ABOS Part I Orthopedic Spine Review: Scoliosis, Disc Pathology & Radiculopathy Management | Part 22165

Key Takeaway
This orthopedic spine review covers critical concepts in spinal deformities and disc pathologies. It details scoliosis types (idiopathic, congenital, neuromuscular), diagnosis, progression, and treatment strategies. Additionally, it addresses lumbar and cervical disc prolapse, radiculopathy, Cauda Equina Syndrome, and their management, essential for ABOS Part I preparation.
ABOS Part I Orthopedic Spine Review: Scoliosis, Disc Pathology & Radiculopathy Management | Part 22165
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
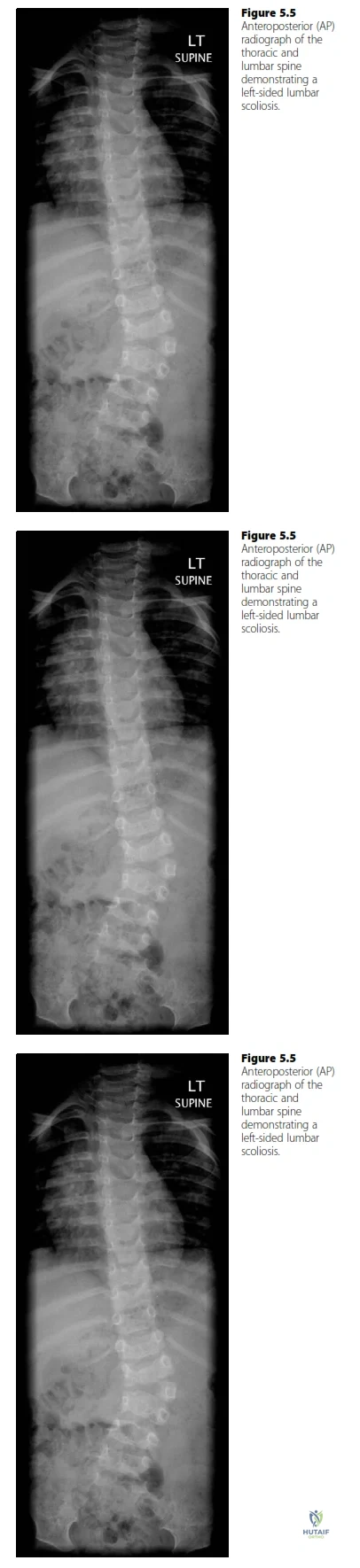
A 12-year-old patient presents with the spinal deformity shown in the radiograph. The examiner identifies a left-sided lumbar scoliosis attributed to a hemivertebra. Which of the following statements regarding the classification and characteristics of this type of scoliosis is most accurate?
Explanation
Correct Answer: C
The radiograph clearly shows a hemivertebra in the lumbar spine, which is a congenital vertebral anomaly. The case explicitly states, 'The radiograph shows a congenital scoliosis. There is a hemivertebra within the lumbar spine producing the scoliosis.' Congenital scoliosis is characterized by vertebral abnormalities present at birth, and the resulting spinal curvature (scoliosis) develops as these abnormal vertebrae grow. This aligns perfectly with the image and case description.
Option A is incorrect because idiopathic scoliosis, while the most common type (70%), has no identifiable cause and typically presents as a right thoracic curve in adolescents. The image shows a clear structural anomaly (hemivertebra) and a left lumbar curve, ruling out idiopathic.
Option B is incorrect because neuromuscular scoliosis arises from a lack of spinal support due to neuromuscular conditions (e.g., cerebral palsy, Duchenne muscular dystrophy) and typically presents as a long, collapsing 'C' shaped curve. The image shows a localized, angular deformity due to a specific vertebral anomaly, not a generalized collapse.
Option D is incorrect because while congenital scoliosis can be early-onset, the definition of early-onset scoliosis (EOS) is typically before age 7, and infantile idiopathic scoliosis (0-3 years) is the type that often resolves spontaneously (80-90%). The case describes a congenital etiology, not necessarily an infantile idiopathic one, and the prognosis for congenital scoliosis is highly variable depending on the anomaly.
Option E is incorrect because miscellaneous scoliosis is associated with systemic conditions like Marfan's syndrome or neurofibromatosis, which are not indicated by the presence of a hemivertebra alone. The primary etiology here is a congenital vertebral malformation.
Question 2
A 14-year-old female patient with adolescent idiopathic scoliosis (AIS) has a 35-degree right thoracic curve. She is premenarchal and has a Risser sign of 0. Based on the natural history of AIS, which of the following factors is the strongest indicator of a high likelihood of curve progression?
Explanation
Correct Answer: C
The case states that 'The development and progression of scoliosis is related to skeletal growth, typically deteriorating most rapidly during the adolescent growth spurt. Features that indicate an increased likelihood of curve progression are therefore associated with but not limited to immaturity. They are: Young age at onset, Premenarchal status, Physical immaturity, Large curves, Female gender.' Premenarchal status combined with a Risser 0 indicates significant skeletal immaturity, meaning the patient has substantial growth remaining. This period of rapid growth is when curves are most likely to progress rapidly.
Option A is incorrect because while female gender is a risk factor for progression (5.4:1 female to male for curves >20 degrees), skeletal immaturity (premenarchal, Risser 0) is a more direct and stronger predictor of rapid progression due to remaining growth potential.
