Master ABOS Orthopedic Board Review: Musculoskeletal Pathology & Bone Disorders | Part 12
20 Jun 2026
54 min read
46 Views

Key Takeaway
This ABOS Orthopedic Board Review covers essential musculoskeletal pathology, including Camurati-Engelmann disease, multiple myeloma, Ewing's sarcoma, Paget's disease, hemophilia arthropathy, algodystrophy, stress fractures, and various arthropathies. It focuses on clinical presentation, radiographic findings, and pathological features for comprehensive exam preparation.
Master ABOS Orthopedic Board Review: Musculoskeletal Pathology & Bone Disorders | Part 12
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
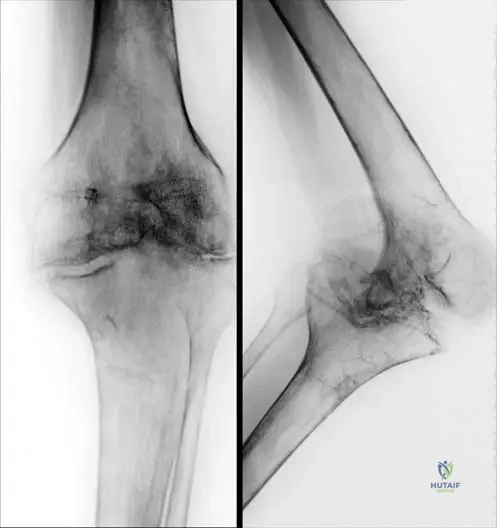
A 55-year-old female presents with severe, burning pain, swelling, and skin color changes in her right hand 6 weeks after sustaining a distal radius fracture treated in a cast. Radiographs reveal the findings shown.
According to current evidence, which of the following interventions initiated at the time of injury could have significantly reduced the risk of developing this condition?
According to current evidence, which of the following interventions initiated at the time of injury could have significantly reduced the risk of developing this condition?
Explanation
The clinical and radiographic presentation (patchy osteopenia/Sudeck's atrophy) is classic for Complex Regional Pain Syndrome (CRPS). High-quality evidence demonstrates that Vitamin C (500 mg daily for 50 days) significantly reduces the incidence of CRPS after distal radius fractures.
Question 2
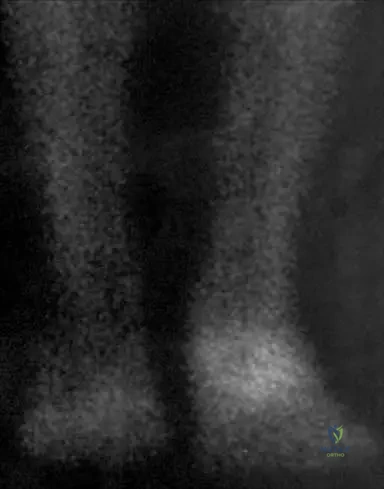
A 65-year-old man presents with worsening back pain and fatigue. Laboratory studies show hypercalcemia, anemia, and elevated creatinine. Radiographs show multiple "punched-out" lytic lesions in the skull and vertebral bodies.
Which of the following is required to establish the definitive diagnosis of this patient's most likely condition?
Which of the following is required to establish the definitive diagnosis of this patient's most likely condition?
Explanation
Multiple myeloma requires a bone marrow biopsy demonstrating >10% clonal plasma cells for definitive diagnosis, along with end-organ damage (CRAB criteria) or a myeloma-defining event. While serum and urine tests are supportive, tissue confirmation is essential.
Question 3
A 10-year-old boy presents with severe leg pain, waddling gait, and progressive weakness. Radiographs demonstrate bilateral symmetrical cortical thickening of the diaphyseal regions of the femurs and tibias, sparing the epiphyses and metaphyses.
Which of the following genetic mutations is responsible for this condition?
Which of the following genetic mutations is responsible for this condition?

Explanation
This is Camurati-Engelmann disease (Progressive Diaphyseal Dysplasia), characterized by diaphyseal cortical thickening. It is caused by an autosomal dominant mutation in the TGFB1 gene, leading to increased bone formation.
Question 4
A 72-year-old man with progressive bowing of his right tibia and hearing loss presents for evaluation. Radiographs demonstrate cortical thickening, trabecular coarsening, and an advancing V-shaped osteolytic lesion in the tibia. You recommend treatment with a bisphosphonate. What is the precise mechanism of action of nitrogen-containing bisphosphonates in this disease?
Explanation
Nitrogen-containing bisphosphonates (like alendronate and zoledronic acid) treat Paget's disease by inhibiting farnesyl pyrophosphate synthase in the mevalonate pathway. This prevents prenylation of small GTPases, leading to osteoclast apoptosis.
Question 5
A 45-year-old woman with a history of celiac disease presents with diffuse bone pain and proximal muscle weakness. Laboratory results reveal low serum calcium, low phosphorus, elevated alkaline phosphatase, and elevated parathyroid hormone. Radiographs show bilateral transverse radiolucencies in the femoral necks. What is the fundamental histopathologic defect in this condition?
Explanation
The clinical picture describes osteomalacia secondary to malabsorption, presenting with Looser zones (pseudofractures). The histopathologic hallmark of osteomalacia is an accumulation of unmineralized osteoid due to defective mineralization.
Question 6
A 50-year-old patient with end-stage renal disease on dialysis presents with severe bone pain. Radiographs of the spine demonstrate sclerotic bands at the superior and inferior endplates of the vertebral bodies, creating a "rugger-jersey" appearance. Which of the following best describes the primary driving pathophysiology of this skeletal finding?
Explanation
The "rugger-jersey" spine is classic for renal osteodystrophy. The diseased kidneys fail to convert 25-OH Vitamin D to 1,25-OH Vitamin D, leading to hypocalcemia and severe secondary hyperparathyroidism.
Question 7
A 65-year-old man presents with severe back pain and fatigue. Radiographs show multiple punched-out lytic lesions in the skull and spine.
Serum protein electrophoresis demonstrates a prominent M-spike. Which of the following is the most likely histological finding upon bone marrow biopsy?
Serum protein electrophoresis demonstrates a prominent M-spike. Which of the following is the most likely histological finding upon bone marrow biopsy?
Explanation
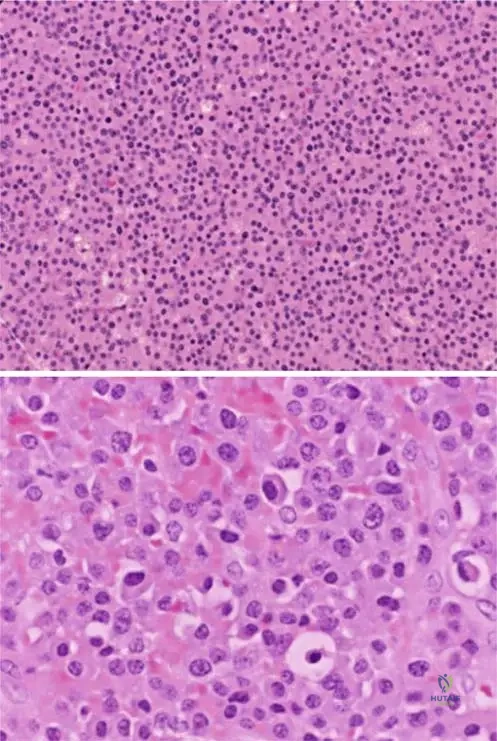
Multiple myeloma is characterized by the neoplastic proliferation of plasma cells in the bone marrow. Histology typically reveals sheets of atypical plasma cells with eccentric nuclei and a perinuclear halo (clock-face chromatin).
