ABOS Part I & AAOS OITE Orthopaedic Review: Bone Tumors & Trauma MCQs | Part 22154

Key Takeaway
The ABOS Part I Comprehensive Review module offers 50 advanced multiple-choice questions mirroring the ABOS Part I and AAOS OITE examinations. It covers critical topics in orthopaedic surgery, including bone tumor diagnosis, biopsy techniques, and comprehensive management of various traumatic fractures and associated complications, derived from high-yield clinical cases.
ABOS Part I & AAOS OITE Orthopaedic Review: Bone Tumors & Trauma MCQs | Part 22154
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 45-year-old male presents with a painful enlarging mass in his proximal humerus. Radiographs show a lytic, destructive lesion. MRI confirms a large lesion with soft tissue extension. The primary diagnostic procedure of choice to confirm the nature of this lesion, keeping in mind definitive treatment, should optimally be:
Explanation
Correct Answer: C
For most primary bone tumors, a core needle biopsy, preferably image-guided (CT or ultrasound), is the preferred initial diagnostic procedure. It provides adequate tissue for histological diagnosis, immunohistochemistry, and molecular studies, while minimizing contamination of surrounding tissues and allowing for planned limb-salvage surgery. FNA often provides insufficient tissue for comprehensive diagnosis of complex bone tumors. Open incisional biopsy carries a higher risk of tumor cell seeding and potential compromise of future surgical margins, making it a second-line option. Excisional biopsy is generally reserved for small, benign-appearing lesions or superficial soft tissue masses where diagnosis and treatment can be achieved simultaneously. Direct aspiration is primarily for cystic lesions or abscesses and typically does not yield sufficient cellular material for definitive diagnosis of solid tumors.
Question 2
When planning a biopsy for a suspected high-grade sarcoma of the distal femur, which of the following is the MOST critical principle to ensure limb salvage is not jeopardized?
Explanation
Correct Answer: D
The most critical principle for biopsy planning in high-grade sarcomas, especially in potential limb-salvage candidates, is to place the biopsy tract strategically. This involves making a small, longitudinal incision, violating only one fascial compartment, and ensuring the entire biopsy tract can be resected en bloc with the definitive tumor specimen. A transverse incision contaminates a broader area and makes definitive resection of the contaminated tissue difficult. While small incisions are good, the placement is paramount. Local anesthesia is often insufficient or inappropriate for bone biopsies. Avoiding joint capsule penetration is important, but less critical than the overall tract placement and fascial compartment violation.
Question 3
A 12-year-old male presents with right distal femoral pain. Imaging reveals a metaphyseal lesion consistent with osteosarcoma. A CT-guided core needle biopsy is planned. Which of the following is the most appropriate approach for specimen handling after obtaining the biopsy core?
Explanation
Correct Answer: C
Optimal handling of biopsy specimens for suspected primary bone tumors requires a multi-pronged approach to maximize diagnostic yield. Cores should be divided to allow for routine histology (formalin fixation), cytogenetics and molecular studies (fresh tissue, often snap-frozen), and potentially microbiological studies if infection is in the differential. Frozen section analysis can be useful intra-operatively for confirming tissue adequacy but is not sufficient for definitive diagnosis. Glutaraldehyde is rarely needed for initial diagnosis. Placing all cores in formalin or saline alone limits the range of advanced diagnostic tests that might be required.
Question 4
A biopsy is performed on a suspected aggressive lesion in the proximal tibia. The pathologist reports 'inadequate specimen for diagnosis'. Which of the following is the most common reason for an 'inadequate specimen' in bone tumor biopsies?
Explanation
Correct Answer: B
Sampling error is a very common reason for an inadequate or non-diagnostic bone biopsy. Tumors, especially large or aggressive ones, can have heterogeneous areas including necrosis, hemorrhage, or cystic degeneration. If the biopsy needle only samples these non-diagnostic areas, the pathologist will not be able to provide a definitive diagnosis. While crush artifact, insufficient quantity, and inappropriate fixation can occur, sampling error remains the most frequent challenge, even for experienced operators.
Question 5
Which of the following scenarios MOST strongly contraindicates an immediate biopsy of a bone lesion?
Explanation
Correct Answer: E
A small, well-defined cortical lesion with classic features of a Non-Ossifying Fibroma (NOF) on radiographs, especially in an asymptomatic patient, typically does not require a biopsy. NOFs are benign lesions with pathognomonic imaging findings. Observation is usually sufficient. In contrast, lesions in a known cancer patient with metastatic disease often require biopsy to confirm the primary origin or rule out a new primary. Rapidly expanding lesions with impending fracture and lesions with soft tissue involvement near neurovascular structures necessitate careful planning but are not absolute contraindications to biopsy; rather, they demand skilled execution.
Question 6
A 70-year-old male with a history of prostate cancer presents with a new lytic lesion in his iliac wing. A CT-guided core needle biopsy is planned. What is the MOST important consideration regarding the biopsy approach for this lesion?
Explanation
Correct Answer: D
When performing a biopsy of the iliac wing, avoiding entry through vital structures like the bowel or bladder is paramount. Penetrating these structures carries a high risk of infection and fistula formation. While avoiding the peritoneum is also important, the bowel and bladder are frequently in closer proximity to common iliac biopsy corridors. Selecting the largest needle is not the 'most' important consideration, and placing the incision over the center is not always the safest approach if vital structures are in the way. General anesthesia is not always required for iliac crest biopsies.
Question 7
A biopsy specimen from a bone lesion shows 'spindle cell neoplasm'. The pathologist requests additional studies. Which of the following is MOST likely to be helpful in differentiating between different types of spindle cell sarcomas (e.g., osteosarcoma, leiomyosarcoma, fibrosarcoma)?
Explanation
Correct Answer: D
When H&E staining reveals a 'spindle cell neoplasm', immunohistochemical (IHC) staining is typically the most helpful next step for differentiation. IHC uses antibodies to detect specific antigens expressed by different tumor types (e.g., desmin for muscle differentiation, S-100 for neural/chondroid differentiation, CD34 for vascular differentiation). This can help categorize the tumor. Electron microscopy can provide ultrastructural details but is less commonly used as a primary diagnostic tool than IHC. Cytogenetic analysis looks for chromosomal abnormalities and is crucial for some specific sarcomas (e.g., Ewing sarcoma translocation), but IHC is often the first-line for broad differentiation of spindle cell tumors. Gram stain and culture are for infection.
Question 8
Which of the following is considered a potential major complication unique to biopsy of bone lesions, particularly in weight-bearing bones?
Explanation
Correct Answer: C
Pathological fracture is a significant and unique complication associated with biopsy of bone lesions, especially in weight-bearing bones like the femur or tibia, or in weakened vertebrae. The biopsy procedure itself can further compromise the structural integrity of an already weakened bone, leading to a fracture. While infection, hematoma, neurovascular injury, and tumor seeding are all potential complications of any biopsy, pathological fracture is specifically related to the biomechanical insult of bone biopsy.
Question 9
A 30-year-old male presents with a painful mass in the distal radius. Radiographs show a lytic, eccentric lesion in the epiphysis. MRI confirms the lesion, which appears locally aggressive. A core needle biopsy is performed. Histology reveals multinucleated giant cells and mononuclear stromal cells. What is the MOST appropriate next step given these findings?
Explanation
Correct Answer: C
The description (multinucleated giant cells and mononuclear stromal cells in an epiphyseal lytic lesion) is highly suggestive of Giant Cell Tumor of Bone (GCT). However, it's crucial to correlate biopsy findings with clinical presentation and imaging. While suggestive, this appearance can rarely be seen in other lesions (e.g., brown tumor of hyperparathyroidism, aneurysmal bone cyst, even chondroblastoma). If the clinical and imaging picture strongly supports GCT, this biopsy result is generally sufficient. If there's any discordance, or if there's concern about sampling error missing a higher-grade component, repeat biopsy or open biopsy may be considered to confirm. Directly proceeding to surgery is often appropriate if the diagnosis is clear. Immediate chemotherapy is incorrect as GCT is typically treated surgically. Observation is inappropriate for an aggressive lesion.
Question 10
A biopsy report for a suspected bone tumor returns as 'benign reactive bone'. However, the clinical and radiological picture remains highly suspicious for malignancy. What is the MOST appropriate next action?
Explanation
Correct Answer: D
When there is a significant discordance between the biopsy results and the clinical/radiological findings (often termed 'clinicopathologic discordance'), the biopsy result should not be blindly accepted. 'Benign reactive bone' could be due to sampling error (e.g., biopsying surrounding reactive bone instead of the tumor), or the lesion might be a low-grade malignancy difficult to diagnose. The most appropriate next step is to carefully review all available data (imaging, clinical history, initial biopsy pathology) and, if suspicion for malignancy remains high, repeat the biopsy, potentially using an open technique to obtain a larger, more representative sample, or re-target with different imaging guidance.
Question 11
A 35-year-old male presents with incidental discovery of a lucent lesion with punctate calcifications in the metadiaphysis of the proximal phalanx of his hand. No pain or swelling.
Based on the provided image, what is the most likely diagnosis?