Option B is incorrect because a 35-degree curve is indeed moderate, and larger curves have a greater potential for progression. However, the rate of progression is most strongly linked to the amount of remaining growth, which is best indicated by skeletal immaturity markers like premenarchal status and Risser 0.
Option D is incorrect because a right thoracic curve is the most common pattern for AIS, but the location itself does not inherently indicate a higher likelihood of progression compared to other factors like skeletal maturity. Atypical curves (e.g., left thoracic) might suggest underlying pathology, but a typical right thoracic curve doesn't predict progression rate.
Option E is incorrect because the absence of severe back pain is a typical feature of AIS and does not indicate a higher likelihood of progression. Severe pain would, in fact, be an 'atypical feature' suggesting possible underlying pathology, not a predictor of progression in typical AIS.
Question 3
A 16-year-old male presents with a progressive thoracolumbar scoliosis measuring 55 degrees Cobb angle. He has completed his growth spurt and has a Risser sign of 5. He reports increasing difficulty with sitting balance and occasional costo-pelvic impingement pain. Which of the following is the most appropriate initial treatment recommendation?
Explanation
Correct Answer: C
The case states that surgery is 'Usually reserved for curves with a magnitude > 50.' This patient has a 55-degree curve, which exceeds this threshold. Furthermore, the patient is experiencing functional problems like difficulty with sitting balance and costo-pelvic impingement, which are common indications for surgery, particularly in neuromuscular scoliosis (though this patient is not explicitly stated to have neuromuscular scoliosis, these are general indications for surgery in severe curves). Even if the patient is skeletally mature, curves over 50 degrees can still progress at approximately 1 degree per year and cause significant functional impairment.
Option A is incorrect because while skeletal maturity (Risser 5) does reduce the rate of progression, a 55-degree curve is considered severe and is typically an indication for surgical intervention, not just observation, especially with functional symptoms. Curves over 50 degrees can continue to progress even after skeletal maturity.
Option B is incorrect because bracing is generally indicated for progressive curves between 25 and 40 degrees in skeletally immature patients to prevent progression. It is not effective for curves over 40-45 degrees or in skeletally mature patients, and certainly not for a 55-degree curve with functional deficits.
Option D is incorrect because while physical therapy can be beneficial for pain management and muscle balance, it does not correct or prevent the progression of structural scoliosis, especially a severe curve of 55 degrees.
Option E is incorrect because while MRI is important for atypical curves (e.g., left thoracic, severe pain, rapid progression, short angular deformities) to rule out intraspinal anomalies, a 55-degree thoracolumbar curve in a male, while somewhat atypical for AIS, is primarily an indication for surgical consideration based on magnitude and symptoms, making surgical evaluation the most immediate and appropriate next step. An MRI might be part of the surgical workup, but the primary recommendation is surgical evaluation.
Question 4
The radiograph shows a congenital scoliosis with a hemivertebra. In the context of congenital scoliosis, which of the following vertebral anomalies carries the worst prognosis for curve progression?
Explanation
Correct Answer: B
The case explicitly states, 'Progression of congenital curves depends on growth potential and whether that growth is balanced. Thus a fully segmented hemivertebra in connection with a contralateral unsegmented bar has the least balanced growth and the worst prognosis.' This combination creates a 'crankshaft' effect, with continuous growth on one side (fully segmented hemivertebra) and no growth on the other (unsegmented bar), leading to severe and rapid progression.
Option A is incorrect because a block vertebra has a benign prognosis, rarely leading to a curve beyond 20 degrees, as stated in the text.
Option C is incorrect because a semi-segmented hemivertebra, while having growth potential, is typically less aggressive than a fully segmented hemivertebra with a contralateral unsegmented bar. A semi-segmented hemivertebra is fused to one adjacent vertebra, limiting growth on that side.
Option D is incorrect because an incarcerated hemivertebra is one that is fully incorporated into the vertebral column, often with minimal growth potential and thus a more benign course compared to a fully segmented hemivertebra.
Option E is incorrect because a wedge vertebra is a partial failure of formation, but its growth potential and prognosis are generally less severe than the combination of a fully segmented hemivertebra and a contralateral unsegmented bar.
Question 5
A 10-year-old patient with severe cerebral palsy presents with a rapidly progressing 'C' shaped thoracolumbar scoliosis. In addition to the spinal deformity, which of the following is a common problem specifically associated with neuromuscular scoliosis that would influence treatment goals?
Explanation
Correct Answer: D
The case lists specific problems associated with neuromuscular scoliosis, including 'Problems with sitting balance causing patients to become hand-dependent sitters, which in turn limits upper limb function.' This is a significant functional concern for patients with neuromuscular conditions like cerebral palsy, directly impacting their quality of life and independence.
Option A is incorrect because severe pain, while a red flag for underlying pathology, is not typically associated with neuromuscular scoliosis in the same way as an osteoid osteoma. Osteoid osteoma is a distinct cause of painful scoliosis, not a common problem associated with neuromuscular scoliosis.
Option B is incorrect because while compensatory curves can develop, the text does not highlight rigid cervical curves as a common problem specifically associated with neuromuscular scoliosis. The primary curve is typically a long, collapsing 'C' shape.
