mechanical compression, the primary mechanism of damage is ischemic, not purely mechanical. The pressure impedes blood flow, leading to hypoxia, which then triggers the cellular cascade of pump failure and swelling.
- E. Reperfusion injury causing massive free radical production and inflammation: Reperfusion injury is a significant complication that occurs after fasciotomy when blood flow is restored to ischemic tissues. It involves the production of reactive oxygen species (free radicals) and inflammatory mediators, which can cause further tissue damage and systemic complications (e.g., rhabdomyolysis, acute kidney injury). However, it is not the mechanism of irreversible damage during the ischemic phase of ACS.
Question 26
The patient underwent a dual-incision four-compartment fasciotomy. The surgical image below shows a typical anterolateral incision for fasciotomy. During the anterolateral incision, which nerve is at greatest risk of iatrogenic injury, and where is it typically located?
Explanation
Correct Answer: C
Explanation:
During the anterolateral incision for fasciotomy, the superficial peroneal nerve is at greatest risk of iatrogenic injury. It typically exits the lateral compartment fascia to become subcutaneous in the distal third of the leg, approximately 10 to 12 cm proximal to the lateral malleolus. Care must be taken during the distal extension of the lateral compartment fascial release to identify and protect this nerve, as injury can lead to sensory loss over the lateral dorsum of the foot and potentially a painful neuroma.
- A. Tibial nerve; deep posterior compartment, posterior to the tibialis posterior muscle: The tibial nerve is located in the deep posterior compartment and is at risk during the posteromedial incision and deep posterior compartment release, not the anterolateral incision.
- B. Common peroneal nerve; wrapping around the fibular neck, proximal to the lateral compartment release: The common peroneal nerve is at risk during the proximal extension of the lateral compartment fascial release, particularly when incising near the fibular head. While important to protect, the superficial peroneal nerve is more commonly injured during the distal aspect of the anterolateral incision due to its superficial course.
- D. Deep peroneal nerve; running with the anterior tibial artery in the anterior compartment: The deep peroneal nerve is located within the anterior compartment. While it is important to avoid direct injury to this nerve during the anterior compartment release, it is generally less susceptible to iatrogenic injury from the fascial incision itself compared to the superficial peroneal nerve, which becomes subcutaneous.
- E. Saphenous nerve; in the subcutaneous tissue along the posteromedial aspect of the leg: The saphenous nerve is located in the subcutaneous tissue along the posteromedial aspect of the leg and is at risk during the posteromedial incision, not the anterolateral incision.
Question 27
Following the emergent four-compartment fasciotomy, the open tibial fracture (Gustilo-Anderson Type II, OTA/AO 42-B3) required stabilization. The patient was physiologically stable. The surgical team opted for unreamed statically locked intramedullary nailing. Which of the following is the MOST compelling reason for choosing unreamed intramedullary nailing over spanning external fixation in this specific clinical scenario?
Explanation
Correct Answer: B
Explanation:
In a physiologically stable patient with an open tibial fracture and acute compartment syndrome, unreamed intramedullary nailing offers several advantages over external fixation. It provides superior biomechanical stability, which is crucial for fracture healing and allows for earlier mobilization. Furthermore, it avoids the complications associated with external fixator pin tracts, such as pin-tract infections, which can complicate subsequent definitive soft tissue coverage and potentially lead to osteomyelitis. The case explicitly states that modern trauma protocols often favor early definitive fixation with an unreamed IMN if the patient is physiologically stable, as it provides superior biomechanical stability and avoids pin-tract infections.
- A. External fixation is contraindicated in open fractures due to high infection rates: External fixation is a valid and often preferred method for initial stabilization of open fractures, especially in unstable patients (damage control orthopedics). While pin-tract infections are a concern, it is not an absolute contraindication for open fractures.
- C. Reamed intramedullary nailing is preferred for open fractures to enhance fracture healing: Reaming the medullary canal can further disrupt endosteal blood supply and potentially increase intra-compartmental pressures, especially in the context of recent fasciotomy. Therefore, unreamed nailing is generally preferred in open fractures and those complicated by ACS to minimize additional soft tissue and vascular insult.
