ABOS Orthopedic Board Review: Bone Tumors, Alcohol-Related Musculoskeletal Issues & PJI | Part 24

Key Takeaway
This ABOS Board Review section offers multiple-choice questions on diverse orthopedic pathologies. Topics include Gorham's disease, avascular necrosis, septic arthritis, gout, nonossifying fibroma, and periprosthetic joint infection. It also covers alcohol-related musculoskeletal issues like osteoporosis and Charcot arthropathy, providing essential insights for exam preparation.
ABOS Orthopedic Board Review: Bone Tumors, Alcohol-Related Musculoskeletal Issues & PJI | Part 24
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 12-year-old boy presents after a mild knee twist. Radiographs reveal an incidental finding in the distal femur metaphysis as seen in the provided image.
The lesion is eccentrically located, lytic, and has a sclerotic margin. The patient is completely asymptomatic. What is the most appropriate next step in management?
Explanation
Question 2
A 45-year-old male with a history of heavy alcohol consumption presents with progressive groin pain. Radiographs and MRI of the hip confirm Ficat Stage II avascular necrosis of the femoral head. There is no evidence of subchondral collapse. Which of the following is the most appropriate initial joint-preserving surgical intervention?
Explanation
Question 3
According to the 2018 International Consensus Meeting (ICM) criteria, which of the following is considered a definitive 'major' criterion confirming a periprosthetic joint infection (PJI)?
Explanation
Question 4
A 22-year-old female presents with progressive weakness and pain in her shoulder over the past year. Radiographs demonstrate severe, progressive bone loss of the clavicle and scapula with tapering of the remaining bone ends.
Biopsy shows benign vascular proliferation without atypia. Which of the following is the most likely diagnosis?
Explanation
Question 5
A 55-year-old male with a history of chronic alcohol abuse presents with palmar nodules and cords causing a flexion contracture of his ring finger. At the cellular level, the pathogenesis of this condition primarily involves the replacement of normal palmar fascia with which of the following?
Explanation
Question 6
A 12-year-old boy presents with knee pain. Radiographs reveal an incidental cortically based, eccentric, lytic lesion with a sclerotic rim in the distal femoral metaphysis.
What is the most appropriate management for this lesion?
Explanation
Question 7
A 45-year-old male presents with spontaneous, progressive shoulder weakness and deformity. Radiographs demonstrate complete disappearance of the proximal humerus and clavicle.
Which histological finding is pathognomonic for this disease process?
Explanation
Question 8
A 40-year-old male with a history of severe chronic alcohol abuse presents with bilateral groin pain. MRI confirms stage II avascular necrosis (AVN) of both femoral heads. Which of the following best describes the pathophysiology of alcohol-induced AVN?
Explanation
Question 9
According to the 2018 International Consensus Meeting (ICM) criteria, which of the following is considered a 'major' criterion that is definitive for periprosthetic joint infection (PJI)?
Explanation
Question 10
A 60-year-old patient presents with a painful, erythematous lower leg 6 months following internal fixation of a tibial shaft fracture. Radiographs show a ununited fracture with loose hardware.
What is the most appropriate definitive management?
Explanation
Question 11
A 16-year-old male presents with a painful distal thigh mass. Imaging shows a destructive metaphyseal lesion with a 'sunburst' periosteal reaction. Biopsy confirms high-grade conventional osteosarcoma. What is the standard systemic chemotherapeutic regimen used in the neoadjuvant and adjuvant settings?
Explanation
Question 12
When treating a staphylococcal periprosthetic joint infection (PJI) with implant retention (DAIR), which of the following antibiotic agents is essential for penetrating the established bacterial biofilm?
Explanation
Question 13
A 28-year-old female is diagnosed with Gorham-Stout disease involving the thoracic spine and ribs.
She is at greatest risk for which of the following potentially fatal complications?
Explanation
Question 14
Chronic alcohol abuse significantly increases the risk of fragility fractures. Which of the following is the primary mechanism by which alcohol directly induces osteoporosis?
Explanation
Question 15
A 32-year-old female presents with a destructive, eccentric, lytic lesion in the proximal tibial epiphysis. Biopsy reveals mononuclear cells and numerous multinucleated giant cells. If the patient is treated with denosumab preoperatively, what is its mechanism of action?
Explanation
Question 16
Which of the following scenarios is the most appropriate indication for Debridement, Antibiotics, and Implant Retention (DAIR) in a patient with a total hip arthroplasty (THA)?