Option C is incorrect because while cardiorespiratory compromise is a significant concern, it is primarily highlighted as a risk in 'early-onset scoliosis' (onset before age 7), where the developing heart and lungs may be affected. While severe neuromuscular curves can eventually impact respiratory function, the text specifically links 'progressive cardiorespiratory compromise' to early-onset scoliosis, not neuromuscular scoliosis as its primary unique complication in the same context.
Option E is incorrect because neuromuscular scoliosis, particularly in severe cerebral palsy, is known for its progressive nature and rarely resolves spontaneously. Spontaneous resolution is more characteristic of infantile idiopathic scoliosis.
Question 6
An 18-month-old infant is diagnosed with an infantile idiopathic scoliosis measuring 28 degrees. The curve is progressive. Based on the case information, what is the most appropriate initial non-surgical management strategy for this patient?
Explanation
Correct Answer: D
The case states under 'Early-onset scoliosis' that 'Patients that present with an idiopathic scoliosis below the age of 3 (infantile scoliosis) have the most heterogeneous prognosis... Treatment is problematic and prolonged. The most common forms of treatment are serial plaster jackets (localizer casts), subsequently bracing and eventually growing rods.'
Option A is incorrect because immediate surgical fusion, especially with growing rods, is typically reserved for curves that fail to respond to conservative measures or are extremely severe and progressive, not as an initial treatment for an 18-month-old with a 28-degree curve, even if progressive. Growing rods are a later stage treatment.
Option B is incorrect because while a significant number of infantile curves (80-90%) can resolve, the question states the curve is progressive. For progressive curves, active intervention is needed, not just observation. The text specifically mentions treatment for those that 'do not resolve'.
Option C is incorrect because while bracing is a treatment option, the text specifically lists 'serial plaster jackets (localizer casts)' as the most common initial form of treatment for infantile idiopathic scoliosis, followed by bracing.
Option E is incorrect because physical therapy alone is not an effective treatment for correcting or preventing the progression of structural scoliosis in an infant.
Question 7
During the physical examination of a 13-year-old girl suspected of having scoliosis, the Adam's forward bend test is performed. What is the primary purpose of this test in the assessment of spinal deformity?
Explanation
Correct Answer: D
The Adam's forward bend test is a clinical maneuver used to assess for rotational deformity of the trunk, which is a key component of scoliosis. When a patient bends forward, a structural scoliosis will typically manifest as a prominence on one side of the back (a rib hump in thoracic curves or a lumbar prominence in lumbar curves) due to vertebral rotation. The case lists 'Adam's forward bend test' under 'Examination – key features', implying its role in assessing the curve's characteristics.
Option A is incorrect because skeletal maturity is assessed using factors like age, menarcheal status, height, and radiographically with Risser's sign, not the Adam's forward bend test.
Option B is incorrect because intraspinal anomalies are detected through neurological examination (e.g., abnormal abdominal reflexes) and confirmed with MRI scanning, not the Adam's forward bend test.
Option C is incorrect because the Cobb angle is a radiographic measurement used to quantify the magnitude of the curve on plain X-rays, not a clinical assessment tool like the Adam's test.
Option E is incorrect because while spinal flexibility is assessed during the examination, the Adam's forward bend test primarily highlights the structural nature of the curve and its rotational component, rather than directly quantifying flexibility. Flexibility is often assessed with lateral bending radiographs.
Question 8
A 10-year-old girl with a newly diagnosed scoliosis undergoes a full-length standing AP radiograph of her spine. The radiograph reveals a Risser sign of 2. What does this finding primarily indicate?
Explanation
Correct Answer: C
The case explicitly states under 'Investigations' that 'Risser’s sign grades the progression of development and fusion of the iliac apophysis, is visible on plain X-rays and is a useful indication of maturity.' A Risser sign of 2 indicates that the iliac apophysis has ossified approximately 25-50% from lateral to medial, signifying that the patient is still skeletally immature and has significant growth remaining. This is a critical factor in predicting curve progression.
Option A is incorrect because the severity of the spinal curvature is measured by the Cobb angle, not the Risser sign.
Option B is incorrect because intraspinal anomalies are detected by MRI scanning, not the Risser sign.
Option D is incorrect because the flexibility of the curve is assessed clinically (e.g., with lateral bending) and radiographically with lateral bending X-rays, not by the Risser sign.
Option E is incorrect because the Risser sign indicates skeletal maturity, not the etiology of the scoliosis. The etiology is determined by clinical history, examination, and specific radiographic findings (like a hemivertebra for congenital scoliosis).
Question 9
A 15-year-old boy presents with a 30-degree left thoracic scoliosis, severe localized back pain, and abnormal abdominal reflexes. His family history is negative for scoliosis. Based on the case information, which of these findings is considered an 'atypical feature' that warrants further investigation beyond standard scoliosis workup?
Explanation
Correct Answer: C
The case states under 'Pattern recognition' that 'Atypical features indicate possible underlying pathology (e.g. left-sided curves, severe pain, rapid progression and short angular deformities.)' Additionally, under 'Neurological examination', it notes that 'abnormal abdominal reflexes are most commonly associated with intraspinal anomalies.' Therefore, the combination of a left thoracic curve, severe pain, and abnormal abdominal reflexes are all significant atypical features strongly suggesting an underlying intraspinal anomaly or other pathology, necessitating further investigation such as an MRI.
