ABOS Part I & OITE Orthopaedic Trauma Review: Shoulder, Elbow, Hand Fractures | Part 22201
Key Takeaway
This module provides 51 advanced multiple-choice questions for ABOS Part I and AAOS OITE, focusing on orthopaedic trauma. Topics include proximal humerus, radial head, olecranon, and distal humerus fractures, plus Jersey finger injuries. Detailed explanations cover diagnosis, management, and complications, offering a robust resource for board exam preparation.
ABOS Part I & OITE Orthopaedic Trauma Review: Shoulder, Elbow, Hand Fractures | Part 22201
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
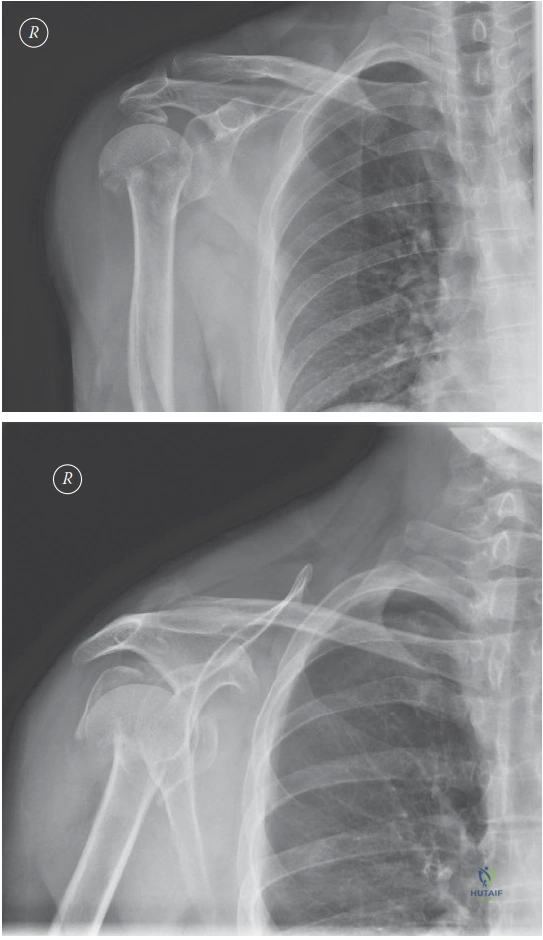
A 45-year-old active male presents to the emergency department after a fall directly onto his shoulder. He complains of severe pain and inability to move his left arm. Radiographs are obtained, as shown below. Based on the provided images and the patient's profile, which of the following best describes the fracture and the most appropriate initial management strategy?

Explanation
Correct Answer: C
The radiographs (AP and axillary lateral views) demonstrate a displaced fracture through the surgical neck of the humerus. There is no clear involvement of the greater or lesser tuberosities as separate fragments, making it a Neer 2-part surgical neck fracture. Given the patient's age (45 years old) and active lifestyle, a displaced fracture of this nature warrants consideration for surgical intervention to optimize functional outcome and reduce the risk of malunion or nonunion. Initial management typically involves immobilization in a sling for comfort and pain control, followed by a thorough discussion of operative versus non-operative options. While non-operative treatment can be considered for patients with very low functional demands, it is less reliably associated with good functional outcomes in active, younger patients with displaced fractures.
Option A is incorrect because the fracture is clearly displaced, not minimally displaced. While a sling is part of initial management, early range of motion would be inappropriate for a displaced fracture before definitive treatment.
Option B is incorrect because the images do not clearly show a 3-part fracture involving the greater tuberosity as a separate, displaced fragment. Immediate ORIF is a treatment option, but the description of the fracture is inaccurate.
Option D is incorrect because the fracture does not appear to be a 4-part fracture with significant head displacement, which would typically involve the anatomical neck, surgical neck, and both tuberosities, often with severe disruption of the blood supply. Reverse total shoulder arthroplasty is generally reserved for older patients with irreparable rotator cuff tears or complex 3- and 4-part fractures, especially in the elderly.
Option E is incorrect because the fracture is displaced, not non-displaced, and it is a surgical neck fracture, not an anatomical neck fracture. Anatomical neck fractures carry a higher risk of osteonecrosis due to disruption of the blood supply to the humeral head.
Question 2
Following the initial assessment, the 45-year-old active male with the displaced proximal humerus surgical neck fracture (as seen in the provided images) elects for surgical management. The orthopedic surgeon plans for open reduction internal fixation (ORIF) using a proximal humerus locking plate via a deltopectoral approach. During the patient counseling, which of the following statements regarding the rationale for surgical intervention in this specific patient is most accurate?
Explanation
Correct Answer: B
For active, physiologically younger patients with displaced proximal humerus fractures, surgical intervention (such as ORIF with a locking plate) is often recommended because it offers a more reliable means to achieve anatomical reduction and stable fixation, which in turn leads to better functional outcomes and a reduced risk of painful malunion or nonunion. While non-operative treatment can result in functional healing, it is less predictable for displaced fractures in this demographic.
Option A is incorrect because surgical fixation is not universally superior for all proximal humerus fractures. Many minimally displaced or stable fractures, especially in less active or elderly patients, are successfully managed non-operatively.
Option C is incorrect because while osteonecrosis is a potential complication of proximal humerus fractures, it is primarily related to the initial injury's disruption of the blood supply, particularly in 3- and 4-part fractures or anatomical neck fractures, rather than being a common complication of non-operative management itself. The primary goal of surgery for a surgical neck fracture in an active patient is functional restoration and prevention of malunion/nonunion.
Option D is incorrect. The PROFHER trial (Proximal Fracture of the Humerus: a Randomised Evaluation of Reverse Shoulder Arthroplasty) actually found no significant difference in patient-reported outcomes between surgical and non-surgical treatment for displaced proximal humerus fractures after 2 years. This is a critical piece of evidence that informs the nuanced discussion with patients, especially those with lower functional demands.
Option E is incorrect. Non-operative treatment is not absolutely contraindicated for all displaced proximal humerus fractures in patients under 60. The decision is individualized, considering fracture pattern, displacement, patient comorbidities, and functional demands. However, for significantly displaced fractures in active younger patients, surgery is generally favored for more predictable outcomes.
Question 3
The orthopedic surgeon proceeds with open reduction internal fixation (ORIF) of the displaced proximal humerus surgical neck fracture in the 45-year-old active male, utilizing a deltopectoral approach. During this approach, which of the following neurovascular structures is most directly at risk of iatrogenic injury?
Explanation
Correct Answer: C
The axillary nerve is the neurovascular structure most directly at risk during a deltopectoral approach to the proximal humerus, especially when dissecting laterally or extending the approach distally. The axillary nerve wraps around the surgical neck of the humerus, approximately 5-7 cm distal to the acromion, and innervates the deltoid and teres minor muscles. Care must be taken to protect it during plate application and screw insertion, particularly with bicortical screws.
Option A (Radial nerve) is primarily at risk with humeral shaft fractures, particularly in the spiral groove, and is less directly exposed or at risk during a standard deltopectoral approach to the proximal humerus.
Option B (Ulnar nerve) is located medially at the elbow (cubital tunnel) and is not typically at risk during a deltopectoral approach to the proximal humerus.
Option D (Median nerve) is located in the anterior compartment of the arm and forearm and is not typically at risk during a deltopectoral approach to the proximal humerus.
Option E (Long thoracic nerve) innervates the serratus anterior muscle and runs along the lateral chest wall. While it can be injured in shoulder girdle trauma or surgery involving the scapula, it is not directly at risk during a deltopectoral approach to the proximal humerus.
Question 4
Six months after successful open reduction internal fixation (ORIF) of his displaced proximal humerus surgical neck fracture, the 45-year-old active male reports persistent shoulder pain and limited range of motion, particularly in external rotation and abduction. Radiographs show good fracture healing and plate position. Physical examination reveals tenderness over the greater tuberosity and pain with resisted external rotation. Which of the following is the most likely cause of his ongoing symptoms?
