ABOS Part I & AAOS OITE Orthopedic Trauma Review: Ankle, Elbow, Calcaneus | Part 22147
Key Takeaway
An orthopedic trauma review for ABOS Part I and AAOS OITE exams covers high-yield clinical cases. Key topics include complex ankle fractures (pilon, posterior malleolus, calcaneal) and terrible triad elbow injuries, focusing on diagnosis, surgical management, and rehabilitation protocols for these challenging conditions.
ABOS Part I & AAOS OITE Orthopedic Trauma Review: Ankle, Elbow, Calcaneus | Part 22147
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 38-year-old male sustains a high-energy ankle injury. Initial radiographs show a trimalleolar fracture with a large posterior malleolus fragment. A pre-operative CT scan, as depicted conceptually below, confirms a displaced posterior malleolus fragment involving 35% of the articular surface and a posterolateral pilon component. The patient is otherwise healthy, and the soft tissue envelope is viable. During the posterolateral approach, after skin incision and subcutaneous dissection, which neurovascular structure is most vulnerable and requires meticulous identification and protection?

Explanation
Correct Answer: C
The sural nerve is a purely sensory nerve that runs superficially along the posterolateral aspect of the lower leg, typically coursing with the small saphenous vein. It is highly vulnerable during the skin incision and initial dissection of the posterolateral approach, especially at the level of the ankle joint. Meticulous identification and retraction (usually anteriorly with the peroneal tendons) are crucial for its preservation.
Option A (Posterior Tibial Nerve): This nerve is located more medially and deep, within the tarsal tunnel (posterior to the medial malleolus). It is generally not at direct risk with a strictly posterolateral approach.
Option B (Peroneal Artery): This artery is located deep in the posterior compartment, more medially, and is not typically at risk with the posterolateral approach.
Option D (Flexor Hallucis Longus Tendon): The FHL tendon is located deep and medial to the Achilles tendon. While it forms part of the medial boundary of the internervous plane and may be exposed during deeper dissection for pilon fractures, it is a tendon, not a neurovascular structure, and is not the most vulnerable structure during initial superficial dissection.
Option E (Tibialis Posterior Tendon): This tendon is located more medially and deeper within the posterior compartment, generally not directly exposed or at risk with the posterolateral approach.
Question 2
A 55-year-old female presents with an ankle fracture after a fall from a height. Initial radiographs are concerning for a pilon fracture. A pre-operative CT scan, as conceptually illustrated below, reveals a posterolateral pilon fracture with significant articular impaction and a 3mm articular step-off. The soft tissues are swollen but without blistering, and the 'wrinkle sign' is present. Which of the following is the most appropriate initial management strategy?

Explanation
Correct Answer: C
High-energy pilon fractures, especially with significant articular impaction and comminution, often present with severe soft tissue swelling. The presence of the 'wrinkle sign' indicates that the soft tissue envelope is improving but does not necessarily mean it is ready for definitive internal fixation, particularly for a high-energy injury like a pilon fracture. Staged management, beginning with external fixation to stabilize the fracture, restore length, and allow the soft tissue swelling to subside, is the most appropriate initial strategy. Definitive ORIF is then performed once the soft tissue envelope is quiescent (typically 7-14 days).
Option A (Immediate ORIF): While the fracture pattern dictates ORIF, immediate surgery for a high-energy pilon fracture with significant swelling, even with a 'wrinkle sign,' carries a high risk of wound complications (dehiscence, infection, necrosis). Delaying definitive fixation is generally safer.
Option B (Closed reduction and casting): This is highly unlikely to achieve or maintain anatomical reduction of a displaced posterolateral pilon fracture with articular impaction, leading to poor outcomes and post-traumatic arthritis.
Option D (Immediate ankle arthrodesis): While severe post-traumatic arthritis can be a sequela, primary arthrodesis is rarely indicated for acute pilon fractures unless there is extensive bone loss, irrecoverable articular damage, or severe patient comorbidities precluding reconstruction. The goal is always to preserve the joint if possible.
Option E (Non-weight bearing in a walking boot): A walking boot provides insufficient immobilization and protection for a displaced pilon fracture and would not allow for anatomical reduction or healing, leading to malunion and severe post-traumatic arthritis.
Question 3
A 28-year-old athlete sustains an ankle injury during a soccer match. Radiographs show a lateral malleolus fracture and a posterior malleolus fracture. A CT scan, as conceptually shown below, confirms a displaced posterior malleolus fragment involving 20% of the distal tibial articular surface, with an associated fibular fracture. Intraoperatively, after reducing and fixing the lateral malleolus, a Cotton test reveals persistent syndesmotic instability. Which of the following statements best explains the biomechanical significance of the posterior malleolus in this scenario?

Explanation
Correct Answer: C
The posterior malleolus serves as the primary attachment site for the Posterior Inferior Tibiofibular Ligament (PITFL), which is a critical component of the syndesmosis. A displaced posterior malleolus fracture, even if relatively small (e.g., 20% as in this case), implies disruption or avulsion of the PITFL from the tibia. This directly compromises syndesmotic stability, leading to persistent instability even after fibular fixation, as demonstrated by the positive Cotton test. Direct reduction and fixation of the posterior malleolus are often necessary to restore PITFL integrity and syndesmotic stability.
Option A (Ankle plantarflexion strength): Ankle plantarflexion strength is primarily provided by the gastrocnemius and soleus muscles via the Achilles tendon, not directly by the posterior malleolus.
Option B (Deltoid ligament attachment): The deltoid ligament attaches to the medial malleolus and is crucial for medial ankle stability, not the posterior malleolus.
Option D (Subtalar joint congruity): The subtalar joint is formed by the talus and calcaneus. While overall ankle alignment can indirectly affect subtalar mechanics, the posterior malleolus primarily affects tibiotalar and syndesmotic stability, not subtalar joint congruity directly.
Option E (Achilles tendon rupture risk): There is no direct correlation between the size of the posterior malleolus fragment and the risk of Achilles tendon rupture. Achilles tendon rupture is a separate injury mechanism.
Question 4
A 42-year-old construction worker presents with a complex ankle fracture after a fall. A CT scan, conceptually shown below, reveals a posterolateral pilon fracture with significant comminution and a large metaphyseal defect after reduction of the articular fragments. During the posterolateral approach, after achieving anatomical reduction of the articular fragments and temporary K-wire fixation, what is the most appropriate next step to ensure stable fixation and prevent collapse?

Explanation
Correct Answer: C
In posterolateral pilon fractures with significant comminution and a metaphyseal defect, simply reducing the articular fragments and fixing them with plates/screws may not be sufficient. The underlying bone loss can lead to collapse of the articular surface over time, resulting in malunion and post-traumatic arthritis. Placing bone graft (autograft or allograft) beneath the reduced articular fragments provides structural support, preventing collapse and promoting healing. This is a critical step in managing these high-energy injuries.