Option A is incorrect because a 30-degree curve is moderate, but the magnitude itself is not an atypical feature that suggests underlying pathology. It's the combination of other factors that makes it atypical.
Option B is incorrect because while AIS is more prevalent in females (5.4:1 for curves >20 degrees), male gender alone is not considered an 'atypical feature' indicating underlying pathology in the same way as a left-sided curve or severe pain. It simply means it's less common for males to develop AIS.
Option D is incorrect because adolescent onset (10-maturity) is the most common age group for idiopathic scoliosis, so this is a typical, not atypical, feature.
Option E is incorrect because while there is a genetic tendency for scoliosis (20% have an affected family member), the absence of a family history does not rule out idiopathic scoliosis and is not considered an 'atypical feature' indicating underlying pathology.
Question 10
The examiner describes the thoraco-abdominal (Hodgson's) approach for excising a hemivertebra. During this procedure, after incising the skin and fat, serratus anterior, external oblique, and latissimus dorsi, and removing the 10th rib subperiosteally, what is the critical next anatomical step to gain access to the retroperitoneum?
Explanation
Correct Answer: C
The case explicitly describes the Hodgson's approach: 'A key step in this procedure is splitting the costal cartilage to enter the retroperitoneum.' This step allows access to the retroperitoneal space where the spine is located, without entering the peritoneal cavity directly.
Option A is incorrect because ligation of segmental vessels occurs later, after the retroperitoneum is accessed and the discs are excised, to prepare for vertebral excision.
Option B is incorrect because the parietal pleura is incised before splitting the costal cartilage, exposing the lung and diaphragm. The question asks for the step after these initial muscle and rib excisions, specifically to enter the retroperitoneum.
Option D is incorrect because excision of the discs above and below the hemivertebra occurs after the retroperitoneum is accessed and the diaphragm is divided, as part of the vertebral excision process.
Option E is incorrect because sweeping away retroperitoneal fascia with swabs occurs after entering the retroperitoneum, to clear the surgical field and expose the vertebral column.
Question 11
A 37-year-old male presents to your clinic with a 3-week history of worsening low back pain radiating down his left leg. He describes the leg pain as burning, associated with numbness and tingling in his posterior calf and lateral foot. He denies any recent trauma. During your initial assessment, which of the following findings would be the most critical red flag to specifically rule out a serious spinal pathology like Cauda Equina Syndrome?
Explanation
Correct Answer: D
The case explicitly lists the characteristics of Cauda Equina Syndrome (CES) as urinary retention, faecal incontinence, saddle area numbness, loss of anal tone, and widespread neurological signs. These are considered red flags indicating a surgical emergency. While options A, B, C, and E are all consistent with a lumbar disc prolapse causing radiculopathy (specifically S1 in this case), they do not represent the acute, severe neurological compromise that defines CES. Early detection and intervention for CES are crucial for improving outcomes, making these symptoms the most critical to identify during the initial assessment.
Question 12
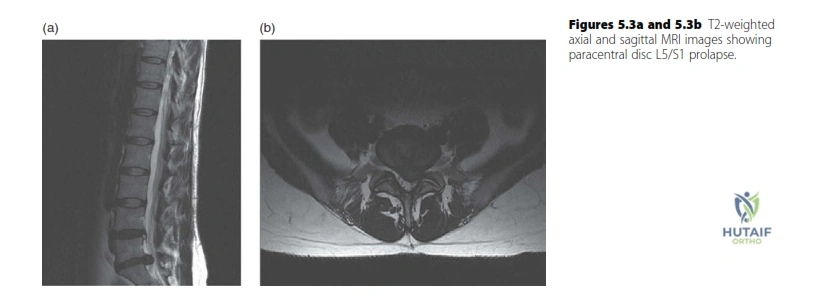
A 37-year-old male presents with back and left lower limb pain. An MRI scan is requested. Review the provided T2-weighted MRI images of the lumbar spine.
Based on the findings shown in the MRI, which nerve root is most likely compressed by the paracentral disc prolapse at the L5/S1 level?
Explanation
Correct Answer: C
The case states that the MRI shows a paracentral disc prolapse at the L5/S1 level. It further clarifies that for a lumbar disc prolapse, the 'traversing' nerve root is most commonly compressed by a common 'paracentral' disc prolapse. In the context of an L5/S1 disc prolapse, the S1 nerve root is the traversing nerve root at that level, making it the most likely to be compressed. The L5 nerve root would typically be affected by an L4/L5 disc prolapse, and the L4 nerve root by an L3/L4 disc prolapse.
Question 13
A 37-year-old male has a confirmed L5/S1 paracentral disc prolapse causing left S1 radiculopathy. Using the provided dermatome and reflex/motor innervation charts, which combination of clinical findings is most consistent with a left S1 radiculopathy?

Explanation
Correct Answer: C
The case explicitly states that for an S1 distribution, one would expect pain, paraesthesia, and numbness in the posterior calf, heel, and lateral border of the foot. The S1 nerve root is responsible for ankle plantarflexion (gastrocnemius/soleus) and the Achilles reflex. Therefore, numbness in this dermatomal pattern, weakness in plantarflexion, and a diminished Achilles reflex are the classic findings for an S1 radiculopathy. Options A, B, D, and E describe findings consistent with L3/L4, L5, L4/L5 (saphenous nerve distribution), and Cauda Equina Syndrome, respectively, which are not consistent with an isolated S1 radiculopathy.