- D. External fixation would further elevate intra-compartmental pressures after fasciotomy: External fixation itself does not typically elevate intra-compartmental pressures after a successful fasciotomy. The concern with external fixation relates more to pin-site issues and less stable fixation compared to IMN.
- E. Unreamed nailing allows for immediate full weight-bearing, accelerating rehabilitation: While IMN provides good stability, a comminuted diaphyseal fracture (OTA 42-B3) fixed with an unreamed nail typically requires a period of protected weight-bearing (e.g., touch-down weight-bearing for 6 weeks, as described in the case) to allow for callus formation and prevent implant failure. Immediate full weight-bearing is generally not advised.
Question 28
The patient's postoperative course included aggressive intravenous fluid resuscitation to maintain a high urine output and monitoring of serum creatine kinase (CK) levels. This management strategy is primarily aimed at preventing which of the following complications?
Explanation
Correct Answer: C
Explanation:
Aggressive intravenous fluid resuscitation and monitoring of serum creatine kinase (CK) levels post-fasciotomy are critical for preventing acute kidney injury (AKI) secondary to rhabdomyolysis. Rhabdomyolysis is the breakdown of damaged muscle tissue, releasing myoglobin into the bloodstream. Myoglobin is nephrotoxic and can precipitate in the renal tubules, leading to acute tubular necrosis and AKI. Maintaining a high urine output helps to flush myoglobin through the renal tubules, while monitoring CK levels tracks the extent of muscle breakdown.
- A. Deep vein thrombosis (DVT): While DVT prophylaxis is important in trauma patients, aggressive fluid resuscitation is not its primary treatment or prevention strategy.
- B. Acute respiratory distress syndrome (ARDS): ARDS is a severe lung injury that can occur in polytrauma patients, but it is not directly addressed by fluid resuscitation for rhabdomyolysis.
- D. Compartment syndrome recurrence: Compartment syndrome recurrence is prevented by ensuring a complete fasciotomy and leaving the wounds open. While fluid management is crucial for systemic health, it does not directly prevent recurrence of local compartment pressure.
- E. Wound infection and dehiscence: Wound infection is managed with antibiotics, meticulous debridement, and proper wound care. Dehiscence is prevented by delayed primary closure or skin grafting when edema has resolved. Fluid resuscitation is not the primary intervention for these wound complications.
Question 29
During the initial clinical examination, the patient demonstrated profound weakness in active dorsiflexion of the ankle and toe extension, with a rapid decline in motor strength from 3/5 to 1/5. Sensation was diminished in the first dorsal webspace. Which nerve is primarily affected by the acute compartment syndrome in this scenario, and what compartment does it innervate?
Explanation
Correct Answer: C
Explanation:
The deep peroneal nerve innervates the muscles of the anterior compartment of the leg, which are responsible for active dorsiflexion of the ankle (tibialis anterior) and toe extension (extensor hallucis longus, extensor digitorum longus). It also provides sensation to the first dorsal webspace. The described motor weakness and sensory deficit are classic signs of deep peroneal nerve compromise due to acute compartment syndrome in the anterior compartment.
- A. Tibial nerve; superficial posterior compartment: The tibial nerve innervates the superficial and deep posterior compartments, responsible for plantarflexion of the ankle and toe flexion. Its sensory distribution includes the sole of the foot.
- B. Superficial peroneal nerve; lateral compartment: The superficial peroneal nerve innervates the muscles of the lateral compartment (peroneus longus and brevis), which are responsible for active eversion of the ankle. Its sensory distribution is the lateral dorsum of the foot. While the case mentions altered sensation in this distribution, the profound motor weakness described points more strongly to the deep peroneal nerve.
- D. Sural nerve; deep posterior compartment: The sural nerve is a purely sensory nerve, providing sensation to the lateral aspect of the foot and ankle. It does not innervate any muscles.
- E. Saphenous nerve; medial compartment: The saphenous nerve is a purely sensory nerve, providing sensation to the medial aspect of the leg and foot. It does not innervate any muscles.
Question 30
The patient sustained an open right tibial diaphyseal fracture. The laceration was 2 cm, without extensive soft tissue damage, avulsions, or degloving, and with adequate soft tissue coverage for the bone. Based on this description, what is the correct Gustilo-Anderson classification for this open fracture?
