Musculoskeletal Tumors: Lipomas, Osteosarcoma, HME for ABOS Board Review | Part 14
Key Takeaway
ABOS Musculoskeletal Tumors Review covers key aspects of lipomatous tumors, osteosarcoma, and hereditary multiple exostoses (HME). This includes clinical presentation, diagnostic imaging (MRI, CT, bone scan), histopathology, and management principles for various benign and malignant bone and soft tissue lesions. Essential for orthopedic board preparation.
Musculoskeletal Tumors: Lipomas, Osteosarcoma, HME for ABOS Board Review | Part 14
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
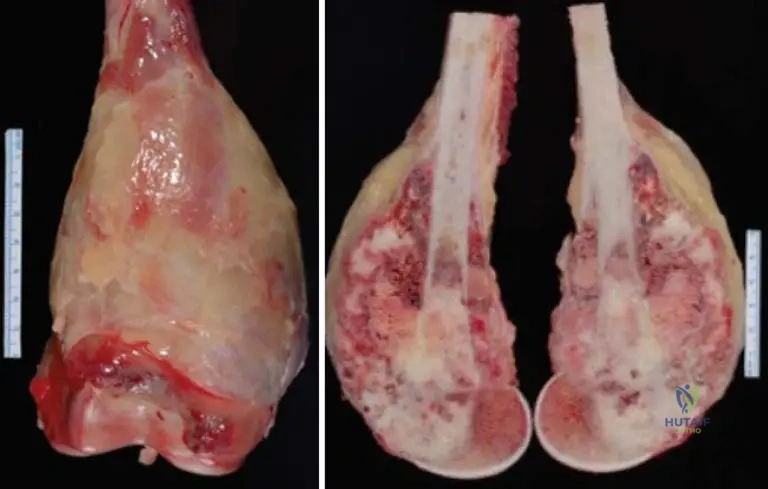
A 12-year-old boy presents with knee pain. Radiographs show a sunburst periosteal reaction in the distal femur, and biopsy confirms conventional osteosarcoma. Which of the following histologic findings following neoadjuvant chemotherapy is the most important prognostic factor?
Explanation
Question 2
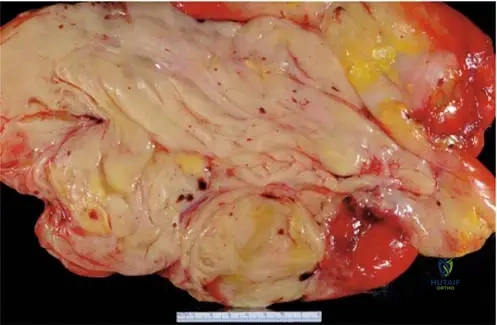
A 55-year-old male presents with a large, slow-growing, painless mass deep in his thigh. MRI shows a predominantly fatty mass with thick septations. Which genetic abnormality confirms the diagnosis of an atypical lipomatous tumor (ALT)?
Explanation
Question 3
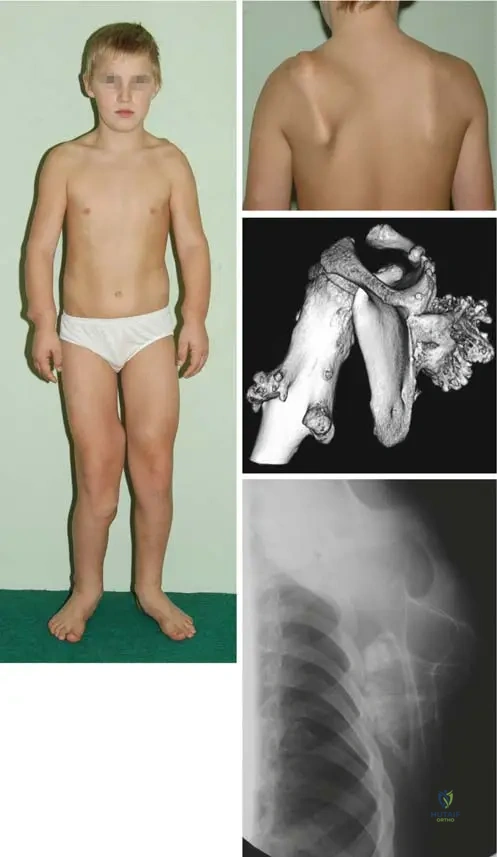
A 28-year-old male with a known history of Hereditary Multiple Exostoses (HME) presents with new, progressive pain in his pelvis. Which of the following MRI findings is most concerning for malignant transformation?

