Comprehensive ABOS Part I Orthopaedic Exam Review: Trauma, Fractures, Osteochondromas | Part 22212

Key Takeaway
This module offers a comprehensive review for the ABOS Part I and AAOS OITE examinations. It features 31 advanced multiple-choice questions covering critical topics in orthopedic surgery, including acute trauma (fractures, dislocations, compartment syndrome) and bone tumors (osteochondromas, HME, chondrosarcoma). Explanations detail immediate management, surgical principles, imaging, and potential complications, providing essential knowledge for board exam preparation.
Comprehensive ABOS Part I Orthopaedic Exam Review: Trauma, Fractures, Osteochondromas | Part 22212
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 45-year-old male presents to the emergency department after a high-speed motor vehicle collision. He is hypotensive (BP 80/50 mmHg) and tachycardic (HR 125 bpm). Physical examination reveals obvious instability of the pelvic ring with ecchymosis over the perineum and pubic symphysis. Initial resuscitation with 2 liters of crystalloid has failed to improve his hemodynamic status. Which of the following is the most appropriate next step in his immediate management?
Explanation
Correct Answer: B
In a hemodynamically unstable patient with a suspected pelvic ring injury, the priority is hemorrhage control. A pelvic binder (or sheet) provides immediate temporary stabilization and reduction of the pelvic volume, which can tamponade bleeding. If the patient remains unstable after initial resuscitation and binder application, the next step is typically emergent surgical stabilization (e.g., external fixation) in the operating room or angiography for embolization, often dictated by local protocol and surgeon preference. While CT scan, Foley catheter insertion, and angiography are important diagnostic and therapeutic steps, immediate mechanical reduction via a binder and early surgical intervention for ongoing instability take precedence for life-threatening hemorrhage. Tranexamic acid and massive transfusion protocol are adjuncts but don't address the primary mechanical cause of bleeding.
Question 2
A 28-year-old male sustains a posterior hip dislocation after a dashboard injury in an MVC. On examination, his hip is internally rotated, adducted, and flexed. He has diminished sensation in the plantar aspect of his foot and weakness in ankle dorsiflexion and eversion. What is the most appropriate initial management step, considering the neurovascular status?
Explanation
Correct Answer: B
Posterior hip dislocations are orthopedic emergencies due to the high risk of avascular necrosis (AVN) of the femoral head and associated sciatic nerve injury. The most critical factor is the time to reduction. A neurological deficit (like the described sciatic nerve palsy) does NOT contraindicate immediate closed reduction. In fact, prompt reduction may allow for neurological recovery. A CT scan is important AFTER successful closed reduction to assess for incarcerated fragments or occult fractures (e.g., femoral head impaction, posterior wall acetabular fracture), but it should not delay reduction. Open reduction is reserved for failed closed reduction or irreducible dislocations. MRI is not an acute management tool.
Question 3
A 35-year-old construction worker sustains an open tibial shaft fracture (Gustilo-Anderson Type IIIA) after being struck by heavy machinery. He arrives in the ED 1 hour after injury. What is the immediate priority in his management after ATLS resuscitation and basic wound coverage?
Explanation
Correct Answer: B
For open fractures, particularly Gustilo-Anderson Type IIIA, emergent irrigation and debridement in the operating room is the most critical step to prevent infection and facilitate healing. While antibiotics are crucial, they are adjuncts to surgical debridement. The 'golden period' for debridement is traditionally considered within 6-8 hours, but earlier is better, especially for higher grades. CTA might be indicated if there's concern for vascular injury, but controlling contamination is paramount. Definitive fixation is performed after initial debridement, often at a later stage once the soft tissue envelope has been optimized. Compartment pressures would be measured if compartment syndrome is suspected, but initial management focuses on the open wound.
Question 4
A 22-year-old football player presents with severe pain in his right lower leg after a direct blow. He complains of paresthesia in his foot and pain on passive dorsiflexion of his toes. The calf is tense to palpation. What is the most reliable diagnostic finding for acute compartment syndrome?
Explanation
Correct Answer: E
The most reliable diagnostic criterion for acute compartment syndrome is a 'delta pressure' (diastolic blood pressure minus intracompartmental pressure) less than 30 mmHg. While an absolute pressure of 30 mmHg or greater is often used as a threshold, it must be considered in relation to the patient's blood pressure, as a lower absolute pressure can still be significant in hypotensive patients. Pain out of proportion to injury, paresthesia, and a tense compartment are classic clinical signs, but they are subjective and can be unreliable in altered mental status or pediatric patients. A palpable distal pulse does not rule out compartment syndrome, as arterial inflow is typically preserved until very late stages. Elevated CK levels indicate muscle damage but are not diagnostic of acute compartment syndrome.
Question 5
A 30-year-old male sustains a high-energy knee injury with gross instability in all planes. Radiographs confirm a knee dislocation without associated fractures. Pulses are diminished in the dorsalis pedis and posterior tibial arteries. What is the most appropriate next step in management?
Explanation
Correct Answer: A
Knee dislocation, especially with vascular compromise, is an orthopedic emergency. The immediate priority is reduction of the knee to restore blood flow and reduce tension on the popliteal artery. Closed reduction should be attempted immediately. After reduction, pulses must be meticulously reassessed. If pulses remain diminished or absent, or if there is any concern for popliteal artery injury (even with palpable pulses if the mechanism suggests high energy), an emergent CT angiogram (or arteriogram) is warranted. Delaying reduction for imaging significantly increases the risk of limb ischemia and potential amputation. Ligament repair and external fixation are important later steps, but re-establishing circulation is paramount.
Question 6
A 40-year-old male falls from a height, landing on his heels. He presents with bilateral heel pain. Radiographs show a displaced calcaneus fracture. Which associated injury should be specifically investigated?
Explanation
Correct Answer: B
Calcaneus fractures, especially those resulting from a fall from a height, are associated with a significant incidence of lumbar spine compression fractures (10-15%). The axial loading mechanism transmits force up the kinetic chain. Therefore, it is critical to obtain imaging of the lumbar spine (lateral X-ray or CT) in all patients with calcaneus fractures from a fall from height. While other injuries can occur, a lumbar spine fracture is the most common and critical associated injury to specifically rule out due to potential neurological sequelae.
Question 7
A 55-year-old female presents with midfoot pain and inability to bear weight after stepping off a curb awkwardly. Radiographs show subtle widening between the first and second cuneiforms. What is the most sensitive imaging modality to confirm a Lisfranc injury and guide management?