Explanation
Correct Answer: B
Explanation:
The Gustilo-Anderson classification system categorizes open fractures based on the size of the wound, the extent of soft tissue damage, and the degree of contamination. In this case, the laceration was 2 cm, which is greater than 1 cm but without extensive soft tissue damage, avulsions, or degloving, and with adequate soft tissue coverage for the bone. This description perfectly matches the criteria for a Gustilo-Anderson Type II open fracture.
- A. Gustilo-Anderson Type I: Characterized by a wound less than 1 cm, with minimal soft tissue damage, and usually a clean wound.
- C. Gustilo-Anderson Type IIIA: Involves extensive soft tissue damage, but with adequate soft tissue coverage of the bone despite the damage. The wound is typically greater than 10 cm.
- D. Gustilo-Anderson Type IIIB: Characterized by extensive soft tissue damage with periosteal stripping and inadequate soft tissue coverage, requiring a flap for coverage.
- E. Gustilo-Anderson Type IIIC: Involves an arterial injury requiring repair, regardless of the size of the wound or the extent of soft tissue damage.
Question 31
The case emphasizes a critical clinical pearl: 'Open fractures do not prevent compartment syndrome.' Which of the following statements best explains why an open tibial fracture, even with a visible laceration, does not reliably decompress the fascial compartments and prevent acute compartment syndrome?
Explanation
Correct Answer: A
Explanation:
The statement 'Open fractures do not prevent compartment syndrome' is a crucial clinical pearl. The primary reason is that the fascial defect created by an open fracture, even if visible, is rarely large enough or strategically located to allow for sufficient decompression of the entire fascial compartment. The non-yielding osseous-fascial envelope remains largely intact, trapping the accumulating hematoma and edematous muscle, leading to a rise in intra-compartmental pressure above the ischemic threshold. The case explicitly states: 'The fascial defect is rarely large enough to allow sufficient extrusion of hematoma and edematous muscle to lower the intra-compartmental pressure below the ischemic threshold.'
- B. Open fractures inherently cause more severe arterial injury, leading to compartment syndrome: While severe open fractures can be associated with arterial injury (Gustilo-Anderson Type IIIC), this is not the inherent mechanism by which open fractures fail to prevent compartment syndrome. Compartment syndrome is a pressure-related phenomenon, not primarily an arterial injury.
- C. The presence of an open wound increases the risk of infection, which directly causes compartment syndrome: Infection (e.g., necrotizing fasciitis) can cause compartment syndrome, but this is a distinct pathology. The failure of an open fracture to decompress is a mechanical issue related to the fascial envelope, not primarily an infectious one.
- D. Open fractures lead to systemic hypotension, which lowers the Delta P and precipitates compartment syndrome: While systemic hypotension can lower the Delta P and make a patient more susceptible to ischemia at a given compartment pressure, open fractures do not inherently cause hypotension. The patient in this case was hemodynamically stable.
- E. The bone fragments in an open fracture directly compress the muscles, causing compartment syndrome regardless of fascial integrity: While displaced bone fragments can contribute to soft tissue injury and hematoma, the primary mechanism of compartment syndrome is the global increase in pressure within the fascial compartment, not direct compression by bone fragments. The fascial envelope's inability to expand is the key factor.
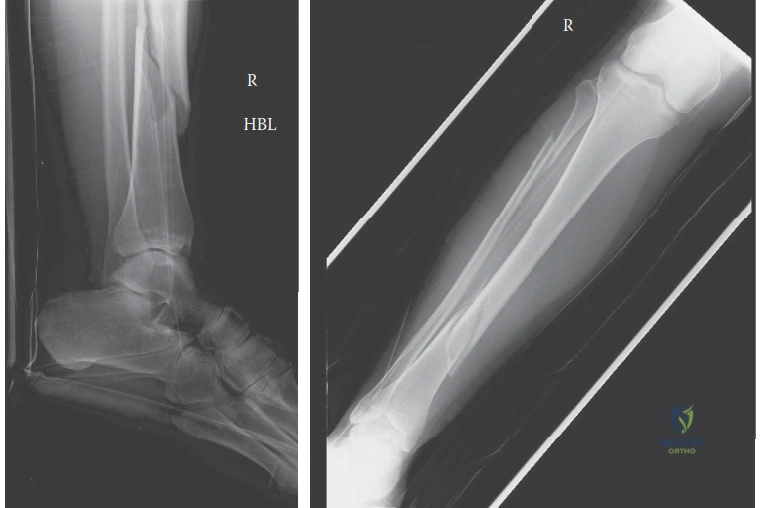
Question 32
The patient's radiographs, shown below, revealed a displaced, comminuted fracture of the middle and distal third junction of the right tibial diaphysis, classified as an OTA/AO 42-B3. This was associated with a segmental fracture of the fibular diaphysis. What does the 'B3' in the OTA/AO classification for the tibia specifically indicate?