Explanation
Correct Answer: C
Enchondromas are the most common benign cartilaginous tumors of the small bones of the hands and feet. Their classic radiographic appearance includes a lucent, intramedullary lesion with characteristic punctate or rings-and-arcs calcifications. The asymptomatic nature and typical location (proximal phalanx) strongly favor enchondroma. Chondrosarcoma is less likely given the benign radiographic features and lack of symptoms. Osteochondroma is an exostosis, not intramedullary. Fibrous dysplasia has a ground-glass matrix. Giant cell tumor is typically epiphyseal and purely lytic.
Question 12
When differentiating a solitary enchondroma from a low-grade chondrosarcoma in a long bone, which of the following radiographic features, as potentially depicted in the image, is most concerning for malignancy?

Explanation
Correct Answer: A
Significant endosteal scalloping, particularly when it exceeds 2/3 of the cortical thickness, is a key radiographic indicator that suggests a more aggressive lesion, such as a low-grade chondrosarcoma, rather than a benign enchondroma. This indicates active erosion of the inner cortex. Punctate calcifications are typical for both benign and malignant chondroid lesions. Intralesional fat is often seen in bone infarcts or areas of marrow, not typically a chondroid tumor. A well-defined sclerotic border and absence of periosteal reaction are features more consistent with a benign lesion.
Question 13
A 40-year-old female has an asymptomatic enchondroma incidentally found in her proximal humerus during a shoulder MRI for rotator cuff impingement. The lesion measures 2x3cm, shows typical chondroid matrix calcifications, and no cortical breach or periosteal reaction, as seen in the representative image. What is the most appropriate initial management?

Explanation
Correct Answer: C
For an asymptomatic, radiographically benign-appearing enchondroma in a low-stress location like the proximal humerus, observation with serial radiographic follow-up (typically annual for 2-3 years) is the standard initial management. This approach monitors for any changes that might suggest malignant transformation or complications. Surgical intervention, biopsy, or more aggressive treatments are reserved for symptomatic lesions, those with concerning radiographic features (e.g., significant growth, cortical destruction, new pain), or evidence of progression.
Question 14
A 12-year-old boy presents with multiple enchondromas affecting the long bones of one limb and multiple cutaneous hemangiomas, as suggested by the clinical image. This presentation is most consistent with:

Explanation
Correct Answer: B
Maffucci's syndrome is characterized by the presence of multiple enchondromas and cutaneous (or visceral) hemangiomas. This combination is pathognomonic for the syndrome. Ollier's disease involves multiple enchondromas but without associated hemangiomas. McCune-Albright syndrome involves fibrous dysplasia, café-au-lait spots, and endocrine dysfunction. Neurofibromatosis Type 1 features neurofibromas and café-au-lait spots. Gorlin syndrome (Basal Cell Nevus Syndrome) involves multiple basal cell carcinomas and jaw keratocysts.
Question 15
On MRI, a benign enchondroma typically demonstrates which of the following signal characteristics, as shown in the representative T1 and T2 images?

Explanation
Correct Answer: A
Benign hyaline cartilage, as seen in an enchondroma, typically appears low signal on T1-weighted images and very high signal on T2-weighted images due to its high water content. It often shows a lobulated configuration with internal septations and peripheral enhancement after contrast, but typically not solid or aggressive enhancement. Fluid-fluid levels are characteristic of aneurysmal bone cysts, and perilesional edema with cortical destruction is indicative of malignancy or infection.
Question 16
A 60-year-old male presents with dull, constant pain in his distal femur. Radiographs show a 4 cm intramedullary lesion with a lobulated contour, speckled calcifications, and mild endosteal scalloping (<1/3 cortical thickness), as shown in the X-ray. A recent MRI shows no clear cortical breach or soft tissue mass, but increased tracer uptake on bone scan compared to previous studies. What is the most appropriate next step?

Explanation
Correct Answer: C
New onset or worsening pain in a chondroid lesion, especially in a long bone of an older patient, coupled with increased tracer uptake on a bone scan (suggesting metabolic activity), are concerning signs for malignant transformation to chondrosarcoma, even if other radiographic features are subtle. While a PET scan could also assess metabolic activity, a definitive diagnosis requires a biopsy (either open or image-guided core biopsy if sufficient tissue can be obtained) to assess the histology and grade the tumor. Observation is inappropriate given the symptoms and bone scan findings. Prophylactic fixation and radiation therapy are not initial diagnostic steps.
Question 17
An enchondroma-like lesion in which of the following locations, as exemplified by the image, carries the highest intrinsic risk of being a low-grade chondrosarcoma, even if radiographically benign-appearing?