Question 14
A 45-year-old patient presents with symptoms consistent with an L5 radiculopathy, including weakness in ankle dorsiflexion and numbness over the dorsum of the foot. An MRI reveals a paracentral disc prolapse. Based on the provided background knowledge regarding nerve root anatomy in the lumbar spine, at which intervertebral level would a paracentral disc prolapse most commonly cause an L5 radiculopathy?
Explanation
Correct Answer: B
The case explains the concept of traversing nerve roots in the lumbar spine: 'Thus an L4/5 disc prolapse commonly affects the L5 nerve root.' This is because the L4 nerve root has already exited the canal below the L4 pedicle, and it is the L5 'traversing' nerve root that is most commonly compressed by a paracentral disc prolapse at the L4/L5 interspace. An L5/S1 disc prolapse would typically affect the S1 nerve root, and an L3/L4 disc prolapse would typically affect the L4 nerve root.
Question 15
A 50-year-old male with a known history of lumbar disc herniation presents to the emergency department with acute onset bilateral leg weakness, urinary hesitancy, and saddle anesthesia. An MRI confirms a large central disc extrusion at L4/L5 compressing the cauda equina. What is the most appropriate immediate management for this patient?
Explanation
Correct Answer: D
The patient's symptoms (bilateral leg weakness, urinary hesitancy, saddle anesthesia) are classic signs of Cauda Equina Syndrome (CES), which is confirmed by MRI. The case emphasizes the critical importance of early detection and intervention for CES, stating that 'early intervention (< 24 hours) has been shown to improve outcome.' Therefore, urgent surgical decompression is the most appropriate immediate management. Options A, B, C, and E represent conservative or delayed approaches that are inappropriate for a neurological emergency like CES.
Question 16
A patient presents with C7 radiculopathy symptoms, including weakness in triceps extension and numbness along the middle finger. Based on the background knowledge provided regarding nerve root anatomy in the cervical spine, which cervical disc level is most commonly associated with a C7 radiculopathy due to a prolapsed disc?
Explanation
Correct Answer: C
The case explains the unique nomenclature in the cervical spine: 'Because the C6 nerve root exits above (not below) the C6 vertebra this double change means a prolapsed cervical disc at the C5/C6 level most commonly affects the C6 nerve root.' Following this pattern, a disc prolapse at the C6/C7 level would most commonly affect the C7 nerve root, as the C7 nerve root exits above the C7 vertebra. Therefore, C6/C7 is the level most commonly associated with C7 radiculopathy.
Question 17
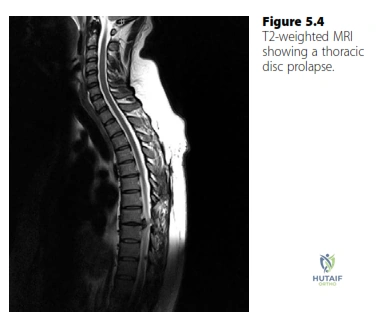
A 60-year-old patient presents with progressive gait disturbance, bilateral leg spasticity, and mid-thoracic back pain. Imaging reveals a calcified disc herniation at T8/T9. Based on the background knowledge provided, what is the most likely diagnosis and the appropriate surgical approach?
Explanation
Correct Answer: C
The case specifically describes thoracic disc prolapse as rare, typically presenting with symptoms and signs of spinal cord compression associated with thoracic back pain. It also notes that 'The discs are usually calcified and require decompression from the front. Treatment therefore is via a thoracotomy and partial vertebrectomy.' The patient's symptoms (gait disturbance, leg spasticity, mid-thoracic back pain) and the finding of a calcified disc herniation are consistent with a thoracic disc prolapse requiring an anterior approach.
Question 18
An MRI report describes a lumbar disc herniation where the disc material has a narrow 'neck' at its base but remains continuous with the parent disc. According to the nomenclature described in the case, how would this type of disc herniation be classified?
Explanation
Correct Answer: C
The case defines disc nomenclature, stating: 'A focal disc herniation may be described as a protrusion or extrusion. An extruded disc has a narrow ‘neck’ at its base.' The description of a narrow neck at its base while remaining continuous with the parent disc perfectly matches the definition of an extrusion. A sequestration would imply the material is no longer in continuity with the disc.
Question 19
The 37-year-old male from the initial case, with an L5/S1 paracentral disc prolapse causing S1 radiculopathy, has been undergoing conservative management for 8 weeks. He reports only minimal improvement in his pain and neurological symptoms. He has no red flag symptoms of Cauda Equina Syndrome. What is the most appropriate next step in management for this patient?
Explanation
Correct Answer: A
The case states the initial treatment for lumbar disc prolapse is conservative, as 'the natural history of most lumbar disc prolapses is that they resolve with time.' It further advises: 'If it has not resolved after 6–12 weeks of conservative management I would offer the patient microdiscectomy.' Since the patient is at 8 weeks with only minimal improvement and no red flags, continuing conservative management for the full 6-12 week period (i.e., another 4 weeks or more) is the most appropriate next step before considering surgical intervention. Immediate microdiscectomy (Option B) is premature, and options C, D, and E are not the primary next steps based on the provided treatment algorithm.