Explanation
Correct Answer: C
Explanation:
The OTA/AO classification system for long bone fractures is hierarchical. For the tibia (bone 4), diaphyseal fractures are group 2. The 'B' indicates a wedge fracture, meaning there is a third fragment (a wedge) that is still in contact with one of the main fragments after reduction. The '3' further specifies the type of wedge. A 'B3' fracture is a wedge fracture with a fragmented wedge, indicating a more comminuted and unstable wedge fragment compared to a simple wedge (B2).
- A. A simple spiral fracture of the tibia: A simple spiral fracture would typically be classified as an A1 fracture (simple, spiral).
- B. A multifragmentary segmental fracture of the tibia: A segmental fracture (two distinct fracture lines creating a free segment) would be classified as a C-type fracture (complex, multifragmentary).
- D. A complex comminuted fracture with bone loss: While the fracture is comminuted, 'bone loss' is not directly indicated by B3. Complex comminuted fractures are generally C-type fractures.
- E. An intra-articular fracture extending into the ankle joint: Intra-articular fractures are classified differently (e.g., 43-A, B, C for distal tibia). The '42' indicates a diaphyseal fracture, not an intra-articular one.
Question 33
A 32-year-old male undergoes intramedullary nailing for a proximal third tibia shaft fracture via an infrapatellar approach. Postoperatively, what is the most common malalignment seen in this fracture pattern using this specific surgical approach?
Explanation
Question 34
To prevent the classic valgus and procurvatum deformity during intramedullary nailing of a proximal third tibia fracture, where should the blocking (Poller) screws be placed relative to the central axis of the medullary canal in the proximal segment?
Explanation
Question 35
A 25-year-old male is intubated following a motorcycle crash and has a closed midshaft tibia fracture. Compartment pressures are measured. Which of the following thresholds is the most universally accepted absolute indication for a four-compartment fasciotomy?
Explanation
Question 36
Based on the findings of the SPRINT (Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures) trial, what is the primary conclusion regarding reamed versus unreamed intramedullary nailing?
Explanation
Question 37
A 40-year-old male presents to the ED 48 hours after a crush injury to his right leg. The leg is woody, cold, and pulseless with profound motor and sensory deficits. Renal labs show severe myoglobinuria. What is the most appropriate management of the lower extremity?
Explanation
Question 38
During intramedullary nailing of a distal third tibia fracture, the surgeon notes valgus malalignment at the fracture site upon nail insertion. Which of the following technical errors most commonly contributes to this specific deformity?
Explanation
Question 39
Which of the following is a primary biomechanical advantage of the suprapatellar approach for tibial intramedullary nailing compared to the traditional infrapatellar approach?
Explanation
Question 40
A 24-year-old male sustains a Gustilo-Anderson Type IIIB open tibia fracture. According to current evidence-based guidelines, which of the following is the most critical initial intervention to prevent deep infection?
Explanation
Question 41
During a standard two-incision, four-compartment fasciotomy of the leg, the medial incision is utilized to release the superficial and deep posterior compartments. Releasing the deep posterior compartment carries the greatest risk of iatrogenic injury to which structure?
Explanation
Question 42
A 45-year-old male presents 9 months after unreamed IM nailing of a closed midshaft tibia fracture with persistent pain. Radiographs demonstrate a hypertrophic nonunion. What is the most appropriate definitive surgical management?
Explanation
Question 43
To minimize the risk of thermal necrosis to the diaphyseal bone during reamed intramedullary nailing of a dense tibia, which of the following surgical techniques is most appropriate?