Explanation
Correct Answer: D
Chondroid lesions in the axial skeleton (pelvis, scapula, sternum, ribs) and proximal long bones (femur, humerus) carry a higher intrinsic risk of being a low-grade chondrosarcoma compared to those in the small bones of the hands and feet or more distal long bones, even when imaging features appear benign. Lesions in the pelvis, in particular, are notorious for challenging differentiation and a higher index of suspicion for malignancy is warranted due to the difficulty in assessing subtle changes and the potential for significant morbidity if mismanaged.
Question 18
What feature, potentially seen in the image, is least suggestive of a benign enchondroma and more concerning for a low-grade chondrosarcoma?

Explanation
Correct Answer: D
Extensive bone destruction and cortical breakthrough with an associated soft tissue mass are definitive signs of an aggressive, malignant process, such as a chondrosarcoma. Benign enchondromas typically have an intact, smooth periosteum, a sharp interface with normal marrow, and do not extend into the soft tissues. A lobulated growth pattern is characteristic of cartilaginous tumors, both benign and malignant, and thus is not a distinguishing feature for malignancy on its own.
Question 19
Recent molecular studies have identified mutations in which gene family as commonly associated with enchondromas and low-grade chondrosarcomas?

Explanation
Correct Answer: C
Somatic mutations in isocitrate dehydrogenase 1 (IDH1) and IDH2 genes are now recognized as common genetic alterations in both solitary enchondromas and central low-grade chondrosarcomas. These mutations lead to the production of an oncometabolite, 2-hydroxyglutarate (2-HG), which plays a role in chondrogenesis and malignant transformation. This discovery has provided significant insights into the pathogenesis of these tumors and offers potential targets for future therapies. TP53 and MYC are associated with various cancers, RUNX2 with osteoblast differentiation, and PTPN11 with Noonan syndrome.
Question 20
In which of the following scenarios, as potentially depicted in the image, would surgical intervention (e.g., curettage and bone grafting) be most strongly considered for an otherwise asymptomatic enchondroma?

Explanation
Correct Answer: C
Significant cortical thinning, especially when it exceeds 50% of the cortical thickness in a weight-bearing long bone like the distal femur, creates a substantial risk of pathological fracture. Even if asymptomatic, prophylactic curettage and bone grafting would be strongly considered in this scenario to prevent a potentially devastating fracture and to restore structural integrity. The other options describe lesions in less mechanically critical locations or without significant fracture risk that would typically be managed with observation if asymptomatic.
Question 21
A 45-year-old male presents to the emergency department after a high-speed motor vehicle collision. He is hypotensive (BP 80/50 mmHg) and tachycardic (HR 125 bpm). Physical examination reveals obvious instability of the pelvic ring with ecchymosis over the perineum and pubic symphysis. Initial resuscitation with 2 liters of crystalloid has failed to improve his hemodynamic status. Which of the following is the most appropriate next step in his immediate management?

Explanation
Correct Answer: B
In a hemodynamically unstable patient with a suspected pelvic ring injury, the priority is hemorrhage control. A pelvic binder (or sheet) provides immediate temporary stabilization and reduction of the pelvic volume, which can tamponade bleeding. If the patient remains unstable after initial resuscitation and binder application, the next step is typically emergent surgical stabilization (e.g., external fixation) in the operating room or angiography for embolization, often dictated by local protocol and surgeon preference. While CT scan, Foley catheter insertion, and angiography are important diagnostic and therapeutic steps, immediate mechanical reduction via a binder and early surgical intervention for ongoing instability take precedence for life-threatening hemorrhage. Tranexamic acid and massive transfusion protocol are adjuncts but don't address the primary mechanical cause of bleeding.
Question 22
A 28-year-old male sustains a posterior hip dislocation after a dashboard injury in an MVC. On examination, his hip is internally rotated, adducted, and flexed. He has diminished sensation in the plantar aspect of his foot and weakness in ankle dorsiflexion and eversion. What is the most appropriate initial management step, considering the neurovascular status?

Explanation
Correct Answer: B
Posterior hip dislocations are orthopedic emergencies due to the high risk of avascular necrosis (AVN) of the femoral head and associated sciatic nerve injury. The most critical factor is the time to reduction. A neurological deficit (like the described sciatic nerve palsy) does NOT contraindicate immediate closed reduction. In fact, prompt reduction may allow for neurological recovery. A CT scan is important AFTER successful closed reduction to assess for incarcerated fragments or occult fractures (e.g., femoral head impaction, posterior wall acetabular fracture), but it should not delay reduction. Open reduction is reserved for failed closed reduction or irreducible dislocations. MRI is not an acute management tool.
Question 23
A 35-year-old construction worker sustains an open tibial shaft fracture (Gustilo-Anderson Type IIIA) after being struck by heavy machinery. He arrives in the ED 1 hour after injury. What is the immediate priority in his management after ATLS resuscitation and basic wound coverage?

Explanation
Correct Answer: B
For open fractures, particularly Gustilo-Anderson Type IIIA, emergent irrigation and debridement in the operating room is the most critical step to prevent infection and facilitate healing. While antibiotics are crucial, they are adjuncts to surgical debridement. The 'golden period' for debridement is traditionally considered within 6-8 hours, but earlier is better, especially for higher grades. CTA might be indicated if there's concern for vascular injury, but controlling contamination is paramount. Definitive fixation is performed after initial debridement, often at a later stage once the soft tissue envelope has been optimized. Compartment pressures would be measured if compartment syndrome is suspected, but initial management focuses on the open wound.
Question 24
A 22-year-old football player presents with severe pain in his right lower leg after a direct blow. He complains of paresthesia in his foot and pain on passive dorsiflexion of his toes. The calf is tense to palpation. What is the most reliable diagnostic finding for acute compartment syndrome?

Explanation
Correct Answer: E
The most reliable diagnostic criterion for acute compartment syndrome is a 'delta pressure' (diastolic blood pressure minus intracompartmental pressure) less than 30 mmHg. While an absolute pressure of 30 mmHg or greater is often used as a threshold, it must be considered in relation to the patient's blood pressure, as a lower absolute pressure can still be significant in hypotensive patients. Pain out of proportion to injury, paresthesia, and a tense compartment are classic clinical signs, but they are subjective and can be unreliable in altered mental status or pediatric patients. A palpable distal pulse does not rule out compartment syndrome, as arterial inflow is typically preserved until very late stages. Elevated CK levels indicate muscle damage but are not diagnostic of acute compartment syndrome.
Question 25
A 30-year-old male sustains a high-energy knee injury with gross instability in all planes. Radiographs confirm a knee dislocation without associated fractures. Pulses are diminished in the dorsalis pedis and posterior tibial arteries. What is the most appropriate next step in management?