Explanation
Correct Answer: C
Persistent shoulder pain and limited range of motion, especially with tenderness over the greater tuberosity and pain with resisted external rotation, 6 months after ORIF of a proximal humerus fracture, with good fracture healing and plate position, strongly suggest subacromial impingement. This can occur due to prominent hardware (e.g., screws extending superiorly, or the plate itself being too proud) or a subtle malunion of the greater tuberosity, which can impinge on the acromion during abduction and rotation. Pain with resisted external rotation specifically points towards rotator cuff involvement, which can be secondary to impingement.
Option A (Avascular necrosis of the humeral head) typically presents with progressive pain and collapse of the humeral head, often visible on radiographs as increased density or flattening. While a risk, the description of 'good fracture healing and plate position' makes it less likely to be the primary cause of these specific symptoms at 6 months, especially if the fracture was a surgical neck fracture with intact blood supply to the head.
Option B (Nonunion of the surgical neck fracture) would typically present with persistent pain, instability, and lack of radiographic healing. The question states 'good fracture healing,' ruling out nonunion.
Option D (Axillary nerve palsy) would primarily manifest as deltoid weakness (difficulty with abduction) and sensory loss over the lateral shoulder. While it can cause weakness and some pain, the specific findings of tenderness over the greater tuberosity and pain with resisted external rotation point more towards a mechanical impingement issue rather than isolated nerve palsy.
Option E (Adhesive capsulitis), or 'frozen shoulder,' can cause significant pain and global restriction of range of motion. While it can occur after shoulder trauma or surgery, the specific findings of tenderness over the greater tuberosity and pain with resisted external rotation, combined with the possibility of hardware prominence, make impingement a more specific and likely diagnosis in this context.
Question 5
A 78-year-old sedentary female with low functional demands presents with a similar displaced proximal humerus surgical neck fracture as shown in the images. She has significant comorbidities, including severe osteoporosis and poorly controlled diabetes. Given her profile, which of the following management strategies would be most appropriate to discuss as a primary option?
Explanation
Correct Answer: C
For an elderly, sedentary patient with low functional demands and significant comorbidities (severe osteoporosis, poorly controlled diabetes), non-operative management with a sling, pain control, and early gentle pendulum exercises is often the most appropriate primary option. Surgical risks are higher in this population, and the potential benefits of surgery in terms of functional outcome may not outweigh these risks, especially given low functional demands. The PROFHER trial supports that for many displaced proximal humerus fractures, non-operative treatment can yield similar patient-reported outcomes to surgery, particularly in less active individuals.
Option A (Immediate ORIF) is less appropriate due to her age, low functional demands, and significant comorbidities, which increase surgical risks (e.g., infection, poor bone quality for fixation, anesthetic risks). The benefits of surgery may not justify the risks in this specific patient.
Option B (Reverse total shoulder arthroplasty) is typically reserved for complex 3- or 4-part fractures, fractures with associated rotator cuff pathology, or failed ORIF, especially in older patients. While it's an option for some elderly patients, for a 2-part surgical neck fracture, it's generally an overtreatment, especially as a primary option, unless there are specific indications like severe comminution or pre-existing cuff arthropathy.
Option D (Hemiarthroplasty) is considered for complex 3- or 4-part fractures, particularly in older patients with compromised blood supply to the humeral head, but it is generally not indicated for a 2-part surgical neck fracture where the humeral head's blood supply is often preserved and fixation is feasible.
Option E (Delayed ORIF after optimizing comorbidities) might be considered if surgery were deemed necessary, but for this patient's profile and fracture type, non-operative management is often the preferred initial discussion point, rather than assuming surgery is the ultimate goal.
Question 6
During the open reduction internal fixation (ORIF) of the displaced proximal humerus surgical neck fracture in the 45-year-old active male, the surgeon uses a proximal humerus locking plate. Which of the following is a primary biomechanical advantage of a locking plate system in this type of fracture compared to a conventional non-locking plate?
Explanation
Correct Answer: B
A primary biomechanical advantage of a locking plate system is that it provides a fixed-angle construct. The screws lock into the plate, creating a stable angular construct that acts like an internal fixator. This is particularly advantageous in osteoporotic bone or comminuted fractures where traditional screws might pull out. The locking mechanism allows the plate to act as a scaffold, supporting the articular segment and resisting collapse, rather than relying solely on screw purchase into potentially poor bone quality.
Option A is incorrect. Conventional non-locking plates, especially with lag screws, are designed to achieve interfragmentary compression. While locking plates can achieve some compression with specific techniques (e.g., using a compression hole), their primary advantage is not greater compression but rather angular stability.
Option C is incorrect. While locking plates can be more forgiving in terms of screw trajectory within the humeral head, precise screw placement is still crucial to avoid articular penetration and to maximize purchase in the strongest bone (e.g., calcar region). It does not mean less precise placement is acceptable for adequate fixation.
Option D is incorrect. Locking plates provide rigid fixation, which generally limits micromotion at the fracture site. While some controlled micromotion can be beneficial for healing (relative stability), the primary goal of a locking plate in a displaced proximal humerus fracture is often absolute stability to maintain reduction and prevent collapse, especially in the metaphyseal region. Excessive micromotion would be detrimental.
Option E is incorrect. While locking plates provide excellent stability, they do not eliminate the need for bone grafting in cases of significant metaphyseal comminution or bone loss, where grafting may still be necessary to promote healing and prevent collapse.
Question 7
A 45-year-old male with a displaced proximal humerus surgical neck fracture, as depicted in the radiographs, is considering surgical intervention. During the discussion of potential complications, the surgeon emphasizes the risk of osteonecrosis of the humeral head. Which of the following fracture characteristics is most strongly associated with an increased risk of avascular necrosis (AVN) of the humeral head?
Explanation
Correct Answer: C
A Neer 4-part fracture with significant displacement is most strongly associated with an increased risk of avascular necrosis (AVN) of the humeral head. In a 4-part fracture, the humeral head is completely separated from its muscular and capsular attachments, leading to a severe disruption of its blood supply, particularly the arcuate artery (branch of the anterior circumflex humeral artery) and posterior circumflex humeral artery. This devascularization significantly increases the risk of AVN.
Option A (Isolated greater tuberosity fracture) typically does not significantly compromise the blood supply to the humeral head, and thus carries a low risk of AVN.
Option B (Minimally displaced surgical neck fracture) generally has a low risk of AVN because the blood supply to the humeral head, primarily through the ascending branch of the anterior circumflex humeral artery and the posterior circumflex humeral artery, is often preserved.
Option D (Isolated lesser tuberosity fracture) also typically does not significantly compromise the blood supply to the humeral head and has a low risk of AVN.
Option E (Non-displaced anatomical neck fracture), while involving the anatomical neck, is non-displaced. However, even non-displaced anatomical neck fractures carry a higher risk of AVN than surgical neck fractures because the fracture line is closer to the main blood supply entering the head. But a displaced 4-part fracture represents a much more severe disruption of the blood supply, making it the highest risk category among the choices.
Question 8
The 45-year-old active male, having undergone successful ORIF for his displaced proximal humerus surgical neck fracture, is now 6 weeks post-operative. He is progressing well with passive range of motion exercises. Which of the following is the most appropriate next step in his rehabilitation protocol?
Explanation
Correct Answer: B
At 6 weeks post-ORIF for a proximal humerus fracture, with good healing progress, the typical rehabilitation protocol transitions from passive range of motion (PROM) to active assisted range of motion (AAROM). This allows the patient to begin engaging their muscles to assist movement, promoting muscle activation and preventing stiffness, while still protecting the healing fracture site from excessive stress. Active abduction against gravity is often avoided initially to protect the deltoid and rotator cuff repair (if any) and the healing fracture from significant shear forces.
Option A is incorrect. Immediate return to full unrestricted activities is far too aggressive at 6 weeks post-ORIF and would risk re-fracture, hardware failure, or soft tissue injury.