Explanation
Question 44
A patient develops clawing of the lesser toes, loss of sensation on the plantar aspect of the foot, and a fixed equinus deformity 6 months after a severe tibia fracture treated with IM nailing. This presentation is most consistent with a missed compartment syndrome of which compartment?
Explanation
Question 45
A 10-year-old boy is admitted after a closed reduction and long leg casting of a displaced tibia shaft fracture. Which of the following is the most sensitive early clinical indicator of developing compartment syndrome in this pediatric patient?
Explanation
Question 46
A patient with a highly contaminated open tibia fracture is initially managed with an external fixator. The surgeon plans to convert to an intramedullary nail. Which of the following factors is most strongly associated with deep infection following this conversion?
Explanation
Question 47
Six months following a statically locked IM nail for a midshaft tibia fracture, a patient has a delayed union with a visible gap. Dynamization is planned. Which of the following fracture patterns is an absolute contraindication to dynamization?
Explanation
Question 48
A patient presents with acute compartment syndrome isolated to the lateral compartment of the lower leg. If left untreated, which of the following functional deficits is most likely to result?
Explanation
Question 49
What is the optimal starting point for a traditional infrapatellar intramedullary nail in the tibia on an anteroposterior (AP) and lateral radiograph?
Explanation
Question 50
A 35-year-old sustains a Gustilo-Anderson IIIB open tibia fracture requiring a free tissue transfer for coverage. According to Godina's classic principles, what is the optimal timeframe for this soft tissue coverage to minimize infection and maximize flap survival?
Explanation
Question 51
A 28-year-old male sustains a proximal third diaphyseal tibia fracture and undergoes infrapatellar intramedullary nailing. Postoperatively, radiographs reveal the most common malalignment associated with this specific injury pattern. Which of the following describes this typical deformity?
Explanation
Question 52
To prevent the typical procurvatum and valgus deformity during intramedullary nailing of a proximal third tibia fracture, a surgeon decides to place blocking (Poller) screws. Where should the blocking screws be placed in the proximal segment relative to the intended path of the nail?
Explanation
Question 53
A 32-year-old intubated multi-trauma patient has a closed, highly comminuted midshaft tibia fracture. His blood pressure is 115/65 mmHg. Intracompartmental pressures of the leg are measured. Which of the following anterior compartment pressures is the threshold to mandate an immediate four-compartment fasciotomy based on the Delta P concept?
Explanation
Question 54
A 45-year-old male is found down and unresponsive in his apartment for an estimated 72 hours with his leg pinned under heavy furniture. He presents with a rigid, swollen calf, absent sensation, and complete motor loss. Arterial doppler signals are present. What is the most appropriate management of his leg?
Explanation
Question 55
A surgeon opts to use a suprapatellar nailing technique in the semi-extended position for a proximal third tibia fracture rather than a standard infrapatellar approach. What is the primary biomechanical advantage of this positioning?
Explanation
Question 56
During a two-incision fasciotomy for acute compartment syndrome of the leg, a surgeon successfully releases the anterior, lateral, and superficial posterior compartments, but struggles to identify and release the deep posterior compartment. Which specific neurologic deficit would most likely persist if this compartment remains untreated?
Explanation
Question 57
A 35-year-old male sustains a Gustilo-Anderson Type IIIB open tibia fracture requiring surgical debridement and intramedullary nailing. A 12-cm soft tissue defect with exposed bone devoid of periosteum remains. To optimize outcomes and minimize infection risk, when is the ideal timeframe for definitive flap coverage?
Explanation
Question 58
A 28-year-old male presents 5 months after static intramedullary nailing of a closed midshaft tibia fracture. He reports moderate pain with weight-bearing. Radiographs show minimal callus formation and no hardware failure. The fracture is axially stable. What is the most appropriate next step in management?
Explanation
Question 59
A patient is admitted following a high-energy tibial shaft fracture. Two hours later, they complain of disproportionate leg pain. Physical examination reveals decreased sensation in the first dorsal webspace and profound pain with passive stretching of the extensor hallucis longus. Which compartment is experiencing the highest tissue pressure?
Explanation
Question 60
During the reaming process for an intramedullary tibial nail, the surgeon is concerned about the risk of thermal necrosis to the diaphyseal bone. Which of the following technical strategies is most effective in minimizing this complication?