Option A (Apply a 1/3 tubular plate to the posterior aspect of the fibula): While fibular fixation is often necessary in combined injuries, it addresses the fibula, not the metaphyseal defect of the tibia. Fibular fixation is typically done to restore length and rotation, which can aid in tibial reduction, but it doesn't directly support the tibial articular surface from collapse.
Option B (Perform a syndesmotic screw fixation): Syndesmotic fixation is indicated if instability persists after reduction of the posterior malleolus and fibula. While important, it does not address the metaphyseal bone defect in a pilon fracture.
Option D (Immediately close the wound and apply a cast): This would be premature and neglect the critical step of providing structural support to the reduced articular fragments, leading to likely failure of fixation and collapse.
Option E (Insert a single lag screw from anterior to posterior): Lag screws are used for interfragmentary compression, typically from posterior to anterior in this approach. While important for fragment fixation, a single lag screw alone would not provide adequate buttress support or address a significant metaphyseal defect in a comminuted pilon fracture.
Question 5
A 60-year-old diabetic patient undergoes ORIF of a displaced posterior malleolus fracture via a posterolateral approach. Two weeks post-operatively, the patient presents with increasing pain, erythema, and purulent discharge from the surgical incision, as conceptually shown below. Cultures confirm a deep surgical site infection. What is the most appropriate immediate management strategy?

Explanation
Correct Answer: C
A deep surgical site infection, especially in a diabetic patient, is a serious complication requiring aggressive management. The presence of purulent discharge and increasing pain/erythema indicates a deep infection. The most appropriate immediate management involves surgical debridement to remove infected and necrotic tissue, initiation of broad-spectrum intravenous antibiotics (tailored to culture results), and often local wound management techniques such as negative pressure wound therapy (NPWT) or antibiotic beads. Hardware removal is typically considered later, once the fracture has healed, unless the infection is uncontrolled or the hardware is clearly contributing to the infection.
Option A (Oral antibiotics and continued observation): Oral antibiotics are generally insufficient for deep surgical site infections, especially with purulent discharge. Observation risks progression of the infection, potentially leading to osteomyelitis or sepsis.
Option B (Hardware removal and immediate wound closure): Hardware removal is usually delayed until fracture healing, unless the infection is refractory. Immediate wound closure without adequate debridement and control of the infection would likely lead to recurrence and worsening of the infection.
Option D (Topical antibiotic ointment and sterile dressing changes): This is appropriate for superficial wound issues but completely inadequate for a deep surgical site infection with purulent discharge.
Option E (Referral to a pain management specialist): While the patient is experiencing pain, the primary issue is an active infection that requires surgical and medical intervention, not just pain management. Addressing the infection is paramount.
Question 6
A 32-year-old male presents with a displaced posterior malleolus fracture involving 18% of the articular surface, along with a stable lateral malleolus fracture. A CT scan, conceptually shown below, confirms a 3mm articular step-off. The patient is otherwise healthy. According to current literature guidelines, what is the most appropriate management strategy?

Explanation
Correct Answer: C
While historically a 25-30% involvement of the articular surface was a common threshold for posterior malleolus fixation, current literature suggests that smaller fragments (e.g., 10-15% or more) warrant operative fixation if they are displaced (>2mm step-off/gap) or contribute to syndesmotic instability. In this case, an 18% fragment with a 3mm articular step-off clearly meets the criteria for operative intervention to restore articular congruity and prevent post-traumatic arthritis. The posterolateral approach offers direct visualization and facilitates anatomical reduction and stable internal fixation.
Option A (Non-operative management): Non-operative management is typically reserved for minimally displaced fragments (<2mm step-off) and smaller fragment sizes (<10-15%) without syndesmotic instability. A 3mm step-off is significant and requires surgical correction.
Option B (Indirect reduction and percutaneous screw fixation): Indirect reduction techniques are often unreliable in achieving and maintaining anatomical congruity, especially for displaced fragments. Direct visualization via an open approach is preferred to ensure anatomical reduction.
Option D (Immediate ankle arthrodesis): Ankle arthrodesis is a salvage procedure for end-stage arthritis and is not indicated as a primary treatment for an acute, reconstructible posterior malleolus fracture.
Option E (External fixation as definitive management): External fixation is primarily used as a temporizing measure for severe soft tissue injuries or highly comminuted pilon fractures, or for definitive management in rare cases of severe comorbidities. It is not appropriate for definitive management of a displaced posterior malleolus fracture requiring articular reduction.
Question 7
A 48-year-old male presents with a complex ankle fracture. Pre-operative planning includes a CT scan, conceptually shown below, which confirms a posterolateral pilon fracture with significant articular involvement. The patient is scheduled for ORIF via a posterolateral approach. Which of the following patient positions offers the best direct visualization of the entire posterior aspect of the distal tibia and fibula for this approach?

Explanation
Correct Answer: C
The prone position offers excellent direct visualization of the entire posterior aspect of the distal tibia and fibula, which is crucial for addressing posterolateral pilon and posterior malleolus fractures. It allows for easy access to the posterior aspect of both the tibia and fibula, facilitating combined fixation if a fibular fracture is also present.
Option A (Supine position with the leg internally rotated): While some posterior malleolus fractures can be approached indirectly or with a limited posterior incision in supine, it does not provide the comprehensive direct visualization needed for complex posterolateral pilon fractures or large posterior malleolus fragments.
Option B (Lateral decubitus position): The lateral decubitus position can be used for the posterolateral approach, and it offers easier anesthetic access. However, direct visualization posteriorly can be more challenging than in prone, and maintaining stable exposure may require specialized leg holders or additional assistants.
Option D (Beach chair position): The beach chair position is typically used for shoulder surgery and is not suitable for ankle surgery.
Option E (Lithotomy position): The lithotomy position is used for perineal or lower abdominal surgery and is not suitable for this ankle approach.
Question 8
During a posterolateral approach for a displaced posterior malleolus fracture, the surgeon identifies the internervous plane. Which of the following structures defines the anterolateral boundary of this surgical interval?

Explanation
Correct Answer: C
The key internervous and internervascular plane for the posterolateral approach is between the Achilles tendon and FHL muscle belly (medially/posteriorly) and the peroneal tendons (longus and brevis) and their muscle belly (anterolaterally). The peroneal tendons are mobilized and retracted anteriorly to expose the posterior aspect of the distal tibia and fibula.
Option A (Achilles tendon): The Achilles tendon forms the posterior/medial boundary of the approach and is retracted medially.
Option B (Flexor Hallucis Longus (FHL) muscle belly): The FHL muscle belly is located deep and medial to the Achilles tendon and forms part of the medial/posterior boundary of the interval, retracted medially.
Option D (Posterior Tibial Artery): The posterior tibial artery is located more medially within the tarsal tunnel and is not part of the direct internervous plane for the posterolateral approach.