Explanation
Question 17
A 9-year-old boy presents with thigh pain and a fever. Radiographs show a permeative diaphyseal lesion in the femur with 'onion-skin' periostitis. Biopsy shows small round blue cells. Which specific genetic translocation is most commonly associated with this tumor?
Explanation
Question 18
A 12-year-old asymptomatic boy has an incidental finding on a knee radiograph: an eccentric, multilocular, lucent cortical lesion with a sclerotic rim in the distal femoral metaphysis.
What is the most appropriate management?
Explanation
Question 19
A 25-year-old female presents with progressive vanishing of her clavicle and upper ribs over the last two years, complicated by a chylothorax.
What is the underlying pathophysiology of her musculoskeletal condition?
Explanation
Question 20
A 68-year-old woman is 3 weeks post-operative from a primary total knee arthroplasty. She presents with 2 days of acute knee pain, swelling, and a draining sinus. Her CRP is 150 mg/L. Joint aspiration yields 55,000 WBC/mcL with 95% neutrophils. What is the most appropriate surgical management?
Explanation
Question 21
A 12-year-old boy presents after a mild knee sprain. Radiographs reveal an incidental eccentric, lytic, bubbly lesion with sclerotic margins in the distal femur metaphysis.
What is the most appropriate management for this patient?
Explanation
Question 22
A 68-year-old patient presents with a painful total knee arthroplasty 3 years post-operatively. ESR is 40 mm/hr and CRP is 15 mg/L. Aspiration yields 2,500 WBC/uL with 65% PMNs, and cultures are negative at 7 days. Which of the following biomarker tests would provide the highest specificity for confirming a periprosthetic joint infection (PJI) in this borderline scenario?
Explanation
Question 23
A 45-year-old male with a history of chronic heavy alcohol abuse presents with insidious onset groin pain. Radiographs reveal a subchondral crescent sign in the femoral head without collapse. Which pathophysiologic mechanism best explains this alcohol-induced condition?
Explanation
Question 24
A 25-year-old female presents with progressive shoulder weakness and pain. Radiographs demonstrate near-complete disappearance of the clavicle and acromion without an associated soft-tissue mass. Biopsy reveals extensive angiomatous and lymphatic proliferation.
What is the most likely diagnosis?
Explanation
Question 25
A 70-year-old female underwent primary total hip arthroplasty 3 weeks ago. She presents with 3 days of acute hip pain, erythema, and a draining sinus tract. She is hemodynamically stable. What is the most appropriate surgical management?
Explanation
Question 26
A 16-year-old male complains of distal femur pain. Imaging shows a permeative metaphyseal lesion with a 'sunburst' periosteal reaction. Biopsy confirms high-grade conventional osteosarcoma. What is the standard sequence of treatment for this patient?
Explanation
Question 27
A 55-year-old alcoholic male with known liver cirrhosis presents with a displaced femoral neck fracture. DEXA scanning reveals severe osteoporosis. Which of the following metabolic abnormalities most directly contributes to his poor bone density?
Explanation
Question 28
A patient presents with a chronically infected nonunion 6 months following an open reduction internal fixation of a tibial plateau fracture.
When planning definitive management, what is the most appropriate initial surgical step?
Explanation
Question 29
A 32-year-old female presents with progressive knee pain. Radiographs show an eccentric, lytic lesion in the proximal tibia extending to the subchondral bone. Biopsy reveals multinucleated giant cells interspersed with mononuclear stromal cells. Which medication specifically targets the primary pathophysiologic mechanism of this tumor?
Explanation
Question 30
A 75-year-old male is diagnosed with a chronic periprosthetic joint infection of his total knee arthroplasty, 2 years after his index surgery. Cultures grow methicillin-resistant Staphylococcus aureus (MRSA). Which surgical intervention is the recognized gold standard for this condition?
Explanation
Question 31
A chronic alcoholic patient is admitted for surgical management of an open tibia fracture. On post-operative day 3, he develops severe tachycardia, hypertension, diaphoresis, visual hallucinations, and extreme agitation. What is the most appropriate immediate pharmacologic treatment?
Explanation
Question 32
A 55-year-old male presents with deep thigh pain. Radiographs demonstrate a lytic lesion in the proximal femur with intralesional 'rings and arcs' calcifications. MRI shows extensive endosteal scalloping. Biopsy confirms a Grade 2 conventional chondrosarcoma. What is the primary modality of treatment?