Question 20
A 12-year-old child presents with persistent low back pain and some vague leg discomfort. Unlike adults, nerve root tension signs are equivocal, and the pain is predominantly axial. Based on the background knowledge provided, which statement best describes the typical presentation and natural history of disc prolapse in children compared to adults?
Explanation
Correct Answer: C
The case provides specific background knowledge on pediatric disc prolapse: 'In children the symptoms and signs of disc prolapse are less well defined and back pain is a more prominent feature. Nerve root tension signs are also less likely to be positive and spontaneous resolution is less likely.' Therefore, option C accurately summarizes these differentiating features compared to adult presentations.
Question 21
A 35-year-old male presents with 6 weeks of severe right-sided leg pain radiating to the lateral border of his foot. Exam reveals an absent Achilles reflex and 4/5 plantar flexion. MRI shows a large paracentral disc extrusion at L5-S1. What is the most likely natural history if managed non-operatively?
Explanation
Question 22
A 45-year-old female presents with neck pain and right arm numbness. Physical examination reveals weakness in wrist extension, a diminished brachioradialis reflex, and decreased sensation over the dorsal web space of the thumb and index finger. A disc herniation at which of the following cervical levels is most likely responsible?
Explanation
Question 23
A 13-year-old premenarchal female with adolescent idiopathic scoliosis (AIS) is evaluated. She has a right thoracic curve of 32 degrees. Risser stage is 1.
What is the most appropriate next step in management?
Explanation
Question 24
An infant is diagnosed with congenital scoliosis. Radiographs reveal a fully unsegmented bar on the left and a fully segmented hemivertebra on the right at the same level. Which of the following statements best describes the prognosis and management of this deformity?
Explanation
Question 25
A 50-year-old male presents with left anterior thigh pain and weakness in knee extension. Physical examination reveals a diminished patellar reflex. MRI demonstrates a far lateral (extraforaminal) disc herniation at L4-L5. Which nerve root is most likely compressed?
Explanation
Question 26
A 14-year-old male with a history of Duchenne muscular dystrophy presents with a progressive scoliosis measuring 48 degrees. His forced vital capacity (FVC) is currently 45% of predicted. What is the most appropriate management?
Explanation
Question 27
A 16-year-old female undergoes posterior spinal fusion for AIS. On post-operative day 4, she develops severe epigastric pain, bilious vomiting, and abdominal distension. Which of the following is the most likely underlying anatomic cause of this complication?
Explanation
Question 28
A 65-year-old male with a history of chronic low back pain presents with neurogenic claudication. He reports his leg pain improves when leaning forward on a shopping cart. MRI shows severe central canal stenosis at L4-L5. According to the SPORT trial results for spinal stenosis, what is the expected outcome of surgical decompression compared to non-operative treatment?
Explanation
Question 29
A 4-year-old child presents with a progressive left thoracic scoliosis of 35 degrees. MRI of the neuroaxis reveals a Chiari I malformation and a syrinx spanning T3-T9. What is the most appropriate initial management?
Explanation
Question 30
A 55-year-old female presents with neck pain and clumsiness in her hands. She notes difficulty buttoning her shirts and frequent tripping. Exam shows hyperreflexia in both lower extremities, a positive Hoffmann's sign, and sustained ankle clonus. What is the most appropriate diagnostic imaging step?
Explanation
Question 31
During an anterior cervical discectomy and fusion (ACDF) via a right-sided approach, the surgeon carefully mobilizes the midline structures. Which of the following nerves is at higher risk of injury during a right-sided lower cervical approach compared to a left-sided approach?
Explanation
Question 32
A 25-year-old male sustains an acute paracentral disc herniation at L4-L5 resulting in an L5 radiculopathy. He has failed 6 weeks of physical therapy and NSAIDs. Which of the following physical exam findings is most specific for an L5 nerve root compression?
Explanation
Question 33
A 45-year-old male presents with right leg pain radiating to the dorsum of the foot and new-onset weakness in great toe extension. MRI demonstrates a posterolateral disc herniation at L4-L5. Which nerve root is most likely compressed?
Explanation
Question 34
A 60-year-old female presents with severe right upper extremity pain radiating to the middle finger, along with weakness in elbow extension. A cervical MRI reveals a herniated disc. Which intervertebral level is most likely affected?
Explanation
Question 35
A 14-year-old female with Adolescent Idiopathic Scoliosis (AIS) has a 32-degree main thoracic curve. She is premenarchal with a Risser stage of 0. Which of the following is the most appropriate evidence-based management?
Explanation
Question 36
A 3-year-old boy is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra at T8. Which of the following additional screening tests is mandatory in the initial workup?
Explanation
Question 37
According to the long-term results of the Spine Patient Outcomes Research Trial (SPORT) for lumbar disc herniation, which of the following statements is true regarding surgical versus nonoperative treatment?
Explanation
Question 38
A 16-year-old non-ambulatory male with Duchenne muscular dystrophy presents with a 45-degree thoracolumbar scoliosis. His forced vital capacity (FVC) is currently 40% of predicted. What is the most appropriate surgical strategy?
Explanation
Question 39
In infantile idiopathic scoliosis, the rib-vertebra angle difference (RVAD) of Mehta is used to predict the natural history of the curve. An RVAD greater than what threshold indicates a high probability of curve progression?