Option C is incorrect. Continued strict immobilization for another 6 weeks would lead to significant shoulder stiffness and poor functional outcomes. Early, controlled motion is crucial for shoulder rehabilitation.
Option D is incorrect. Aggressive strengthening exercises are typically initiated much later in the rehabilitation process (e.g., 10-12 weeks or more post-op), after sufficient bone healing and restoration of basic range of motion. Starting too early could compromise fixation or healing.
Option E is incorrect. Discontinuing physical therapy at 6 weeks would be detrimental to the patient's recovery. Rehabilitation for a proximal humerus fracture is a prolonged process, often lasting several months, to regain full strength and function.
Question 9
A 45-year-old active male presents with a displaced proximal humerus surgical neck fracture, as shown in the images. He is concerned about the long-term implications of non-operative management, specifically the risk of malunion. Which of the following is the most common functional consequence of a significant malunion of a proximal humerus fracture?
Explanation
Correct Answer: B
A significant malunion of a proximal humerus fracture, especially with varus angulation or displacement of the tuberosities, can alter the normal anatomy of the shoulder joint. This often leads to subacromial impingement, where the humeral head or greater tuberosity abuts against the acromion during shoulder movement. This impingement causes pain and significantly limits the range of motion, particularly abduction and external rotation, which are critical for overhead activities and daily functions.
Option A (Chronic elbow stiffness and pain) is not a direct consequence of a proximal humerus malunion. Elbow issues are more common with distal humerus fractures or prolonged immobilization of the elbow.
Option C (Radial nerve palsy with wrist drop) is associated with humeral shaft fractures, not typically with proximal humerus malunion.
Option D (Recurrent shoulder dislocation) is usually a consequence of glenohumeral instability, often due to labral tears or bony defects, not typically a direct result of a proximal humerus malunion, although severe malunion could theoretically contribute to altered joint mechanics.
Option E (Brachial plexus injury with complete arm paralysis) is a severe acute complication of high-energy trauma or fracture-dislocations, not a chronic consequence of malunion.
Question 10
During the surgical approach for open reduction internal fixation of a proximal humerus fracture, the deltopectoral interval is utilized. Which of the following anatomical landmarks is crucial for identifying and safely developing this interval?
Explanation
Correct Answer: C
The cephalic vein is the crucial anatomical landmark for identifying and safely developing the deltopectoral interval. This vein consistently runs within the groove between the deltoid and pectoralis major muscles. By identifying the cephalic vein, the surgeon can safely separate these two muscles, either retracting the deltoid laterally and the pectoralis major medially, or vice versa, while protecting the vein (often retracted laterally with the deltoid) to gain access to the anterior aspect of the shoulder joint and proximal humerus.
Option A is incorrect. The posterior border of the deltoid and anterior border of the teres major define a different surgical interval (posterior approach to the shoulder), not the deltopectoral interval.
Option B is incorrect. While the deltopectoral interval is indeed between the deltoid and pectoralis major, simply stating their borders doesn't identify the specific, consistent landmark (the cephalic vein) that guides the dissection.
Option D is incorrect. The axillary nerve runs around the surgical neck of the humerus and is a structure to be protected after the deltopectoral interval is developed and deeper dissection proceeds. It does not define the interval itself.
Option E is incorrect. The long head of the biceps tendon is an intra-articular structure and is encountered much deeper in the dissection, not as a landmark for the initial deltopectoral interval.
Question 11
The PROFHER trial, mentioned in the case discussion, compared surgical intervention (ORIF) to non-operative treatment for displaced proximal humerus fractures. For the 45-year-old active male with a displaced surgical neck fracture, how should the findings of the PROFHER trial influence the patient counseling regarding his treatment options?
Explanation
Correct Answer: C
The PROFHER trial (Proximal Fracture of the Humerus: a Randomised Evaluation of Reverse Shoulder Arthroplasty) is a landmark study that found no significant difference in patient-reported outcomes (e.g., Oxford Shoulder Score) between surgical intervention (ORIF) and non-operative treatment for displaced proximal humerus fractures at 2 years. This is a crucial piece of evidence that informs shared decision-making. It suggests that for many patients, including those with displaced fractures, non-operative treatment can yield comparable functional results to surgery. Therefore, it highlights that non-operative treatment is a reasonable option, particularly if patient demands are lower, surgical risks are high, or the patient prefers to avoid surgery. For an active 45-year-old, while surgery might still be favored for more predictable anatomical reduction and stability, the trial's findings necessitate a nuanced discussion about the potential for good outcomes with non-operative care, especially if the patient is hesitant about surgery.
Option A is incorrect. The trial did not prove surgery is always superior; in fact, it found no significant difference in outcomes.
Option B is incorrect. The trial does not suggest non-operative treatment is always preferred. It indicates comparable outcomes, allowing for individualized decision-making, but doesn't negate the role of surgery for specific fracture patterns or patient expectations.
Option D is incorrect. While the trial included a broad age range, its findings are relevant across adult populations with displaced proximal humerus fractures, including active younger patients, as it challenges the assumption of surgical superiority for all displaced fractures.
Option E is incorrect. The PROFHER trial did not support immediate reverse total shoulder arthroplasty for all displaced fractures. It focused on ORIF versus non-operative treatment, and reverse arthroplasty is a more complex procedure reserved for specific indications.
Question 12
A 45-year-old male sustains a fall onto an outstretched hand, resulting in a radial head fracture. Radiographs show a displaced, comminuted fracture involving 40% of the articular surface with a 3mm step-off, but no mechanical block to forearm rotation. Which Mason-Johnston classification best describes this injury?
Explanation
Correct Answer: C
Mason-Johnston Type III fractures are characterized by significant comminution and/or displacement, often involving more than 30% of the articular surface and/or displacement of more than 2mm, or with a mechanical block. While a Type II involves a single displaced fragment, a Type III implies more extensive disruption, typically precluding successful closed reduction and often requiring surgical intervention. In this case, the fracture involves 40% of the articular surface and is comminuted with a 3mm step-off, clearly placing it in the Type III category. Type I is a non-displaced crack. Type IV involves an associated elbow dislocation.
Question 13
A 30-year-old male presents with persistent wrist pain and instability following a radial head fracture managed non-operatively 6 weeks ago. Initial radiographs showed a Mason-Johnston Type II radial head fracture. On examination, there is tenderness over the distal radio-ulnar joint (DRUJ) and a positive 'shuck test' at the wrist. What is the most likely underlying diagnosis causing these new symptoms?
Explanation
Correct Answer: C
The combination of a radial head fracture, interosseous membrane disruption (leading to proximal radial migration), and distal radio-ulnar joint (DRUJ) injury (manifested by wrist pain and instability/positive shuck test) constitutes an Essex-Lopresti lesion. This severe injury often leads to chronic pain and dysfunction if not recognized and treated appropriately, typically with radial head replacement and potentially DRUJ stabilization. Radial head non-union might cause local pain but wouldn't explain DRUJ instability. Heterotopic ossification and LCL insufficiency are elbow-centric and wouldn't directly cause DRUJ instability in this context. Cubital tunnel syndrome is a nerve compression issue.
Question 14
A 62-year-old female presents with a Mason-Johnston Type II radial head fracture with 2mm displacement and a palpable block to terminal forearm pronation. There is no associated elbow dislocation or other obvious ligamentous injury. What is the most appropriate initial management strategy?
Explanation
Correct Answer: B
A Mason-Johnston Type II fracture with a mechanical block to forearm rotation (even with only 2mm displacement) is a strong indication for surgical intervention, typically ORIF if the fragment is amenable. The mechanical block signifies impingement of the displaced fragment, which will prevent full range of motion and lead to chronic dysfunction if not addressed. Sling immobilization alone is insufficient. Radial head excision is generally reserved for severely comminuted fractures not amenable to ORIF, or in low-demand patients, and can lead to proximal radial migration and DRUJ issues. Radial head replacement is typically indicated for highly comminuted (Type III/IV) fractures not reconstructible, or in Essex-Lopresti injuries. Attempting closed reduction is unlikely to succeed with a palpable block from a displaced articular fragment.