Explanation
Question 61
A resident is planning an infrapatellar intramedullary nail for a midshaft tibia fracture. To achieve ideal fracture alignment and prevent iatrogenic deformity, what is the optimal anatomic starting point on the anteroposterior (AP) radiograph?
Explanation
Question 62
A 33-year-old female presents for her 1-year follow-up after an uncomplicated, fully healed infrapatellar intramedullary nailing of a closed tibia fracture. Radiographs show a well-consolidated fracture. What is the most frequently reported chronic complication she is likely to experience?
Explanation
Question 63
A 40-year-old female undergoes intramedullary nailing for a distal metaphyseal-diaphyseal junction tibia fracture. Because the distal metaphysis is wide and offers poor cortical contact for the nail, what is the most common postoperative malalignment encountered in this region?
Explanation
Question 64
A surgeon attempts a single-incision lateral (perifibular) fasciotomy to release all four compartments of the leg. Compared to the gold-standard double-incision technique, this single-incision approach carries a significantly higher risk of iatrogenic injury to which nerve?
Explanation
Question 65
According to established orthopedic principles, which of the following scenarios is generally considered an absolute contraindication to reamed antegrade intramedullary nailing of a tibial shaft fracture?
Explanation
Question 66
Modern conventional antegrade tibial intramedullary nails are manufactured with a distinct proximal bend, known as the Herzog curve. What is the primary biomechanical purpose of this design feature?
Explanation
Question 67
During the pathophysiologic cascade of acute compartment syndrome in a fractured tibia, the sequence of microvascular compromise is predictable. Which of the following clinical signs or physiological parameters is typically the LAST to be lost or altered?
Explanation
Question 68
A 35-year-old male smoker has an 8-month-old aseptic hypertrophic nonunion of a midshaft tibia fracture. He was originally treated with an 8-mm unreamed intramedullary nail. There is no bone loss or deformity. What is the most successful definitive surgical intervention?
Explanation
Question 69
A 22-year-old agricultural worker sustains a Gustilo-Anderson Type IIIB open tibia fracture highly contaminated with soil and manure. Alongside immediate surgical debridement, what is the most appropriate prophylactic intravenous antibiotic regimen based on standard trauma guidelines?
Explanation
Question 70
A 40-year-old male sustains an isolated, closed midshaft tibia fracture. Radiographs confirm that the ipsilateral fibula is entirely intact. If this injury is treated non-operatively in a cast, what is the most significant structural complication associated with this specific injury pattern?
Explanation
Question 71
A 30-year-old male undergoes intramedullary (IM) nailing for a closed midshaft tibia fracture. Based on the findings of the SPRINT trial, what is the primary clinical advantage of utilizing a reamed IM nail compared to an unreamed IM nail in this specific patient population?
Explanation
Question 72
When performing intramedullary nailing of a proximal third extra-articular tibia fracture using a standard infrapatellar approach, the fracture is most susceptible to which of the following classic malalignment patterns?
Explanation
Question 73
To prevent the classic valgus and procurvatum deformity during intramedullary nailing of a proximal third tibia fracture, blocking (Poller) screws can be utilized. Relative to the planned path of the nail, where should these screws be placed in the proximal fragment?
Explanation
Question 74
A 25-year-old male sustains a severe crush injury to his left leg. His blood pressure is 110/70 mmHg. Intracompartmental pressure monitoring is initiated due to a tense calf. Which of the following thresholds is the most reliable and widely accepted indication to perform a four-compartment fasciotomy?
Explanation
Question 75
A 40-year-old male is found down 36 hours after a drug overdose with his leg crushed beneath his body. He has a tense, firm calf, an absent dorsalis pedis pulse, dense foot drop, and absent sensation in the deep peroneal nerve distribution. Pressures measure >70 mmHg. What is the most appropriate initial management?
Explanation
Question 76
During a standard two-incision, four-compartment fasciotomy for acute compartment syndrome of the leg, the medial incision is utilized to decompress the superficial and deep posterior compartments. Which of the following structures must be explicitly detached or mobilized to adequately decompress the deep posterior compartment?