Explanation
Correct Answer: D
Lisfranc injuries (tarsometatarsal joint complex disruption) can be subtle on standard plain radiographs, especially non-displaced or purely ligamentous injuries. While weight-bearing and stress radiographs are crucial for initial assessment, a CT scan is considered the most sensitive imaging modality to definitively diagnose and characterize Lisfranc injuries. It provides detailed bony anatomy, identifies small avulsion fractures, and measures subtle diastasis not visible on plain films. This information is critical for surgical planning. MRI is excellent for soft tissue injuries (ligaments) but often follows a CT scan for bony detail. A bone scan is not an acute management tool.
Question 8
A 60-year-old obese male sustains a high-energy knee injury, resulting in a Schatzker Type VI tibial plateau fracture. He has multiple open wounds and significant soft tissue swelling. What is the most appropriate initial surgical approach for this injury?
Explanation
Correct Answer: B
Schatzker Type VI tibial plateau fractures are complex, high-energy injuries often associated with severe soft tissue damage, swelling, and open wounds. Immediate definitive ORIF carries a high risk of wound complications, infection, and flap necrosis due to the compromised soft tissue envelope. The preferred initial management is often damage control orthopedics: emergent external fixation with provisional joint spanning (spanning ex-fix) to stabilize the fracture, protect the soft tissues, and allow swelling to subside. Definitive ORIF is then performed in a delayed fashion (typically 7-14 days) once the 'wrinkle sign' appears and the soft tissues are amenable to surgery. Closed reduction and casting are inadequate for displaced, unstable, or articular fractures. Arthroplasty is not an acute treatment for fractures. Arthroscopic assistance is primarily for less severe fractures.
Question 9
A 48-year-old female presents after a motor vehicle accident with a comminuted fracture of the distal tibia extending into the ankle joint (pilon fracture). There is significant soft tissue swelling and blistering. What is the primary goal of immediate non-operative management?
Explanation
Correct Answer: C
Pilon fractures are challenging due to their articular involvement and often severe soft tissue injury. Significant soft tissue swelling and blistering indicate a compromised soft tissue envelope that is not ready for definitive surgical intervention. The primary goal of immediate non-operative management (often with a spanning external fixator for provisional stability) is to allow the soft tissues to recover, reduce swelling, and improve the skin condition. This 'waiting game' is crucial to minimize the high risk of wound complications (dehiscence, infection) associated with early surgery on inflamed tissues. Anatomical reduction is the ultimate goal, but it must be achieved when the soft tissues allow. Early weight-bearing is contraindicated. DVT prophylaxis is important but not the primary goal of local fracture management in this context.
Question 10
A 32-year-old male involved in a motorcycle accident sustains multiple long bone fractures (bilateral femoral and tibial shaft fractures). Three days post-injury, he develops acute respiratory distress, petechial rash on his chest and axilla, and altered mental status. What is the most likely diagnosis?
Explanation
Correct Answer: C
The classic triad of respiratory distress, neurological dysfunction (altered mental status), and petechial rash appearing 12-72 hours after long bone fractures is highly suggestive of Fat Embolism Syndrome (FES). While pulmonary embolism and ARDS are serious complications, the presence of the petechial rash and the specific timing post-multiple long bone fractures strongly point to FES. Pneumonia and cerebral infarct are less likely given the specific constellation of symptoms and the acute post-traumatic timeline. FES is a life-threatening complication, with management being primarily supportive.
Question 11
A 10-year-old male presents with a painless, palpable mass on the medial aspect of his distal femur. Radiographs show a bony exostosis arising from the metaphyseal cortex, with the cortex and medullary cavity continuous with the parent bone. The lesion points away from the joint. What is the most likely diagnosis?
Explanation
Correct Answer: C
The description of a bony exostosis with continuity of the cortex and medullary cavity with the parent bone, arising from the metaphysis and pointing away from the joint, is pathognomonic for an osteochondroma. Osteochondromas are the most common benign bone tumors. Enchondromas are intramedullary. Osteoid osteomas are small, painful lesions with a nidus. Parosteal osteosarcoma is a malignant surface lesion, usually in older patients, and lacks the medullary continuity. Chondroblastomas are epiphyseal.
Question 12
A 35-year-old man with a known solitary osteochondroma of the proximal tibia reports new onset of increasing pain, warmth, and a rapidly enlarging mass. Radiographs show a poorly defined lesion, and MRI reveals a cartilage cap thickness of 3.5 cm. What is the most appropriate next step in management?
Explanation
Correct Answer: E
New onset pain, rapid growth in an adult, and a cartilage cap thickness exceeding 2 cm (in adults) are highly suspicious for malignant transformation to a secondary chondrosarcoma. A percutaneous biopsy is the most appropriate initial diagnostic step to confirm the diagnosis and grade the tumor before definitive surgical planning. Wide margins are indicated for chondrosarcoma, but biopsy confirms. Observation, NSAIDs, and radiation are inappropriate given the suspicion of malignancy.
Question 13
Which of the following genetic mutations is most commonly associated with Hereditary Multiple Exostoses (HME)?
Explanation
Correct Answer: B
Hereditary Multiple Exostoses (HME), also known as Multiple Osteochondromas, is an autosomal dominant disorder caused by germline mutations in either the EXT1 or EXT2 genes. These genes encode glycosyltransferases involved in heparan sulfate synthesis, a critical component of the extracellular matrix. TP53 is associated with sarcomas (e.g., Li-Fraumeni). COL1A1 is linked to osteogenesis imperfecta. IDH1/IDH2 mutations are seen in some chondrosarcomas (including dedifferentiated). SMAD3 is not directly linked to HME.
Question 14
A 7-year-old child with Hereditary Multiple Exostoses (HME) presents with progressive genu valgum and a noticeable limb length discrepancy. What is the most common mechanism leading to angular deformities in HME?
Explanation
Correct Answer: E
Angular deformities and limb length discrepancies in HME are primarily due to asymmetric growth plate disturbance. Osteochondromas arising from the physis can tether or distort a portion of the growth plate, leading to asymmetric growth arrest or retardation, thereby causing progressive angulation (e.g., genu valgum from lateral tibial physis involvement) and limb length discrepancies. Premature physeal closure on the convex side is incorrect; it's the concave side that's often affected by growth disturbance. Other options are less common or incorrect mechanisms.
Question 15
Which imaging modality is most effective for evaluating the cartilage cap thickness of an osteochondroma, especially when assessing for malignant transformation?
Explanation
Correct Answer: C
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the cartilage cap thickness of an osteochondroma. The cartilage cap appears as a high signal intensity on T2-weighted images. A cap thickness greater than 2 cm in an adult is a strong indicator of malignant transformation to a secondary chondrosarcoma. Plain radiographs and CT are excellent for bony morphology but poor for cartilage visualization. Bone scintigraphy can show increased uptake but is not specific for cap thickness. Ultrasound can sometimes visualize the cap but is less reliable and quantitative than MRI.