Question 8
A 55-year-old woman is 6 weeks post-closed reduction and casting of a distal radius fracture. She presents with severe burning pain, hypersensitivity, and erythema of the hand.
Which of the following radiographic findings is most characteristic of her condition?
Which of the following radiographic findings is most characteristic of her condition?
Explanation
Complex Regional Pain Syndrome (CRPS), formerly known as Sudeck's atrophy or algodystrophy, is characterized by patchy periarticular osteopenia on radiographs. This results from localized rapid bone turnover associated with vasomotor instability.
Question 9
A 7-year-old boy presents with severe leg pain, easy fatigability, and a waddling gait. Radiographs reveal bilateral, symmetric cortical thickening of the long bone diaphyses.
This condition is most commonly associated with a mutation in which of the following genes?
This condition is most commonly associated with a mutation in which of the following genes?
Explanation
Camurati-Engelmann disease (progressive diaphyseal dysplasia) is an autosomal dominant disorder caused by a mutation in the TGFB1 gene. It leads to marked cortical thickening of the diaphyses of long bones and presents with bone pain and muscle weakness.
Question 10
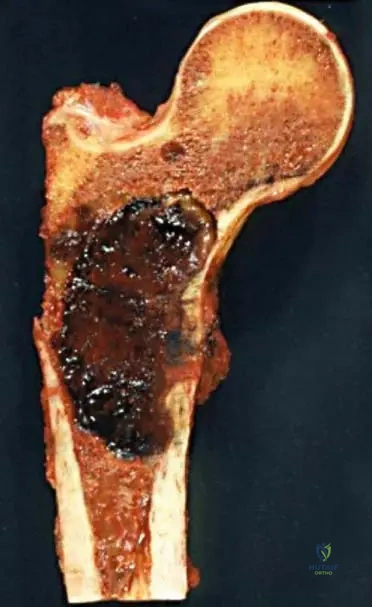
A 70-year-old female is diagnosed with multiple myeloma after presenting with hypercalcemia and a pathologic femur fracture.
Which of the following imaging modalities is most appropriate for staging her overall skeletal tumor burden?
Which of the following imaging modalities is most appropriate for staging her overall skeletal tumor burden?
Explanation
Whole-body low-dose CT or PET/CT is the gold standard for staging skeletal lesions in multiple myeloma. Technetium-99m bone scans rely on osteoblastic activity and are often falsely negative in multiple myeloma due to its purely osteolytic nature.
Question 11
A 42-year-old male develops early complex regional pain syndrome (CRPS) in his right foot following a minor crush injury.
What is the most effective initial management strategy for this condition?
What is the most effective initial management strategy for this condition?

Explanation
The cornerstone of early management in CRPS is functional restoration through early active mobilization and physical therapy. While medications may be adjunctive, strict immobilization actively worsens the condition.
Question 12
A 14-year-old boy presents with right thigh pain and swelling. Radiographs reveal a destructive diaphyseal lesion in the femur with a prominent "onion-skin" periosteal reaction. Biopsy shows small round blue cells. Which chromosomal translocation is most characteristic of this tumor?
Explanation
Ewing sarcoma typically presents as a diaphyseal lesion in children with an "onion-skin" periosteal reaction. The t(11;22)(q24;q12) translocation creates the EWS-FLI1 fusion protein and is found in the vast majority of cases.
Question 13
A 16-year-old girl is diagnosed with high-grade osteosarcoma of the distal femur. She completes neoadjuvant chemotherapy and undergoes wide surgical resection. What is the most important prognostic factor for her long-term survival?
Explanation
In high-grade osteosarcoma, the degree of tumor necrosis (>90% is considered a good response) following neoadjuvant chemotherapy is the single most important prognostic indicator for long-term survival.
Question 14
A 32-year-old woman presents with wrist pain. Radiographs show an expansile, eccentrically located lytic lesion extending into the epiphysis of the distal radius. Biopsy confirms a Giant Cell Tumor of bone. If medical therapy is considered for an unresectable lesion, which of the following agents is most appropriate?
Explanation
Giant Cell Tumors of bone express RANK ligand (RANKL) on the neoplastic stromal cells, which recruits multinucleated osteoclast-like giant cells. Denosumab, a monoclonal antibody against RANKL, is an effective targeted medical therapy for these tumors.
Question 15
A 72-year-old man presents with deep, aching bone pain in his lower legs and notes an increase in his hat size. Laboratory tests show a markedly elevated serum alkaline phosphatase with normal calcium and phosphorus levels. The primary pathogenesis of this disorder is driven by abnormalities in which cell type?
Explanation
Paget's disease is initiated by an intense, focal increase in osteoclastic bone resorption, followed by disorganized and excessive osteoblastic bone formation. The primary defect lies in the overactive and enlarged osteoclasts.
Question 16
A 19-year-old male presents with painful scoliosis and back pain that is poorly relieved by NSAIDs. Imaging reveals a 2.5 cm radiolucent lesion in the posterior elements of L3 with a mineralized center. What is the most likely diagnosis?
Explanation
The presentation of a painful, bone-forming lesion in the posterior spinal elements is typical for osteoblastoma or osteoid osteoma. A size greater than 2.0 cm generally distinguishes an osteoblastoma from an osteoid osteoma, and the pain is often less responsive to NSAIDs.
Question 17
A 65-year-old man presents with severe lower back pain and fatigue. Radiographs reveal diffuse osteopenia and multiple punched-out lytic lesions in the skull and spine.
Which of the following is the most likely cause of false-negative technetium-99m bone scans in this condition?
Which of the following is the most likely cause of false-negative technetium-99m bone scans in this condition?
Explanation
Multiple myeloma lesions are purely lytic and characteristically lack reactive osteoblastic activity due to the secretion of factors like Dkk-1 by myeloma cells, which inhibits osteoblasts. Thus, technetium-99m bone scans, which rely on osteoblastic activity for tracer uptake, are often false-negative.
Question 18
A 9-year-old boy presents with severe leg pain, a waddling gait, and delayed puberty. Radiographs show bilateral, symmetric cortical thickening of the diaphyseal regions of the femur and tibia.
Which genetic mutation is characteristic of this condition?
Which genetic mutation is characteristic of this condition?
Explanation
Progressive diaphyseal dysplasia (Camurati-Engelmann disease) is an autosomal dominant disorder caused by mutations in the TGFB1 gene. It is characterized by cortical thickening of the long bone diaphyses, bone pain, and muscle weakness.
Question 19
A 55-year-old woman is 6 weeks post-operative from a distal radius fracture open reduction and internal fixation. She presents with severe, burning pain, allodynia, skin color changes, and edema in the affected hand.
According to the Budapest Criteria, which of the following is an absolute requirement to make the diagnosis?
According to the Budapest Criteria, which of the following is an absolute requirement to make the diagnosis?
Explanation
The Budapest Criteria for Complex Regional Pain Syndrome (CRPS) strictly require the presence of continuing pain that is disproportionate to any inciting event. Objective tests like bone scans and sympathetic blocks can support the diagnosis but are not required criteria.