Explanation
Question 33
During the first stage of a two-stage exchange arthroplasty for an infected total hip, the surgeon opts to place an articulating antibiotic PMMA spacer rather than a static spacer. Which of the following is a recognized advantage of an articulating spacer?
Explanation
Question 34
A 65-year-old male presents with severe back pain. Imaging shows a pathological compression fracture of L4. Laboratory tests reveal hypercalcemia, anemia, and an elevated total serum protein. Which diagnostic test is most essential to confirm the underlying diagnosis and identify the specific protein abnormality?
Explanation
Question 35
When evaluating a painful total hip arthroplasty for potential infection, which of the following represents a 'major' criterion for the diagnosis of PJI according to the Musculoskeletal Infection Society (MSIS) / International Consensus Meeting (ICM)?
Explanation
Question 36
A 60-year-old male with a 30-year history of severe alcohol abuse presents with a swollen, painless midfoot. He is not diabetic. Radiographs show fragmentation, massive osteolysis, and subluxation of the tarsometatarsal joints. What is the primary underlying mechanism of this joint destruction?
Explanation
Question 37
A 14-year-old boy presents with fever, malaise, and localized thigh pain. Radiographs reveal a diaphyseal destructive lesion with an 'onion-skin' periosteal reaction. Which specific chromosomal translocation is the diagnostic hallmark of the most likely bone tumor?
Explanation
Question 38
Which of the following synovial fluid biomarkers demonstrates the highest combined sensitivity and specificity for diagnosing periprosthetic joint infection (PJI) in the setting of a concurrent systemic inflammatory disease?
Explanation
Question 39
An asymptomatic 12-year-old boy presents after a mild knee injury. Radiographs show a well-circumscribed, eccentrically located, multilobulated radiolucent lesion with a sclerotic margin in the distal femoral metaphysis.
What is the most appropriate next step in management?
Explanation
Question 40
A 25-year-old patient presents with progressive, painless shoulder weakness and deformity over several years. Radiographs reveal progressive resorption of the proximal humerus and glenoid without evidence of malignant cells or infection.
What is the pathophysiological mechanism of this disease?
Explanation
Question 41
A 45-year-old man with a history of severe alcohol use disorder presents with bilateral groin pain. MRI reveals bilateral femoral head avascular necrosis (Ficat Stage II). How does chronic alcohol consumption primarily contribute to osteonecrosis?
Explanation
Question 42
A 65-year-old patient who underwent total knee arthroplasty 3 weeks ago presents with acute onset of knee pain, swelling, and erythema for 2 days. Synovial fluid aspiration yields a WBC count of 35,000 cells/uL with 90% PMNs. What is the most appropriate surgical management?
Explanation
Question 43
A patient develops a deep wound infection with hardware exposure 10 days following an open reduction and internal fixation of a distal tibia fracture.
The hardware remains rigidly fixed. What is the most appropriate initial management strategy?
Explanation
Question 44
A 40-year-old patient has an incidentally discovered cartilaginous lesion in the proximal humerus. Which of the following findings is most suggestive of secondary malignant transformation to chondrosarcoma?
Explanation
Question 45
A 50-year-old chronic alcoholic presents with a painless, swollen, and deformed midfoot. Radiographs show tarsometatarsal destruction, fragmentation, and subluxation. What is the primary underlying etiology of this condition?
Explanation
Question 46
Cutibacterium acnes is a common cause of periprosthetic joint infection, particularly following shoulder arthroplasty. Which of the following best describes the microbiological characteristics of this organism?
Explanation
Question 47
A 19-year-old male is diagnosed with Gorham-Stout disease of the pelvis and proximal femur. Which of the following systemic pharmacological treatments has been most commonly utilized to slow down the osteolytic process in this disease?
Explanation
Question 48
During a revision total hip arthroplasty for presumed PJI, the explanted components are sent for sonication. What is the primary purpose of sonication in this setting?
Explanation
Question 49
A 35-year-old patient with severe alcohol use disorder sustains a closed tibial shaft fracture. Chronic alcohol consumption impairs fracture healing through which of the following mechanisms?
Explanation
Question 50
A 32-year-old woman presents with knee pain. Radiographs reveal an eccentric, lytic lesion in the proximal tibial epiphysis extending to the subchondral bone without a sclerotic rim. Biopsy confirms a Giant Cell Tumor (GCT) of bone. Denosumab may be used in the treatment of advanced cases. What is its mechanism of action?
Explanation
Question 51
According to the 2018 International Consensus Meeting (ICM) criteria for Periprosthetic Joint Infection, which of the following is considered a major criterion for definitive diagnosis?