Explanation
Question 40
A 45-year-old male presents with severe right leg pain, weakness in great toe extension, and diminished sensation over the dorsal aspect of the right foot. He has a normal Achilles reflex. Which of the following disc herniations is the most likely cause of his symptoms?
Explanation
Question 41
A 50-year-old female presents with neck pain radiating down her arm to her index and middle fingers. On examination, she has weakness in elbow extension and an absent triceps reflex. Which cervical nerve root is most likely affected?
Explanation
Question 42
A 13-year-old premenarchal female with Adolescent Idiopathic Scoliosis (AIS) presents with a 32-degree right thoracic curve. Her Risser stage is 0. What is the most appropriate next step in management?
Explanation
Question 43
A newborn is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra at T8. In addition to a comprehensive physical exam, which of the following screening tests is most critical?
Explanation
Question 44
A 65-year-old male presents with bilateral calf pain that worsens with walking and improves when he leans forward on a shopping cart. To reliably differentiate between neurogenic and vascular claudication, which of the following non-invasive tests is most appropriate initially?
Explanation
Question 45
A 15-year-old female with AIS has a main thoracic curve of 50 degrees, a proximal thoracic curve of 20 degrees (which corrects to 10 degrees on side-bending), and a lumbar curve of 35 degrees (which corrects to 15 degrees on side-bending). According to the Lenke classification, what is her curve type?
Explanation
Question 46
An 8-month-old male is evaluated for infantile idiopathic scoliosis with a 25-degree left thoracic curve. The rib-vertebral angle difference (RVAD) of Mehta is measured at 28 degrees. What is the most appropriate next step in management?
Explanation
Question 47
A 42-year-old female presents to the emergency department with severe back pain, bilateral leg pain, and saddle anesthesia. Which of the following is considered the most sensitive early clinical finding for cauda equina syndrome?
Explanation
Question 48
During a neurological examination for suspected cervical spondylotic myelopathy, the examiner flicks the distal phalanx of the patient's middle finger, eliciting reflex flexion of the thumb and index finger. What is the name of this clinical sign?
Explanation
Question 49
A 55-year-old intravenous drug user presents with severe back pain. MRI reveals L3-L4 discitis and adjacent osteomyelitis without epidural compression. He is hemodynamically stable and neurologically intact. Blood cultures have been drawn but are pending. What is the next best step in management?
Explanation
Question 50
A 12-year-old male with spastic quadriplegic cerebral palsy presents with a 75-degree thoracolumbar neuromuscular scoliosis and a 25-degree pelvic obliquity. He is non-ambulatory and has difficulty sitting in his wheelchair. What is the most appropriate surgical strategy?
Explanation
Question 51
A 16-year-old gymnast complains of chronic low back pain worsening with extension. Radiographs confirm a Grade 2 isthmic spondylolisthesis at L5-S1. She has failed 6 months of physical therapy and bracing. What is the most appropriate surgical treatment?
Explanation
Question 52
A 50-year-old female presents with severe left anterior thigh pain, weakness in left hip flexion and knee extension, and a diminished left patellar reflex. MRI demonstrates a far lateral disc herniation at the L3-L4 level. Which nerve root is most likely compressed?
Explanation
Question 53
When planning corrective surgery for adult spinal deformity, achieving appropriate sagittal balance is highly correlated with improved patient-reported outcomes. Which of the following target thresholds for the Sagittal Vertical Axis (SVA) is considered optimal?
Explanation
Question 54
A 40-year-old male presents with isolated C5-C6 radiculopathy. The surgeon is considering a cervical disc arthroplasty (CDA) versus an anterior cervical discectomy and fusion (ACDF). Which of the following is an absolute contraindication to CDA?
Explanation
Question 55
A 45-year-old male presents with progressive myelopathy. MRI reveals a large, central, heavily calcified T8-T9 disc herniation causing severe cord compression. Which surgical approach carries the highest risk of iatrogenic spinal cord injury and should generally be avoided?
Explanation
Question 56
A 15-year-old male presents with an increased thoracic kyphosis measuring 65 degrees. To meet the radiographic Sorensen criteria for classical Scheuermann's disease, there must be anterior wedging of at least 5 degrees in a minimum of how many consecutive vertebrae?
Explanation
Question 57
A 65-year-old female is diagnosed with L4-L5 degenerative spondylolisthesis. Which of the following anatomic variations is the most significant predisposing risk factor for developing this specific condition?
Explanation
Question 58
A 55-year-old male undergoes a 9-hour posterior spinal fusion for complex adult deformity. Upon waking, he complains of painless, bilateral visual loss. His pupils are sluggish to light, but the anterior eye segments are normal. What is the most likely diagnosis?
Explanation
Question 59
A 60-year-old male is diagnosed with pyogenic spondylodiscitis at L4-L5 growing Methicillin-susceptible Staphylococcus aureus (MSSA). He is hemodynamically stable without epidural abscess or neurologic deficit. What is the minimum recommended duration of appropriate antimicrobial therapy?
Explanation
Question 60
A 13-year-old premenarchal female with adolescent idiopathic scoliosis (AIS) presents with a right thoracic curve. Radiographs show a Cobb angle of 32 degrees and a Risser stage of 0. Which of the following is the most appropriate management, and what is the optimal duration of daily treatment to prevent curve progression?