Question 20
Regarding the clinical scenario of Complex Regional Pain Syndrome (Sudeck's atrophy) following a distal radius fracture, which of the following prophylactic therapies has been shown in clinical trials to reduce its incidence?
Explanation
Daily supplementation with 500 mg of Vitamin C for 50 days following a distal radius fracture has been shown in prospective randomized trials to significantly reduce the risk of developing CRPS.
Question 21
A 62-year-old female presents with hypercalcemia, anemia, and acute renal failure. A skeletal survey reveals multiple osteolytic lesions.
Which of the following describes the characteristic histological finding of the primary neoplastic cells in this disease?
Which of the following describes the characteristic histological finding of the primary neoplastic cells in this disease?

Explanation
Multiple myeloma is characterized by the malignant proliferation of plasma cells in the bone marrow. These cells typically display eccentric, 'clock-face' nuclei and a prominent perinuclear halo representing the Golgi apparatus.
Question 22
A 32-year-old woman presents with progressive knee pain. Imaging reveals an eccentric, purely lytic lesion in the distal femoral epiphysis extending into the metaphysis. Biopsy confirms Giant Cell Tumor of bone. What is the mechanism of action of the targeted medical therapy most commonly used for unresectable cases?
Explanation
Denosumab is a monoclonal antibody that binds RANK-L, preventing its interaction with RANK receptors. In Giant Cell Tumor, the neoplastic mononuclear cells overexpress RANK-L, which drives the recruitment of the destructive, reactive osteoclast-like giant cells.
Question 23
A 68-year-old man presents with severe back pain and fatigue. Radiographs demonstrate diffuse osteopenia and multiple punched-out lytic lesions in the skull and vertebral bodies.
Which of the following is the most sensitive test to establish the diagnosis?
Which of the following is the most sensitive test to establish the diagnosis?
Explanation
Serum and urine protein electrophoresis (SPEP/UPEP) with immunofixation are the most sensitive initial tests for Multiple Myeloma, detecting monoclonal proteins. Bone scintigraphy is often cold (negative) because myeloma suppresses osteoblast activity.
Question 24
A 12-year-old boy presents with a waddling gait, severe leg pain, and easy fatigability. Radiographs reveal bilateral, symmetric, fusiform cortical thickening of the femoral and tibial diaphyses, sparing the metaphyses and epiphyses.
What is the genetic basis of this disorder?
What is the genetic basis of this disorder?
Explanation
Progressive diaphyseal dysplasia (Camurati-Engelmann disease) is an autosomal dominant condition caused by mutations in the TGFB1 gene. It presents with progressive diaphyseal cortical thickening, leg pain, and proximal muscle weakness.
Question 25
A 55-year-old woman is 6 weeks post-closed reduction and casting of a distal radius fracture. She reports agonizing, burning pain in her hand, out of proportion to her injury. Examination shows a swollen, erythematous, and diaphoretic hand with restricted finger motion.
Which of the following prophylactic measures has been shown to reduce the incidence of this condition following distal radius fractures?
Which of the following prophylactic measures has been shown to reduce the incidence of this condition following distal radius fractures?
Explanation
Vitamin C (500 mg daily for 50 days) has been shown in some studies to significantly decrease the risk of developing Complex Regional Pain Syndrome (CRPS) following distal radius fractures. CRPS is characterized by autonomic dysfunction, hyperalgesia, and spotty osteopenia.
Question 26
A 32-year-old woman presents with knee pain. Radiographs show an eccentric, expansile, lytic lesion in the distal femur extending to the subchondral bone. Histology reveals multinucleated giant cells in a background of mononuclear stromal cells. Which of the following best describes the role of the giant cells in this tumor?
Explanation
In Giant Cell Tumor of bone, the mononuclear stromal cells are the actual neoplastic cells and harbor the H3F3A mutation. These neoplastic cells secrete RANKL, which recruits and activates the reactive, non-neoplastic multinucleated giant cells (osteoclasts).
Question 27
A 15-year-old boy presents with a rapidly enlarging mass over his proximal tibia. MRI demonstrates an eccentric metaphyseal lesion with multiple fluid-fluid levels. Biopsy confirms an aneurysmal bone cyst (ABC). What is the most common cytogenetic abnormality associated with primary ABC?
Explanation
Primary aneurysmal bone cysts are true neoplasms driven by a USP6 gene rearrangement on chromosome 17p13. Fluid-fluid levels are characteristic on MRI due to blood products separating by density.
Question 28
A 60-year-old woman is diagnosed with multiple myeloma. Her skeletal survey shows punched-out lytic lesions.
Which of the following statements explains the mechanism of bone destruction in this disease process?
Which of the following statements explains the mechanism of bone destruction in this disease process?
Explanation
Myeloma cells interact with bone marrow stromal cells, leading to increased production of RANKL and decreased production of OPG. This severe imbalance results in massive osteoclast activation and the characteristic lytic bone lesions.
Question 29
A patient with suspected Complex Regional Pain Syndrome (CRPS) undergoes a three-phase bone scan.
Which finding on the bone scan is most classic for established CRPS?
Which finding on the bone scan is most classic for established CRPS?

Explanation
The classic finding of CRPS on a three-phase technetium bone scan is increased periarticular uptake in the delayed (third) phase. The first two phases (flow and blood pool) may also show asymmetry depending on the stage of the disease.
Question 30
A 14-year-old boy presents with a painful mass near his knee. Radiographs reveal a metaphyseal lesion with a sunburst pattern of periosteal reaction and a Codman triangle. A biopsy confirms conventional osteosarcoma. What is the standard treatment protocol for this patient?
Explanation
The standard of care for conventional high-grade osteosarcoma is neoadjuvant chemotherapy, followed by wide surgical resection (limb-salvage or amputation), and completed with adjuvant chemotherapy. Radiation therapy is typically not utilized as osteosarcoma is relatively radioresistant.
Question 31
A 65-year-old male presents with deep bone pain in his lower back and ribs. Laboratory results show hypercalcemia and normocytic anemia. Radiographs reveal multiple "punched-out" lytic lesions in the skull and axial skeleton.
Which of the following is the most appropriate initial diagnostic test to confirm the underlying etiology?
Which of the following is the most appropriate initial diagnostic test to confirm the underlying etiology?
Explanation
The clinical presentation and "punched-out" lytic lesions are classic for Multiple Myeloma. SPEP and UPEP are the most appropriate initial tests, revealing a monoclonal spike (M-protein) in the majority of patients. It is the most common primary bone malignancy in adults.
Question 32
A 55-year-old female sustains a distal radius fracture treated with open reduction and internal fixation. To prevent the development of the condition shown in the clinical image below, what pharmacological prophylaxis should be initiated?
Explanation
The image demonstrates trophic skin changes and swelling consistent with Complex Regional Pain Syndrome (CRPS). Studies have shown that Vitamin C (500 mg daily for 50 days) significantly reduces the incidence of CRPS following distal radius fractures. Other medications listed are used for treatment, not proven primary prophylaxis.
Question 33
A 9-year-old boy presents with severe leg pain, waddling gait, and bilateral muscle weakness. Radiographs demonstrate symmetrical cortical thickening of the diaphyses of the femurs and tibias with sparing of the epiphyses.