Option E (Tibialis Posterior tendon): The Tibialis Posterior tendon is located more medially and deeper within the posterior compartment, generally not directly exposed or at risk with the posterolateral approach.
Question 9
A 70-year-old patient undergoes ORIF of a complex trimalleolar ankle fracture, including a large, displaced posterior malleolus fragment, via a posterolateral approach. Post-operatively, the patient is placed in a well-padded posterior splint. At the 6-week follow-up, radiographs, conceptually shown below, demonstrate early signs of fracture healing, and the patient reports minimal pain. What is the most appropriate next step in the rehabilitation protocol?

Explanation
Correct Answer: C
For complex ankle fractures, especially those involving the posterior malleolus and requiring ORIF, non-weight bearing (NWB) is typically maintained for 6-8 weeks. At 6 weeks, with radiographic evidence of early healing and minimal pain, the patient can usually transition from a posterior splint to a removable walking boot (CAM walker). This allows for controlled protection while gradually progressing to partial weight-bearing (PWB) over the next 4-6 weeks, as tolerated and guided by clinical and radiographic assessment. Gentle active and passive range of motion exercises can also be initiated out of the boot.
Option A (Full weight-bearing in a regular shoe): Full weight-bearing at 6 weeks is too early for a complex trimalleolar fracture, risking hardware failure, loss of reduction, or delayed healing.
Option B (Initiate aggressive ankle strengthening exercises): While gentle range of motion and isometric exercises can begin, aggressive strengthening with resistance bands is typically reserved for later phases (Phase 3: Advanced Strengthening & Functional Return), after significant weight-bearing has been achieved and fracture healing is more robust.
Option D (Immediate return to pre-injury activities): This is far too early and would almost certainly lead to re-injury or complications. Return to sport/activity is typically 4-6 months or longer, depending on the injury and patient.
Option E (Continue non-weight bearing in the posterior splint for another 6 weeks): While some complex pilon fractures might require longer NWB, for a posterior malleolus fracture with early healing at 6 weeks, continuing strict NWB in a splint for another 6 weeks is overly conservative and would delay rehabilitation unnecessarily. Transitioning to a boot with PWB is the appropriate next step.
Question 10
A 35-year-old male undergoes ORIF of a posterolateral pilon fracture. During the procedure, after reduction of the articular fragments, the surgeon notes a significant metaphyseal defect. Bone graft is placed to support the articular surface. For definitive fixation, which of the following plating strategies is most appropriate for this fracture pattern?

Explanation
Correct Answer: C
For posterolateral pilon fractures, specialized posterior pilon plates (often pre-contoured) or conventional locking plates applied to the posterior or posterolateral surface of the distal tibia are most appropriate. These plates provide crucial buttress support to the articular fragments, preventing posterior displacement and collapse, especially when there is a metaphyseal defect that has been grafted. Locking plates offer angular stability, which is beneficial in comminuted fractures and osteopenic bone.
Option A (Anterior plating): Anterior plating is used for anterior pilon fragments but would not provide direct buttress support for a posterolateral fragment and would require a separate incision or extensive soft tissue dissection.
Option B (Medial plating): Medial plating is used for medial malleolus fractures or medial pilon fragments. It would not adequately address a posterolateral pilon fracture.
Option D (External fixation as the sole definitive treatment): While external fixation can be a temporizing measure, it is rarely the sole definitive treatment for displaced articular pilon fractures, as it does not allow for anatomical reduction and stable internal fixation of the articular surface, leading to poor outcomes.
Option E (Isolated lag screw fixation without a plate): While lag screws are critical for interfragmentary compression, isolated lag screw fixation is generally insufficient for complex pilon fractures with comminution and metaphyseal defects. A plate is needed to provide buttress support and overall construct stability.
Question 11
A 50-year-old male presents with a chronic, symptomatic malunion of a posterior malleolus fracture, which was initially treated non-operatively. He experiences persistent pain, stiffness, and limited range of motion. Radiographs and a CT scan, conceptually shown below, confirm a significant residual articular step-off and altered ankle mechanics. Which of the following complications is he most likely experiencing, and what is the most appropriate long-term management strategy?

Explanation
Correct Answer: D
The description of a chronic, symptomatic malunion with persistent pain, stiffness, limited range of motion, and significant residual articular step-off strongly indicates the development of post-traumatic arthritis (PTA). Malunion and residual articular incongruity are primary causes of PTA. For advanced, diffuse PTA with debilitating symptoms, long-term management options include ankle arthrodesis (fusion) or total ankle arthroplasty (replacement), depending on patient factors and surgeon preference.
Option A (Sural nerve neuroma): While sural nerve injury is a known complication of the posterolateral approach, it typically presents with neuropathic pain and sensory deficits, not primarily with chronic stiffness, limited ROM, and altered ankle mechanics from a malunion. Also, this patient was treated non-operatively, so surgical nerve injury is less likely.
Option B (Hardware irritation): This patient was treated non-operatively, so there is no hardware to cause irritation.
Option C (Deep vein thrombosis): DVT is an acute complication, typically presenting with calf pain and swelling, and is managed with anticoagulation. It does not explain chronic malunion symptoms.
Option E (Syndesmotic malreduction): While syndesmotic malreduction can lead to pain and instability, the primary issue described is a malunion of the posterior malleolus itself, leading to articular incongruity and arthritis, rather than isolated syndesmotic issues. Revision syndesmotic fixation would not address the established arthritis from the malunion.
Question 12
A 38-year-old male presents to the emergency department after a fall onto an outstretched hand with his forearm supinated, experiencing an axial load and valgus stress on his elbow. Clinical examination and imaging confirm a terrible triad injury. Based on the described mechanism, which of the following structures is most likely the *initial* ligamentous injury to occur in this sequential pattern?
Explanation
Correct Answer: C
The case explicitly states that the terrible triad injury (TTI) typically results from a fall onto an outstretched hand with the forearm supinated, leading to an axial load, valgus stress, and external rotation moment. This mechanism initiates a sequential pattern of soft tissue and bony injury, beginning with the LUCL complex, progressing to the radial head, and finally involving the coronoid. The LUCL is the primary stabilizer against posterolateral rotatory subluxation and is invariably disrupted in TTI.
Options A and B are incorrect because the MCL complex is typically spared in a primary TTI, although its integrity must always be assessed. Options D and E are components of the lateral collateral ligament complex, but the LUCL is specifically identified as the primary stabilizer against posterolateral rotatory subluxation and the initial structure to fail in this injury pattern.
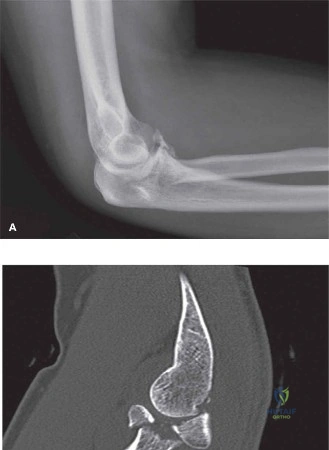
Question 13
A terrible triad injury involves a combination of radial head fracture, coronoid process fracture, and disruption of the lateral ulnar collateral ligament (LUCL) complex. Each of these components contributes to elbow stability. Which of the following bony structures is described as a key anterior stabilizer, primarily resisting posterior displacement of the ulna relative to the humerus?