Explanation
Question 77
A 45-year-old male sustains a Gustilo-Anderson Type IIIB open tibia fracture with a 10 cm exposed soft tissue and bone defect over the distal third of the anterior tibia. After skeletal stabilization and serial debridements, which of the following is the most appropriate soft tissue coverage option?
Explanation
Question 78
A 35-year-old smoker presents 8 months following statically locked intramedullary nailing of a closed midshaft tibia fracture. He reports pain with weight-bearing. Radiographs demonstrate a hypertrophic nonunion with broken distal locking screws. What is the most successful surgical intervention?
Explanation
Question 79
Irreversible necrosis of muscle tissue in acute compartment syndrome of the lower extremity typically begins after what duration of continuous ischemia?
Explanation
Question 80
A surgeon elects to perform a single-incision (perifibular) four-compartment fasciotomy rather than the traditional dual-incision technique. Which of the following is a recognized risk specifically increased with this single-incision approach?
Explanation
Question 81
A 28-year-old female with a high-energy diaphyseal tibia fracture is undergoing intramedullary nailing. The anesthesia team offers a continuous popliteal nerve block for postoperative pain control. Why is continuous regional anesthesia generally discouraged in this specific scenario?
Explanation
Question 82
Following successful union of a tibia fracture treated with an antegrade intramedullary nail via an infrapatellar approach, what is the most frequently reported long-term complication by patients?
Explanation
Question 83
Which of the following describes a primary biomechanical advantage of utilizing a suprapatellar approach (with the knee in a semi-extended position) over a traditional infrapatellar approach for tibial intramedullary nailing?
Explanation
Question 84
A 50-year-old male presents with a high-energy closed tibia fracture and massive soft tissue swelling with fracture blisters (Tscherne Grade 3). A temporizing spanning external fixator is placed. When is the most appropriate time to safely convert to an intramedullary nail?
Explanation
Question 85
According to current evidence-based guidelines for the management of open tibia fractures, which of the following interventions is the most critical factor in reducing the rate of deep surgical site infection?
Explanation
Question 86
A 42-year-old male is undergoing intramedullary nailing of a proximal-third tibia shaft fracture. To prevent the typical apex anterior and apex medial (valgus) deformities commonly seen with this injury, where should blocking (Poller) screws be placed relative to the path of the intramedullary nail in the proximal fragment?
Explanation
Question 87
A 25-year-old male is admitted with a closed midshaft tibia fracture. Overnight, he develops severe leg pain that is unresponsive to parenteral opioids. On examination, he has exquisite pain with passive toe extension. His blood pressure is 110/70 mmHg. Intracompartmental pressure monitoring reveals a pressure of 45 mmHg in the anterior compartment and 35 mmHg in the deep posterior compartment. What is the most appropriate next step in management?
Explanation
Question 88
Based on the SPRINT (Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures) trial, which of the following is the most significant finding when comparing reamed and unreamed intramedullary nailing for tibial shaft fractures?
Explanation
Question 89
A 40-year-old male is transferred to a tertiary trauma center 4 days after sustaining a closed tibial shaft fracture following a drug overdose. He has received no prior medical care. The leg is tense and woody, and lacks any sensation or motor function below the knee. Distal pulses are intact. Intracompartmental pressure is measured at 60 mmHg. What is the most appropriate management?
Explanation
Question 90
When performing a single-incision perifibular approach for a four-compartment fasciotomy of the leg, which two compartments are accessed by dissecting posterior to the fibula?
Explanation
Question 91
A 22-year-old female sustains a closed, isolated, minimally displaced midshaft tibia fracture. She is treated non-operatively in a long leg cast. According to standard criteria for acceptable alignment in the non-operative management of tibial shaft fractures, what is the maximum acceptable varus/valgus angulation?
Explanation
Question 92
Compared to the traditional infrapatellar approach, the suprapatellar approach for intramedullary nailing of tibial shaft fractures provides which of the following mechanical or clinical advantages?
Explanation
Question 93
A 30-year-old male sustains a Gustilo-Anderson Type IIIB open tibia fracture treated with immediate debridement, irrigation, and intramedullary nailing. According to current orthopedic principles, when is the optimal timeframe to perform definitive soft-tissue coverage with a flap to minimize infection and maximize flap survival?
Explanation
None