Explanation
Correct Answer: A
Knee dislocation, especially with vascular compromise, is an orthopedic emergency. The immediate priority is reduction of the knee to restore blood flow and reduce tension on the popliteal artery. Closed reduction should be attempted immediately. After reduction, pulses must be meticulously reassessed. If pulses remain diminished or absent, or if there is any concern for popliteal artery injury (even with palpable pulses if the mechanism suggests high energy), an emergent CT angiogram (or arteriogram) is warranted. Delaying reduction for imaging significantly increases the risk of limb ischemia and potential amputation. Ligament repair and external fixation are important later steps, but re-establishing circulation is paramount.
Question 26
A 78-year-old female presents after a ground-level fall, complaining of right hip pain. Radiographs show a displaced, comminuted subtrochanteric femur fracture. She has multiple comorbidities including hypertension, diabetes, and atrial fibrillation. Which of the following is the most appropriate definitive management for this fracture?

Explanation
Correct Answer: C
Subtrochanteric femur fractures are typically high-energy injuries in younger patients and low-energy in osteoporotic elderly patients. The standard of care for displaced subtrochanteric fractures, particularly comminuted ones, is intramedullary nailing (IMN) with a long cephalomedullary nail. This implant provides biomechanical stability, allows for early weight-bearing, and has better outcomes compared to plate fixation in this region, which is subject to high bending forces. DHS is primarily used for intertrochanteric fractures and is biomechanically less suitable for subtrochanteric fractures. Hemiarthroplasty or THR are used for femoral neck fractures or certain highly comminuted intertrochanteric fractures not amenable to IMN, but not typically for subtrochanteric fractures. Non-operative management with traction is associated with high mortality and morbidity in the elderly and is generally avoided.
Question 27
A 40-year-old male falls from a height, landing on his heels. He presents with bilateral heel pain. Radiographs show a displaced calcaneus fracture. Which associated injury should be specifically investigated?

Explanation
Correct Answer: B
Calcaneus fractures, especially those resulting from a fall from a height, are associated with a significant incidence of lumbar spine compression fractures (10-15%). The axial loading mechanism transmits force up the kinetic chain. Therefore, it is critical to obtain imaging of the lumbar spine (lateral X-ray or CT) in all patients with calcaneus fractures from a fall from height. While other injuries can occur, a lumbar spine fracture is the most common and critical associated injury to specifically rule out due to potential neurological sequelae.
Question 28
A 55-year-old female presents with midfoot pain and inability to bear weight after stepping off a curb awkwardly. Radiographs show subtle widening between the first and second cuneiforms. What is the most sensitive imaging modality to confirm a Lisfranc injury and guide management?

Explanation
Correct Answer: D
Lisfranc injuries (tarsometatarsal joint complex disruption) can be subtle on standard plain radiographs, especially non-displaced or purely ligamentous injuries. While weight-bearing and stress radiographs are crucial for initial assessment, a CT scan is considered the most sensitive imaging modality to definitively diagnose and characterize Lisfranc injuries. It provides detailed bony anatomy, identifies small avulsion fractures, and measures subtle diastasis not visible on plain films. This information is critical for surgical planning. MRI is excellent for soft tissue injuries (ligaments) but often follows a CT scan for bony detail. A bone scan is not an acute management tool.
Question 29
A 60-year-old obese male sustains a high-energy fall onto his knee, resulting in a Schatzker Type VI tibial plateau fracture. He has multiple open wounds and significant soft tissue swelling. What is the most appropriate initial surgical approach for this injury?

Explanation
Correct Answer: B
Schatzker Type VI tibial plateau fractures are complex, high-energy injuries often associated with severe soft tissue damage, swelling, and open wounds. Immediate definitive ORIF carries a high risk of wound complications, infection, and flap necrosis due to the compromised soft tissue envelope. The preferred initial management is often damage control orthopedics: emergent external fixation with provisional joint spanning (spanning ex-fix) to stabilize the fracture, protect the soft tissues, and allow swelling to subside. Definitive ORIF is then performed in a delayed fashion (typically 7-14 days) once the 'wrinkle sign' appears and the soft tissues are amenable to surgery. Closed reduction and casting are inadequate for displaced, unstable, or articular fractures. Arthroplasty is not an acute treatment for fractures. Arthroscopic assistance is primarily for less severe fractures.
Question 30
A 48-year-old female presents after a motor vehicle accident with a comminuted fracture of the distal tibia extending into the ankle joint (pilon fracture). There is significant soft tissue swelling and blistering. What is the primary goal of immediate non-operative management?

Explanation
Correct Answer: C
Pilon fractures are challenging due to their articular involvement and often severe soft tissue injury. Significant soft tissue swelling and blistering indicate a compromised soft tissue envelope that is not ready for definitive surgical intervention. The primary goal of immediate non-operative management (often with a spanning external fixator for provisional stability) is to allow the soft tissues to recover, reduce swelling, and improve the skin condition. This 'waiting game' is crucial to minimize the high risk of wound complications (dehiscence, infection) associated with early surgery on inflamed tissues. Anatomical reduction is the ultimate goal, but it must be achieved when the soft tissues allow. Early weight-bearing is contraindicated. DVT prophylaxis is important but not the primary goal of local fracture management in this context.
Question 31
A 12-year-old boy presents with a painless, firm mass on the medial aspect of his distal femur. Plain radiographs are obtained. Which specific feature on the X-ray confirms the diagnosis of an osteochondroma and differentiates it from other surface lesions?

Explanation
Correct Answer: C
The hallmark radiographic feature of an osteochondroma is the continuity of the cortical and medullary bone of the exostosis with that of the underlying parent bone. This is crucial for differentiation. 'Sunburst' reaction suggests osteosarcoma. Lytic lesions with sclerotic rims are seen in osteoid osteoma. A purely cartilaginous mass is not typical for an osteochondroma, which is osteocartilaginous. Internal calcifications can be seen in various cartilaginous lesions.
Question 32
A 45-year-old man, with a known osteochondroma of the proximal tibia since childhood, reports a recent increase in size and new dull aching pain over the past 6 months. Radiographs are equivocal for changes, but an MRI shows a heterogeneous cartilage cap measuring 2.8 cm. What is the most appropriate next management step?

Explanation
Correct Answer: C
The new pain, recent growth in an adult, and a cartilage cap thickness greater than 2 cm are highly suspicious for malignant transformation to a secondary peripheral chondrosarcoma. A percutaneous core needle biopsy is the most appropriate next step to confirm the diagnosis and determine the grade of the tumor, which will guide definitive surgical planning. Observation or conservative treatment is inappropriate given the suspicion. Prophylactic amputation is never indicated without confirmed malignancy and extensive disease.
Question 33
A 7-year-old child presents with multiple bony masses and a family history of similar lesions. Genetic testing is considered. Which of the following genetic mutations is most commonly associated with Hereditary Multiple Exostoses (HME)?