Question 15
A 55-year-old painter presents with a Mason-Johnston Type III radial head fracture with 4 fragments, involving 60% of the articular surface. He is very active and desires a full return to function. There is no associated elbow dislocation. What is the preferred surgical option to restore function and stability?
Explanation
Correct Answer: C
For highly comminuted (Mason-Johnston Type III or IV) radial head fractures, particularly in active patients where restoration of articular congruity and preservation of radial length are critical, radial head replacement is often the preferred surgical option. ORIF may be difficult or impossible with 4 fragments involving 60% of the articular surface. Radial head excision can lead to proximal radial migration and DRUJ issues, especially in younger, active patients. Arthrodesis is a salvage procedure for end-stage arthritis or instability, not a primary option for acute fractures. Non-operative management is not appropriate for a significantly comminuted, displaced Type III fracture in an active individual.
Question 16
What is the primary concern when considering radial head excision for a comminuted radial head fracture in a young, active patient?
Explanation
Correct Answer: D
The primary concern with radial head excision, especially in younger, active patients, is the loss of longitudinal stability of the forearm, leading to proximal migration of the radius and subsequent distal radio-ulnar joint (DRUJ) instability. This can cause significant wrist pain and dysfunction. While elbow stiffness and heterotopic ossification are potential complications of any elbow trauma or surgery, proximal migration and DRUJ issues are specific and major drawbacks of radial head excision.
Question 17
Which surgical approach provides the best exposure for ORIF of a radial head fracture while minimizing the risk to the posterior interosseous nerve (PIN)?
Explanation
Correct Answer: A
The posterolateral approach, also known as the Kocher approach, is widely preferred for radial head fractures. It uses the interval between the anconeus and extensor carpi ulnaris (ECU) muscles. This approach protects the posterior interosseous nerve (PIN), which typically lies within the supinator muscle, distal and anterior to the radial head. The anterior (Henry) approach risks the PIN more directly, and medial or direct posterior approaches are generally not suitable for radial head fixation. The lateral approach with anconeus muscle split is similar to Kocher but the key is the safe interval.
Question 18
When performing open reduction and internal fixation (ORIF) of a radial head fracture, what is the ideal placement for fixation screws to minimize impingement with the capitellum during forearm rotation?
Explanation
Correct Answer: E
To avoid impingement of hardware against the capitellum, screws and plates should ideally be placed in the 'safe zone' of the radial head. This zone is typically defined as the non-articulating portion of the radial head that does not articulate with the capitellum through a full range of forearm rotation. This zone is generally considered to be a 110-degree arc on the radial head, typically in the posterolateral quadrant when the forearm is in neutral rotation, or approximately between 90 degrees of supination and 90 degrees of pronation. Placing hardware in the anterior, posterior, or superior articulating zones is prone to impingement and pain.
Question 19
Which of the following ligaments is most commonly injured in a 'terrible triad' injury of the elbow?
Explanation
Correct Answer: C
The 'terrible triad' of the elbow consists of a posterior elbow dislocation, a radial head fracture, and a coronoid process fracture. The most consistently injured ligament in this complex is the lateral ulnar collateral ligament (LUCL), which is crucial for posterolateral rotatory stability of the elbow. MCL injury can also occur, but the LUCL is the key structure disrupting posterolateral stability in this injury pattern. The annular ligament is injured as part of the radial head fracture, but the LUCL is the primary stabilizer injured in the dislocation component.
Question 20
A 40-year-old male undergoes radial head replacement for a complex Mason-Johnston Type III fracture. Post-operatively, he develops progressive elbow stiffness. Which complication is most likely contributing to this stiffness?
Explanation
Correct Answer: C
Heterotopic ossification (HO) is a common and challenging complication after elbow trauma and surgery, especially in the context of complex fractures and dislocations. It involves the formation of new bone in soft tissues around the joint, leading to progressive loss of motion and stiffness. While infection and aseptic loosening are possible complications, HO is particularly known for causing severe stiffness after elbow surgery. Radial and ulnar nerve palsies would primarily cause neurological symptoms rather than direct stiffness.
Question 21
A patient is scheduled for ORIF of a radial head fracture. Pre-operative assessment reveals a high-riding radial head relative to the ulna on the ipsilateral wrist X-ray. This finding suggests which associated injury?
Explanation
Correct Answer: D
A high-riding radial head (or a positive ulnar variance, relative shortening of the radius) on an ipsilateral wrist X-ray following a radial head fracture is a classic sign of an Essex-Lopresti lesion. This indicates disruption of the interosseous membrane and/or distal radio-ulnar joint, allowing for proximal migration of the radius due to the loss of the radial head's stabilizing effect. This finding is critical for surgical planning as it indicates the need for radial head replacement to restore radial length.
Question 22
A 45-year-old male sustains a direct fall onto his elbow, resulting in a displaced olecranon fracture. Which of the following structures is *least likely* to be directly involved in the primary function of the olecranon as an anatomical structure and lever arm for extension?
Explanation
Correct Answer: D
The olecranon serves as the primary insertion point for the triceps brachii tendon (A), forming a critical lever arm for elbow extension. The anconeus muscle (B) originates from the lateral epicondyle and inserts onto the lateral aspect of the olecranon and proximal ulna, assisting in extension and stabilizing the ulnohumeral joint. The joint capsule (C) encompasses the ulnohumeral joint, and its integrity is often compromised in intra-articular fractures. The ulnar nerve (E) runs in the cubital tunnel posterior to the medial epicondyle, making it vulnerable to injury with olecranon fractures or surgical approaches. The radial collateral ligament (D) is located laterally and stabilizes the humeroradial and proximal ulnar joints against varus stress, having a less direct role in the primary function of the olecranon's lever arm for extension compared to the other options. While indirect involvement or associated injury is possible, its direct contribution to the olecranon's lever arm function is less central.
Question 23
A 68-year-old female presents with an olecranon fracture classified as Mayo Type IIB. Which characteristic best describes this specific fracture pattern?
Explanation
Correct Answer: E
The Mayo Classification for olecranon fractures categorizes them based on displacement, stability, and comminution. Type II fractures are displaced. Subtype IIB specifically denotes a displaced, comminuted, yet stable fracture. Stability implies the ulnohumeral joint remains congruent despite the fracture, meaning the fracture is not associated with elbow instability or dislocation.
Question 24
A patient falls directly onto the point of their elbow. Which of the following olecranon fracture patterns is *most commonly* associated with this mechanism?
Explanation
Correct Answer: C
A direct fall onto the point of the elbow typically results in high-energy trauma, driving the olecranon directly against the trochlea. This commonly leads to highly comminuted fractures with significant articular involvement (C) due to the crushing force. Avulsion fractures (D) are more often due to indirect mechanisms (sudden triceps contraction). Transverse non-displaced fractures (A) or simple oblique fractures (B) can occur with direct trauma but are less characteristic of high-energy impact onto the olecranon apex. Anterior coronoid fractures (E) are often associated with posterior dislocations and varus posteromedial rotatory instability, not typically a direct impact mechanism to the olecranon apex itself.
Question 25
A 32-year-old male presents after a motorcycle accident with a suspected olecranon fracture. On examination, he has a visible deformity, swelling, and ecchymosis over the posterior elbow. He is unable to actively extend his elbow against gravity. What is the *most critical* initial finding to assess regarding ulnohumeral joint stability?