Explanation
Question 4
Which of the following osteosarcoma subtypes is typically characterized as low-grade, occurs primarily on the posterior aspect of the distal femur, and is often associated with MDM2 and CDK4 amplification?
Explanation
Question 5
A 16-year-old boy undergoes resection of a distal femur conventional osteosarcoma.
What is the standard neoadjuvant chemotherapy regimen utilized for this malignancy?
Explanation
Question 6
A 45-year-old female presents with a soft tissue mass in her subcutaneous forearm. MRI reveals a homogeneous mass that is hyperintense on T1-weighted images and demonstrates complete suppression on STIR sequences. What is the most likely diagnosis?
Explanation
Question 7
Hereditary Multiple Exostoses (HME) is an autosomal dominant disorder caused by mutations in the EXT1 or EXT2 genes. What is the primary function of the proteins encoded by these genes?
Explanation
Question 8
An 18-year-old presents with acute thigh pain. Radiographs show a purely lytic, expansile lesion in the distal femur. MRI demonstrates multiple fluid-fluid levels. Biopsy reveals high-grade malignant cells producing osteoid. What is the most likely diagnosis?
Explanation
Question 9
A 10-year-old girl with Hereditary Multiple Exostoses (HME) presents for evaluation of forearm deformity.
Which of the following patterns of forearm deformity is most characteristic of this condition?
Explanation
Question 10
A 60-year-old man has a biopsy-proven atypical lipomatous tumor (ALT) in his posterior thigh.
There is no clinical or histologic evidence of dedifferentiation. Which of the following is the most appropriate surgical management?
Explanation
Question 11
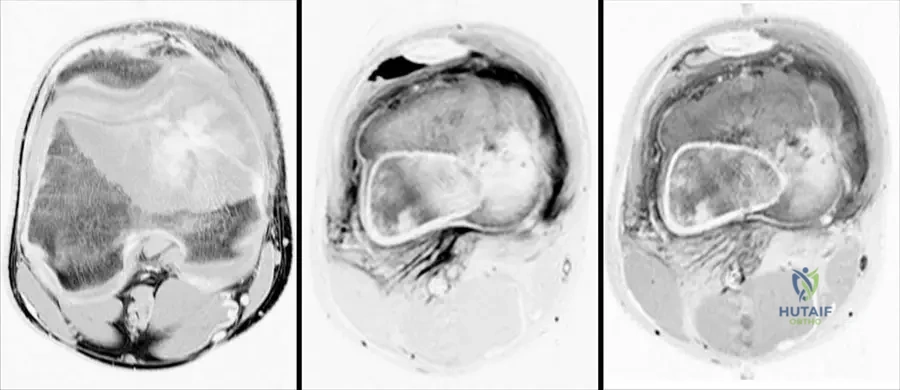
A 14-year-old girl is diagnosed with a conventional osteosarcoma of the proximal tibia. As part of her local staging, an MRI of the entire tibia is ordered. What is the primary purpose of imaging the entire involved bone?
Explanation
Question 12
When evaluating a soft-tissue mass suspected to be lipomatous, which of the following features on MRI is most indicative of an atypical lipomatous tumor (ALT) or liposarcoma rather than a simple lipoma?
Explanation
Question 13
A 15-year-old male presents with distal femur pain. Imaging reveals a mixed lytic/sclerotic lesion with a 'sunburst' periosteal reaction. Biopsy confirms conventional high-grade osteosarcoma.