Explanation
Correct Answer: B
Hereditary Multiple Exostoses (HME), also known as Multiple Osteochondromas, is an autosomal dominant disorder caused by germline mutations in either the EXT1 or EXT2 genes. These genes encode glycosyltransferases involved in heparan sulfate synthesis, a critical component of the extracellular matrix. TP53 is associated with sarcomas (e.g., Li-Fraumeni). COL1A1 is linked to osteogenesis imperfecta. IDH1/IDH2 mutations are seen in some chondrosarcomas (including dedifferentiated). SMAD3 is not directly linked to HME.
Question 34
A 30-year-old patient with a known osteochondroma is being evaluated for new onset pain and potential malignant transformation. Which imaging modality is most effective for evaluating the cartilage cap thickness of an osteochondroma, especially when assessing for malignant transformation?

Explanation
Correct Answer: C
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the cartilage cap thickness of an osteochondroma. The cartilage cap appears as a high signal intensity on T2-weighted images. A cap thickness greater than 2 cm in an adult is a strong indicator of malignant transformation to a secondary chondrosarcoma. Plain radiographs and CT are excellent for bony morphology but poor for cartilage visualization. Bone scintigraphy can show increased uptake but is not specific for cap thickness. Ultrasound can sometimes visualize the cap but is less reliable and quantitative than MRI.
Question 35
A 16-year-old active athlete presents with a painful, enlarging mass over a known osteochondroma on the posterior aspect of his distal femur. Examination reveals a fluctuant, tender swelling. What is the most likely complication?

Explanation
Correct Answer: D
The development of a painful, enlarging, fluctuant mass over an osteochondroma, particularly in an area subject to friction or repetitive motion, is highly suggestive of symptomatic bursa formation. The bursa develops in response to irritation from the osteochondroma. While other complications are possible, the description best fits bursitis. Malignant transformation typically presents with a hard, rapidly enlarging mass and increased pain, but less often fluctuant. Fracture causes acute, sharp pain. Pseudoaneurysm would have pulsatile swelling. Nerve compression causes neurological symptoms.
Question 36
Which of the following statements regarding the malignant transformation of a solitary osteochondroma is FALSE?

Explanation
Correct Answer: E
Malignant transformation of osteochondromas typically occurs in adults, usually after skeletal maturity, not in children under 10. The average age for secondary chondrosarcoma is 30-40 years. The other statements are true: HME carries a higher risk (5-25%) than solitary lesions (<1%), it transforms into peripheral chondrosarcoma, and the described signs are indeed warning signs.
Question 37
A 22-year-old male presents with a new onset of weakness in dorsiflexion and eversion of his right foot, consistent with foot drop. Imaging reveals a large osteochondroma near the knee. Which anatomical structure's involvement by an osteochondroma would typically cause symptoms of foot drop?

Explanation
Correct Answer: C
An osteochondroma at the proximal fibular neck can directly compress the common peroneal nerve, leading to symptoms of foot drop (weakness in dorsiflexion and eversion of the foot). The other nerves listed, if compressed, would cause different neurological deficits. Femoral nerve compression would affect quadriceps. Ulnar nerve at elbow causes intrinsic hand weakness. Tibial nerve in popliteal fossa causes calf and foot intrinsic weakness. Median nerve in carpal tunnel causes thumb and index/middle finger paresthesia and thenar weakness.
Question 38
A 6-year-old boy is diagnosed with an osteochondroma of the distal femur. His parents are concerned about its future growth. Which of the following describes the typical growth pattern of an osteochondroma?

Explanation
Correct Answer: B
Osteochondromas typically grow slowly during childhood, mimicking the growth of the adjacent growth plate. Their growth usually ceases with the closure of the adjacent physis at skeletal maturity. Any growth or enlargement after skeletal maturity, particularly if accompanied by pain, raises suspicion for malignant transformation. Rapid invasive growth or cycles of regression are not typical.
Question 39
A 40-year-old patient with a history of Hereditary Multiple Exostoses (HME) presents with a new, rapidly enlarging, painful mass in the pelvic region. Given the patient's history, what is the approximate risk of malignant transformation for a patient with HME?

Explanation
Correct Answer: C
The risk of malignant transformation in patients with Hereditary Multiple Exostoses (HME) is significantly higher than in solitary osteochondromas. Estimates range from 5% to 25%, depending on the study and diagnostic criteria. Solitary lesions have a risk of less than 1%. The clinical scenario strongly suggests malignant transformation, reinforcing the importance of knowing the increased risk in HME.
Question 40
A 13-year-old female presents with a painful osteochondroma of the distal femur that impinges on the vastus medialis muscle during knee flexion, causing significant functional limitation. Which of the following is the most appropriate treatment?