Question 16
A 16-year-old active athlete presents with a painful, enlarging mass over a known osteochondroma on the posterior aspect of his distal femur. Examination reveals a fluctuant, tender swelling. What is the most likely complication?
Explanation
Correct Answer: D
The development of a painful, enlarging, fluctuant mass over an osteochondroma, particularly in an area subject to friction or repetitive motion, is highly suggestive of symptomatic bursa formation. The bursa develops in response to irritation from the osteochondroma. While other complications are possible, the description best fits bursitis. Malignant transformation typically presents with a hard, rapidly enlarging mass and increased pain, but less often fluctuant. Fracture causes acute, sharp pain. Pseudoaneurysm would have pulsatile swelling. Nerve compression causes neurological symptoms.
Question 17
Which of the following statements regarding the malignant transformation of a solitary osteochondroma is FALSE?
Explanation
Correct Answer: E
Malignant transformation of osteochondromas typically occurs in adults, usually after skeletal maturity, not in children under 10. The average age for secondary chondrosarcoma is 30-40 years. The other statements are true: HME carries a higher risk (5-25%) than solitary lesions (<1%), it transforms into peripheral chondrosarcoma, and the described signs are indeed warning signs.
Question 18
A 25-year-old male presents with acute, severe pain after a fall directly onto his knee. He has a known osteochondroma arising from the distal femur. Radiographs show a distinct lucent line across the base of the stalk of the exostosis. What is the most likely diagnosis?
Explanation
Correct Answer: C
Acute, severe pain following trauma to a known osteochondroma, with radiographic evidence of a lucent line across its base, is characteristic of a fracture through the stalk of the osteochondroma. This is a recognized complication and can be quite painful. Malignant degeneration would not typically present with acute trauma and a clear fracture line. Other options are less likely given the acute traumatic event and specific radiographic finding.
Question 19
Which location of an osteochondroma carries a higher risk for neurological complications due to compression?
Explanation
Correct Answer: D
Osteochondromas occurring in the vertebral body or near neural foramina, although rare, have a significantly higher risk of causing neurological complications due to compression of the spinal cord or nerve roots. Other common locations like the distal femur, proximal tibia, proximal humerus, or ribs are less likely to cause neurological deficits unless very large or atypically located. The question asks for 'neurological complications', making the vertebral body the prime suspect.
Question 20
A 6-year-old boy presents with a growing mass near his ankle. Clinical examination reveals an osteochondroma arising from the distal tibia. His parents are concerned about its impact on future growth. What is the most common growth disturbance associated with lower extremity osteochondromas in children?
Explanation
Correct Answer: C
The most common growth disturbance associated with lower extremity osteochondromas, particularly in the distal tibia or fibula, is progressive angular deformity, often genu valgum or varus, and limb length discrepancy. This occurs due to asymmetric growth disturbances at the physis. While limb length discrepancy can occur, angular deformity is explicitly stated as common. Overgrowth is rare. Pes cavus and AVN are not typical complications.
Question 21
A 29-year-old female horse rider presents to the emergency department after falling off her horse, sustaining an isolated closed injury to her left foot. Initial radiographs are obtained:
Based on these initial findings, what is the most appropriate immediate next step in the management of this patient?

Explanation
Correct Answer: C
Explanation:
The initial radiographs (Figure 8.16) clearly show a displaced, comminuted fracture of the body of the navicular bone with overlap of mid-tarsal bones. While the diagnosis of a navicular fracture is evident, the complex anatomy of the midfoot and the comminuted nature of this intra-articular fracture necessitate further detailed imaging for definitive surgical planning. A CT scan is the gold standard for evaluating complex foot fractures, especially those involving the tarsal bones, as it provides superior detail regarding fracture lines, comminution, articular involvement, and displacement in multiple planes (coronal, sagittal, axial). This information is critical for determining the optimal surgical approach, fixation strategy, and prognosis.
- A. Proceed directly to open reduction and internal fixation (ORIF) given the clear displacement: While operative intervention is likely, proceeding directly to surgery without a CT scan is premature and could lead to inadequate planning and suboptimal outcomes. The CT scan is essential for understanding the 3D anatomy of the fracture.
- B. Apply a short leg cast and discharge with instructions for non-weight bearing: This is an unstable, displaced intra-articular fracture. Non-operative management is generally not favored for such injuries due to the high risk of malunion, post-traumatic arthritis, and loss of foot function. Furthermore, a CT scan is still needed to confirm the extent of injury before deciding on definitive management.
- D. Perform an immediate MRI to evaluate for ligamentous injuries and soft tissue compromise: While MRI is excellent for soft tissue and ligamentous injuries, it is not the primary imaging modality for detailed bony architecture in acute, complex fractures like this. A CT scan is more crucial for surgical planning of the bone injury itself. MRI might be considered later if there are specific concerns about ligamentous instability not addressed by CT.
- E. Initiate broad-spectrum intravenous antibiotics due to the high-energy mechanism: The case states this is an isolated closed injury. There is no indication of an open fracture or infection, so prophylactic antibiotics are not warranted at this stage.
Question 22
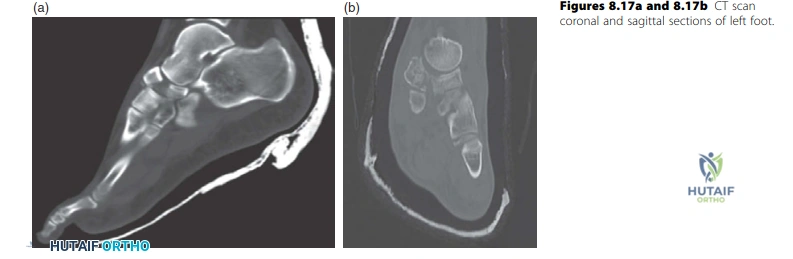
Following the initial assessment, a CT scan of the foot is obtained, confirming a displaced, comminuted, unstable intra-articular fracture of the navicular body:
Based on the case discussion, which of the following is the MOST critical factor influencing the decision to favor operative intervention over non-operative management for this specific injury?
Explanation
Correct Answer: C
Explanation:
The case explicitly states, 'It is an unstable displaced intra-articular fracture and I would favour operative intervention rather than non-operative. The principles of management are to restore the articular surface, stabilize and hold the fracture to allow early mobilization.' The most critical factor driving the decision for operative management in navicular body fractures is the involvement of the articular surface and the degree of displacement and comminution. Intra-articular fractures, especially when displaced, disrupt the joint congruity, leading to high rates of post-traumatic osteoarthritis, pain, and functional impairment if not anatomically reduced and stabilized.