After initiating multi-agent neoadjuvant chemotherapy, what is the most important histologic prognostic factor evaluated at the time of wide surgical resection?
Explanation
Question 14
Hereditary Multiple Exostoses (HME) is an autosomal dominant condition linked to mutations in the EXT1 and EXT2 genes. Which of the following best describes the pathophysiologic consequence of these genetic mutations?
Explanation
Question 15
A 58-year-old man presents with a large, slow-growing mass deep in his right thigh. MRI demonstrates a predominantly lipomatous mass with thick, nodular septations.
Core needle biopsy confirms an Atypical Lipomatous Tumor (ALT). Which of the following genetic alterations is diagnostic for this lesion?
Explanation
Question 16
A 22-year-old female presents with a painless mass on the posterior aspect of her distal femur. Radiographs show a dense, lobulated, heavily ossified mass on the surface of the bone with a radiolucent cleft between the tumor and the underlying cortex.
What is the most likely diagnosis?
Explanation
Question 17
A 32-year-old male with a known history of Hereditary Multiple Exostoses (HME) presents with new, increasing pain and enlargement of an osteochondroma on his left ilium.
Which of the following MRI findings is most indicative of malignant transformation to a secondary chondrosarcoma?
Explanation
Question 18
A 14-year-old boy undergoes neoadjuvant chemotherapy followed by wide surgical resection for conventional osteosarcoma of the distal femur. Which of the following is the most important independent prognostic factor for his overall survival?
Explanation
Question 19
A 10-year-old child presents with multiple bony prominences. Genetic testing reveals a mutation in the EXT1 gene. The normal product of this gene is primarily involved in which of the following cellular processes?
Explanation
Question 20
A 55-year-old man presents with a slow-growing, deep thigh mass. Biopsy demonstrates mature adipocytes with focal areas of atypical, hyperchromatic stromal cells. Fluorescence in situ hybridization (FISH) is most likely to show amplification of which of the following?
Explanation
Question 21
A 28-year-old woman presents with a slow-growing mass on the posterior aspect of her distal femur. Radiographs reveal a heavily ossified, lobulated mass arising from the surface of the bone with a broad base. Which of the following is characteristic of this lesion?
Explanation
Question 22
A 16-year-old boy presents with knee pain. Radiographs show a purely lytic, destructive lesion of the distal femur. MRI demonstrates fluid-fluid levels. Biopsy reveals blood-filled spaces with highly pleomorphic, anaplastic cells in the septa producing osteoid. What is the most likely diagnosis?
Explanation
Question 23
A 35-year-old man with Hereditary Multiple Exostoses (HME) notices a rapid increase in the size of a long-standing pelvic mass. Which of the following MRI findings is most indicative of malignant transformation to secondary chondrosarcoma?
Explanation
Question 24
A 9-year-old girl with Hereditary Multiple Exostoses presents with a progressive forearm deformity. Which of the following best describes the classic deformity pattern seen in this condition?

Explanation
Question 25
A 45-year-old woman undergoes ankle radiographs for a sprain, revealing an incidental, well-circumscribed radiolucent lesion in the calcaneus with central calcification. What is the most likely diagnosis?
Explanation
Question 26
A 30-year-old man presents with a slow-growing, painless mass in his thigh. MRI shows a lipomatous tumor with prominent vascularity. PET scan demonstrates extremely high FDG avidity. Biopsy reveals multivacuolated fat cells with eosinophilic granular cytoplasm. What is the diagnosis?
Explanation
Question 27
A 15-year-old girl is diagnosed with a high-grade conventional osteosarcoma of the proximal tibia. What is the most appropriate imaging modality to evaluate for the presence of skip metastases within the affected limb?
Explanation
Question 28
Which of the following bone surface tumors is typically a high-grade lesion that shares the same prognosis and treatment protocol as conventional intramedullary osteosarcoma?
Explanation
Question 29
Which of the following is the radiographic hallmark required for the definitive diagnosis of an osteochondroma?