A mutation in which of the following genes is most likely responsible for this condition?
A mutation in which of the following genes is most likely responsible for this condition?
Explanation
This presentation is characteristic of Camurati-Engelmann disease (progressive diaphyseal dysplasia). It is an autosomal dominant disorder caused by a mutation in the TGFB1 gene on chromosome 19. The mutation leads to increased osteoblastic activity resulting in cortical thickening.
Question 34
A 60-year-old female with known multiple myeloma presents with thigh pain. Radiographs reveal a purely lytic lesion in the subtrochanteric femur occupying 50% of the cortical diameter. She describes moderate pain with weight-bearing. Using the Mirels' criteria, what is the appropriate management?
Explanation
The Mirels' score for this lesion is 10: Site (lower limb = 3), Pain (moderate = 2), Lesion type (lytic = 3), Size (1/3 to 2/3 = 2). A score of 9 or greater indicates impending fracture and warrants prophylactic internal fixation, typically followed by radiotherapy.
Question 35
Which of the following clinical tools is considered the gold standard for diagnosing Complex Regional Pain Syndrome (CRPS)?
Explanation
The diagnosis of CRPS is primarily clinical, utilizing the Budapest Criteria. These criteria require the patient to report at least one symptom in three of four categories (sensory, vasomotor, sudomotor/edema, motor/trophic) and display at least one sign in two of the same categories. Imaging can support the diagnosis but is not the gold standard.
Question 36
A 12-year-old boy with known Camurati-Engelmann disease is experiencing debilitating bilateral thigh pain and a severely abnormal gait. Which of the following is considered the mainstay of medical treatment to relieve his symptoms?
Explanation
Systemic corticosteroids are the medical treatment of choice for Camurati-Engelmann disease. They are highly effective in relieving bone pain, improving muscle weakness, and sometimes normalizing gait and radiographic appearances. Bisphosphonates have shown conflicting results and can sometimes worsen the condition.
Question 37
In patients with Multiple Myeloma, the characteristic severe osteolytic bone lesions are primarily caused by which of the following mechanisms?
Explanation
Myeloma cells induce uncoupled bone remodeling favoring profound osteoclastogenesis. This occurs primarily through the secretion of factors that upregulate RANKL (Receptor Activator of Nuclear factor Kappa-B Ligand) and downregulate osteoprotegerin (OPG), leading to uninhibited osteoclast activity.
Question 38
A 45-year-old male presents with polyneuropathy, organomegaly, endocrinopathy, an M-protein spike, and skin changes. Skeletal survey reveals predominantly osteosclerotic bone lesions. What is the most likely diagnosis?
Explanation
POEMS syndrome is a rare paraneoplastic disorder secondary to a plasma cell dyscrasia. The acronym stands for Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal protein, and Skin changes. Unlike classic multiple myeloma, the bone lesions in POEMS syndrome are predominantly osteosclerotic.
Question 39
A 50-year-old patient is diagnosed with a solitary plasmacytoma of the L2 vertebral body. Systemic workup, including bone marrow biopsy and skeletal survey, is negative. What is the standard definitive treatment for this isolated lesion?
Explanation
The standard of care for a solitary plasmacytoma of bone is definitive local radiotherapy, as these lesions are highly radiosensitive. Surgery is reserved for structural instability or rapid neurological deterioration. Lifelong monitoring is required due to a high rate of progression to multiple myeloma.
Question 40
A 42-year-old female presents with severe, burning pain, allodynia, and swelling of her right hand 6 weeks following a casted distal radius fracture. If a three-phase technetium-99m bone scan is ordered, what is the classic finding indicative of her suspected diagnosis?
Explanation
The diagnosis is Complex Regional Pain Syndrome (CRPS). The classic finding on a three-phase bone scan for CRPS is diffuse, increased periarticular uptake in the affected limb during the delayed (third) phase. The initial blood flow and blood pool phases may also show asymmetric flow.
Question 41
A patient with multiple myeloma develops progressive acute kidney injury. Which of the following is the most common pathophysiologic cause of renal failure in these patients?
Explanation
Cast nephropathy (myeloma kidney) is the most common cause of renal failure in multiple myeloma. It is caused by the precipitation of monoclonal free light chains (Bence Jones proteins) with Tamm-Horsfall proteins in the distal convoluted tubules, forming obstructing casts. This leads to tubular damage and obstruction.
Question 42
Which radiographic finding is most characteristic of advanced Sudeck's atrophy (Complex Regional Pain Syndrome) in the hand and wrist?

Explanation
Sudeck's atrophy (CRPS) classically manifests radiographically as patchy, periarticular demineralization (osteopenia) due to localized hyperemia and disuse. Subperiosteal resorption is seen in hyperparathyroidism, while acro-osteolysis is associated with scleroderma or hyperparathyroidism.
Question 43
A 68-year-old male undergoes prophylactic intramedullary nailing for a large, painful lytic lesion in the diaphysis of the femur caused by multiple myeloma. Which of the following is the most appropriate next step in local management?
Explanation
Following prophylactic fixation of an impending pathologic fracture due to multiple myeloma (or metastatic disease), postoperative external beam radiation therapy is required. Radiation provides local tumor control, halts continued bone destruction, and alleviates pain. Healing of the defect requires local tumor eradication.
Question 44
A subset of patients with multiple myeloma may develop Carpal Tunnel Syndrome or macroglossia. This specific clinical presentation is most directly related to which complication of the disease?
Explanation
Primary (AL) amyloidosis is caused by the tissue deposition of misfolded monoclonal immunoglobulin light chains produced by the clonal plasma cells in multiple myeloma. Deposition in the transverse carpal ligament leads to carpal tunnel syndrome, and deposition in the tongue causes macroglossia.
Question 45
A 25-year-old female presents with an asymmetric, painful, sclerotic thickening of her right tibial diaphysis. The condition began after puberty. Biopsy shows normal bone remodeling with no malignant cells. What is the most likely diagnosis?
Explanation
Ribbing disease (multiple diaphyseal sclerosis) presents after puberty with asymmetric, painful diaphyseal sclerosis. This contrasts with Camurati-Engelmann disease, which presents in childhood and is typically symmetric. Both conditions affect the diaphyses but differ in onset and symmetry.
Question 46
When evaluating a patient with newly diagnosed Multiple Myeloma, which imaging modality is historically notorious for yielding falsely negative results when screening for bone lesions?
Explanation
Technetium-99m bone scans rely on osteoblastic activity (bone formation) to show uptake. Multiple myeloma lesions are purely osteolytic, mediated by uncoupled osteoclastic activity with suppressed osteoblastic function. Therefore, bone scans are often falsely negative ("cold") in multiple myeloma.
Question 47
What is the primary cellular abnormality observed in the bone marrow biopsy of a patient with Multiple Myeloma?
Explanation
Multiple myeloma is a clonal proliferation of malignant plasma cells. On histology, these cells have eccentric nuclei, coarse "clock-face" or "cartwheel" chromatin, and a perinuclear halo. Intracytoplasmic inclusions of immunoglobulins (Russell bodies) or Mott cells may also be seen.
Question 48
Complex Regional Pain Syndrome (CRPS) is thought to involve a complex interplay of central and peripheral nervous system abnormalities. Which neuropeptide is most closely associated with the neurogenic inflammation seen in the early phases of CRPS?