Explanation
Correct Answer: B
While all options are important, the question specifically asks for the 'most critical initial finding to assess regarding ulnohumeral joint stability' in the context of a suspected olecranon fracture. A palpable gap at the fracture site (B) directly indicates significant displacement of the olecranon, which often correlates with profound disruption of the triceps mechanism and compromise of the ulnohumeral joint's posterior stability. The inability to actively extend the elbow against gravity is already mentioned, which points to disruption. Varus/valgus stress testing (D) assesses collateral ligament integrity, which is important, but a displaced olecranon fragment itself significantly compromises the posterior stability. Assessment of ulnar nerve function (C) and distal neurovascular status (E) are crucial for managing complications but do not directly assess ulnohumeral mechanical stability related to the fracture pattern itself. Passive elbow flexion (A) provides information about potential stiffness but not acute stability.
Question 26
A 55-year-old patient presents with an olecranon fracture. Standard AP and lateral radiographs show a transverse, displaced fracture. What additional radiographic view is *most beneficial* for further characterization, particularly to assess comminution and articular involvement?
Explanation
Correct Answer: B
While standard AP and lateral views are essential, oblique views (B) provide additional perspectives that can be invaluable. They help to better delineate the fracture pattern, identify comminution not clearly seen on orthogonal views, and assess the extent of articular involvement (e.g., small intra-articular fragments or subtle step-offs). This detailed information is crucial for surgical planning. Radial head-capitellum view (A) is for radial head fractures. Axillary view (C) is typically for shoulder dislocations. Stress views (D) assess ligamentous instability. Contralateral views (E) are for comparing anatomical variations or growth plate status in children.
Question 27
Which of the following conditions is an absolute contraindication to non-operative management of an olecranon fracture?
Explanation
Correct Answer: D
An open fracture (D) with a breach in the skin over the fracture site is an absolute contraindication to non-operative management. This is due to the extremely high risk of infection, requiring urgent surgical debridement, irrigation, antibiotics, and stabilization. Patient preference (A) is a relative factor. An elderly, low-demand patient (B) or a completely non-displaced fracture (C) are typically indications for non-operative management. Mild comminution without articular step-off (E) can sometimes be managed non-operatively, especially if stable and nondisplaced.
Question 28
A 40-year-old healthy male sustains a simple transverse, displaced olecranon fracture with intact articular surface. Which surgical technique is generally considered the *gold standard* for fixation in this scenario?
Explanation
Correct Answer: D
For simple transverse, displaced olecranon fractures (especially Mayo Type IIA) with intact articular surface and good bone stock, tension band wiring (D) is considered the gold standard. It effectively converts tensile forces from the triceps pull into compressive forces at the fracture site, promoting healing and allowing for early mobilization. Plate and screw fixation (A) is preferred for comminuted fractures, unstable fractures, or osteoporotic bone. Intramedullary screw fixation (B) has limited, specific indications. Excision of the proximal fragment (C) is reserved for very small, distal fragments in low-demand patients or severely comminuted segments that cannot be reconstructed. Total elbow arthroplasty (E) is a salvage procedure for highly complex, unreconstructable fractures, especially in the elderly.
Question 29
When considering plate fixation for an olecranon fracture, which of the following scenarios would *most strongly* indicate a locking plate over a conventional compression plate?
Explanation
Correct Answer: C
Locking plates provide angular stability independent of plate-bone compression, making them particularly advantageous in osteoporotic bone or highly comminuted fractures (C) where conventional screw purchase may be inadequate. In these cases, locking screws 'lock' into the plate, creating a fixed-angle construct that resists collapse and provides stable fixation even with poor bone quality. Simple transverse (A) or oblique fractures (B) in good bone quality often respond well to tension band wiring or conventional compression plating. Avulsion fractures (D) are typically managed with tension band wiring or direct suture. Distal ulna shaft extension (E) would indicate a longer plate but not necessarily a locking plate without other factors.
Question 30
Following surgical fixation of an olecranon fracture, what is the *most common* long-term complication reported?
Explanation
Correct Answer: D
Stiffness and loss of range of motion, particularly extension, is the most common long-term complication following olecranon fracture fixation, occurring in a significant percentage of patients. While nonunion (A), ulnar nerve neuropathy (B), infection (C), and hardware failure (E) can occur, elbow stiffness is a near-universal concern that requires diligent rehabilitation and patient compliance to minimize its impact.
Question 31
During surgical exposure for an olecranon fracture, the ulnar nerve is identified. What is the *most appropriate* management strategy if the nerve is found to be intact but compressed by surrounding hematoma or scar tissue, especially in a fracture requiring internal fixation?
Explanation
Correct Answer: C
If the ulnar nerve is found to be compressed or at high risk of post-operative compression/irritation (e.g., due to hardware placement or significant swelling, or pre-existing cubital tunnel syndrome), anterior transposition (C) is often performed prophylactically or therapeutically. This moves the nerve out of the cubital tunnel and into a less constrained anterior position, reducing the risk of neuropathy. Neurolysis in situ (B) may be considered for milder cases but is less definitive if significant risk factors for ongoing compression are present. No intervention (A) would be inappropriate if compression is present or anticipated. Posterior interosseous nerve release (D) is for radial nerve issues. Immediate nerve graft (E) is for transected nerves.
Question 32
A 48-year-old male sustains a comminuted intra-articular distal humerus fracture (AO/OTA 13-C3) after a high-energy fall. Clinical examination reveals significant swelling and tenderness, but no neurovascular deficits. Plain radiographs confirm the fracture pattern. Given the complexity and need for anatomical reduction, which surgical approach is generally considered the 'workhorse' for optimal visualization of the entire articular surface and both columns?
Explanation
Correct Answer: D
For complex, comminuted intra-articular distal humerus fractures (AO/OTA 13-C3), a posterior approach with an olecranon osteotomy (e.g., Chevron osteotomy) provides the most extensive and direct visualization of the entire distal humeral articular surface and both columns. This panoramic view is critical for achieving precise anatomical reduction of articular fragments and applying robust plate fixation. Without this level of exposure, accurate reduction of multiple small articular fragments can be extremely challenging, leading to poor functional outcomes and post-traumatic arthritis.
Option A (Anterior approach) is generally reserved for specific fracture patterns like isolated capitellar fractures or for less complex supracondylar fractures, and does not provide adequate exposure for bicondylar C3 fractures.
Option B (Medial approach) primarily exposes the medial column and is insufficient for comprehensive management of a bicondylar fracture.
Option C (Lateral approach) primarily exposes the lateral column and capitellum, also insufficient for a C3 fracture.
Option E (Triceps-sparing posterior approach), while avoiding an osteotomy, often provides a more limited visualization of the articular surface compared to an olecranon osteotomy, making it less ideal for severely comminuted intra-articular fractures where precise articular reduction is paramount.
Question 33
Following open reduction and internal fixation (ORIF) of a bicondylar distal humerus fracture, a 68-year-old patient with known osteoporosis develops increasing pain and loss of reduction within the first few weeks post-operatively. Radiographs show screws backing out of the bone. What is the most likely cause of this early complication?
Explanation
Correct Answer: C
In osteoporotic patients, the primary concern for early mechanical complication after ORIF of a comminuted distal humerus fracture is hardware pull-out or failure. Poor bone quality provides inadequate purchase for screws, leading to loss of reduction and implant failure. This often necessitates specific techniques like locking plates, longer screws, and sometimes bone augmentation to achieve stable fixation. The scenario describes screws backing out, which is a direct manifestation of hardware pull-out.
Option A (Infection) is a possible complication but typically presents with signs like erythema, warmth, drainage, and systemic symptoms, not primarily with hardware backing out.
Option B (Heterotopic ossification) is a later complication that causes stiffness and new bone formation, not early hardware failure.
Option D (Ulnar nerve entrapment) would cause neurological symptoms (paresthesia, weakness) rather than mechanical failure of the construct.
Option E (Nonunion) is a failure of bone healing over a longer period (typically 6-9 months) and is not an early complication presenting within weeks with hardware pull-out.
Question 34
A 35-year-old construction worker sustains a displaced intra-articular distal humerus fracture. Initial plain radiographs are obtained. What is the most crucial next step in the diagnostic workup to guide surgical planning for this type of injury?