Explanation
Correct Answer: C
When an osteochondroma causes mechanical symptoms such as muscle impingement and pain during movement, surgical excision is the definitive treatment. Conservative measures like physical therapy, NSAIDs, or steroid injections are unlikely to resolve mechanical impingement. Observation would allow symptoms to persist or worsen. Surgical excision relieves the mechanical obstruction.
Question 41
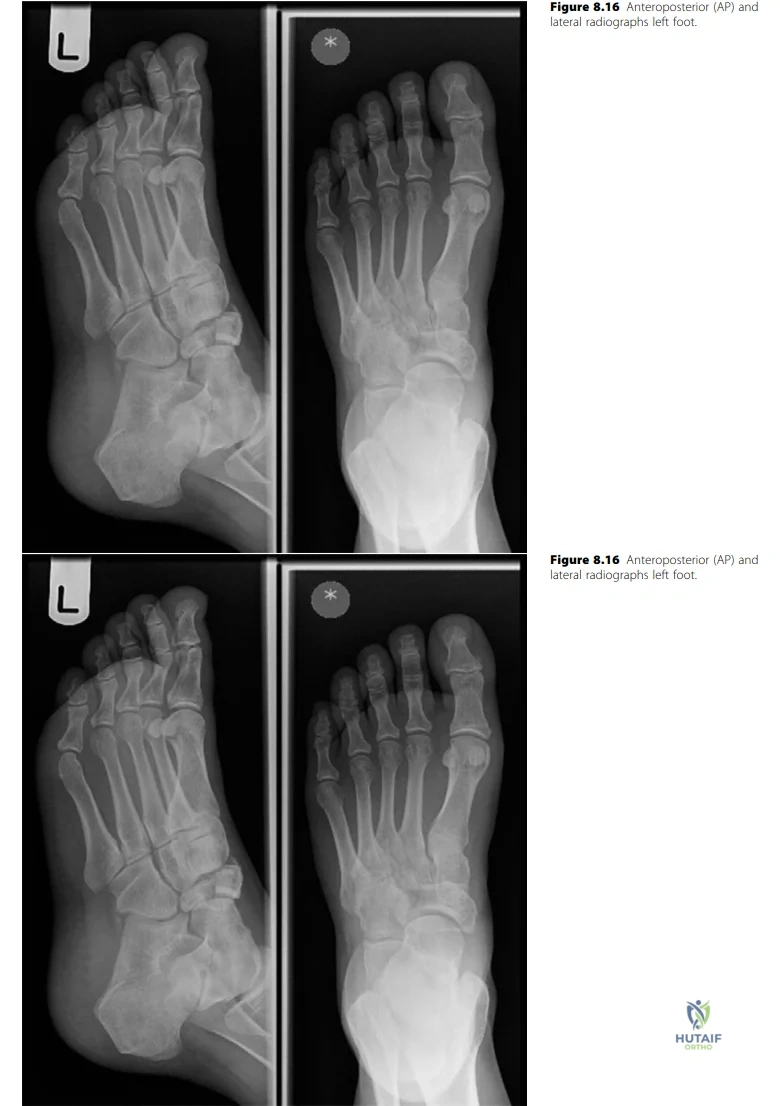
A 29-year-old female horse rider presents to the emergency department after falling off her horse, sustaining an isolated closed injury to her left foot. Initial radiographs are obtained as shown below.
Explanation
Correct Answer: C
The case explicitly states that after initial radiographs showing a displaced, comminuted navicular body fracture, the candidate would 'request further imaging, the modality of choice being CT scan.' A CT scan is crucial for detailed assessment of intra-articular involvement, comminution, and displacement, which are critical for surgical planning. While MRI can assess soft tissues, the immediate priority for a complex bony injury like this is detailed bone morphology. Immediate surgical exploration is premature without a full understanding of the fracture pattern, and other options are not the most appropriate next diagnostic step.
Question 42
A 29-year-old female presents after falling off a horse. Initial radiographs of her left foot are provided.
Explanation
Correct Answer: C
The candidate's initial assessment of the radiographs states: 'The radiographs of the left foot, AP and oblique show a displaced fracture of the body of navicular bone with comminution. There is overlap of mid-tarsal bones and I can’t exclude fractures of other tarsal bones.' The images clearly demonstrate significant disruption of the navicular body, consistent with a displaced and comminuted intra-articular fracture. Options A and B describe less severe or different types of navicular fractures. Options D and E describe fractures of different anatomical regions, although a Lisfranc injury could be associated, the primary and most evident injury described is the navicular body fracture.
Question 43
Following initial assessment of a 29-year-old female with a displaced, comminuted navicular body fracture, what is the most appropriate immediate non-operative management?
Explanation
Correct Answer: C
The case explicitly outlines the initial non-operative management: 'I would initially treat the injured foot in a backslab, with strict elevation and intermittent cryotherapy, adequate analgesia and close monitoring for evolving compartment syndrome.' This approach aims to control swelling, pain, and protect the injured foot while awaiting definitive management and ruling out acute complications like compartment syndrome. Immediate weight-bearing or range of motion exercises would be contraindicated for an unstable fracture. Systemic corticosteroids are not standard initial management for acute fractures.
Question 44
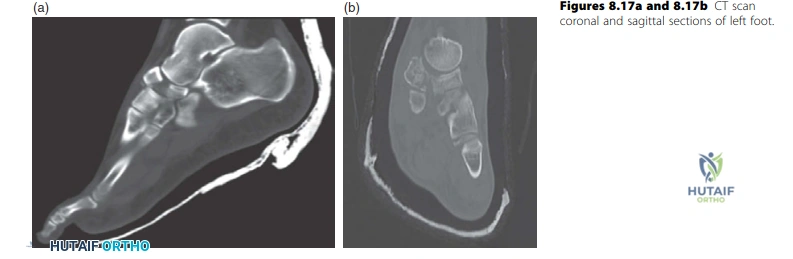
A 29-year-old female presents with a navicular body fracture. CT imaging is obtained, as shown below, confirming an unstable, displaced intra-articular fracture.
Explanation
Correct Answer: C
The candidate states: 'These coronal and sagittal sections of the CT scan confirm X-ray findings of a displaced fracture of the body of navicular bone with comminution. It is an unstable displaced intra-articular fracture and I would favour operative intervention rather than non-operative. The principles of management are to restore the articular surface, stabilize and hold the fracture to allow early mobilization.' While primary talonavicular arthrodesis (Option B) is mentioned as a consideration for severe comminution where restoration is not possible, the primary goal and preferred definitive management for an unstable, displaced intra-articular fracture is ORIF to restore the articular surface. Non-operative management is generally not suitable for unstable, displaced intra-articular fractures. Percutaneous fixation without reduction is unlikely to achieve articular congruity in a comminuted fracture.
Question 45
For operative management of this navicular body fracture, the surgeon plans an open reduction and internal fixation. Which surgical approach is most commonly utilized for direct visualization and reduction of a navicular body fracture, as described in the case?
Explanation
Correct Answer: C
The candidate explicitly states the surgical approach: 'I would use a medial approach, between the tibialis anterior and tibialis posterior tendons, preserving the remaining blood supply as much as possible, reduce the articular surface and stabilize with cannulated screws from lateral to medial.' This approach provides excellent access to the medial aspect of the navicular, which is crucial for reduction and fixation. Other approaches listed are either for different anatomical regions or do not provide optimal access to the navicular body.
Question 46
A 29-year-old female has an unstable, displaced intra-articular navicular body fracture confirmed by CT. The decision is made for operative intervention. What are the primary principles of operative management for this type of fracture?
Explanation
Correct Answer: C
The candidate clearly outlines the principles of management: 'The principles of management are to restore the articular surface, stabilize and hold the fracture to allow early mobilization.' This is the cornerstone of treating intra-articular fractures to minimize post-traumatic osteoarthritis and optimize functional outcomes. Immediate full weight-bearing (A) is generally not advisable. Primary fusion (B) is reserved for severe comminution, not all cases. Closed reduction and percutaneous fixation (D) may not be sufficient for displaced, comminuted fractures. Prophylactic antibiotics (E) are part of perioperative care but not the primary principle of fracture management itself.
Question 47
A 29-year-old female undergoes operative fixation for a displaced, comminuted navicular body fracture. Which of the following is considered a potential late complication specifically associated with this type of navicular fracture?
Explanation
Correct Answer: D
The case lists 'Late complications include non-union and loss of medial longitudinal arch support, painful talonavicular joint, post-traumatic osteoarthritis, as well as avascular necrosis and collapse.' Post-traumatic osteoarthritis is a common and significant late complication of intra-articular fractures, especially if articular congruity is not perfectly restored. Compartment syndrome (A), nerve injury (B), and anesthetic complications (E) are classified as immediate or early complications. Deep vein thrombosis (C) is a general surgical complication but not specifically highlighted as a late complication of this fracture in the same way OA is.
Question 48
The examiner asks about the occurrence of non-union and avascular necrosis in navicular fractures. What is the primary anatomical reason cited for the high risk of avascular necrosis and non-union in navicular body fractures?
Explanation
Correct Answer: C
The candidate explains: 'The navicular bone, similar to talus, has a large articular surface area and for the blood supply it relies on the radial arcade of vessels arising from the dorsalis pedis and medial planter arteries and this could be injured either at the time of fracture or during surgery, which could lead to AVN, non-union and/or collapse of the bone resulting in a painful mid-foot.' This unique and often tenuous blood supply makes the navicular susceptible to AVN and non-union following trauma or surgical disruption. Options A, B, D, and E are incorrect descriptions of the navicular's vascular anatomy or its biomechanical role.