Explanation
Neurogenic inflammation in CRPS is mediated by the release of neuropeptides from primary afferent nerve terminals. Substance P and Calcitonin Gene-Related Peptide (CGRP) cause potent vasodilation and protein extravasation, leading to the characteristic edema, warmth, and redness in acute CRPS.
Question 49
A 10-year-old child presents with progressive waddling gait, severe lower extremity pain, and diminished muscle mass. Radiographs reveal symmetric bilateral cortical thickening of the diaphyseal regions of the long bones.
Which portion of the bone remains characteristically uninvolved in this disease?
Which portion of the bone remains characteristically uninvolved in this disease?

Explanation
In Camurati-Engelmann disease (progressive diaphyseal dysplasia), new bone formation occurs on both the endosteal and periosteal surfaces of the diaphysis. The defining radiographic feature is that the epiphyses and metaphyses are characteristically spared.
Question 50
A patient with long-standing Complex Regional Pain Syndrome (CRPS) enters the third (late) stage of the disease. Which clinical features are most characteristic of this stage?
Explanation
CRPS classically progresses through three stages: acute (vasomotor), dystrophic, and atrophic. The third (atrophic) stage is characterized by thin, shiny, and cyanotic skin, severe muscle atrophy, and irreversible joint contractures. The intense pain may spread proximally.
Question 51
A 68-year-old man presents with severe lower back pain and fatigue. Radiographs demonstrate multiple punched-out lytic lesions in his skull and vertebral bodies. Laboratory testing confirms a monoclonal gammopathy.
Which of the following factors secreted by the neoplastic cells is primarily responsible for the suppression of osteoblastic bone formation in this disease?
Which of the following factors secreted by the neoplastic cells is primarily responsible for the suppression of osteoblastic bone formation in this disease?
Explanation
Multiple myeloma cells secrete DKK-1, which inhibits the Wnt/beta-catenin signaling pathway, leading to severe suppression of osteoblast differentiation and activity. While MM cells also stimulate osteoclasts via RANKL up-regulation (driven by IL-6 and MIP-1a), DKK-1 is specifically responsible for the characteristic lack of osteoblastic response (uncoupling) seen in these lytic lesions.
Question 52
A 45-year-old female presents with ongoing severe burning pain, allodynia, and distinct color and temperature asymmetry in her right hand, 8 weeks after closed reduction and casting of a distal radius fracture.
According to the most widely accepted clinical criteria for diagnosing this condition, which of the following is required?
According to the most widely accepted clinical criteria for diagnosing this condition, which of the following is required?
Explanation
The Budapest criteria are the standard for diagnosing Complex Regional Pain Syndrome (CRPS). They require continuing pain disproportionate to the inciting event, at least one symptom in three of four categories (sensory, vasomotor, sudomotor/edema, motor/trophic), and at least one sign in two of the same categories.
Question 53
A 12-year-old boy presents with progressive severe leg pain, easy fatigability, and a waddling gait. Radiographs reveal bilateral symmetrical cortical thickening of the femoral and tibial diaphyses, with sparing of the metaphyses.
What is the most effective medical therapy for achieving symptomatic relief of pain and muscle weakness in this specific condition?
What is the most effective medical therapy for achieving symptomatic relief of pain and muscle weakness in this specific condition?
Explanation
This patient has Camurati-Engelmann disease (progressive diaphyseal dysplasia), caused by a mutation in the TGFB1 gene. Systemic corticosteroids are the mainstay of medical treatment, significantly reducing bone pain, improving muscle weakness, and potentially improving radiographic findings.
Question 54
A 62-year-old man is suspected of having multiple myeloma after routine lab work shows elevated total protein with normal serum albumin. Which of the following imaging modalities is considered the most sensitive for detecting early osteolytic skeletal involvement and extramedullary disease in this patient?
Explanation
Whole-body MRI (and PET/CT) is significantly more sensitive than a plain radiographic skeletal survey for detecting early bone marrow involvement and extramedullary lesions in multiple myeloma. Technetium-99m bone scans are highly insensitive for myeloma because the lesions typically lack an osteoblastic response.
Question 55
A 50-year-old woman develops severe hyperalgesia, swelling, and localized erythema in her foot after a minor crush injury. What pathophysiological mechanism is primarily responsible for the initial warm, erythematous phase of this syndrome?
Explanation
In the early (warm) phase of Complex Regional Pain Syndrome (CRPS), retrograde depolarization of C-fibers leads to the release of neuropeptides like Substance P and calcitonin gene-related peptide (CGRP). This causes marked neurogenic inflammation, vasodilation, and protein extravasation, leading to the characteristic warmth and edema.
Question 56
A 72-year-old man presents with anterior bowing of his tibia and new-onset hearing loss. His serum alkaline phosphatase is markedly elevated, but calcium and phosphorus are normal. What is the primary cellular defect underlying this patient's condition?
Explanation
Paget's disease of bone is characterized by a primary abnormality of the osteoclasts, which are greatly increased in number, abnormally large, and have excessive nuclei (up to 100 per cell). This leads to chaotic and intense osteoclastic bone resorption followed by disorganized osteoblastic bone formation.
Question 57
A 14-year-old girl presents with a Shepherd's crook deformity of her proximal femur and irregularly bordered café-au-lait macules on her trunk. What is the underlying genetic and molecular mechanism of her disease?
Explanation
This patient has McCune-Albright syndrome, a severe form of polyostotic fibrous dysplasia. It is caused by a post-zygotic activating somatic mutation in the GNAS gene, which encodes the alpha subunit of the stimulatory G protein (Gs), resulting in continuous, unregulated production of intracellular cAMP.
Question 58
An infant presents with severe anemia, hepatosplenomegaly, and diffuse sclerosis of all skeletal structures on radiographs, with a lack of medullary canals. Which of the following is the definitive curative treatment for the malignant infantile form of this condition?
Explanation
Malignant infantile osteopetrosis is caused by defective osteoclast function. Because osteoclasts are derived from the hematopoietic macrophage-monocyte lineage, a hematopoietic stem cell transplant can provide normal osteoclast precursors and is considered the only definitive curative treatment.
Question 59
A 45-year-old recent immigrant presents with diffuse bone pain and proximal muscle weakness. Radiographs reveal bilateral pseudofractures (Looser zones) in the femoral neck. Which of the following laboratory profiles is most consistent with this diagnosis?
Explanation
The clinical picture describes osteomalacia, typically due to severe Vitamin D deficiency. This leads to decreased intestinal calcium and phosphorus absorption, resulting in hypocalcemia, secondary hyperparathyroidism (High PTH), renal phosphate wasting (Low Phosphate), and increased bone turnover (High Alkaline Phosphatase).
Question 60
A 65-year-old female with a known history of multiple myeloma presents with increasing pain in her right thigh when walking. Radiographs show a 3.5 cm lytic lesion in the proximal diaphyseal region of the right femur involving 60% of the cortical diameter. Her Mirels score is 10. What is the most appropriate management?
Explanation
A Mirels score of 9 or greater indicates a high risk for impending pathologic fracture. The standard of care for a high-risk diaphyseal impending fracture in multiple myeloma is prophylactic stabilization (e.g., intramedullary nailing) to prevent fracture, followed by postoperative radiation for local tumor control.