Explanation
Correct Answer: C
For intra-articular distal humerus fractures, a CT scan with 3D reconstructions is crucial for operative planning. Plain radiographs often underestimate the degree of articular comminution, displacement, and the exact morphology of the fracture fragments. The CT scan provides detailed information about fragment size, location, and the extent of articular involvement, which is essential for guiding the choice of surgical approach, the sequence of reduction, and the fixation strategy. This detailed understanding helps the surgeon achieve anatomical reduction and stable fixation.
Option A (Immediate surgical exploration and ORIF) without a CT scan is suboptimal, as it risks encountering unexpected fracture patterns that could prolong surgery or compromise the outcome.
Option B (Application of a long-arm cast) is inappropriate for displaced intra-articular fractures, as it will not achieve or maintain anatomical reduction, leading to poor function and post-traumatic arthritis.
Option D (Begin immediate active range of motion exercises) is contraindicated pre-operatively for a displaced fracture, as it could worsen displacement and soft tissue injury.
Option E (Perform an MRI) is excellent for soft tissue and ligamentous injury but provides less detail on complex bony architecture than a CT scan, making it less critical for initial surgical planning of the fracture itself.
Question 35
During a posterior approach to the distal humerus for fracture fixation, the ulnar nerve is identified, mobilized, and protected. After successful fracture reduction and plating, what is the most common and often recommended management strategy for the ulnar nerve to prevent post-operative complications?
Explanation
Correct Answer: C
After identification and protection during distal humerus fracture surgery, the ulnar nerve is commonly transposed anteriorly. This is done to prevent potential entrapment in scar tissue, hardware, or malunion post-operatively, as well as to accommodate for any changes in the cubital tunnel anatomy during fixation. Anterior transposition (either subcutaneously or submuscularly, under the flexor-pronator mass) moves the nerve to a less vulnerable position. This is a proactive measure to prevent delayed ulnar nerve neuropathy.
Option A (Resection) is highly detrimental and would cause permanent neurological deficit; it is never performed for nerve protection.
Option B (Leaving it in situ) carries a significant risk of post-operative entrapment, especially after extensive dissection, hardware placement, or if the cubital tunnel anatomy is altered.
Option D (Repairing it to the triceps muscle) is not a recognized procedure for ulnar nerve management in this context.
Option E (Rarely identified) is incorrect; the ulnar nerve is superficial in the cubital tunnel and is routinely identified and protected during posterior approaches to the distal humerus.
Question 36
A 72-year-old female with a sedentary lifestyle and multiple medical comorbidities (including severe osteoporosis) presents with a highly comminuted, unreconstructible intra-articular distal humerus fracture (AO/OTA 13-C3). She desires pain relief and the ability to perform basic activities of daily living. What is the most appropriate surgical treatment option for this patient?
Explanation
Correct Answer: D
For elderly, low-demand patients with severe osteoporosis and highly comminuted, unreconstructible intra-articular distal humerus fractures, Total Elbow Arthroplasty (TEA) is an increasingly accepted and often preferred option. TEA provides immediate stability, allows for early range of motion, and typically results in good pain relief and functional outcomes for basic activities of daily living. Attempting ORIF in such a scenario often leads to poor fixation due to bone quality, high rates of nonunion, and prolonged rehabilitation with a high risk of stiffness.
Option A (Aggressive ORIF) is often technically challenging and prone to failure in severe osteoporosis and comminution, especially in the elderly.
Option B (Non-operative management) for an unreconstructible, displaced intra-articular fracture would lead to severe malunion, pain, and extremely poor function.
Option C (Elbow arthrodesis) results in a stiff elbow, which is highly disabling for activities of daily living and generally reserved for specific indications like chronic infection or failed TEA in younger, high-demand patients.
Option E (Excision arthroplasty) creates a flail, unstable, and often painful elbow, which is rarely performed today due to poor outcomes.
Question 37
A patient undergoes ORIF of a distal humerus fracture. Six months post-operatively, radiographs show stable hardware but no evidence of bony bridging across the fracture site, and the patient reports persistent pain and limited function. This clinical and radiographic presentation is most consistent with which complication?
Explanation
Correct Answer: C
The scenario describes a fracture that has not healed after a reasonable period (6 months post-ORIF), with stable hardware but no radiographic signs of bony union, accompanied by persistent pain and limited function. This is the classic definition and presentation of a nonunion. A nonunion is a failure of a fracture to heal after a sufficient time period, typically considered 6-9 months, with no further signs of progression towards healing.
Option A (Malunion) refers to a fracture that has healed, but in an anatomically unacceptable position (e.g., angulation, rotation, shortening), leading to deformity and functional impairment.
Option B (Heterotopic ossification) involves the formation of new bone in soft tissues where bone does not normally exist, leading to stiffness and pain, but not necessarily a failure of the fracture itself to unite.
Option D (Chronic infection) would typically present with signs such as persistent drainage, erythema, warmth, and possibly systemic symptoms, which are not mentioned as primary complaints.
Option E (Hardware failure) would be evident on radiographs as broken plates, bent screws, or screws pulled out of the bone, which is distinct from stable hardware without union.
Question 38
What is the primary biomechanical principle that makes orthogonal plating (e.g., a medial plate and a posterior/posterolateral plate) a superior construct for complex bicondylar distal humerus fractures compared to parallel plating?
Explanation
Correct Answer: C
The primary biomechanical advantage of orthogonal plating (typically a medial plate and a posterior or posterolateral plate) for bicondylar distal humerus fractures is that it provides multiplanar stability, resisting axial, varus/valgus, and torsional forces. By placing plates at approximately 90 degrees to each other (relative to the distal humerus, not necessarily the bone's long axis), the construct effectively buttresses both columns and provides robust resistance to the complex forces acting on the elbow. This enhanced stability is crucial for allowing early range of motion and preventing loss of reduction in comminuted fractures.
Option A (Less rigid fixation) is incorrect; orthogonal plating aims for rigid fixation to allow early motion.
Option B (Simplifies plate contouring) is generally incorrect; contouring two plates in an orthogonal fashion can be more challenging than parallel plating, depending on the fracture morphology.
Option D (Maximizes interfragmentary compression) is a goal of fracture fixation, but it's not the primary unique advantage of orthogonal plating over other stable constructs; rather, it's the multiplanar stability that sets it apart.
Option E (Reduces implant weight) is not a primary biomechanical principle or advantage of orthogonal plating; the total weight of two plates is generally similar to two parallel plates.
Question 39
A 28-year-old male sustains an open distal humerus fracture (Gustilo Type II) after a motorcycle accident. He is hemodynamically stable. What is the most critical initial management step once the patient is in the emergency department?
Explanation
Correct Answer: C
For an open fracture, the most critical initial management step, once the patient is hemodynamically stable, is emergent surgical debridement, copious irrigation in the operating room, and the administration of broad-spectrum intravenous antibiotics. This is a surgical emergency aimed at minimizing contamination, removing devitalized tissue, and reducing the high risk of deep infection, which can be devastating for limb salvage and function. The 'golden period' for debridement is typically considered to be within 6 hours of injury.
Option A (Oral antibiotics and discharge) is completely inadequate for an open fracture and would lead to severe infection.
Option B (Splint and physical therapy) is insufficient; while splinting is part of initial stabilization, it does not address the open wound or infection risk.
Option D (Primary wound closure) is generally contraindicated for open fractures, especially Gustilo Type II or higher, as it can trap bacteria and increase infection risk. Wounds are often left open for delayed primary closure or secondary healing after repeat debridements.
Option E (MRI) is not an emergent diagnostic modality for an acute open fracture; the priority is infection control and surgical debridement.
Question 40
In the early post-operative period (first 3-7 days) following stable open reduction and internal fixation (ORIF) of a distal humerus fracture, what is the primary goal of rehabilitation?