Explanation
Correct Answer: C
The case states under 'Surgical Anatomy & Biomechanics' that the 'Coronoid process is a key anterior stabilizer, resisting posterior displacement of the ulna relative to the humerus. Fractures of the coronoid significantly compromise this inherent bony stability.' This highlights its crucial role in preventing posterior dislocation of the elbow.
The radial head (Option A) contributes to valgus stability and resistance to axial loading. The olecranon process (Option B) forms the posterior part of the trochlear notch but is not the primary anterior buttress. The lateral epicondyle (Option D) is an origin for ligaments and muscles, not a primary anterior bony stabilizer. The capitellum (Option E) is part of the distal humerus and articulates with the radial head, but it is not an anterior stabilizer of the ulna.
Question 14
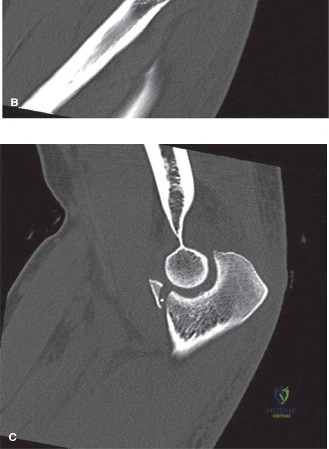
A 55-year-old patient presents with a suspected terrible triad injury after a fall. Initial plain radiographs confirm an elbow dislocation and a comminuted radial head fracture. The surgeon is planning for operative intervention.
Based on the provided image and the case description, which imaging modality is *absolutely essential* for comprehensive pre-operative planning in this case, and what specific information does it provide?
Explanation
Correct Answer: C
The case explicitly states under 'Diagnostic Workup' that a 'Computed Tomography (CT) Scan: Absolutely essential. A high-resolution CT scan with 3D reconstructions provides invaluable information regarding: Coronoid fracture morphology (size, comminution, displacement, and involvement of the sublime tubercle); Radial head fracture pattern (number of fragments, displacement, articular step-off, and associated impaction); Humerus and ulna integrity; Congruity of reduction.' The image provided is an example of such a CT scan, further emphasizing its importance.
Option A (MRI) can provide detailed information about ligamentous injuries but is not routinely required acutely and is described as supplementary. Option B (Ultrasound) is useful for soft tissue and vascular assessment but does not provide the detailed bony architecture needed for surgical planning of complex fractures. Option D (Stress radiographs) can confirm instability but does not provide the detailed fracture morphology. Option E (Arthrography) is rarely used acutely for TTI and is less informative than CT for bony injuries.
Question 15
A 42-year-old patient presents with an elbow dislocation, a Mason Type III radial head fracture, and an O'Driscoll Type II coronoid fracture involving 15% of the coronoid height. After closed reduction, the elbow remains grossly unstable through a 30-130 degree arc of motion with gentle valgus and rotational stress. The patient is medically fit for surgery. Based on the case description, what is the most appropriate management strategy?
Explanation
Correct Answer: C
The case states that 'All terrible triad injuries: By definition, the combination of radial head fracture, coronoid fracture, and LUCL disruption leads to gross elbow instability, necessitating surgical stabilization.' It further specifies operative indications for Mason Type III radial head fractures and O'Driscoll Type II coronoid fractures (especially if >10-15% of coronoid height is involved), and the necessity of LUCL repair. The description of gross instability after reduction is a definitive indication for surgery.
Option A is incorrect because non-operative management is 'extremely rare for true TTI' and typically leads to poor outcomes. Option B (radial head excision) is 'generally contraindicated in TTI' due to profound loss of valgus and axial stability. Option D (dynamic external fixation alone) is not the primary treatment for TTI; internal fixation of the bony components and ligament repair are essential. Option E (total elbow arthroplasty) is a salvage procedure for severe end-stage disease or recurrent instability, not typically the immediate treatment for an acute TTI in a 42-year-old.
Question 16
During surgical repair of a terrible triad injury, the surgeon encounters an O'Driscoll Type I coronoid fracture, characterized by a >2mm fragment from the tip. The fragment is displaced and contributes to the overall instability. The surgeon has gained adequate exposure through a lateral approach. Which of the following is the most appropriate technique for managing this coronoid fracture, considering its size and the overall instability of a TTI?
Explanation
Correct Answer: B
The case, under 'Coronoid Fracture Management', states: 'For Type I and some Type II fractures (tip or anteromedial facet fractures), the fragment can often be visualized and addressed through the lateral approach... Suture Lasso/Lariat Technique: For small to medium-sized fragments (O'Driscoll Type I/II), sutures are passed through drill holes in the proximal ulna, lassoing the coronoid fragment and tying it down, restoring its position.'
Option A (excision) is incorrect as the coronoid is a critical stabilizer and fragments should be repaired if possible. Option C (lag screw fixation) and Option D (small plate fixation) are typically reserved for larger, non-comminuted fragments or comminuted basal fractures (O'Driscoll Type III), often requiring a separate medial incision for direct visualization and reduction, which is not specified as necessary for a Type I fragment in this scenario. Option E (non-operative management) is generally contraindicated for TTI due to inherent instability.
Question 17
A surgeon is addressing a terrible triad injury in a 60-year-old patient. The radial head is found to be severely comminuted (Mason Type IV) and unreconstructible, making ORIF unfeasible.
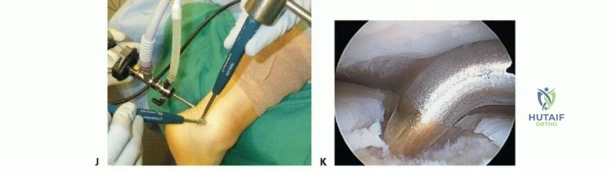
Referring to the intra-operative field shown and the principles outlined in the case, which of the following is the *preferred* management strategy for this radial head fracture in the context of a terrible triad injury?
Explanation
Correct Answer: C
The case states under 'Radial Head Fracture Management' that 'Radial Head Arthroplasty (Replacement): The preferred option for severely comminuted or unreconstructible Mason Type III or IV fractures. Implants can be metal (cobalt-chrome, titanium) or pyrocarbon. The goal is to restore the correct radial length and provide a buttress against valgus stress.' The image shows the exposure of the radial head, which would be necessary for either ORIF or arthroplasty.