Question 61
A 50-year-old female presents with recurrent kidney stones and bone pain. Radiographs show an expansile, multiloculated lytic lesion in her third metacarpal. Biopsy reveals multinucleated giant cells clustered in a highly vascular, fibroblastic stroma with extensive hemosiderin deposition. What is the most appropriate next step in management?
Explanation
The clinical presentation and histology (giant cells, hemosiderin) are highly suggestive of a Brown tumor associated with hyperparathyroidism. The correct next step is to evaluate her serum calcium and PTH levels to confirm the diagnosis, as treatment is directed at correcting the hyperparathyroidism, not primary bone resection.
Question 62
A 70-year-old man is newly diagnosed with multiple myeloma. Which of the following serum markers is considered the most significant independent prognostic factor for survival in this disease?
Explanation
Serum Beta-2 microglobulin is the single most powerful and reliable independent prognostic factor for survival in multiple myeloma. It is used alongside serum albumin to stage the disease according to the International Staging System (ISS).
Question 63
A 55-year-old male with severe Type I CRPS of the right lower extremity has failed to improve after 4 months of intensive physical therapy, oral NSAIDs, and gabapentin. He exhibits pronounced allodynia and hyperhidrosis. What is the most appropriate next step in confirming the diagnosis of sympathetically maintained pain and providing therapeutic relief?
Explanation
For CRPS that is refractory to initial conservative therapy, a regional sympathetic block (such as a lumbar sympathetic block for the lower extremity) is the appropriate next step. It serves both a diagnostic purpose (differentiating sympathetically maintained pain from sympathetically independent pain) and a therapeutic purpose.
Question 64
A 55-year-old man with end-stage renal disease on hemodialysis presents with chronic bone pain. Spine radiographs demonstrate alternating bands of sclerosis and radiolucency parallel to the vertebral endplates (Rugger-Jersey spine). What is the primary driving mechanism of this patient's bone pathology?
Explanation
The patient has renal osteodystrophy (osteitis fibrosa cystica). In chronic kidney disease, failing kidneys cannot excrete phosphate or adequately synthesize active Vitamin D (1,25-OH D). This combination causes hypocalcemia, severely driving secondary hyperparathyroidism and resulting in characteristic bone changes like the Rugger-Jersey spine.
Question 65
A 65-year-old man is incidentally found to have an isolated elevation of serum alkaline phosphatase. Radiographs reveal marked cortical thickening and coarsened trabeculae in his right proximal femur, and he is diagnosed with Paget's disease. He is completely asymptomatic. What is the primary indication to initiate bisphosphonate therapy in this patient?
Explanation
Treatment of asymptomatic Paget's disease is highly indicated when metabolically active disease involves weight-bearing bones (like the femur or tibia), the spine, or areas near major joints. Medical suppression with bisphosphonates helps prevent disease progression, severe bowing deformities, and secondary osteoarthritis.
Question 66
A 30-year-old male is evaluated for a minor knee sprain. Incidentally, plain radiographs reveal multiple small, symmetric, well-defined circular sclerotic foci clustered in the periarticular regions of the distal femur and proximal tibia. He has no prior medical history. Which genetic mutation is most commonly associated with this benign condition?
Explanation
This radiographic appearance is pathognomonic for Osteopoikilosis (spotted bone disease). It is a benign, autosomal dominant sclerosing bone dysplasia caused by a loss-of-function mutation in the LEMD3 gene, which is also associated with Buschke-Ollendorff syndrome.
Question 67
A 68-year-old man presents with severe lower back pain, fatigue, and recent onset of renal impairment. Radiographs demonstrate multiple sharply marginated "punched-out" lytic lesions in the skull and spine.
Which of the following is most commonly detected in the urine of patients with this condition?
Which of the following is most commonly detected in the urine of patients with this condition?
Explanation
Multiple myeloma is characterized by the neoplastic proliferation of plasma cells, which frequently secrete monoclonal immunoglobulin light chains. These free light chains are filtered by the kidneys and can be detected in the urine as Bence Jones proteins.
Question 68
A 45-year-old woman develops severe, burning pain, allodynia, and trophic skin changes in her right hand 8 weeks after sustaining a minimally displaced distal radius fracture treated in a cast.
According to the Budapest criteria, the diagnosis of Complex Regional Pain Syndrome (CRPS) is made. What is the cornerstone of initial management?
According to the Budapest criteria, the diagnosis of Complex Regional Pain Syndrome (CRPS) is made. What is the cornerstone of initial management?
Explanation
The cornerstone of initial management for CRPS is aggressive physical and occupational therapy to maintain range of motion and function. This is typically combined with pharmacological management such as gabapentin, pregabalin, or tricyclic antidepressants.
Question 69
A 12-year-old boy presents with progressive muscle weakness, a waddling gait, and severe, aching leg pain. Radiographs demonstrate marked, symmetrical bilateral cortical thickening of the femoral and tibial diaphyses, sparing the metaphyses and epiphyses.
Which of the following medical treatments has been shown to provide significant symptomatic relief for this condition?
Which of the following medical treatments has been shown to provide significant symptomatic relief for this condition?
Explanation
Progressive diaphyseal dysplasia (Camurati-Engelmann disease) is caused by a mutation in the TGFB1 gene. Corticosteroids (and sometimes NSAIDs like indomethacin) are the mainstay of medical treatment, significantly reducing bone pain and improving muscle strength.
Question 70
A 55-year-old man undergoes a biopsy of a solitary lytic lesion in the T10 vertebral body, which confirms a solitary bone plasmacytoma. A bone marrow biopsy shows less than 5% plasma cells, and a skeletal survey is otherwise negative. What is the approximate probability that this condition will progress to multiple myeloma within 10 years?
Explanation
Solitary bone plasmacytomas have a high rate of progression to systemic multiple myeloma. Studies demonstrate that approximately 85% of patients with a solitary bone plasmacytoma will progress to multiple myeloma within 10 years.
Question 71
A 70-year-old man complains of progressive hearing loss and an increasing hat size. Laboratory studies show a markedly elevated serum alkaline phosphatase with normal serum calcium and phosphorus levels. Histologic examination of a bone biopsy reveals a characteristic "mosaic" pattern of lamellar bone. What is the primary cellular defect in this disease?
Explanation
Paget's disease of bone is primarily a disorder of osteoclasts, which are unusually large, multinucleated, and hyperactive. They characteristically contain viral-like paramyxovirus inclusion bodies, leading to excessive bone resorption followed by disorganized osteoblastic bone formation (mosaic pattern).
Question 72
A 30-year-old woman presents with knee pain. Radiographs reveal an eccentric, lytic lesion in the distal femoral epiphysis extending to the subchondral bone. Biopsy confirms a giant cell tumor of bone. Denosumab therapy is considered for her locally aggressive disease. What is the mechanism of action of this drug?
Explanation
Denosumab is a fully human monoclonal antibody that specifically binds to the Receptor Activator of Nuclear factor Kappa-B Ligand (RANKL). This prevents RANKL from binding to the RANK receptor on the surface of osteoclasts, thereby inhibiting osteoclast formation, function, and survival.
Question 73
A 15-year-old boy presents with shoulder pain after a minor fall. Radiographs show an expansile, eccentric lytic lesion in the proximal humeral metaphysis. Biopsy reveals blood-filled spaces lacking a true endothelial lining, interspersed with fibrous septa containing giant cells. Which genetic translocation is highly specific for this primary lesion?