Explanation
Question 30
A 45-year-old man presents with a palpable mass in the proximal, lateral aspect of his forearm and weakness in extending his fingers. Radiographs show a radiolucent soft tissue mass causing focal hyperostosis of the underlying proximal radius. What is the most likely diagnosis?
Explanation
Question 31
A 12-year-old boy with a family history of early-onset breast cancer and adrenocortical carcinoma is diagnosed with osteosarcoma. Which of the following genetic mutations is most likely responsible for this patient's condition?
Explanation
Question 32
Regarding the clinical behavior of atypical lipomatous tumors (ALT) / well-differentiated liposarcomas of the extremity, which of the following statements is true?
Explanation
Question 33
A 72-year-old man with a long history of Paget's disease presents with a sudden, severe increase in left thigh pain and a new palpable mass. Radiographs show a destructive lytic lesion with cortical breakthrough. What is the most likely diagnosis?
Explanation
Question 34
A 16-year-old boy with a known osteochondroma of the posterior distal femur presents with a newly enlarging, pulsatile mass behind the knee and decreased distal pulses. What is the most likely complication that has occurred?
Explanation
Question 35
Which of the following chemotherapy agents are considered the standard first-line neoadjuvant regimen for conventional high-grade osteosarcoma?
Explanation
Question 36
Patients with Hereditary Multiple Exostoses (HME) are at risk for malignant transformation to chondrosarcoma. Which genotype has been linked to a higher risk of malignant transformation and more severe disease burden?
Explanation
Question 37
When evaluating a deep soft tissue fatty mass on MRI, which of the following features is most reliable for differentiating an atypical lipomatous tumor from a benign lipoma?

Explanation
Question 38
A 12-year-old male with Hereditary Multiple Exostoses (HME) presents for routine evaluation.
Which of the following best describes the underlying molecular pathophysiology of his condition?
Explanation
Question 39
Which of the following genetic mutations and corresponding molecular mechanisms are primarily responsible for the development of Hereditary Multiple Exostoses (HME)?
Explanation
Question 40
A 55-year-old male presents with a deep 8 cm soft tissue mass in the anterior thigh. Biopsy shows mature adipocytes with focal atypical cells and thickened fibrous septa. Which genetic aberration definitively distinguishes this Atypical Lipomatous Tumor (ALT) from a benign lipoma?
Explanation
Question 41
A 16-year-old male with conventional osteosarcoma of the distal femur completes a 10-week course of neoadjuvant MAP (methotrexate, doxorubicin, cisplatin) chemotherapy followed by wide resection. Which histologic finding in the resected specimen is the most critical independent predictor of long-term survival?
Explanation
Question 42
A 28-year-old female presents with a painless, slow-growing mass behind her knee. Radiographs reveal a densely ossified, lobulated mass arising from the posterior cortex of the distal femur, separated from the underlying bone by a narrow radiolucent cleft (the "string sign"). What is the most likely diagnosis?
Explanation
Question 43
In a child with Hereditary Multiple Exostoses (HME), what is the most common forearm deformity requiring surgical intervention?
Explanation
Question 44
A 14-year-old female presents with severe distal thigh pain. MRI reveals a lytic, expansile metaphyseal lesion with prominent fluid-fluid levels. Core needle biopsy demonstrates blood-filled spaces separated by septa containing highly pleomorphic cells producing delicate osteoid. What is the diagnosis?
Explanation
Question 45
Which of the following surface osteosarcoma variants is typically intermediate-grade, has a prominent chondroblastic histologic component, and classically presents as a "sunburst" periosteal reaction on the diaphyseal surface without medullary involvement?
Explanation
Question 46
A 15-year-old boy presents with the radiographic findings shown. Biopsy confirms conventional osteosarcoma. What is the most common initial site of metastasis for this disease?
Explanation
Question 47
An asymptomatic 60-year-old male has a 12 cm intramuscular lipomatous mass in his anterior thigh. Core biopsy confirms Atypical Lipomatous Tumor (ALT). What is the most appropriate surgical management for this extremity lesion?