Explanation
Question 52
A 16-year-old male complains of right thigh pain that is worse at night and dramatically relieved by ibuprofen. Imaging shows a cortical thickening with a 7 mm radiolucent nidus in the femoral diaphysis. Radiofrequency ablation (RFA) is planned. What is the most critical anatomical consideration when performing RFA for this lesion?
Explanation
Question 53
A patient develops a necrotizing soft tissue infection 5 days after internal fixation of a pilon fracture, resulting in exposed hardware and necrotic tendons over the anterior ankle.
Following serial debridements resulting in a sterile but large composite defect, what is the best reconstructive option for soft tissue coverage?
Explanation
Question 54
A 14-year-old asymptomatic boy underwent knee radiographs following minor trauma, revealing the incidental finding shown.
If a biopsy were performed, what would be the most likely histopathological finding?
Explanation
Question 55
A 14-year-old boy presents with mild thigh pain. Radiographs show a well-circumscribed, eccentric, lucent lesion with a sclerotic rim in the distal femoral metaphysis.
If this lesion occupies 60% of the bone diameter, what is the recommended management?
Explanation
Question 56
A 68-year-old man presents with a painful total knee arthroplasty 3 years postoperatively. Synovial fluid analysis reveals a WBC count of 3,500 cells/uL with 75% PMNs. Which of the following synovial fluid biomarkers has the highest specificity for confirming a periprosthetic joint infection (PJI) according to the 2018 ICM criteria?
Explanation
Question 57
A 42-year-old man with a history of chronic alcoholism presents with bilateral hip pain. MRI confirms stage II osteonecrosis of the femoral head. What is the primary pathophysiological mechanism by which chronic alcohol abuse induces osteonecrosis?
Explanation
Question 58
A 28-year-old woman presents with progressive shoulder pain and profound regional bone resorption seen on imaging.
Biopsy demonstrates angiomatosis with thin-walled vascular channels replacing bone without cellular atypia. What is the most likely diagnosis?

Explanation
Question 59
A 72-year-old female underwent a primary total hip arthroplasty 3 weeks ago. She presents with 3 days of fever, hip pain, and a draining sinus tract. What is the most appropriate definitive surgical management?
Explanation
Question 60
A 16-year-old boy is diagnosed with high-grade conventional osteosarcoma of the distal femur. He undergoes 10 weeks of neoadjuvant chemotherapy. Which of the following is the most important prognostic factor for long-term survival in this patient?
Explanation
Question 61
A patient undergoes revision total knee arthroplasty for a suspected PJI, as depicted in the clinical image.
According to current guidelines, how many periprosthetic tissue samples should ideally be obtained using separate instruments to optimize culture yield?

Explanation
Question 62
A 55-year-old male with chronic alcohol dependence sustains a displaced femoral neck fracture. He is scheduled for a hemiarthroplasty. He is at increased risk for which of the following postoperative complications compared to a non-alcoholic matched cohort?
Explanation
Question 63
A 35-year-old woman presents with knee pain. Imaging reveals an eccentric, lytic lesion in the proximal tibia extending to the subchondral bone, characteristic of a giant cell tumor. Neoadjuvant treatment with denosumab is considered. What is the mechanism of action of denosumab?
Explanation
Question 64
A 78-year-old man with severe medical comorbidities has a chronic PJI of the hip caused by coagulase-negative Staphylococcus. He is deemed medically unfit for explantation or revision surgery. Chronic oral suppressive antibiotic therapy is planned. Which of the following is essential for the success of this strategy?
Explanation
Question 65
A patient with confirmed Gorham-Stout disease (massive osteolysis) of the cervicothoracic spine and ribs is admitted.
What is the most common life-threatening complication associated with this specific anatomical presentation?
Explanation
Question 66
A 45-year-old male with a history of heavy daily alcohol use is admitted for an open tibia fracture. On postoperative day 3, he becomes tachycardic, hypertensive, diaphoretic, and severely agitated with visual hallucinations. What is the most appropriate immediate pharmacologic management?
Explanation
Question 67
A 62-year-old man with known renal cell carcinoma presents with a solitary, destructive lytic lesion in the proximal humerus with impending fracture. Before proceeding with prophylactic internal fixation, what preoperative intervention is highly recommended?
Explanation
Question 68
During a revision hip arthroplasty for suspected PJI, the explanted components are sent for sonication.
What is the primary purpose of sonicating the explanted hardware in diagnosing PJI?