Question 49
During the discussion of management options for a navicular body fracture, the candidate mentions an alternative for cases with severe comminution. In cases of severe comminution of the articular surface of the navicular, what alternative surgical intervention might be considered, as mentioned by the candidate?
Explanation
Correct Answer: B
The candidate states: 'However, sometimes that is not possible due to severe comminution of the articular surface, in which case I may consider primary fusion of the talonavicular joint.' This highlights that if the articular surface cannot be adequately reconstructed due to severe comminution, a primary fusion may be a more predictable option to achieve a pain-free and stable foot, albeit at the cost of motion. External fixation (A) is typically a temporary measure or for highly contaminated open fractures. Excision (C) is generally not performed for the navicular. Non-operative management (D) is usually insufficient for severe comminution. Bone grafting (E) is often an adjunct to fixation, not a standalone definitive treatment for an unstable fracture.
Question 50
A 29-year-old female undergoes operative fixation for a displaced, comminuted navicular body fracture. Which of the following is an early complication specifically mentioned in the context of operative management for this injury?
Explanation
Correct Answer: D
The candidate lists 'Early complications include infection, nerve injury (branches of superficial and deep peroneal nerves) and vascular injury (dorsalis pedis).' Nerve injury, particularly to the superficial or deep peroneal nerves, is a recognized early complication of foot and ankle surgery due to their anatomical proximity to surgical approaches and fracture sites. Options A, B, C, and E are all listed as potential late complications in the case.
Question 51
A 15-year-old boy presents with a pathologic fracture of the distal femur through a mixed lytic and blastic metaphyseal lesion. Radiographs reveal aggressive periosteal reaction. What is the most appropriate initial management?
Explanation
Question 52
A 65-year-old woman with a history of breast cancer presents with moderate thigh pain. Radiographs show a 2.5 cm lytic lesion in the peritrochanteric region of the femur that occupies 70% of the cortical diameter. Which of the following factors contributes the most points to her Mirels' score for prophylactic fixation?
Explanation
Question 53
A 60-year-old man sustains a pathologic subtrochanteric fracture. Biopsy confirms metastatic renal cell carcinoma. Before definitive surgical stabilization with an intramedullary nail, which intervention is most critical to perform?
Explanation
Question 54
A 16-year-old male sustains a pathologic fracture through a biopsy-proven distal femur osteosarcoma. How does the presence of this fracture alter his prognosis and treatment options compared to a patient without a fracture?
Explanation
Question 55
A 9-year-old boy falls and sustains a pathologic fracture through a centrally located, completely lytic lesion in the proximal humerus diaphysis. A radiopaque fragment is seen dependent within the cyst. What is the most appropriate initial management?
Explanation
Question 56
A 12-year-old boy presents with a minimally displaced pathologic fracture of the distal tibia through an eccentric, cortically based, multiloculated lucent lesion with a sclerotic margin. What is the most appropriate management?
Explanation
Question 57
A 32-year-old woman presents with a pathologic fracture of the proximal tibia through an expansile, lytic epiphyseal-metaphyseal lesion extending to subchondral bone. Biopsy shows a giant cell tumor. What medical therapy is indicated to facilitate future joint-salvage surgery?
Explanation
Question 58
A 45-year-old man presents with this painful destructive lesion of the distal femur. A core needle biopsy is planned. Which of the following is the most critical technical principle for the biopsy trajectory?
Explanation
Question 59
A 55-year-old man presents with an enlarging mass in the right ilium. Radiographs reveal a large lytic lesion with "popcorn" intralesional calcifications. Biopsy confirms grade 2 chondrosarcoma. What is the mainstay of definitive treatment?
Explanation
Question 60
A 14-year-old boy presents with severe thigh pain after a minor football injury. Radiographs show a permeative diaphyseal lesion with an "onion-skin" periosteal reaction. Which of the following translocations is most characteristic of the likely diagnosis?
Explanation
Question 61
A 25-year-old man presents with a hard mass in the posterior thigh, noticed 8 weeks after a blunt contusion. Radiographs show a soft tissue mass with dense peripheral ossification and a radiolucent center. What is the most appropriate management?
Explanation
Question 62
A 30-year-old man presents with a dull ache in his anterior leg. Radiographs reveal multiple, sharply circumscribed, eccentric lytic lesions with a "soap bubble" appearance in the anterior tibial diaphysis. What is the most likely diagnosis?
Explanation
Question 63
A 35-year-old woman sustains a minor injury to her ring finger. Radiographs show a minimally displaced fracture through a well-circumscribed, lytic lesion with stippled calcifications within the proximal phalanx. What is the appropriate initial step?
Explanation
Question 64
A 65-year-old woman treated with radiation for breast cancer 12 years ago presents with a new lytic lesion in her scapula. Biopsy shows high-grade pleomorphic sarcoma. According to Cahan's criteria for radiation-induced sarcoma, which of the following is required?
Explanation
Question 65
A 19-year-old runner presents with night pain in the thigh that dramatically improves with ibuprofen. Imaging reveals a 1 cm radiolucent nidus surrounded by thick cortical sclerosis. If conservative management fails, what is the preferred definitive treatment?
Explanation
Question 66
A 70-year-old man presents with a pathologic humeral fracture. A skeletal survey reveals multiple "punched-out" lytic lesions, and labs confirm multiple myeloma. Which imaging modality is most critical for detecting impending spinal cord compression in this patient?
Explanation
Question 67
A 14-year-old girl presents with an eccentric, expansile, lytic lesion in the proximal tibia metaphysis after a fall. MRI demonstrates multiple fluid-fluid levels. What is the underlying genetic abnormality commonly associated with the primary form of this lesion?
Explanation
Question 68
A 50-year-old man presents with bilateral stress fractures of the lower extremities and profound muscle weakness. Labs show severe hypophosphatemia, normal calcium, and elevated FGF-23 levels. What is the most likely underlying pathology?
Explanation
Question 69
A 15-year-old boy presents with severe thigh pain primarily at night, which is relieved significantly by ibuprofen. Radiographs and the provided imaging demonstrate a small radiolucent nidus surrounded by dense reactive sclerosis in the proximal femur.
What is the most appropriate definitive management if non-operative measures fail?
Explanation
Question 70
An 82-year-old female with a history of severe knee osteoarthritis sustains a comminuted intra-articular distal femur fracture following a ground-level fall.
She lives independently but struggles with rehabilitation protocols. What is the most reliable surgical option that allows immediate full weight-bearing?
Explanation
Question 71
A 14-year-old male presents with a permeative lytic lesion in the fibular diaphysis with an "onion-skin" periosteal reaction. Core biopsy reveals small, round, blue cells. Which specific chromosomal translocation is most characteristically associated with this tumor?
Explanation
Question 72