Explanation
Question 48
A 14-year-old with multiple bony protuberances around his knees and shoulders has a known genetic condition. What is the primary cellular function of the mutated genes responsible for this disorder?
Explanation
Question 49
A 25-year-old female presents with a painless mass behind her knee. Radiographs reveal a densely ossified mass attached to the posterior cortex of the distal femur by a broad base, with no medullary involvement. Which genetic abnormality is the hallmark of this lesion?
Explanation
Question 50
A 60-year-old male presents with a deep, painless thigh mass.
MRI reveals a predominantly fatty mass with thick nodular septations greater than 2 mm. What is the most appropriate initial step in management?
Explanation
Question 51
A 19-year-old male has a lytic, expansile metaphyseal lesion of the proximal tibia. MRI shows prominent fluid-fluid levels. Biopsy reveals blood-filled spaces lined by highly pleomorphic, atypical spindle cells producing osteoid matrix. What is the correct diagnosis?
Explanation
Question 52
A 10-year-old girl with hereditary multiple exostoses presents with progressive forearm deformity.
Which of the following describes the most classic pattern of forearm deformity seen in this condition?
Explanation
Question 53
A 72-year-old man with a history of an enlarging skull and bowing of his long bones presents with severe, progressive right hip pain. Radiographs show mixed lytic and sclerotic changes in the hemipelvis with cortical destruction and an expansile soft tissue mass. What is the most likely underlying condition predisposing him to this malignancy?
Explanation
Question 54
A 45-year-old female undergoes marginal excision of an intramuscular lipoma in her deltoid. Pathology confirms a benign lipoma with skeletal muscle fibers interspersed among mature adipocytes. What is the most important clinical consideration regarding this specific tumor type?
Explanation
Question 55
A 16-year-old boy presents with an enlarging mass on the anterior aspect of his mid-tibia. Radiographs demonstrate a broad-based, surface lesion with a sunburst appearance and no medullary involvement. Histology reveals a predominantly chondroblastic matrix with intermediate-grade atypia. What is the diagnosis?
Explanation
Question 56
A 32-year-old male with Hereditary Multiple Exostoses presents for routine surveillance. He asks about his risk for developing a malignancy from his bone lesions. In which of the following anatomic locations is malignant transformation to chondrosarcoma most likely to occur?
Explanation
Question 57
The standard neoadjuvant chemotherapy regimen for conventional high-grade osteosarcoma typically includes methotrexate, doxorubicin, and cisplatin. What is the primary antineoplastic mechanism of action of cisplatin?
Explanation
Question 58
A 65-year-old man undergoes resection of a massive retroperitoneal mass. Histology shows areas of mature fat with thick septations alongside discrete areas of high-grade, non-lipogenic pleomorphic spindle cells. Which of the following statements is true regarding this diagnosis?
Explanation
Question 59
An 18-year-old male with a solitary osteochondroma of the distal femur presents with new-onset pain. An MRI is obtained to evaluate the cartilage cap. At what minimum cartilage cap thickness in an adult should the surgeon be highly concerned for malignant transformation?
Explanation
Question 60
A 15-year-old boy is diagnosed with conventional osteosarcoma of the proximal tibia.
Before definitive surgical resection, which imaging modality is essential to properly identify skip metastases?
Explanation
Question 61
Which of the following genetic abnormalities is most consistently associated with the pathogenesis of Hereditary Multiple Exostoses (HME), and what is the resulting pathophysiologic defect?
Explanation
Question 62
A 60-year-old male presents with a deep, painless thigh mass. MRI demonstrates a predominantly fatty tumor with thick, nodular septations (>2 mm).
Which of the following molecular findings is definitive for diagnosing this lesion as an Atypical Lipomatous Tumor (ALT) rather than a benign lipoma?
Explanation
Question 63
A 25-year-old female presents with a slowly enlarging mass on the posterior aspect of her knee. Radiographs reveal a dense, heavily ossified mass arising from the posterior distal femur with a radiolucent cleft separating the tumor from the underlying cortex (string sign). What is the most likely diagnosis?