- A. The patient's young age and active lifestyle as a horse rider: While these are factors that support aggressive treatment to restore function, they are not the primary pathological reason for choosing surgery. The nature of the fracture itself is the main driver.
- B. The presence of significant soft tissue swelling around the midfoot: Soft tissue swelling is common in high-energy foot injuries and can delay surgery, but it is not an indication for surgery itself. It's a factor to manage pre-operatively.
- D. The isolated nature of the injury without other associated fractures: An isolated injury might simplify surgical planning, but it doesn't inherently mandate surgery. The characteristics of the navicular fracture are what dictate the need for operative intervention.
- E. The potential for compartment syndrome if not surgically stabilized: While compartment syndrome is a serious complication to monitor for, surgical stabilization of the fracture itself is not the primary treatment for compartment syndrome. Fasciotomy is. Furthermore, the potential for compartment syndrome is a risk of the injury, not the primary reason for choosing operative fixation of the navicular fracture.
Question 23
The surgeon plans operative intervention for the displaced, comminuted navicular body fracture. A medial approach is chosen. Which of the following describes the correct anatomical interval for this approach and a critical neurovascular structure at risk?
Explanation
Correct Answer: B
Explanation:
The case explicitly states, 'I would use a medial approach, between the tibialis anterior and tibialis posterior tendons, preserving the remaining blood supply as much as possible...' The medial approach to the navicular is typically performed through the interval between the tibialis anterior tendon (anteriorly) and the tibialis posterior tendon (posteriorly). The dorsalis pedis artery is a continuation of the anterior tibial artery and runs on the dorsum of the foot. While the primary approach is medial, the blood supply to the navicular relies on the radial arcade of vessels arising from the dorsalis pedis and medial plantar arteries. Injury to these vessels, particularly the dorsalis pedis artery and its branches, can compromise the already tenuous blood supply to the navicular, leading to complications like avascular necrosis (AVN) and non-union, as highlighted in the case.
- A. Between the extensor hallucis longus and tibialis anterior tendons; risk to the deep peroneal nerve: This interval is more dorsal and lateral, typically used for approaches to the talus or first metatarsal, not the navicular. The deep peroneal nerve is at risk in this region.
- C. Between the flexor digitorum longus and flexor hallucis longus tendons; risk to the posterior tibial nerve: This interval is on the plantar aspect of the foot, not a standard approach for a navicular body fracture. The posterior tibial nerve is in the tarsal tunnel.
- D. Between the tibialis anterior and tibialis posterior tendons; risk to the medial plantar nerve: While the medial plantar nerve is present on the medial side of the foot, the primary neurovascular structure at risk for the navicular's blood supply, as discussed in the context of AVN, is the arterial supply (dorsalis pedis and medial plantar arteries). The dorsalis pedis artery is a more direct concern for the navicular's dorsal blood supply.
- E. Between the peroneus longus and brevis tendons; risk to the superficial peroneal nerve: This interval is on the lateral side of the foot, not a medial approach to the navicular. The superficial peroneal nerve is at risk laterally.
Question 24
The examiner asks about the high incidence of non-union and avascular necrosis (AVN) in navicular fractures. The candidate correctly explains that the navicular bone's blood supply is vulnerable. Which specific arterial arcade is primarily responsible for the navicular's blood supply and is most susceptible to injury in these fractures?
Explanation
Correct Answer: C
Explanation:
The case explicitly states, 'The navicular bone, similar to talus, has a large articular surface area and for the blood supply it relies on the radial arcade of vessels arising from the dorsalis pedis and medial planter arteries and this could be injured either at the time of fracture or during surgery, which could lead to AVN, non-union and/or collapse of the bone resulting in a painful mid-foot.' This directly answers the question. The navicular's blood supply is indeed precarious, primarily derived from a radial arcade formed by branches of the dorsalis pedis artery dorsally and the medial plantar artery plantarly. This dual supply can be compromised by high-energy fractures or surgical dissection, leading to the dreaded complications of AVN and non-union.
- A. Perforating branches of the peroneal artery: The peroneal artery primarily supplies the lateral compartment of the leg and lateral ankle/hindfoot, not the navicular.
- B. Arcuate artery from the dorsalis pedis artery: The arcuate artery is a branch of the dorsalis pedis artery that supplies the metatarsals, but it is not the primary or sole supply to the navicular body. The 'radial arcade' is a more comprehensive description of the navicular's supply.
- D. Lateral tarsal artery from the dorsalis pedis artery: The lateral tarsal artery is a branch of the dorsalis pedis artery that supplies the lateral tarsus, but again, it's not the primary arcade for the navicular body.
- E. Medial malleolar artery from the posterior tibial artery: The medial malleolar artery supplies the medial malleolus and surrounding ankle structures, not the navicular bone.
Question 25
The candidate discusses the management options for the navicular fracture, stating that operative intervention is favored. However, they also mention a specific scenario where primary fusion of the talonavicular joint might be considered. What is this specific indication for primary fusion, as outlined in the case?
Explanation
Correct Answer: C
Explanation:
The case states, 'The principles of management are to restore the articular surface, stabilize and hold the fracture to allow early mobilization. The aim of the treatment is to have a mobile, pain-free and functional joint. However, sometimes that is not possible due to severe comminution of the articular surface, in which case I may consider primary fusion of the talonavicular joint.' This directly indicates that severe comminution of the articular surface, rendering anatomical reduction and restoration of joint congruity unachievable, is the primary indication for considering primary talonavicular fusion.
- A. Patient refusal for internal fixation: While patient preference is always a factor in consent, it is not a clinical indication for primary fusion in the context of fracture severity.
- B. Significant soft tissue compromise precluding open reduction: Soft tissue compromise might delay surgery or influence the approach, but it doesn't directly lead to a decision for primary fusion of the joint unless the soft tissue damage is so severe that it prevents any form of reconstruction or fixation. The case focuses on articular comminution as the reason for fusion.
- D. Associated Lisfranc injury requiring concurrent fusion: The case describes an 'isolated closed injury of the foot' and does not mention a Lisfranc injury. While a Lisfranc injury might require fusion, it's not the reason for primary talonavicular fusion in this specific navicular fracture scenario.
- E. Presence of pre-existing talonavicular arthritis: Pre-existing arthritis would certainly make fusion a more attractive option, but the case does not mention this. The indication given in the case is specifically related to the acute fracture's severity.
Question 26
During the discussion of potential complications, the candidate lists early complications including nerve injury. Which specific nerve branches are highlighted as being at risk during a medial approach to the navicular?