A 35-year-old male sustains a Gustilo-Anderson Type IIIB open tibia fracture. He undergoes urgent debridement and external fixation. According to current literature, what is the optimal timeframe for definitive soft tissue coverage to minimize deep infection rates?
Explanation
Question 73
A 55-year-old male is diagnosed with a grade 2 conventional chondrosarcoma of the proximal femur. Which of the following is the most appropriate definitive treatment?
Explanation
Question 74
A 28-year-old male is brought to the trauma bay with a heart rate of 120 bpm and blood pressure of 85/50 mmHg. Pelvic radiographs show an anteroposterior compression (APC-III) injury. To be maximally effective, a pelvic binder should be centered over which anatomic landmark?
Explanation
Question 75
A 32-year-old female has a large, eccentric lytic lesion in the distal femur epiphysis confirmed by biopsy to be a Giant Cell Tumor (GCT). If medical therapy is considered to downstage the tumor prior to surgery, which mechanism of action is utilized?
Explanation
Question 76
Six hours after intramedullary nailing of a closed diaphyseal tibia fracture, a patient complains of severe leg pain out of proportion to the injury. Passive stretch of the toes exacerbates the pain. Which of the following compartment pressure measurements is the accepted threshold for performing a fasciotomy?
Explanation
Question 77
A 45-year-old female has an incidental finding of a cartilaginous lesion in the proximal humerus. Which radiographic feature is most suggestive of a low-grade chondrosarcoma rather than a benign enchondroma?
Explanation
Question 78
A 25-year-old male sustains a vertically oriented (Pauwels Type III) femoral neck fracture. Which biomechanical force contributes most to the high rate of nonunion and displacement in this specific fracture pattern?
Explanation
Question 79
A 62-year-old male with multiple myeloma presents with a painful lytic lesion in the proximal femur involving 70% of the cortical diameter. Pain increases with weight-bearing. According to the Mirels criteria, what is the most appropriate management?
Explanation
Question 80
A 40-year-old male presents with a closed, highly comminuted tibial pilon fracture with severe soft tissue swelling. A spanning external fixator is applied. What is the most appropriate clinical indicator that the soft tissues are ready for definitive open reduction and internal fixation?
Explanation
Question 81
A 16-year-old female undergoes neoadjuvant chemotherapy followed by wide resection for a distal femur osteosarcoma. Which of the following histologic findings in the resected specimen is the most important prognostic factor for her overall survival?
Explanation
Question 82
A 30-year-old male sustains a displaced talar neck fracture with subluxation of the subtalar joint, while the ankle and talonavicular joints remain perfectly congruent. What is the Hawkins classification for this injury, and what is the approximate risk of avascular necrosis (AVN)?
Explanation
Question 83
A 9-year-old boy presents with mild shoulder pain after a minor fall. Radiographs show a centrally located, lucent metaphyseal lesion in the proximal humerus with a "fallen leaf" sign. What is the most appropriate initial management?
Explanation
Question 84
A 22-year-old athlete sustains a purely ligamentous Lisfranc injury with 3 mm of displacement between the medial and middle cuneiforms. Based on current literature comparing treatment modalities for purely ligamentous midfoot injuries, what is the best definitive surgical treatment?
Explanation
Question 85
A 65-year-old male presents with a large, destructive metastatic lesion in the proximal humerus. Biopsy confirms metastatic renal cell carcinoma. Before proceeding with wide resection and endoprosthetic reconstruction, what is the most critical preoperative intervention to minimize intraoperative morbidity?
Explanation
Question 86
A 24-year-old male falls onto an outstretched hand and sustains a displaced fracture of the proximal pole of the scaphoid. The high risk of avascular necrosis in this region is primarily due to the retrograde blood supply from which vessel?
Explanation
Question 87
A 10-year-old girl is evaluated for precocious puberty, café-au-lait macules with irregular borders (coast of Maine), and multiple lytic bone lesions showing a "ground-glass" appearance on radiographs. What is the underlying genetic mutation responsible for this syndrome?
Explanation
Question 88
A 45-year-old skier sustains a Schatzker Type II tibial plateau fracture. During open reduction and internal fixation, the surgeon must be prepared to address an associated soft-tissue injury. Which of the following is the most commonly associated intra-articular injury with this fracture pattern?
Explanation
Question 89
A 55-year-old male presents with a large soft tissue mass in the anterior compartment of his thigh. Imaging is highly suspicious for a soft tissue sarcoma. An incisional biopsy is planned. Which of the following is the most critical principle to adhere to during the biopsy?
Explanation
Question 90
A 62-year-old female with a history of breast cancer presents with increasing right thigh pain. Radiographs reveal a 4 cm lytic lesion in the peritrochanteric region with 50% cortical destruction.
According to Mirels' criteria, what is the most appropriate management?
Explanation
Question 91
A 30-year-old female undergoes intralesional curettage and cementation for a giant cell tumor of the distal femur. Two years later, she presents with recurrence. She is started on denosumab therapy prior to re-operation. What is the specific mechanism of action of this medication?
Explanation
Question 92
A 50-year-old man presents with dull pelvic pain. Imaging reveals a large, destructive lesion in the right ilium with stippled calcifications. Biopsy confirms a grade II chondrosarcoma. What is the most appropriate definitive management?
Explanation
Question 93
A 14-year-old boy trips and sustains a closed fracture of the distal femur. Initial radiographs and subsequent MRI strongly suggest a primary osteosarcoma at the fracture site. A diagnostic biopsy confirms high-grade osteosarcoma. What is the recommended treatment strategy?
Explanation
Question 94
A 68-year-old male presents with severe right arm pain and an impending pathologic fracture of the humerus. Workup reveals a solitary, destructive lytic lesion and a new diagnosis of metastatic renal cell carcinoma.
If surgical stabilization is planned, what preoperative intervention is most critical to decrease perioperative morbidity?
Explanation
Question 95
A 65-year-old male presents with back pain, anemia, hypercalcemia, and elevated creatinine. Radiographs show multiple punched-out lytic lesions in the skull and spine. Which of the following imaging modalities is LEAST likely to accurately reflect the extent of his skeletal disease?
Explanation
Question 96
A 12-year-old boy presents with a painful, swollen mid-thigh. Radiographs show a permeative diaphyseal lesion with an onion-skin periosteal reaction. A biopsy is performed. Which of the following cytogenetic abnormalities is most characteristic of this diagnosis?
Explanation
Question 97
A 45-year-old female presents with a displaced fracture of the femoral shaft. She has a history of a soft tissue sarcoma of the thigh treated with wide resection and adjuvant external beam radiation 7 years ago. Which of the following best describes the healing potential of this fracture?
Explanation
Question 98
During a biopsy of a suspected high-grade sarcoma of the proximal tibia, the surgeon utilizes a transverse incision, elevates large fasciocutaneous flaps, and inadvertently exposes the adjacent popliteal neurovascular bundle. What is the most significant consequence of this technical error?
Explanation
None