Explanation
Primary aneurysmal bone cysts (ABCs) are neoplastic processes characterized by recurrent translocations involving the USP6 gene, most commonly t(16;17). This leads to USP6 upregulation, which drives the cystic and expansile growth.
Question 74
An 8-year-old boy presents with acute arm pain after throwing a baseball. Radiographs demonstrate a centrally located, completely lytic lesion in the proximal humeral metaphysis with a subtle "fallen leaf" sign and a pathologic fracture. What is the most appropriate initial management?
Explanation
The patient has a unicameral bone cyst (UBC) that has sustained a pathologic fracture. The best initial management is conservative treatment (sling immobilization) to allow the fracture to heal. Up to 15% of UBCs may resolve spontaneously after a fracture.
Question 75
A 25-year-old woman presents with a Shepherd's crook deformity of the proximal femur. Radiographs display a large intramedullary lesion with a "ground-glass" appearance. She is diagnosed with fibrous dysplasia, which is caused by a somatic activating mutation in the GNAS gene. What is the direct intracellular consequence of this mutation?
Explanation
The GNAS gene encodes the alpha subunit of the stimulatory G protein (Gs). A mutation causes constitutive activation of adenylate cyclase, leading to persistently increased levels of intracellular cyclic AMP (cAMP), which disrupts normal osteoblast differentiation.
Question 76
An 18-year-old male complains of deep, aching pain in his right thigh that is worse at night and dramatically relieved by ibuprofen. Radiographs reveal a 1 cm radiolucent nidus surrounded by intense reactive sclerosis in the femoral diaphysis. What is the most common anatomic location for this type of lesion?
Explanation
The clinical presentation and radiographic findings are classic for an osteoid osteoma. More than 50% of osteoid osteomas occur in the long bones of the lower extremity, with the proximal femur being the most common specific anatomic location.
Question 77
A 50-year-old woman develops Complex Regional Pain Syndrome (CRPS) following a minor crush injury to her foot. Radiographs demonstrate patchy periarticular osteopenia.
In the pathophysiology of CRPS, which neuropeptide released from C-fiber terminals is primarily responsible for mediating the localized neurogenic inflammation?
In the pathophysiology of CRPS, which neuropeptide released from C-fiber terminals is primarily responsible for mediating the localized neurogenic inflammation?
Explanation
CRPS involves exaggerated neurogenic inflammation driven by the release of neuropeptides, particularly Substance P and calcitonin gene-related peptide (CGRP), from the peripheral terminals of nociceptive C-fibers. This causes vasodilation and protein extravasation.
Question 78
A 15-year-old boy presents with progressive, worsening pain and swelling around his knee. Radiographs reveal a destructive lesion in the distal femoral metaphysis with a "sunburst" periosteal reaction and a Codman triangle. Biopsy confirms conventional high-grade osteosarcoma. What is the current standard of care for this patient?
Explanation
The standard of care for conventional high-grade osteosarcoma consists of multiagent neoadjuvant chemotherapy, followed by definitive limb-sparing wide surgical resection, and concluding with adjuvant chemotherapy. Osteosarcoma is generally radioresistant.
Question 79
A 12-year-old boy presents with fever, weight loss, and severe pain in his leg. Radiographs reveal a permeative, destructive lesion in the tibial diaphysis with a multi-layered "onion-skin" periosteal reaction. Cytogenetics demonstrate a t(11;22) translocation. Which immunohistochemical marker is characteristically strongly positive in this tumor?
Explanation
The diagnosis is Ewing sarcoma, characterized by the t(11;22) translocation forming the EWS-FLI1 fusion protein. Immunohistochemically, Ewing sarcoma cells typically display strong, diffuse membranous staining for CD99 (also known as MIC2).
Question 80
A 10-year-old asymptomatic boy has a knee radiograph taken after a minor contusion. The imaging reveals an incidental eccentric, lobulated, bubbly radiolucent lesion with a well-defined sclerotic margin located in the distal femoral metaphysis, measuring 2 cm in length. What is the most appropriate management?
Explanation
The radiographic appearance is classic for a non-ossifying fibroma (NOF). Since the lesion is small, asymptomatic, and does not pose a significant risk of fracture, the best management is observation and reassurance, as these lesions spontaneously ossify and resolve during skeletal maturity.
Question 81
A 60-year-old man presents with a painful, destructive, lytic lesion in his proximal femur. He has a history of a nephrectomy for clear cell renal carcinoma 3 years ago. The lesion is judged to be at high risk for an impending pathologic fracture, and prophylactic intramedullary nailing is planned. What preoperative intervention is highly recommended to minimize surgical morbidity?
Explanation
Metastatic renal cell carcinoma and thyroid carcinoma lesions are notoriously hypervascular. Preoperative transarterial embolization of the lesion is highly recommended within 24 to 48 hours prior to surgical fixation to minimize massive intraoperative blood loss.
Question 82
A 7-year-old boy presents with mid-back pain. Radiographs reveal the complete collapse of the T8 vertebral body, appearing as a thin dense line ("vertebra plana"), with adjacent discs maintained. Biopsy reveals cells containing tennis-racket-shaped Birbeck granules on electron microscopy. Which immunohistochemical stain is classically positive in this disease?
Explanation
The diagnosis is Langerhans Cell Histiocytosis (Eosinophilic Granuloma). The pathological Langerhans cells characteristically express CD1a and S-100 on immunohistochemistry, and feature distinctive Birbeck granules on electron microscopy.
Question 83
A 55-year-old man presents with a 6-month history of dull shoulder pain. Radiographs show a large lytic lesion in the proximal humerus with intralesional "popcorn" and "ring-and-arc" calcifications. MRI demonstrates endosteal scalloping involving more than 2/3 of the cortical thickness. Biopsy confirms conventional grade II chondrosarcoma. What is the mainstay of treatment?
Explanation
Conventional intermediate to high-grade (Grade II/III) chondrosarcomas are generally resistant to both chemotherapy and radiation. Therefore, the gold standard of treatment is wide surgical resection with negative margins to prevent local recurrence.
Question 84
A 65-year-old woman presents with isolated right hip pain. Radiographs demonstrate a single 5 cm lytic lesion in the right ilium.
A biopsy confirms monoclonal plasma cells. Comprehensive staging, including a bone marrow biopsy, reveals less than 5% clonal plasma cells elsewhere, and no end-organ damage. What is the preferred primary treatment for this condition?
A biopsy confirms monoclonal plasma cells. Comprehensive staging, including a bone marrow biopsy, reveals less than 5% clonal plasma cells elsewhere, and no end-organ damage. What is the preferred primary treatment for this condition?
Explanation
The diagnosis is a solitary bone plasmacytoma. Because plasma cells are highly radiosensitive, the primary treatment of choice for a solitary bone plasmacytoma is definitive local external beam radiation therapy, which offers excellent local control.
Question 85
A 14-year-old boy with a family history of multiple bony protuberances presents with painless bumps around his knees and shoulders. Radiographs show multiple pedunculated and sessile bone lesions pointing away from the joint lines, with cortex continuous with the host bone. Genetic testing reveals a mutation in the EXT1 gene. What is the normal function of the protein encoded by this gene?