Option A (radial head excision) is explicitly stated as 'Generally contraindicated in TTI' due to profound loss of valgus and axial stability. Option B (ORIF) is for reconstructible fractures, which is not the case here. Option D (non-operative management) is inappropriate for a TTI. Option E (external fixation) is not a primary treatment for the radial head fracture itself but might be used as an adjunct for overall elbow stability in very unstable cases, not as a substitute for addressing the radial head.
Question 18
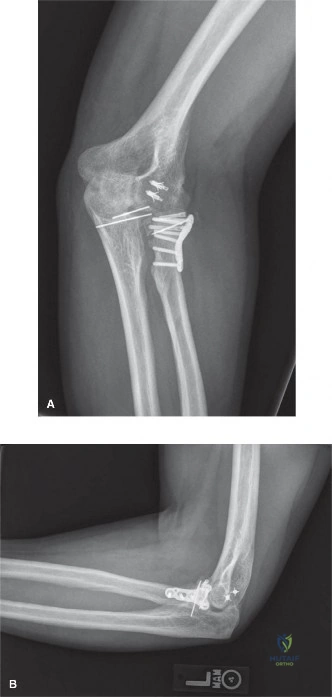
Following successful repair of the coronoid and radial head in a terrible triad injury, the surgeon proceeds to address the lateral ulnar collateral ligament (LUCL). The LUCL is found to be avulsed from its humeral origin at the lateral epicondyle, with good tissue quality.
Based on the typical surgical sequence and the principles outlined in the case, which of the following best describes the next step for LUCL repair and its appropriate tensioning?
Explanation
Correct Answer: B
The case, under 'Lateral Ulnar Collateral Ligament (LUCL) Repair/Reconstruction', states: 'If the tissue quality is good and the ligament can be reapproximated to its anatomic origin on the lateral epicondyle, suture anchors (typically 2-3) are placed into the epicondyle. Non-absorbable sutures are passed through the avulsed ligamentous tissue and tied down with the forearm in pronation and the elbow flexed to 60-90 degrees to tension the LUCL appropriately.' The image shows a post-operative radiograph consistent with internal fixation and likely ligamentous repair, supporting the surgical approach.
Option A is incorrect because the forearm should be in pronation and the elbow flexed to tension the LUCL correctly, not supination and full extension. Option C (reconstruction) is for severely damaged or chronic LUCL tissue, not good quality tissue. Option D (excision) and Option E (non-operative management) are incorrect as LUCL repair is crucial for posterolateral rotatory stability and is a core component of TTI management.
Question 19
A patient has undergone successful surgical repair of a terrible triad injury, including coronoid fixation, radial head arthroplasty, and LUCL repair. Post-operatively, the elbow is initially immobilized in a posterior splint. In the immediate post-operative protective phase (Weeks 0-6), which of the following rehabilitation principles is most critical for optimizing outcomes while protecting the surgical repairs?
Explanation
Correct Answer: C
The case, under 'Post-Operative Rehabilitation Protocols', emphasizes 'Early Motion: Initiate controlled range of motion as soon as possible to prevent adhesion formation and stiffness.' Specifically, for the Protective Phase (Weeks 0-6): 'Active-assisted and gentle passive ROM: Initiated within the first few days to a week. The brace's range of motion is progressively increased... Forearm Rotation: Gentle pronation/supination within comfort and stability limits, often favoring pronation initially to protect the LUCL.'
Option A (aggressive passive ROM into full extension) is incorrect as it risks stressing the LUCL repair and causing instability. Option B (immediate full weight-bearing and strengthening) is too aggressive and would jeopardize the repairs. Option D (complete immobilization for 6 weeks) is incorrect as it would lead to severe stiffness, which is a common complication. Option E (MUA at 2 weeks) is a treatment for acute stiffness, not a routine part of immediate post-operative rehabilitation.
Question 20
A patient is 3 months post-operative from a terrible triad repair. They complain of persistent elbow stiffness and a palpable, painful mass around the elbow. Radiographs confirm the presence of mature heterotopic ossification (HO) that is functionally limiting. Which of the following is the most appropriate management strategy for this patient's heterotopic ossification, and what prophylactic measure could have been considered immediately post-operatively?
Explanation
Correct Answer: B
The case, under 'Complications & Management' for Heterotopic Ossification (HO), states: 'Prophylaxis: Indomethacin (for 3-6 weeks post-op) or radiation therapy (single dose within 24-72 hours). Salvage Strategies: Surgical excision after maturation (typically 6-12 months post-onset) if functionally limiting.' Since the HO is mature and functionally limiting, surgical excision is a consideration, but it's important to ensure full maturation and to have considered prophylaxis.
Option A (immediate surgical excision) is incorrect because excision should ideally occur after maturation (typically 6-12 months post-onset) to minimize recurrence. Option C (radiation therapy as primary treatment for mature HO) is incorrect; radiation is primarily a prophylactic measure, not a treatment for mature, functionally limiting HO. Option D (MUA) is for stiffness, but not specifically for breaking up mature HO. Option E (total elbow arthroplasty) is a salvage procedure for end-stage arthritis, not the primary treatment for HO.
Question 21
A surgeon is reviewing the literature on terrible triad injuries. The case mentions that the need for Medial Collateral Ligament (MCL) repair in TTI is debated, as it is typically spared in the primary injury. According to the provided case material, under what specific circumstance would an acute repair of the MCL typically be indicated in a terrible triad injury?
Explanation
Correct Answer: B
The case, under 'Medial Collateral Ligament (MCL) Assessment', states: 'Though less commonly injured primarily in TTI, the MCL should be dynamically stressed after the lateral structures are stabilized. If gross valgus instability persists after LUCL, coronoid, and radial head stabilization, an acute repair of the MCL (typically the anterior bundle) is indicated.' This highlights the specific intra-operative finding that would necessitate MCL repair.
Option A is incorrect because the MCL is on the medial side and would not be visualized during a standard lateral approach. Option C (prophylactic repair) is not supported by the case, which states its role is debated. Option D (chronic instability) would be a delayed presentation, whereas the question asks about acute repair. Option E (coronoid fracture involving the sublime tubercle) is important because the sublime tubercle is the attachment site for the MCL, and its fracture can compromise MCL stability. However, the case specifies that MCL repair is indicated if gross valgus instability persists after addressing all other components, implying a dynamic assessment of overall stability, not just the presence of a specific fracture pattern.
Question 22
A 38-year-old male presents after a 10-foot fall onto both feet, experiencing severe bilateral heel pain and inability to bear weight. Initial assessment reveals significant swelling, ecchymosis, and a negative 'wrinkle test' on the left hindfoot. Given the high-energy axial load mechanism, which of the following associated injuries is most critical to actively screen for during the initial evaluation?