Explanation
Question 69
Chronic heavy alcohol consumption is a known secondary cause of osteoporosis. Which of the following best describes its direct effect on bone remodeling?
Explanation
Question 70
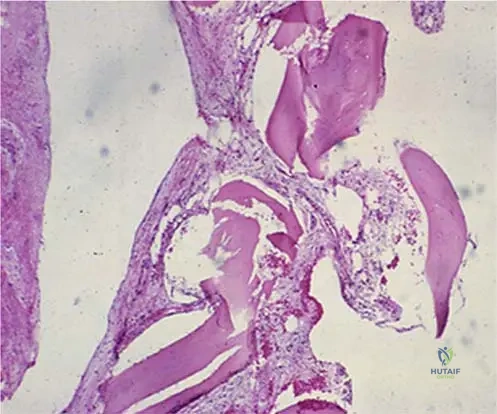
A 28-year-old male presents with a progressive, painless loss of function in his left shoulder over the past two years. Radiographs demonstrate the 'vanishing bone' appearance of the clavicle and scapula as seen in the provided image.
Which of the following is the defining histological characteristic of this condition?
Explanation
Question 71
A 14-year-old boy presents to the emergency department with severe thigh pain after a minor fall. Radiographs demonstrate a displaced transverse fracture through a large, eccentric, multiloculated lytic lesion in the distal femur metaphysis, as seen in the imaging.
If a biopsy were performed, what would be the expected histopathological findings?
Explanation
Question 72
A 65-year-old male with a 5-year history of a primary total hip arthroplasty presents with 4 days of acute severe hip pain, fevers, and chills following a dental extraction. Radiographs show well-fixed implants without lucencies. Aspiration yields 65,000 WBC/uL with 95% neutrophils. What is the most appropriate initial surgical management?
Explanation
Question 73
A 42-year-old male with a known history of severe chronic alcohol abuse is admitted for an intramedullary nailing of a closed tibia fracture. On postoperative day 3, he becomes agitated, profoundly tachycardic (135 bpm), diaphoretic, and begins experiencing visual hallucinations. What is the most appropriate first-line pharmacologic treatment for this patient's acute systemic condition?
Explanation
Question 74
A 55-year-old heavy alcohol user with known multifocal medullary bone infarcts in the distal femur and proximal tibia presents with a 3-month history of rapidly worsening knee pain. Recent imaging reveals a destructive, permeative soft-tissue mass arising from an area of chronic infarction in the distal femur. What is the most common malignant transformation associated with this chronic lesion?
Explanation
Question 75
A 70-year-old female complains of persistent pain 2 years following a total knee arthroplasty. Aspiration yields synovial fluid with 2,500 WBC/uL and 75% PMNs. Serum CRP is 12 mg/L. Which of the following synovial fluid biomarkers offers the highest specificity for confirming a chronic periprosthetic joint infection?
Explanation
Question 76
A patient develops a deep periprosthetic infection 4 weeks after a total knee arthroplasty, caused by a virulent strain of Staphylococcus aureus as seen in similar iatrogenic hardware infections.
Which essential component of the biofilm matrix is primarily responsible for adhering the bacteria to the implant and protecting them from systemic antibiotics?
Explanation
Question 77
A 25-year-old male presents with a progressive vanishing of the clavicle and ribs over several years, leading to a visible deformity and aching pain. A biopsy of the remaining clavicular bone shows extensive vascular proliferation replacing the normal bone trabeculae.
What is the most likely diagnosis?

Explanation
Question 78
A 30-year-old female undergoes intralesional curettage for a recurrent Giant Cell Tumor (GCT) of the sacrum. Due to the high risk of surgical morbidity, she is pre-operatively managed with denosumab to consolidate the tumor margins. What is the precise mechanism of action of this medication?
Explanation
Question 79
During the workup of a painful total knee arthroplasty, a synovial fluid sample is sent for alpha-defensin testing. What specific cellular process does the presence of alpha-defensin primarily reflect in the context of periprosthetic joint infection (PJI)?
Explanation
Question 80
A 40-year-old male with severe, chronic alcohol use disorder develops bilateral femoral head osteonecrosis. What is the primary cellular mechanism by which chronic alcohol abuse induces this condition?
Explanation
Question 81
A 68-year-old female presents with an acutely painful total hip arthroplasty 14 days post-operatively. Her vitals are stable, but the wound is actively draining purulent fluid. Radiographs show well-fixed components. According to current guidelines, what is the most critical indication that supports a Debridement, Antibiotics, and Implant Retention (DAIR) procedure over a 2-stage revision?