Explanation
Correct Answer: C
With stable open reduction and internal fixation (ORIF) of a distal humerus fracture, the primary goal in the early post-operative period (typically within the first week) is to initiate early active range of motion (AROM) exercises. This is crucial for preventing debilitating elbow stiffness, which is a very common and challenging complication after distal humerus fractures. The stability achieved by rigid internal fixation allows for controlled motion without jeopardizing the fracture healing.
Option A (Achieve full elbow extension) is an eventual goal, but attempting it immediately is unrealistic and potentially harmful.
Option B (Resisted strengthening exercises) are introduced much later in the rehabilitation process (typically 6-12 weeks), once significant bone healing has occurred.
Option D (Rigid immobilization for 6 weeks) would almost certainly lead to severe elbow stiffness and is generally avoided after stable ORIF.
Option E (CPM for 12 hours daily) is a modality that can be used, but the primary goal is active patient participation in motion, and CPM is not universally indicated or the sole focus of early rehab.
Question 41
A 50-year-old patient presents with a distal humerus fracture. During the initial physical examination, you note an inability to extend the wrist and fingers, along with sensory loss over the dorsal aspect of the hand and forearm. Which nerve injury is most likely?
Explanation
Correct Answer: C
The clinical presentation of an inability to extend the wrist and fingers (often described as 'wrist drop' and 'finger drop'), combined with sensory loss in the dorsal forearm and hand, is pathognomonic for a radial nerve injury. The radial nerve innervates the extensor muscles of the wrist and fingers and provides sensation to the dorsal aspect of the forearm and hand (excluding the small finger and ulnar half of the ring finger, which are ulnar nerve territory).
Option A (Ulnar nerve injury) typically affects intrinsic hand muscles (e.g., interossei, hypothenar muscles), causing clawing of the ring and small fingers, and sensory loss on the ulnar side of the hand and small finger.
Option B (Median nerve injury) affects forearm pronation, wrist flexion, thumb opposition, and sensation in the radial 3.5 digits (thumb, index, middle, and radial half of ring finger).
Option D (Musculocutaneous nerve injury) primarily affects elbow flexion (biceps and brachialis) and sensation over the lateral forearm.
Option E (Anterior interosseous nerve injury) is a motor branch of the median nerve affecting deep forearm flexors (flexor pollicis longus, flexor digitorum profundus to index/middle fingers, pronator quadratus) and does not cause sensory loss or wrist/finger drop.
Question 42
A 24-year-old rugby player presents 48 hours after sustaining an injury to his left ring finger while tackling an opponent. He reports his finger was forcibly extended while he was gripping the opponent's jersey. On examination, he has swelling and tenderness over the palmar aspect of the distal phalanx. He is unable to actively flex the DIP joint of the ring finger. The remaining fingers show normal cascade. Passive DIP flexion is full. X-rays show no bony avulsion. Which of the following Leddy and Packer types is most likely, and what is the primary concern driving urgent treatment?
Explanation
Correct Answer: C
This scenario describes a classic Type I Jersey finger. A Type I injury involves rupture of the FDP tendon without a bony avulsion, and the tendon typically retracts into the palm, losing its vincula blood supply. The primary concern driving the urgency for repair (ideally within 7-10 days, but sooner if possible) is the preservation of the tendon's intrinsic vascularity to prevent necrosis and facilitate healing. Type II also lacks a bony avulsion but the tendon is retained at the A3 pulley level, often with intact vincula, making it less urgent than Type I. Type III involves a bony avulsion fragment, which prevents further retraction and maintains tendon blood supply, making it less urgent. Type IV involves an avulsed bone fragment with the tendon avulsed from the fragment, and Type V involves an intra-articular fracture with tendon avulsion; these are also distinct from the given scenario.
Question 43
Regarding the surgical repair of a chronic FDP rupture (presenting 6 months post-injury) in a 35-year-old manual laborer, which of the following is the most appropriate initial management strategy if direct primary repair is not feasible?
Explanation
Correct Answer: C
For chronic FDP ruptures where direct primary repair is not feasible due to significant tendon retraction and shortening, staged tendon reconstruction using a silicone rod (Hunter rod) is often the preferred strategy. The silicone rod creates a pseudosheath, which then facilitates the passage of an autogenous tendon graft (commonly palmaris longus or plantaris) in a second stage. FDP advancement is only feasible for gaps typically less than 1 cm. Delayed primary repair with an interpositional graft is a possibility, but less predictable than staged reconstruction for significant gaps. Amputation is overly aggressive, and observation alone will not restore function in a chronic rupture.
Question 44
A 19-year-old basketball player presents with a suspected Jersey finger of his small finger. On examination, he has full active flexion of his PIP joint but lacks active flexion of his DIP joint. A modified tabletop test reveals a normal cascade for all fingers except the small finger, which remains extended at the DIP joint. What is the most reliable maneuver to confirm an FDP rupture in this digit?
Explanation
Correct Answer: C
The most reliable maneuver to confirm an FDP rupture is to isolate the action of the FDP tendon. This is done by stabilizing the PIP joint in full extension and asking the patient to actively flex the DIP joint. If the FDP is ruptured, active DIP flexion will be absent. Assessing passive range of motion will typically be full, as the FDP rupture is an active deficit. Palpating a tender gap can be indicative but is not always reliable, especially with swelling. Grip strength is a global measure and not specific enough. Finkelstein's test is for De Quervain's and irrelevant here.
Question 45
Which of the following statements most accurately describes the 'quadriga effect' as a potential complication following FDP repair, particularly when using advancement techniques?
Explanation
Correct Answer: A
The quadriga effect is a well-known complication of FDP repair, particularly when the tendon is shortened (e.g., through advancement or overtightening during repair). Because the FDP tendons of the medial four fingers share a common muscle belly (or are closely intertwined proximally), overtensioning of one FDP tendon will restrict full flexion of the adjacent, healthy FDP tendons. This results in the inability of the adjacent digits to fully flex. The other options describe different complications or aspects of tendon repair.
Question 46
A 40-year-old construction worker sustained a Jersey finger injury to his index finger 3 weeks ago. X-rays reveal a small bony avulsion fragment from the palmar aspect of the distal phalanx, with the fragment retracted to the level of the A4 pulley. He has minimal pain but lacks active DIP flexion. Which Leddy and Packer type is this, and what is the typical management recommendation?
Explanation
Correct Answer: C
This is a classic Type III Leddy and Packer injury. It involves a bony avulsion fragment from the distal phalanx that typically retracts to the A4 pulley. The key feature is that the bone fragment prevents further tendon retraction and, importantly, preserves the tendon's blood supply via the vincula. This makes the repair less urgent than a Type I or even Type II injury, allowing for repair up to 3-4 weeks post-injury without significantly compromising outcomes. Immediate repair is for Type I. Type II lacks a bony fragment. Type IV involves tendon avulsed from the fragment. Type V involves an intra-articular fracture.
Question 47
Which of the following anatomical structures is MOST critical for providing blood supply to the flexor digitorum profundus (FDP) tendon in the distal finger, particularly relevant in Type I Jersey finger injuries?
Explanation
Correct Answer: C
The vincula tendinum are mesotendinous structures that connect the flexor tendons to the phalanges and provide the primary blood supply to the tendons within the flexor sheath. In a Type I Jersey finger, the FDP tendon avulses distal to the vincula longa and retracts into the palm, often stripping it of its vincula and thus its blood supply, leading to a high risk of tendon necrosis. The A2 pulley is a critical mechanical structure but not primarily a source of blood supply to the tendon itself. The flexor sheath provides an environment, not the primary blood supply. Annular ligaments are the pulleys. Lumbrical muscles have their own blood supply but do not supply the FDP tendon directly.
Question 48
A 28-year-old rock climber presents with chronic stiffness and an inability to fully extend her ring finger DIP joint 8 months after a surgically repaired Jersey finger. Radiographs show no fracture or hardware issues. This is most likely due to:
Explanation
Correct Answer: C
Chronic stiffness and limited range of motion, particularly an inability to fully extend, following flexor tendon repair are most commonly due to adhesions forming within the flexor sheath. This restricts the smooth gliding of the repaired tendon. Re-rupture would present with loss of active flexion, not stiffness in extension. Quadriga effect limits flexion of adjacent fingers. Lumbrical plus phenomenon involves paradoxical DIP extension with attempted strong grip. Insufficient extensor strength would primarily affect active extension, not passive range of motion if adhesions are the cause.