Explanation
Correct Answer: C
Explanation:
The case states, 'Early complications include infection, nerve injury (branches of superficial and deep peroneal nerves) and vascular injury (dorsalis pedis).' This directly identifies the superficial and deep peroneal nerves as being at risk. While a medial approach is used for the navicular, the deep peroneal nerve runs dorsally and can be at risk during dissection or retraction, especially if the approach extends more dorsally or if there's significant swelling. The superficial peroneal nerve, though more lateral, can also be at risk with extensive dissection or positioning. It's important to consider all major nerves in the vicinity of the surgical field.
- A. Sural nerve and its branches: The sural nerve is located on the posterolateral aspect of the ankle and foot, not typically at direct risk during a medial navicular approach.
- B. Saphenous nerve and its infrapatellar branch: The saphenous nerve is a sensory nerve on the medial side of the leg and ankle, but its infrapatellar branch is much higher, around the knee. While the saphenous nerve itself can be at risk more proximally on the medial ankle, the case specifically mentions peroneal nerves.
- D. Posterior tibial nerve and its calcaneal branches: The posterior tibial nerve is located in the tarsal tunnel on the posteromedial aspect of the ankle, primarily supplying the plantar foot. It is generally not at direct risk during a medial approach to the navicular body.
- E. Medial plantar nerve and its digital branches: The medial plantar nerve is a terminal branch of the posterior tibial nerve, located on the plantar aspect of the foot. While it's on the medial side, it's deep and plantar, not typically at direct risk during a dorsal or medial approach to the navicular body.
Question 27
A 29-year-old female horse rider undergoes operative fixation for a displaced, comminuted intra-articular navicular body fracture. Despite successful anatomical reduction and stable fixation, she develops persistent midfoot pain and stiffness several years post-surgery. Which of the following late complications is most commonly associated with this type of injury, even after optimal surgical management?
Explanation
Correct Answer: C
Explanation:
The case lists 'Late complications include non-union and loss of medial longitudinal arch support, painful talonavicular joint, post-traumatic osteoarthritis, as well as avascular necrosis and collapse.' Among these, post-traumatic osteoarthritis (OA) is a very common and often debilitating long-term complication of intra-articular fractures, especially in weight-bearing joints like the talonavicular joint. Even with anatomical reduction, damage to the articular cartilage at the time of injury, subtle incongruities, or altered biomechanics can lead to progressive degenerative changes and pain.
- A. Chronic regional pain syndrome (CRPS): CRPS is a potential complication of any extremity trauma or surgery, but it is not the most commonly associated late complication specifically with intra-articular navicular fractures after successful fixation.
- B. Recurrent compartment syndrome: Compartment syndrome is an immediate or early complication, not a late complication that recurs years after successful fixation.
- D. Stress fracture of an adjacent metatarsal: While possible, a stress fracture of an adjacent metatarsal is not a direct or most common late complication of a navicular body fracture itself.
- E. Deep vein thrombosis (DVT): DVT is an early complication related to immobility and surgery, not a late complication occurring years post-operatively.
Question 28
The candidate discusses the immediate management of the patient's high-energy foot injury prior to definitive surgical planning. Which of the following is the most critical immediate management step for this type of injury, as mentioned in the case?
Explanation
Correct Answer: C
Explanation:
The case states, 'I would initially treat the injured foot in a backslab, with strict elevation and intermittent cryotherapy, adequate analgesia and close monitoring for evolving compartment syndrome.' For high-energy foot injuries, compartment syndrome is a critical and potentially devastating complication. Early recognition and monitoring are paramount to prevent irreversible tissue damage. Therefore, close monitoring for compartment syndrome is the most critical immediate management step.
- A. Immediate weight-bearing mobilization to prevent stiffness: This is contraindicated for an unstable, displaced fracture. Non-weight bearing and immobilization are necessary.
- B. Administration of prophylactic antibiotics to prevent infection: The case specifies an 'isolated closed injury.' There is no indication for prophylactic antibiotics in a closed fracture unless there are specific risk factors for infection (e.g., immunocompromised patient, severe contamination if open).
- D. Urgent reduction of the fracture in the emergency department: While reduction might be considered, especially if there is significant deformity or neurovascular compromise, the primary immediate concern for a high-energy foot injury is compartment syndrome. A formal reduction is often performed in the operating room after definitive imaging and planning.
- E. Application of a rigid plaster cast for definitive immobilization: A backslab (splint) is preferred initially over a rigid cast to allow for swelling and to facilitate compartment syndrome monitoring. A rigid cast could contribute to compartment syndrome if swelling occurs.
Question 29
Reviewing the initial radiographs of the 29-year-old female horse rider's left foot:
What is the most accurate description of the injury based solely on these images and the initial case presentation?

Explanation
Correct Answer: B
Explanation:
The case description and the candidate's initial assessment explicitly state: 'The radiographs of the left foot, AP and oblique show a displaced fracture of the body of navicular bone with comminution. There is overlap of mid-tarsal bones...' The provided radiographs (Figure 8.16) visually confirm these findings, showing multiple fragments and disruption of the navicular's normal contour and articulation, consistent with a displaced, comminuted intra-articular fracture of the navicular body. The 'overlap of mid-tarsal bones' suggests involvement of the surrounding joints, making it an intra-articular injury.
- A. Isolated non-displaced navicular tuberosity fracture with no mid-tarsal involvement: The images clearly show a fracture involving the main body of the navicular, not just the tuberosity, and it is displaced and comminuted, not non-displaced. There is also mid-tarsal overlap.
- C. Stress fracture of the navicular with associated cuneiform subluxation: A stress fracture typically appears as a subtle cortical break or sclerosis, not a grossly displaced and comminuted fracture as seen here. While cuneiform subluxation might be present, the primary injury is a high-energy fracture.
- D. Avulsion fracture of the navicular with significant talonavicular dislocation: An avulsion fracture is typically a small fragment pulled off by a ligament or tendon. This is a much larger, comminuted fracture of the bone body. While there is disruption, 'significant talonavicular dislocation' is not the primary description given.
- E. Isolated cuboid fracture with secondary navicular impaction: The primary fracture is clearly of the navicular bone, not the cuboid. While impaction might occur, the main injury is the navicular fracture.
Question 30
The candidate outlines the principles of operative management for the navicular fracture: 'to restore the articular surface, stabilize and hold the fracture to allow early mobilization.' Which of the following is NOT a primary goal for operative intervention in this specific navicular body fracture, as implied by the case discussion?
Explanation
Correct Answer: D
Explanation:
The case emphasizes 'to restore the articular surface, stabilize and hold the fracture to allow early mobilization.' While early mobilization is a goal, 'early mobilization' does not equate to 'immediate full weight-bearing.' For a comminuted intra-articular fracture of a weight-bearing bone like the navicular, immediate full weight-bearing would jeopardize the fixation and the healing process. Non-weight bearing or protected weight-bearing is typically required for several weeks to months post-operatively.