Explanation
Question 82
A 15-year-old male treated with neoadjuvant chemotherapy for a distal femur osteosarcoma undergoes wide surgical resection. Pathologic evaluation of the excised tumor is performed to determine the histologic response. According to the Huvos grading system, what percentage of tumor necrosis represents a 'good' response associated with improved survival?
Explanation
Question 83
A 50-year-old alcoholic male undergoes emergency open reduction and internal fixation of a severe tibial plateau fracture. On post-operative day 3, he develops severe agitation, tachycardia, diaphoresis, and visual hallucinations. What is the most appropriate first-line pharmacologic treatment for this acute complication?
Explanation
Question 84
A 60-year-old male presents with deep pelvic pain. Radiographs and subsequent MRI demonstrate a large, destructive, expansile lesion in the ilium with classic 'rings and arcs' calcifications. A core needle biopsy confirms a Grade 2 conventional chondrosarcoma. What is the standard of care for this lesion?
Explanation
Question 85
A 14-year-old girl is found to have a permeative diaphyseal lesion in her femur with an associated 'onion skin' periosteal reaction. A biopsy is planned to confirm the suspected diagnosis of Ewing sarcoma. Which cytogenetic abnormality is most likely to be identified?
Explanation
Question 86
During a revision total hip arthroplasty for a suspected chronic periprosthetic joint infection, the removed components undergo sonication in the microbiology lab. What is the primary purpose of utilizing sonication in this scenario?
Explanation
Question 87
A 10-year-old boy sustains a minor twisting injury while running and presents with leg pain. Radiographs reveal a pathologic fracture through a cortically based, eccentric, bubbly radiolucent lesion in the distal tibial metaphysis.
What is the most appropriate initial management for this specific lesion?
Explanation
Question 88
Which of the following organisms is most notorious for causing chronic, indolent periprosthetic joint infections due to its robust ability to produce a polysaccharide intercellular adhesin (PIA) that forms a resilient protective biofilm?
Explanation
Question 89
A 55-year-old male with a history of heavy, daily alcohol consumption presents with an acutely swollen, erythematous, and exquisitely tender first metatarsophalangeal (MTP) joint. Joint aspiration yields negatively birefringent needle-shaped crystals. How does chronic alcohol consumption primarily exacerbate this specific condition?
Explanation
Question 90
A 65-year-old male presents with generalized bone pain, severe fatigue, and a large radiolucent lesion in the proximal femur. Laboratory workup shows hypercalcemia, normocytic anemia, and an M-spike on serum protein electrophoresis. Which distinct radiographic characteristic of the bone lesion is classically associated with the underlying pathophysiology of this disease?
Explanation
Question 91
When preparing an articulating polymethylmethacrylate (PMMA) antibiotic spacer for a two-stage revision of an infected total knee arthroplasty, which specific characteristic of the chosen antibiotic is most crucial to ensure effective local elution and efficacy?
Explanation
Question 92
A 24-year-old female presents with progressive, dull aching shoulder pain over 2 years and notable deformity. Radiographs show dramatic resorption of the proximal humerus and scapula, as seen in the provided image. Biopsy reveals benign vascular proliferation with thin-walled channels replacing bone, without any malignant features.
What is the underlying pathophysiology of this condition?
Explanation
Question 93
A 14-year-old male sustains a minor twisting injury to his ankle. Radiographs demonstrate an incidental eccentrically located, multilobulated radiolucent lesion with a sclerotic margin in the distal tibial metaphysis.
If advanced imaging confirms this lesion occupies 60% of the bone's cross-sectional diameter, what is the most appropriate management?
Explanation
Question 94
A 65-year-old male presents with acute onset of severe right knee pain, swelling, and erythema 2 weeks after an uncomplicated primary total knee arthroplasty (TKA). Joint aspiration yields 45,000 WBC/uL with 92% neutrophils, and the implant appears well-fixed on radiographs. What is the most appropriate initial surgical management?
Explanation
Question 95
A 52-year-old male with a known history of chronic, severe alcohol use disorder is admitted for surgical fixation of a closed highly comminuted tibial plateau fracture. On postoperative day 3, he develops tachycardia, hypertension, diaphoresis, and severe agitation with visual hallucinations. What is the primary mechanism of the first-line pharmacologic treatment for this patient's acute postoperative complication?
Explanation
None