Explanation
Correct Answer: C
The mechanism of injury (high-energy axial load, fall from height) that causes calcaneal fractures is also associated with other significant injuries, particularly to the spine. The case explicitly states, 'specific inquiry was made regarding other potential injuries, especially those associated with high-energy axial loading. This included symptoms referable to the lumbar spine, which is crucial given the incidence of concomitant spinal fractures (up to 10-15% in calcaneal fractures).' Therefore, a lumbar spine fracture is the most critical associated injury to screen for due to its potential for neurological compromise and the high incidence rate. While other options like talar fractures, pilon fractures, and contralateral calcaneal fractures are important to consider in the differential for hindfoot trauma, the lumbar spine carries a higher risk of severe systemic implications and is specifically highlighted in the case as a crucial consideration for this mechanism.
Question 23
The patient's clinical examination revealed tense, shiny skin over the lateral aspect of the left heel, and the 'wrinkle test' was negative. This finding has which of the following implications for the immediate surgical management of his displaced intra-articular calcaneal fracture?
Explanation
Correct Answer: C
The case explicitly states, 'The 'wrinkle test' was negative on the left side, meaning the skin could not be pinched into fine wrinkles, signifying that the swelling had exceeded the elastic capacity of the dermis. Proceeding with an extensile lateral approach in the presence of a negative wrinkle test carries an unacceptably high risk of postoperative wound dehiscence.' This finding is a critical indicator of severe soft tissue compromise due to edema. Therefore, surgery must be delayed until the swelling has subsided and the wrinkle test becomes positive, typically 10 to 21 days post-injury, to minimize the risk of devastating wound complications. While compartment syndrome is a concern with high-energy injuries, a negative wrinkle test primarily relates to skin viability for surgical incision, not directly to compartment pressures. It does not confirm adequate soft tissue for immediate surgery; rather, it contraindicates it.
Question 24
Initial plain radiographs of the left calcaneus demonstrated a Bohler's angle of 5 degrees (normal 20-40 degrees) and Gissane's angle of 140 degrees (normal 100-120 degrees). These specific radiographic findings are most indicative of which of the following?
Explanation
Correct Answer: C
The case states that a Bohler's angle of 5 degrees (significantly decreased from the normal 20-40 degrees) is 'indicative of substantial collapse of the posterior facet and loss of calcaneal height.' Concurrently, an increased Gissane's angle to 140 degrees (normal 100-120 degrees) reflects 'the disruption of the lateral process of the talus and the primary fracture line.' Both angles are critical indicators of displaced intra-articular calcaneal fractures. A decreased Bohler's angle signifies loss of calcaneal height and posterior facet depression, while an increased Gissane's angle indicates disruption of the lateral process of the talus, which acts as a wedge in the injury mechanism. These findings are pathognomonic for significant intra-articular involvement and collapse, not normal morphology, extra-articular fractures, or isolated sustentacular injuries.
Question 25
Based on the provided case description and the typical coronal CT appearance for a Sanders Type IIIBC calcaneal fracture, which of the following best describes the articular fragments of the posterior facet?
Explanation
Correct Answer: B
The case explicitly states, 'The CT analysis of the left calcaneus revealed a highly comminuted posterior facet. The coronal cuts demonstrated three distinct articular fragments with fracture lines located centrally and laterally within the posterior facet, consistent with a Sanders Type IIIBC classification.' The Sanders classification system, based on coronal CT cuts, divides the posterior facet into three potential fracture lines (A, B, and C). A Type III fracture indicates three-part articular fractures (two fracture lines) with a centrally depressed fragment. Specifically, IIIBC means there are fracture lines centrally (B) and laterally (C), resulting in three distinct articular fragments (medial, central, and lateral). The image provided is a coronal CT, which is the plane used for Sanders classification, visually supporting the concept of multiple fragments.
Question 26
The sagittal CT cuts of the patient's calcaneal fracture confirmed a 'tongue-type variant.' This specific classification, based on the Essex-Lopresti system, implies which of the following about the fracture morphology?
Explanation
Correct Answer: C
The case clearly defines the Essex-Lopresti classification: 'Our patient exhibits a tongue-type variant. This distinction is critical for reduction maneuvers. In a tongue-type fracture, the entire posterior facet and tuberosity unit can often be manipulated via a Schanz pin placed percutaneously into the posterior tuberosity (the Essex-Lopresti maneuver). Plantarflexion of the pin elevates the posterior facet, while varus/valgus manipulation corrects the coronal alignment.' It further clarifies: 'The sagittal cuts confirmed a tongue-type variant where the secondary fracture line exited posteriorly through the tuberosity, rather than superiorly just behind the posterior facet (which would indicate a joint depression type).' Therefore, a tongue-type fracture is characterized by the secondary fracture line exiting posteriorly through the calcaneal tuberosity, meaning the posterior facet remains attached to the posterior tuberosity fragment.
Question 27
The patient has a 15 pack-year smoking history and works as a construction worker. Considering the landmark Buckley trial (JBJS 2002) and the principles highlighted in the case regarding operative management of displaced intra-articular calcaneal fractures, which of the following statements is most accurate?
Explanation
Correct Answer: C
The case explicitly discusses the impact of smoking: 'His 15 pack-year smoking history is a critical prognostic factor... In the context of calcaneal fractures, smoking significantly increases the risk of devastating postoperative wound complications, including marginal flap necrosis, deep infection, and subsequent osteomyelitis. Studies, notably the landmark trial by Buckley et al., have demonstrated that smokers with displaced intra-articular calcaneal fractures often have poorer outcomes following operative intervention compared to non-smokers, making the decision to proceed with open reduction and internal fixation (ORIF) highly nuanced in this demographic.' The Buckley trial specifically showed that while young, healthy, non-smokers had better outcomes with surgery, smokers had outcomes that were not significantly different from, or were worse than, those managed non-operatively, along with a drastically higher rate of wound complications. Therefore, smoking significantly increases complication risks and can negate the benefits of surgery.
Question 28
During the surgical intervention for this Sanders IIIBC calcaneal fracture, an extensile lateral approach is utilized. To minimize the risk of postoperative marginal flap necrosis, the surgeon employs a 'no-touch' technique and uses three 1.6 mm K-wires driven into the lateral talus, talar neck, and cuboid to retract the full-thickness flap. This specific K-wire retraction technique primarily serves which of the following purposes?
Explanation
Correct Answer: D
The case details the meticulous soft tissue handling: 'To retract the flap without causing crush injury to the microvasculature, self-retaining retractors are strictly avoided. Instead, three 1.6 mm Kirschner wires (K-wires) are driven into the lateral talus, the talar neck, and the cuboid. The full-thickness flap is then gently retracted superiorly and held in place by bending the K-wires over the soft tissue. This technique eliminates continuous point pressure on the flap edges, significantly reducing the risk of postoperative marginal necrosis.' The primary goal of this specific K-wire retraction method is to protect the delicate soft tissue flap and its microcirculation, which is particularly vulnerable in smokers and in the presence of significant swelling.
Question 29
Following surgical exposure via the extensile lateral approach for this Sanders Type IIIBC tongue-type calcaneal fracture, a logical, step-wise reduction sequence is crucial. What is the most appropriate initial step in the fracture reduction sequence?