- A. Achieve anatomical reduction of the articular surface: This is a stated primary principle: 'restore the articular surface.'
- B. Provide stable fixation to allow for early range of motion: This is a stated primary principle: 'stabilize and hold the fracture to allow early mobilization.'
- C. Prevent avascular necrosis of the navicular bone: The case extensively discusses the vulnerability of the navicular's blood supply and the risk of AVN. While surgery itself can sometimes compromise blood supply, a well-planned surgery aims to preserve it and stabilize the fracture to promote healing, thereby preventing AVN and non-union.
- E. Minimize the risk of post-traumatic osteoarthritis: By restoring the articular surface and achieving stable fixation, the primary goal is to maintain joint congruity and function, which directly aims to minimize the long-term risk of post-traumatic osteoarthritis.
Question 31
The examiner asks the candidate to describe the general consent process. The candidate refers to GMC guidelines. Which of the following principles is NOT a core component of the informed consent process as outlined in the case?
Explanation
Correct Answer: D
Explanation:
The case outlines the GMC guidelines for consent, which emphasize shared decision-making and patient autonomy. The listed components are: '(a) I listen to patients and respect their views about their health; (b) discuss with patients what their views about diagnosis, prognosis, treatment and care involve; (c) share with patients the information they want or need in order to make decisions; (d) maximize patients’ opportunities, and their ability to make decisions for themselves; (e) respect patients’ decisions.'
- A. Respecting patients' decisions, even if they differ from the medical recommendation: This is explicitly stated as point (e).
- B. Maximizing patients' opportunities and ability to make decisions for themselves: This is explicitly stated as point (d).
- C. Sharing with patients the information they want or need to make decisions: This is explicitly stated as point (c).
- D. Ensuring the patient agrees to all aspects of the proposed treatment without question: This statement contradicts the principles of informed consent and shared decision-making. Patients are encouraged to ask questions, express concerns, and make decisions based on comprehensive information, not to agree without question. This represents a paternalistic approach, which is contrary to modern ethical guidelines.
- E. Discussing with patients their views about diagnosis, prognosis, treatment, and care: This is explicitly stated as point (b).
Question 32
A 35-year-old male with a history of multiple hereditary exostoses presents with a rapidly enlarging mass on his proximal femur and increasing pain. MRI demonstrates an osteochondroma with a cartilage cap thickness of 2.5 cm. What is the most likely diagnosis?
Explanation
Question 33
A 42-year-old female is brought in after a rollover MVC. She is hemodynamically unstable. A pelvic radiograph shows a widened pubic symphysis of 4 cm and disrupted posterior sacroiliac ligaments. Where is the most anatomically correct placement for a pelvic circumferential compression device?
Explanation
Question 34
A 24-year-old male sustains a subtrochanteric femur fracture. During closed reduction for intramedullary nailing, the proximal fragment is noted to be flexed, abducted, and externally rotated. Which muscle group is primarily responsible for the flexion deformity of the proximal fragment?
Explanation
Question 35
A 29-year-old male undergoes reamed intramedullary nailing of a closed tibial shaft fracture. Postoperatively, he requires increasing doses of opioids and complains of severe pain with passive toe stretch. His diastolic blood pressure is 70 mmHg. What intracompartmental pressure reading strongly supports the diagnosis of acute compartment syndrome?
Explanation
Question 36
A 12-year-old boy presents with multiple bony prominences around his knees and wrists. Radiographs reveal numerous sessile and pedunculated lesions pointing away from the joints. A mutation in which of the following genes, leading to impaired heparan sulfate synthesis, is most likely responsible?
Explanation
Question 37
A 30-year-old male sustains a vertically oriented (Pauwels Type III) femoral neck fracture. Biomechanically, what is the primary mode of failure for this specific fracture pattern if treated with three parallel cannulated screws alone?
Explanation
Question 38
A 55-year-old female presents with an inability to flex her thumb interphalangeal joint 6 months after open reduction and internal fixation of a distal radius fracture with a volar locking plate. What surgical technical error most likely led to this complication?
Explanation
Question 39
A 28-year-old motorcyclist sustains a high-energy midshaft femur fracture. According to standard trauma protocols, which imaging modality is considered the gold standard to rule out an ipsilateral associated fracture in this scenario?
Explanation
Question 40
A 14-year-old boy has a known pedunculated osteochondroma on the distal medial femur. He recently started cross-country running and complains of new-onset localized pain over the lesion. Radiographs show no change in size or appearance. What is the most common cause of pain in this scenario?
Explanation
Question 41
A 45-year-old male sustains a medial tibial plateau fracture with significant displacement (Schatzker IV) following a varus-directed force. What is the most appropriate surgical approach for optimal buttress plating of this specific fracture pattern?
Explanation
Question 42
A 38-year-old male sustains a Gustilo-Anderson Type IIIB open tibial shaft fracture. Following serial debridements, he requires soft tissue coverage with a free flap. According to the Godina principles, within what timeframe should the free flap ideally be performed to minimize infection and flap failure rates?
Explanation
Question 43
A 4-year-old boy presents with an asymmetric, painless swelling on the medial aspect of his ankle. Radiographs reveal an irregular, lobulated, ossified mass arising from the medial epiphysis of the distal tibia. What is the most likely diagnosis?
Explanation
Question 44
A 26-year-old male sustains a Hawkins Type III talar neck fracture (fracture with subluxation/dislocation of both the subtalar and tibiotalar joints). What is the estimated rate of avascular necrosis (AVN) of the talar body associated with this injury type?
Explanation
Question 45
A 40-year-old female twists her ankle. Radiographs show a short oblique fracture of the distal fibula at the level of the syndesmosis and a transverse medial malleolus fracture. Based on the Lauge-Hansen classification (Supination-External Rotation), what is the first structure injured in this sequence?
Explanation
Question 46
A 50-year-old female sustains a distal femur fracture. CT scan reveals a coronal plane fracture of the lateral femoral condyle. What is the optimal direction of screw placement to achieve the most biomechanically stable fixation for this specific fragment?
Explanation
Question 47
A 10-year-old girl with multiple hereditary exostoses presents for routine follow-up. Which of the following is the most classic forearm deformity associated with this condition?
Explanation
Question 48
A 28-year-old male presents with dorsal wrist pain after a fall on an outstretched hand. Radiographs reveal a widened scapholunate interval of 4 mm. Which portion of the scapholunate interosseous ligament is the primary stabilizer and most crucial to repair?