Question 49
When performing a primary repair of a retracted FDP tendon, which of the following is considered the gold standard suture technique for strength and preventing pull-out?
Explanation
Correct Answer: D
The gold standard for flexor tendon repair involves a strong core suture technique that provides robust mechanical strength against gapping and pull-out. The Modified Kessler (or similar variations like Lim-Tsai, Modified Becker, Pennington) is a common and effective core suture. An epitendinous suture is typically used in addition to a core suture to create a smooth gliding surface and add some strength, but it is not sufficient on its own for primary repair strength. Simple interrupted, horizontal mattress, and running locking sutures are not typically used as primary core sutures in flexor tendon repair due to lower strength and potential for gapping or strangulation.
Question 50
What is the typical presentation of a 'lumbrical plus' phenomenon, which can be a complication of FDP repair or shortening?
Explanation
Correct Answer: B
The 'lumbrical plus' phenomenon occurs when the FDP tendon is advanced and overtensioned, or the repair site is too stiff, causing the lumbrical muscle to be pulled proximally. When the patient attempts to flex the finger (activating the FDP), the lumbrical is put under tension before the FDP can flex the DIP joint. Since the lumbrical inserts into the extensor mechanism, its contraction paradoxically extends the DIP joint instead of allowing FDP flexion. This results in the DIP joint extending or remaining extended when the patient attempts to make a full fist. Option E describes the quadriga effect.
Question 51
A 16-year-old athlete presents with an acute Jersey finger (Type I Leddy and Packer) of his long finger. He is scheduled for surgical repair. What is the most common approach to access the FDP tendon and achieve primary repair?
Explanation
Correct Answer: E
The Brunner's zigzag incision is the most common and preferred approach for surgical access to the flexor tendons in the finger. This incision provides excellent exposure, allows for good visualization of the flexor sheath and tendon, and minimizes the risk of creating a longitudinal scar that could lead to flexion contracture. A midaxial incision is typically used for bony procedures or accessing the neurovascular bundles, not direct flexor tendon repair. Transverse incisions would limit exposure. A straight volar incision is contraindicated due to the high risk of contracture. A dorsal approach is for extensor tendon or dorsal bony injuries.
Question 52
A 35-year-old male sustains a high-energy blunt trauma to his shoulder resulting in an isolated scapula fracture. Which of the following parameters represents a generally accepted absolute or relative indication for operative reduction and internal fixation of a scapular body or neck fracture?
Explanation
Question 53
A 28-year-old male sustains a midshaft clavicle fracture. Which of the following fracture characteristics or patient demographics has the highest predictive value for the development of a nonunion if managed nonoperatively?
Explanation
Question 54
A 65-year-old female presents with a displaced 4-part proximal humerus fracture.
Which of the following arteries is currently recognized in the literature as providing the predominant blood supply to the humeral head, and is most critical to evaluate for disruption regarding avascular necrosis risk?
Explanation
Question 55
A 30-year-old male sustains a Holstein-Lewis fracture of the distal third of his humerus. He demonstrates an inability to extend his wrist and fingers upon presentation. At what specific anatomic location is the nerve most commonly entrapped or injured in this fracture pattern?
Explanation
Question 56
A 40-year-old gymnast falls from a height and sustains an anteromedial facet fracture of the coronoid process. If left untreated, this specific fracture pattern most predictably leads to which of the following instability patterns?
Explanation
Question 57
A 50-year-old male sustains a terrible triad injury of the elbow consisting of an elbow dislocation, radial head fracture, and coronoid fracture. According to standard treatment algorithms, what is the most appropriate sequence of surgical repair?
Explanation
Question 58
During surgery for a highly comminuted radial head fracture, the surgeon decides to place a radial head arthroplasty. If the implanted prosthesis is excessively long (overstuffed), what is the most likely clinical and biomechanical consequence?
Explanation
Question 59
A 60-year-old female undergoes tension band wiring for a displaced transverse olecranon fracture. Six months postoperatively, her fracture is healed, but she complains of focal pain at the surgical site. What is the most common complication following tension band wiring of the olecranon?
Explanation
Question 60
A 45-year-old male sustains a Bado Type I Monteggia fracture-dislocation. What is the most appropriate definitive management strategy for this adult patient?
Explanation
Question 61
A surgeon is repairing a Galeazzi fracture in a 32-year-old male. Following anatomic open reduction and rigid internal fixation of the radial shaft, the distal radioulnar joint (DRUJ) remains grossly unstable. What is the most appropriate next step in management?
Explanation
Question 62
A 55-year-old female presents with sudden inability to flex the interphalangeal joint of her thumb. Seven months prior, she underwent volar locking plate fixation for a distal radius fracture. Radiographs reveal the volar plate is positioned distal to the watershed line. Which tendon is most likely injured?
Explanation
Question 63
A 22-year-old male sustains a scaphoid fracture after a fall on an outstretched hand. Which of the following anatomic locations of the scaphoid has the highest inherent risk of progressing to a nonunion and avascular necrosis?
Explanation
Question 64
According to the Mayfield classification of progressive perilunate instability, a Stage III injury is defined by the disruption of which of the following specific ligamentous structures?
Explanation
Question 65
A 32-year-old male is involved in a high-speed motorcycle collision. He sustains an isolated, displaced scapular body fracture. Which of the following parameters is an accepted indication for operative fixation of a scapular body fracture?
Explanation
Question 66
A 65-year-old female sustains a comminuted intra-articular distal humerus fracture. The surgeon elects to perform an open reduction internal fixation (ORIF) via a posterior approach with an olecranon osteotomy. Which of the following is the most common complication specifically associated with this surgical approach?
Explanation
Question 67
A 25-year-old male sustains a minimally displaced fracture of the scaphoid waist. He opts for non-operative management with cast immobilization. The scaphoid is at high risk for nonunion and avascular necrosis due to its tenuous blood supply. The primary blood supply to the proximal pole of the scaphoid is derived from which of the following?
Explanation
Question 68
During surgical reconstruction of a 'terrible triad' injury of the elbow (elbow dislocation, radial head fracture, and coronoid fracture), which of the following represents the most widely accepted sequence of structural repair to restore stability?
Explanation
Question 69
A 55-year-old female presents with a displaced proximal humerus fracture after a fall. According to Hertel's radiographic criteria, which of the following isolated features is the strongest predictor of humeral head ischemia?
Explanation
Question 70
A 35-year-old male is involved in a high-speed motorcycle collision and sustains an extra-articular scapular neck fracture. The decision is made to evaluate the glenopolar angle (GPA) on AP radiographs of the shoulder. A GPA less than which of the following values is generally considered a relative indication for surgical fixation due to severe rotational malalignment?
Explanation
Question 71
A 60-year-old female presents with a sudden inability to actively extend her thumb interphalangeal joint 6 weeks after a non-operatively treated, undisplaced distal radius fracture. What is the primary pathomechanism of this specific complication?
Explanation
Question 72
A 28-year-old carpenter falls from a ladder, sustaining a comminuted trans-olecranon fracture-dislocation. The surgeon decides against using tension band wiring for this injury. What is the primary mechanical reason tension band wiring is contraindicated in this specific fracture pattern?
Explanation
Question 73
A 30-year-old male sustains a Bennett fracture during a fistfight. Radiographs reveal a fracture at the base of the first metacarpal with significant proximal and dorsal displacement of the metacarpal shaft. Which muscle is primarily responsible for this displacing force?
Explanation
Question 74
A 22-year-old male cyclist sustains a midshaft clavicle fracture. Which of the following clinical or radiographic findings is an absolute indication for open reduction and internal fixation?
Explanation
None