Explanation
Correct Answer: D
The case outlines the fracture reduction sequence: 'The reduction of a highly comminuted Sanders IIIBC fracture must follow a logical, step-wise progression, working from the known (the constant fragment) to the unknown (the displaced lateral fragments).' The first step listed is: '1. Tuberosity Reduction: A 5.0 mm Schanz pin is inserted percutaneously from posterior to anterior into the dense bone of the calcaneal tuberosity fragment. Using this pin as a joystick, axial traction is applied to restore calcaneal length. The tuberosity is then translated medially and rotated out of varus to restore the mechanical axis of the hindfoot.' This initial step establishes calcaneal length and corrects the varus deformity, providing a stable base before addressing the articular fragments.
Question 30
In the definitive internal fixation of this Sanders IIIBC calcaneal fracture, a low-profile, anatomically contoured calcaneal perimeter plate is utilized. The case emphasizes the critical importance of strategic screw placement. Which of the following screw placements is described as most critical for securing the lateral construct to the constant medial fragment?
Explanation
Correct Answer: C
The case highlights the importance of sustentacular screws: 'The most critical screws are placed through the plate, just inferior to the posterior facet, directed from lateral to medial into the dense bone of the sustentaculum tali. These screws (typically 3.5 mm cortical or locking screws) secure the lateral construct to the constant medial fragment. Absolute care must be taken to ensure these screws are of appropriate length; over-penetration medially can tether the flexor hallucis longus (FHL) tendon or injure the posterior tibial neurovascular bundle.' These screws are crucial because the sustentaculum tali is part of the 'constant' fragment, which remains attached to the talus, providing a stable anchor for the reconstructed lateral calcaneus.
Question 31
A patient presents to the emergency department with severe hindfoot pain, swelling, and inability to bear weight after a high-energy fall. While a calcaneal fracture is a strong consideration, the differential diagnosis for axial load injuries to the hindfoot is broad. Which of the following clinical findings would most strongly suggest a subtalar dislocation as the primary diagnosis, rather than an isolated calcaneal fracture?
Explanation
Correct Answer: C
The differential diagnosis table in the case provides key differentiating features. For subtalar dislocation, the 'Key Clinical Findings' are 'Gross deformity of the hindfoot (medial or lateral shift), skin tenting, locked joint.' In contrast, intra-articular calcaneal fractures typically present with a 'widened heel, decreased height, Mondor's sign, varus tuberosity.' While Mondor's sign and localized tenderness over the calcaneus are characteristic of calcaneal fractures, and a decreased Bohler's angle is a radiographic hallmark, a gross deformity with skin tenting and a locked joint is a more specific and immediate indicator of a subtalar dislocation, which involves disruption of the talocalcaneal and talonavicular joints.
Question 32
A 35-year-old male sustains a high-energy ankle injury. Plain radiographs demonstrate a highly displaced ankle fracture-dislocation that is irreducible in the emergency department. A subsequent CT scan reveals that the proximal fragment of a distal fibula fracture is trapped behind the posterior tubercle of the distal tibia. What is the most appropriate diagnosis?
Explanation
Question 33
A 60-year-old diabetic smoker presents with a tongue-type calcaneus fracture. Clinical examination reveals severe posterior heel swelling with distinct blanching of the skin overlying the posterior tuberosity fragment. What is the most appropriate next step in management?
Explanation
Question 34
Surgical management of the 'terrible triad' of the elbow traditionally follows a specific sequence to sequentially restore stability. After addressing the coronoid and radial head fractures, what is the next most critical ligamentous structure to repair?
Explanation
Question 35
A 40-year-old female presents with a highly comminuted radial head fracture and significant distal radioulnar joint (DRUJ) pain following a fall. If this injury is incorrectly managed with isolated radial head excision, what is the most likely long-term complication?
Explanation
Question 36
During the evaluation of an ankle syndesmotic injury, it is important to understand the biomechanical contributions of the syndesmotic ligaments. Which of the following structures provides the greatest resistance to diastasis of the distal tibiofibular joint?
Explanation
Question 37
A patient with an intra-articular calcaneus fracture is undergoing preoperative planning. Which imaging modality and specific slice view is standardly used to determine the Sanders classification?
Explanation
Question 38
A 25-year-old male sustains an elbow dislocation. A post-reduction CT scan demonstrates an isolated fracture of the anteromedial facet of the coronoid process. What specific ligamentous injury is pathognomonic for this fracture pattern?
Explanation
Question 39
Six weeks following open reduction and internal fixation of a talar neck fracture, a subchondral radiolucent band is visualized in the talar dome on the AP mortise radiograph. What does this radiographic finding indicate?
Explanation
Question 40
During an extensile lateral approach for a calcaneus fracture, a full-thickness subperiosteal flap is elevated. If the inferior and proximal limb of the incision is carried too far posteriorly, which of the following structures is at greatest risk of iatrogenic injury?
Explanation
Question 41
A patient presents with a capitellum fracture classified as a Dubberley type 3B. What defining characteristic of this specific fracture type often necessitates structural bone grafting or a posterior approach?
Explanation
Question 42
According to the Lauge-Hansen classification, what is the exact sequence of structures injured in a Pronation-External Rotation (PER) stage IV ankle fracture?
Explanation
Question 43
A 32-year-old female sustains a twisting injury to her foot. Radiographs demonstrate an avulsion fracture of the anterior process of the calcaneus. Tension from which of the following ligaments is the most common cause of this fracture?
Explanation
Question 44
An adult patient undergoes plate fixation for a Bado type II Monteggia fracture (posterior dislocation of the radial head with an apex-posterior ulnar diaphyseal fracture). Intraoperatively, after the ulnar plate is applied, the radial head remains dislocated. What is the most appropriate next step in management?
Explanation
Question 45
A surgeon uses the standard anterolateral approach to the distal tibia for open reduction and internal fixation of a pilon fracture.
This surgical approach utilizes an internervous plane between which two nerves?
Explanation
Question 46
An apex-distal chevron olecranon osteotomy is utilized to expose the articular surface for the fixation of a highly comminuted intra-articular distal humerus fracture. What is the most common complication associated specifically with this osteotomy?
Explanation
Question 47
During open reduction and internal fixation of a calcaneus fracture, screws are placed from lateral to medial into the sustentaculum tali. If these screws are excessively long and penetrate the inferior cortex of the sustentaculum, which tendon is at direct risk of tethering or injury?
Explanation
Question 48
A 45-year-old male falls from a height and sustains a displaced intra-articular calcaneus fracture. During an extensile lateral approach, the surgeon elevates a full-thickness subperiosteal flap. Which of the following vascular structures is the primary blood supply to this lateral soft tissue flap and must be meticulously protected?
Explanation
Question 49
A 38-year-old female presents with a 'terrible triad' injury of the elbow consisting of a dislocation, a comminuted radial head fracture, and a type II coronoid fracture. Following closed reduction, the joint remains unstable. What is the most appropriate biomechanical sequence of surgical reconstruction?