Explanation
Question 49
A 6-year-old boy sustains a completely displaced extension-type supracondylar humerus fracture. On presentation, the radial pulse is absent, but the hand is warm and pink with brisk capillary refill. What is the most appropriate initial management?
Explanation
Question 50
A 13-year-old male has an asymptomatic, 2 cm osteochondroma on the proximal humerus. The parents request excision due to cosmetic concerns. What is the most appropriate recommendation regarding surgical excision?
Explanation
Question 51
A 24-year-old male with a history of Multiple Hereditary Exostoses (MHE) presents with enlarging, painless masses around his knees. He brings genetic testing results indicating a mutation in the EXT1 gene. What is the precise molecular consequence of this mutation?
Explanation
Question 52
A 35-year-old female with a known solitary osteochondroma of the proximal tibia reports new-onset localized pain and a recent increase in the size of the mass. An MRI is obtained. Which of the following MRI findings is the most reliable indicator of malignant transformation to secondary chondrosarcoma?
Explanation
Question 53
A 68-year-old male sustains a high-energy distal femur fracture. CT imaging reveals a coronal plane fracture of the lateral femoral condyle. What is the most appropriate fixation strategy for this specific fracture pattern?
Explanation
Question 54
A 42-year-old male presents with an unstable pelvic ring injury after a fall from a height. The surgeon plans an anterior intrapelvic (modified Stoppa) approach. Which of the following anatomic structures must be carefully identified and ligated to prevent catastrophic hemorrhage near the superior pubic ramus?
Explanation
Question 55
A 29-year-old motorcyclist sustains a Gustilo-Anderson Type IIIB open tibial shaft fracture.
After initial debridement, external fixation, and appropriate systemic antibiotic initiation, what is the current guideline for the duration of prophylactic antibiotics in this setting?
Explanation
Question 56
A 12-year-old child with Multiple Hereditary Exostoses (MHE) presents with increasing forearm deformity. Radiographs demonstrate the classic Masada Type I deformity. Which of the following is the hallmark radiographic feature of this specific forearm deformity?
Explanation
Question 57
A 22-year-old male complains of severe leg pain out of proportion to examination 6 hours after undergoing intramedullary nailing for a closed tibial shaft fracture. His blood pressure is 110/70 mmHg. Compartment pressures are measured. At what absolute pressure or Delta P threshold is fasciotomy definitively indicated?
Explanation
Question 58
An 18-year-old female presents with a displaced talar neck fracture following a snowboarding accident. She undergoes open reduction and internal fixation. Six weeks postoperatively, a subchondral radiolucent band is visible in the talar dome on the AP radiograph (Hawkins sign). What does this finding indicate?
Explanation
Question 59
A 45-year-old male falls from a roof and sustains a displaced intra-articular calcaneus fracture. The surgeon utilizes the Sanders classification for preoperative planning. On which specific imaging view is this classification system based?
Explanation
Question 60
A 26-year-old male sustains a high-energy femoral neck fracture with a vertical fracture line (Pauwels Type III). What is the primary biomechanical rationale for utilizing a fixed-angle device (e.g., sliding hip screw or cephalomedullary nail) rather than multiple cancellous screws for this injury?
Explanation
Question 61
A polytrauma patient presents with a femur fracture, bilateral pulmonary contusions, and a Glasgow Coma Scale of 7.
His initial serum lactate is 4.5 mmol/L and pH is 7.21. According to the principles of Damage Control Orthopedics (DCO), what is the most appropriate initial management of the femur fracture?
Explanation
Question 62
A 19-year-old male with a solitary distal femur osteochondroma presents with a pulsatile mass in his popliteal fossa and diminished distal pulses. What is the most common etiology of this vascular complication?
Explanation
Question 63
A 50-year-old male is involved in a motor vehicle collision and sustains a complex acetabular fracture.
An obturator oblique radiograph demonstrates the classic 'spur sign'. Which Letournel fracture pattern is pathognomonic for this finding?
Explanation
Question 64
A 4-year-old boy presents with an asymmetric, painless swelling on the medial aspect of his left ankle. Radiographs show an irregular, ossified mass arising from the medial distal tibial epiphysis. What is the most likely diagnosis?
Explanation
Question 65
A 27-year-old female sustains a Lisfranc injury during a horseback riding fall. She has a 'fleck sign' on her AP foot radiograph. This sign represents a bony avulsion of the Lisfranc ligament from which of the following anatomic locations?
Explanation
Question 66
A 33-year-old male undergoes open reduction and internal fixation of a terrible triad injury of the elbow. The standard surgical sequence involves fixing the coronoid, then the radial head. What is the crucial final step in restoring stability to this elbow?
Explanation
Question 67
A 21-year-old motorcyclist sustains a traumatic scapulothoracic dissociation. Physical examination reveals massive shoulder swelling and an insensate, flail upper extremity. Which of the following injuries has the highest association with this clinical entity and largely dictates the ultimate functional prognosis?
Explanation
Question 68
A 60-year-old female sustains a split-depression fracture of the lateral tibial plateau (Schatzker Type II) following a valgus stress injury. During surgical approach and articular elevation, which intra-articular structure is most commonly found incarcerated within the fracture site?
Explanation
Question 69
A 16-year-old male presents with a painful, firm nodule beneath the nail bed of his great toe. Radiographs demonstrate an exophytic bony mass projecting from the dorsal aspect of the distal phalanx. Histology reveals a cartilage cap, but imaging shows no medullary continuity with the host bone. What is the diagnosis?
Explanation
Question 70
A 70-year-old female on long-term alendronate therapy for osteoporosis presents with atraumatic thigh pain. Radiographs reveal a transverse, non-comminuted fracture of the femoral shaft with localized lateral cortical thickening. Which of the following is an expected histologic or biological feature of this specific type of fracture?
Explanation
Question 71
A 15-year-old boy presents with a painless, bony prominence on the distal medial aspect of his thigh. Radiographs demonstrate a pedunculated osseous lesion pointing away from the joint line with distinct corticomedullary continuity. What is the histologic composition of the cartilaginous cap covering this lesion?
Explanation
Question 72
A 12-year-old female with a family history of multiple bony deformities is diagnosed with Hereditary Multiple Exostoses (HME). Genetic testing is most likely to reveal a mutation affecting which of the following cellular processes?
Explanation
Question 73
A 35-year-old male with known Hereditary Multiple Exostoses presents with rapidly increasing pain and swelling over a long-standing lesion on his proximal humerus. Magnetic resonance imaging (MRI) is obtained. Which of the following findings is most highly predictive of secondary malignant transformation to chondrosarcoma?
Explanation
Question 74
A 22-year-old male incidentally discovers a hard mass around his left knee. He has no pain, neurovascular symptoms, or mechanical blocks to motion. Radiographs reveal a sessile exostosis on the distal femur with medullary continuity.