Explanation
Question 61
A 45-year-old male presents with right arm pain, numbness in his long finger, and weakness with elbow extension and wrist flexion. An MRI of the cervical spine is most likely to show a posterolateral disc herniation at which of the following levels?
Explanation
Question 62
A 6-month-old infant is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra at T8. Given the association of congenital scoliosis with other systemic anomalies, which of the following routine screening modalities is most appropriate?
Explanation
Question 63
A 52-year-old female presents with severe right leg pain radiating to her anterior thigh and medial leg, along with weakness in knee extension. MRI reveals a far lateral disc herniation at the L4-L5 level. Which nerve root is most likely compressed?
Explanation
Question 64
A 14-year-old female undergoes a posterior spinal fusion for adolescent idiopathic scoliosis. On postoperative day 5, she develops severe nausea, bilious emesis, and abdominal distension. What is the most likely pathophysiologic mechanism for her complication?
Explanation
Question 65
A 65-year-old male with long-standing cervical spondylosis experiences a hyperextension injury during a motor vehicle collision. He presents with severe bilateral upper extremity weakness and relatively preserved lower extremity strength. What is the expected prognosis regarding his motor recovery?
Explanation
Question 66
During a physical exam for suspected cervical myelopathy, tapping the distal brachioradialis tendon results in reflexive flexion of the fingers without elbow flexion. What is this clinical sign called, and what level of spinal cord compression does it indicate?
Explanation
Question 67
A 55-year-old male undergoes an uneventful C3-C6 laminectomy and fusion for cervical myelopathy. On postoperative day 2, he develops profound new weakness in bilateral deltoids and biceps, with preserved strength in his hands and legs. What is the most widely accepted mechanism for this postoperative complication?
Explanation
Question 68
A 68-year-old female presents with low back pain and severe neurogenic claudication. Flexion-extension radiographs show a Grade 1 degenerative spondylolisthesis at L4-L5. Which of the following is the most accurate statement regarding the typical neurologic compromise in this condition?
Explanation
Question 69
An 8-month-old male is evaluated for infantile idiopathic scoliosis. Radiographs demonstrate a left thoracic curve of 28 degrees. Measurement of the rib-vertebra angle difference (RVAD) at the apical vertebra is 25 degrees. What is the most likely natural history for this patient's deformity?
Explanation
Question 70
A 70-year-old male undergoes evaluation for a significant adult spinal deformity. Standing full-length radiographs reveal a pelvic incidence (PI) of 60 degrees, a lumbar lordosis (LL) of 30 degrees, and a sagittal vertical axis (SVA) of +8 cm. If surgical correction is planned, what is the primary radiographic goal to improve postoperative health-related quality of life (HRQOL)?
Explanation
Question 71
A 40-year-old man has a 6-week history of right-sided sciatica due to an extruded L5-S1 disc herniation. He has normal motor function but severe pain. He elects for continued conservative management. Which of the following best describes the physiological process by which spontaneous disc resorption occurs?
Explanation
Question 72
According to the Lenke Classification system for adolescent idiopathic scoliosis, which of the following criteria defines a 'structural' minor curve that must be included in the fusion construct?
Explanation
Question 73
A 50-year-old female presents with acute profound lower extremity weakness, sensory loss below the umbilicus, and urinary retention. MRI reveals a massive central, calcified T8-T9 disc herniation severely compressing the spinal cord. Which of the following surgical approaches is CONTRAINDICATED in the management of this patient?
Explanation
Question 74
A 16-year-old male with adolescent idiopathic scoliosis undergoes a posterior spinal fusion. During the deformity correction, the neuromonitoring technician reports a sudden, complete loss of motor evoked potentials (MEPs) in the lower extremities, while somatosensory evoked potentials (SSEPs) remain perfectly intact. Which neural pathway and associated vascular supply are most likely compromised?
Explanation
Question 75
A 35-year-old male with a history of intravenous drug use presents with severe back pain, fever, and an ESR of 95 mm/hr. MRI of the lumbar spine reveals fluid in the L3-L4 disc space with marrow edema in the adjacent vertebral bodies. Blood cultures are negative, and the patient is neurologically intact. What is the most appropriate next step in management?
Explanation
Question 76
A 48-year-old male presents with bilateral lower extremity radicular pain, saddle anesthesia, and urinary overflow incontinence. A post-void residual (PVR) ultrasound shows 400 mL of retained urine. MRI confirms a massive L4-L5 disc extrusion. Which of the following is the most critical factor in maximizing the recovery of his bladder function?
Explanation
Question 77
A 14-year-old elite gymnast presents with progressive low back pain worsened by extension. Radiographs reveal a Grade 2 isthmic spondylolisthesis at L5-S1. Despite 6 months of rest and core strengthening, she has persistent severe pain. If surgical intervention is chosen, what is the most appropriate procedure?
Explanation
Question 78
During posterior instrumentation of the thoracic spine, pedicle screws are being placed. Which of the following anatomic landmarks is most accurate for identifying the starting point for a mid-thoracic pedicle screw?
Explanation
Question 79
A 42-year-old female is diagnosed with a C5-C6 soft disc herniation causing medically refractory radiculopathy. She is considering cervical disc replacement (CDR) versus anterior cervical discectomy and fusion (ACDF). Which of the following is a recognized absolute contraindication for CDR in this patient?
Explanation
None