Explanation
Question 50
A 22-year-old male sustains a high-energy ankle fracture-dislocation that is irreducible in the emergency department. A post-reduction attempt CT scan shows the proximal fibular fragment entrapped posterior to the posterolateral ridge of the distal tibia. What is the most likely diagnosis?
Explanation
Question 51
A 55-year-old diabetic patient sustains a tongue-type calcaneus fracture. Clinical examination reveals profound swelling and distinct blanching of the skin directly over the posterior heel. What is the most appropriate initial management?
Explanation
Question 52
A 62-year-old female undergoes open reduction and internal fixation of a comminuted distal humerus fracture utilizing a chevron olecranon osteotomy. Which of the following complications is uniquely associated with this specific approach compared to triceps-sparing approaches?
Explanation
Question 53
According to the Lauge-Hansen classification, what is the precise sequential order of ligamentous and osseous injury in a Supination-External Rotation (SER) stage IV ankle fracture?
Explanation
Question 54
A 40-year-old female presents with a Dubberley type 3B capitellum fracture, characterized by capitellar and trochlear involvement with severe posterior condylar comminution. What is the optimal fixation strategy via a lateral approach?
Explanation
Question 55
A 45-year-old male falls from a ladder and sustains a displaced, intra-articular calcaneus fracture. He undergoes open reduction and internal fixation via a standard extensile lateral approach. Which of the following is the most frequently encountered complication specific to this surgical approach?
Explanation
Question 56
A 35-year-old female presents with a 'terrible triad' injury of the elbow after a fall onto an outstretched hand.
If surgical intervention is undertaken using a standard lateral approach, what is the generally recommended sequence of reconstruction?
Explanation
Question 57
A 25-year-old male sustains a twisting injury to his ankle. Radiographs show a widened medial clear space but no fracture of the lateral malleolus. Full-length tibia-fibula films reveal a proximal third fibula fracture (Maisonneuve injury). Disruption of which of the following structures is primarily responsible for the lateral talar shift and widening of the medial clear space?
Explanation
Question 58
When evaluating a lateral radiograph of the foot for a suspected calcaneus fracture, Böhler's angle is measured.
Which of the following correctly describes the anatomical landmarks used to draw the two intersecting lines for this angle?
Explanation
Question 59
A 40-year-old female sustains a fall onto an outstretched hand resulting in a capitellum fracture. Radiographic evaluation and subsequent surgical exploration classify the injury as a Kocher-Lorenz (Type II) fracture. Which of the following best describes this specific fracture type?
Explanation
Question 60
A 32-year-old male is brought to the emergency department after a severe ankle twisting injury. Closed reduction is unsuccessful, and the ankle remains rigidly dislocated. Radiographs demonstrate that the proximal fibular fragment is entrapped behind the posterior tubercle of the distal tibia. What is the eponym for this specific fracture-dislocation?
Explanation
Question 61
Which imaging modality and specific plane of view are required to properly classify intra-articular calcaneus fractures according to the Sanders classification system?
Explanation
Question 62
A 6-year-old boy sustains a Bado Type III Monteggia fracture (lateral or anterolateral dislocation of the radial head with a proximal ulnar fracture). Which nerve is at the highest risk of injury in this specific Bado subtype?
Explanation
Question 63
A 45-year-old male sustains a high-energy pilon fracture. The extremity exhibits massive soft tissue swelling and multiple hemorrhagic fracture blisters. A spanning external fixator is placed. What is the most widely accepted clinical indicator that the soft tissues are ready for definitive open reduction and internal fixation?
Explanation
Question 64
During percutaneous fixation of a calcaneus fracture, a surgeon directs a screw from lateral to medial into the sustentaculum tali. If this screw is excessively long and breaches the medial cortex of the sustentaculum, which anatomical structure is at greatest risk of being injured or tethered?
Explanation
Question 65
A 40-year-old female sustains a Mason Type II radial head fracture. On examination in the emergency department, she has a reproducible mechanical block to forearm rotation despite aspiration of the hematoma and intra-articular local anesthetic injection. What is the most appropriate management?
Explanation
Question 66
A 45-year-old female falls on an outstretched hand and sustains a 'terrible triad' injury of the elbow. Radiographs and CT demonstrate a posterior elbow dislocation, a comminuted radial head fracture, and a Regan-Morrey Type II coronoid fracture. During surgical reconstruction, what is the most widely accepted sequence of fixation to reliably restore elbow stability?
Explanation
Question 67
A 35-year-old male undergoes open reduction and internal fixation of a displaced intra-articular calcaneus fracture utilizing an extensile lateral approach. To minimize the risk of full-thickness apex wound necrosis, the 'no-touch' subperiosteal flap must be elevated off the lateral wall to protect which of the following primary vascular structures?
Explanation
Question 68
A 25-year-old male sustains an ankle injury during a rugby match. Radiographs reveal an irreducible fracture-dislocation.
Intraoperatively, closed reduction maneuvers fail completely. What is the primary anatomic block to reduction in this specific injury pattern?
Explanation
Question 69
A 60-year-old female sustains an AO/OTA 13-C3 comminuted intra-articular distal humerus fracture. An olecranon osteotomy is utilized to gain optimal articular visualization. Which of the following is the most common complication specifically associated with the olecranon osteotomy approach?
Explanation
Question 70
A 45-year-old male smoker presents to the emergency department after a fall from a ladder. Examination reveals significant swelling and severe blanching of the skin over the posterior heel. Radiographs demonstrate a displaced tongue-type calcaneus fracture. What is the most appropriate definitive management to prevent catastrophic soft tissue failure?
Explanation
Question 71
A 30-year-old male undergoes internal fixation of a pronation-external rotation ankle fracture. After fibular plating, the surgeon performs a Cotton test and suspects syndesmotic instability. When using intraoperative fluoroscopy, which parameter on the mortise view is the most reliable indicator of syndesmotic malreduction compared to the uninjured contralateral ankle?
Explanation
Question 72
A 22-year-old gymnast presents with acute elbow pain after a fall. CT imaging reveals a coronal shear fracture of the capitellum extending into the medial trochlea, consistent with a Dubberley Type 3A fracture.
Based on the medial extension, what surgical approach is most appropriate for adequate visualization and fixation?
Explanation
Question 73
A 50-year-old female with poorly controlled diabetes presents with a high-energy pilon fracture (AO/OTA 43-C). The soft tissues are severely swollen with extensive fracture blisters. The decision is made to place a temporizing joint-spanning external fixator. At what anatomical location should the proximal pins ideally be placed?
Explanation
Question 74
A 40-year-old male sustains a closed intra-articular calcaneus fracture after a fall.
The Sanders classification is used to guide treatment. Which specific imaging view and anatomical landmark does this classification system primarily evaluate?
Explanation
None