Explanation
Multiple Hereditary Exostoses (Osteochondromatosis) is caused by autosomal dominant mutations in the EXT1 or EXT2 genes. These genes encode glycosyltransferases essential for the biosynthesis of heparan sulfate proteoglycans, which are critical for normal physeal signaling.
Question 86
A 3-year-old boy presents with painless anterior bowing of the tibia. Radiographs demonstrate multiple intracortical osteolytic lesions in the anterior tibial diaphysis. Biopsy reveals a bland fibroblastic stroma with spicules of woven bone rimmed by active osteoblasts. This specific condition is closely related to, and can occasionally be a precursor for, which of the following malignant tumors?
Explanation
The clinical presentation and histology are characteristic of osteofibrous dysplasia (Campanacci disease). This condition almost exclusively affects the tibia and is considered closely related to adamantinoma, a low-grade malignant tumor that can sometimes develop from or coexist with these lesions.
Question 87
A 68-year-old male presents with a pathologic proximal femur fracture. Workup reveals monoclonal gammopathy and Bence-Jones proteinuria. Bone marrow biopsy confirms the diagnosis.
What is the primary cellular mechanism driving the distinct osteolytic lesions seen in this disease process?
What is the primary cellular mechanism driving the distinct osteolytic lesions seen in this disease process?
Explanation
Myeloma cells secrete factors like MIP-1 alpha and IL-6 that upregulate RANKL and downregulate OPG. This leads to profound osteoclast activation and the classic punched-out osteolytic lesions.
Question 88
A 42-year-old female presents 3 months post-carpal tunnel release with severe burning pain, allodynia, asymmetric sweating, and decreased ROM in her digits.
According to the Budapest criteria, which additional clinical sign must be present to establish a clinical diagnosis of Complex Regional Pain Syndrome (CRPS)?
According to the Budapest criteria, which additional clinical sign must be present to establish a clinical diagnosis of Complex Regional Pain Syndrome (CRPS)?
Explanation
The Budapest criteria require at least one symptom in three of four categories: sensory, vasomotor, sudomotor/edema, and motor/trophic. She currently lacks documentation of vasomotor changes to meet the clinical diagnostic threshold.
Question 89
A 12-year-old girl is evaluated for severe, agonizing pain in both legs and extreme fatigue. Radiographs show pronounced cortical thickening of the bilateral femoral and tibial diaphyses, with sparing of the metaphyses.
Genetic testing confirms a mutation in the TGFB1 gene. Which of the following medical therapies has been shown to be most consistently effective for alleviating her bone pain and muscle weakness?
Genetic testing confirms a mutation in the TGFB1 gene. Which of the following medical therapies has been shown to be most consistently effective for alleviating her bone pain and muscle weakness?
Explanation
Systemic corticosteroids are the mainstay of medical treatment for symptomatic Camurati-Engelmann disease. They effectively relieve bone pain, improve muscle strength, and can sometimes reverse radiographic changes.
Question 90
A 60-year-old woman with a known history of multiple myeloma presents with progressive thigh pain with weight-bearing. Radiographs show a 3.5 cm lytic lesion in the peritrochanteric region of the femur involving greater than 50% of the cortical diameter.
What is her Mirels score, and what is the most appropriate management?
What is her Mirels score, and what is the most appropriate management?
Explanation
The Mirels score is 11 (Site: Lower extremity = 2, Pain: Functional = 3, Lesion: Lytic = 3, Size: >2/3 cortical diameter = 3). A score greater than or equal to 9 indicates a high risk of fracture, warranting prophylactic internal fixation.
Question 91
A 35-year-old man undergoes an open reduction and internal fixation of a distal radius fracture. Postoperatively, he develops severe, burning pain, edema, and trophic skin changes in the affected hand.
EMG and nerve conduction studies reveal a distinct, partial injury to the median nerve. Which of the following best classifies this patient's condition?
EMG and nerve conduction studies reveal a distinct, partial injury to the median nerve. Which of the following best classifies this patient's condition?
Explanation
CRPS Type II (formerly known as causalgia) is distinguished from CRPS Type I by the presence of a distinct, identifiable peripheral nerve injury. Type I occurs without a definable nerve lesion.
Question 92
A 70-year-old male with new-onset back pain is diagnosed with multiple myeloma after radiographs demonstrate diffuse osteopenia and punched-out lytic lesions in his lumbar spine.
Which of the following laboratory values is considered the most significant independent prognostic indicator for overall survival in this patient?
Which of the following laboratory values is considered the most significant independent prognostic indicator for overall survival in this patient?
Explanation
Serum beta-2 microglobulin reflects both tumor burden and renal function. It is widely considered the most powerful independent prognostic factor for survival in multiple myeloma.
Question 93
A 9-year-old boy presents with an awkward, waddling gait and generalized muscle weakness. Plain radiographs of the lower extremities are obtained.
If this patient has Camurati-Engelmann disease, which of the following best describes the expected pattern of bone involvement?
If this patient has Camurati-Engelmann disease, which of the following best describes the expected pattern of bone involvement?
Explanation
Camurati-Engelmann disease (Progressive Diaphyseal Dysplasia) is characterized by bilateral, symmetrical cortical thickening of the long bone diaphyses. It classically spares the metaphyses and epiphyses.
Question 94
A 48-year-old female with CRPS Type I of the right lower extremity has failed extensive conservative management, including physical therapy, neuropathic pain medications, and multiple sympathetic nerve blocks.
Her pain remains debilitating and prevents her from participating in rehabilitation. What is the next most appropriate evidence-based intervention?
Her pain remains debilitating and prevents her from participating in rehabilitation. What is the next most appropriate evidence-based intervention?
Explanation
In patients with severe CRPS who are refractory to conservative treatment and sympathetic blocks, spinal cord stimulation is highly effective. It improves pain relief and functional outcomes in treatment-resistant cases.
Question 95
A 62-year-old male presents with acute kidney injury, hypercalcemia, and a lytic lesion in his right humerus. Serum protein electrophoresis shows a monoclonal spike. A diagnosis of multiple myeloma is suspected.
What is the most common underlying mechanism for renal failure in this patient population?
What is the most common underlying mechanism for renal failure in this patient population?
Explanation
The most common cause of renal failure in multiple myeloma is "myeloma kidney" (cast nephropathy). This results from the precipitation of toxic monoclonal free light chains (Bence-Jones proteins) in the distal tubules.
Question 96
A 50-year-old male presents with isolated back pain. Imaging demonstrates a single osteolytic lesion in the L3 vertebral body. Biopsy confirms a monoclonal proliferation of plasma cells, but bone marrow aspirate shows only 2% plasma cells. Whole-body MRI reveals no other skeletal lesions. What is the most appropriate initial treatment for this patient?
Explanation
The patient has a Solitary Plasmacytoma of Bone (SPB). The standard of care is localized external beam radiation therapy, which is highly effective and often locally curative, although many patients eventually progress to multiple myeloma.
None
Previous ChapterABOS Orthopedic Board Review: Paget's Disease, Gout, Hyperp…
Next Chapter ABOS Orthopedic Board Review: Bone Tumors, Alcohol-Related …

Medically Verified Content by
Prof. Dr. Mohammed Hutaif Clinic
Consultant Orthopedic & Spine Surgeon