What is the most appropriate management for this patient?
Explanation
Question 75
A 28-year-old snowboarder sustains a high-energy talar neck fracture. Six weeks post-operatively, an anteroposterior radiograph of the ankle reveals a subchondral lucency spanning the talar dome. What does this radiographic finding indicate?
Explanation
Question 76
A 6-year-old boy falls from monkey bars and sustains a significantly displaced extension-type supracondylar humerus fracture. On examination, he is unable to make an 'A-OK' sign. Which of the following muscle functions is directly impaired?
Explanation
Question 77
A 25-year-old male sustains a vertically oriented femoral neck fracture (Pauwels Type III) after a high-speed motorcycle accident. Biomechanically, which of the following best explains the high rate of failure and nonunion associated with this specific fracture pattern?
Explanation
Question 78
A 32-year-old male is admitted with a closed midshaft tibia fracture. Six hours later, he complains of severe leg pain out of proportion to the injury, significantly worsened by passive toe extension. Which of the following absolute or delta pressure criteria is widely accepted as an indication for emergency fasciotomy?
Explanation
Question 79
A 40-year-old male requires an ilioinguinal approach for open reduction and internal fixation of an anterior column acetabular fracture. During the dissection, massive hemorrhage occurs near the superior pubic ramus. The injured vessel is most likely an anastomosis between which two vascular systems?
Explanation
Question 80
A 29-year-old farmer sustains an open tibial shaft fracture with massive soft tissue stripping and gross soil contamination (Gustilo-Anderson Type IIIA) from a tractor rollover. In addition to a first-generation cephalosporin and an aminoglycoside, which of the following antibiotics is strongly indicated?
Explanation
Question 81
A 55-year-old female presents with a Schatzker II (split-depression) lateral tibial plateau fracture following a fall. She is scheduled for open reduction and internal fixation. Preoperative MRI is most likely to reveal an associated injury to which of the following structures?
Explanation
Question 82
An extensile lateral approach is planned for the operative fixation of a displaced intra-articular calcaneus fracture. To minimize the risk of full-thickness skin flap necrosis, the surgeon must carefully preserve the primary arterial supply to the corner of the flap. Which artery supplies this crucial angiosome?
Explanation
Question 83
A 35-year-old male undergoes intramedullary nailing of a comminuted femoral shaft fracture on a fracture table. Postoperatively, he complains of numbness in his perineal region. What is the primary etiology of this complication?
Explanation
Question 84
A 60-year-old male sustains a completely displaced supracondylar distal femur fracture. Radiographs show a characteristic deformity where the distal articular fragment is extended. Which muscle is primarily responsible for this deforming force?
Explanation
Question 85
A 68-year-old female presents with a complex proximal humerus fracture. Based on the Hertel radiographic criteria, which of the following features is most predictive of ischemia and subsequent avascular necrosis of the humeral head?
Explanation
Question 86
A 72-year-old female on long-term alendronate therapy sustains a low-energy, transverse subtrochanteric femur fracture with a medial cortical spike. What is the primary cellular mechanism by which bisphosphonates increase the risk of this specific atypical fracture pattern?
Explanation
Question 87
A 24-year-old football player sustains an injury to his midfoot. Weight-bearing radiographs show a 3 mm diastasis between the first and second metatarsal bases. The primary ligament injured in this condition connects which two osseous structures?
Explanation
Question 88
A 45-year-old male is undergoing evaluation for adult spinal deformity. The surgeon calculates the pelvic incidence (PI) to guide sagittal balance correction. Which of the following equations correctly defines pelvic incidence?
Explanation
Question 89
A 33-year-old unrestrained driver is involved in a high-speed collision, sustaining a traumatic spondylolisthesis of the axis (Hangman's fracture). The most common mechanism of injury producing this specific fracture pattern is:
Explanation
Question 90
A 26-year-old male is brought to the trauma bay with a 'floating knee' injury (ipsilateral closed fractures of the femoral shaft and tibial shaft). He is hemodynamically stable. What is the greatest systemic benefit of early operative stabilization (within 24 hours) of both fractures?
Explanation
Question 91
A 12-year-old boy presents with multiple painless, hard bony bumps around his knees and ankles. Radiographs reveal multiple sessile and pedunculated lesions pointing away from the joint line. Mutations in which of the following genes are most commonly associated with this patient's underlying condition?
Explanation
Question 92
A 35-year-old male with a known history of Multiple Hereditary Exostoses presents with a newly enlarging, painful mass over his proximal humerus. MRI demonstrates an osteochondroma with a thickened cartilage cap. A cartilage cap thicker than what measurement in a skeletally mature adult is highly suspicious for secondary malignant transformation?
Explanation
Question 93
A 25-year-old male sustains a vertically oriented femoral neck fracture (Pauwels type III) after a fall from a height. Which of the following internal fixation constructs provides the greatest biomechanical stability against shear forces for this specific fracture pattern?
Explanation
Question 94
A 42-year-old skier sustains a twisting injury to her knee. Radiographs reveal a depressed lateral tibial plateau fracture.
During the surgical approach for open reduction and internal fixation, the surgeon decides on an anterolateral approach. Which structure is at greatest risk of iatrogenic injury during meniscal elevation (submeniscal arthrotomy)?
Explanation
Question 95
A 28-year-old male is involved in a high-speed motor vehicle collision and sustains a Hawkins type III talar neck fracture. What is the approximate rate of avascular necrosis (AVN) of the talar body associated with this specific injury pattern?
Explanation
Question 96
A 14-year-old boy presents with a symptomatic pedunculated osteochondroma on the distal medial femur causing snapping of the pes anserinus tendons. Which of the following is the most critical technical principle when excising this lesion to prevent recurrence?
Explanation
Question 97
A 30-year-old farmer sustains a severe open midshaft tibia fracture (Gustilo-Anderson IIIB) with gross soil contamination after a tractor accident. According to classic orthopedic trauma guidelines, which of the following is the most appropriate initial prophylactic antibiotic regimen?
Explanation
Question 98
A 22-year-old male develops severe, unrelenting leg pain out of proportion to his injury 12 hours after intramedullary nailing of a closed tibial shaft fracture. Pain is exacerbated by passive stretch of the hallux. If intracompartmental pressures are measured, which of the following thresholds is the most widely accepted absolute indication for four-compartment fasciotomy?
Explanation
Question 99
A 45-year-old roofer falls from a ladder and sustains a displaced intra-articular calcaneus fracture.
He is indicated for open reduction and internal fixation via an extensile lateral approach. Which complication is most frequently associated with this specific surgical approach?
Explanation
None