Explanation
Question 64
Neoadjuvant chemotherapy has significantly improved survival rates in patients with conventional high-grade osteosarcoma. Which of the following regimens represents the standard first-line combination therapy?
Explanation
Question 65
A 10-year-old boy with Hereditary Multiple Exostoses (HME) presents with progressive forearm deformity and loss of pronation. Which of the following is the characteristic pattern of forearm dysplasia typically seen in HME?
Explanation
Question 66
A 15-year-old male presents with severe pain in his distal femur. Radiographs show a destructive, expansile lytic lesion. MRI demonstrates multiple fluid-fluid levels. Core needle biopsy shows blood-filled spaces lined by malignant cells producing delicate lace-like osteoid. What is the diagnosis?
Explanation
Question 67
A 70-year-old male with a 20-year history of Paget's disease of bone develops acute, severe pain and rapid swelling in his right proximal femur. Radiographs show a new destructive lytic lesion with cortical breakthrough. What is the most likely etiology?
Explanation
Question 68
A 45-year-old female complains of chronic, painless swelling in her right knee. MRI reveals a diffuse, frond-like synovial mass that is hyperintense on T1-weighted images and demonstrates complete signal loss on fat-suppressed sequences. What is the most likely diagnosis?
Explanation
Question 69
A 35-year-old male with Hereditary Multiple Exostoses (HME) reports an enlarging, painful mass in his pelvis over the last 6 months.
Which of the following MRI features is the most reliable indicator of malignant transformation to a secondary chondrosarcoma?
Explanation
Question 70
A 20-year-old female presents with a palpable mass on the anterior midshaft of her tibia. Radiographs show a broad-based surface lesion with a sunburst 'hair-on-end' periosteal reaction. There is no medullary involvement. Biopsy reveals an intermediate-grade chondroblastic matrix. What is the diagnosis?
Explanation
Question 71
A 55-year-old male presents with a painless, slow-growing, subcutaneous mass on his posterior neck. Excisional biopsy histology reveals mature adipocytes admixed with uniform spindle cells and thick ropey collagen bundles. Immunohistochemistry is strongly positive for CD34. What is the correct diagnosis?
Explanation
Question 72
When evaluating a newly diagnosed patient with conventional high-grade osteosarcoma, what is the most significant independent prognostic factor for long-term overall survival?
Explanation
Question 73
An incisional biopsy is planned for a suspected high-grade osteosarcoma of the distal femur. To avoid compromising the definitive limb-salvage surgery, which of the following oncologic biopsy principles must be strictly adhered to?
Explanation
Question 74
Atypical Lipomatous Tumors (ALTs) and Well-Differentiated Liposarcomas (WDLPS) share identical histologic features and MDM2 amplification. The designation WDLPS is specifically reserved for tumors occurring in which anatomic location due to their inherent risk of lethal local progression?
Explanation
Question 75
Osteochondromas in patients with Hereditary Multiple Exostoses characteristically point away from the adjacent joint as they grow. Pathophysiologically, these lesions originate from aberrant endochondral ossification occurring in which specific region?
Explanation
Question 76
A 16-year-old male presents with knee pain, and radiographs reveal a mixed lytic/sclerotic metaphyseal lesion highly suspicious for osteosarcoma.
To adequately plan the level of surgical resection, which imaging modality is mandatory to evaluate for intramedullary skip metastases?
Explanation
Question 77
A 55-year-old male undergoes a marginal 'shell-out' excision of a deep, intermuscular thigh mass presumed to be a simple lipoma. Final pathology reveals an Atypical Lipomatous Tumor (ALT) with positive microscopic margins but no dedifferentiation. What is the expected clinical behavior if only observation is pursued?
Explanation
Question 78
A 14-year-old boy presents with progressive, non-mechanical knee pain. Radiographs demonstrate a mixed sclerotic and lytic lesion in the distal femoral metaphysis with a Codman's triangle and sunburst periosteal reaction. Which of the following MRI sequences is most critical for surgical planning of the resection?
Explanation
Question 79
A 10-year-old girl is evaluated for multiple painless, bony bumps around her knees and wrists. Radiographs reveal multiple osteochondromas pointing away from the joint line.
Which of the following accurately describes the molecular pathogenesis of her condition?
Explanation
Question 80
A 62-year-old man presents with a deep, painless 12 cm mass in his vastus lateralis. MRI demonstrates a predominantly lipomatous mass with thickened septations (>2 mm) and focal nodularity.
Core needle biopsy confirms an atypical lipomatous tumor (ALT). What is the most appropriate definitive management?
Explanation
Question 81
A 24-year-old female presents with a painless mass at the posterior aspect of her distal thigh. Radiographs demonstrate a heavily ossified mass arising from the posterior cortex of the distal femur. Biopsy reveals low-grade spindle cells with woven bone. What is the most common genetic abnormality associated with this tumor?
Explanation
Question 82
A 14-year-old male with Hereditary Multiple Exostoses (HME) presents with progressive deformity and limited pronation/supination of his left forearm. Radiographs typically demonstrate which of the following patterns in this condition?
Explanation
Question 83
A 15-year-old boy with conventional high-grade osteosarcoma of the proximal tibia is undergoing neoadjuvant MAP chemotherapy (Methotrexate, Doxorubicin, Cisplatin). He suddenly develops dyspnea and bilateral lower extremity edema. Echocardiography shows a severely reduced ejection fraction. Which chemotherapeutic agent is most likely responsible for this complication?
Explanation
Question 84
A 16-year-old female presents with acute thigh pain following a minor fall. Radiographs show an aggressive, purely lytic lesion in the distal femoral metaphysis with a pathologic fracture. MRI shows fluid-fluid levels throughout the lesion. Biopsy reveals blood-filled spaces with highly pleomorphic, atypical, malignant spindle cells in the septa producing osteoid. What is the diagnosis?
Explanation
Question 85
A 72-year-old male with a long-standing history of Paget's disease of bone presents with rapidly worsening pain and swelling in his right humerus. Radiographs show a new area of cortical destruction and a soft tissue mass. Biopsy confirms high-grade osteosarcoma. Which of the following best describes the prognosis of this patient compared to a pediatric patient with primary conventional osteosarcoma?
Explanation
Question 86
A 55-year-old male presents with a painless, slow-growing mass on the posterior aspect of his neck and upper back. Excisional biopsy is performed. Histopathology reveals mature adipocytes mixed with uniform spindle cells, ropey collagen, and a myxoid background. Immunohistochemistry is strongly positive for CD34 and shows loss of Rb1 expression. What is the diagnosis?
Explanation
Question 87
A 35-year-old female with a history of Hereditary Multiple Exostoses (HME) presents with progressive, deep pelvic pain. She notes that a long-standing bump on her iliac wing has recently started growing.
MRI demonstrates a cartilage cap of 2.5 cm with new heterogeneous signal characteristics. What is the most likely diagnosis?
Explanation
Question 88
A 19-year-old male complains of a lump on the anterior aspect of his mid-tibia. Radiographs show a radiolucent surface lesion with perpendicular sunburst periosteal reaction and cortical scalloping, but no medullary involvement. Biopsy reveals a predominantly chondroblastic matrix with malignant cells. What is the diagnosis?
Explanation
Question 89
A 65-year-old woman is diagnosed with an atypical lipomatous tumor (ALT) in her retroperitoneum. Which of the following explains why a retroperitoneal ALT has a worse long-term prognosis compared to an extremity ALT?
Explanation
Question 90
A 12-year-old girl is evaluated for worsening right knee pain. Plain films demonstrate an ill-defined, mixed lytic and sclerotic lesion in the proximal tibial metaphysis penetrating the cortex.
Which of the following histologic findings is required to confirm the diagnosis of conventional osteosarcoma?
Explanation
None
