Orthopedic Board Review: Musculoskeletal Tumors, Ankylosing Spondylitis, Synovial Chondromatosis | Part 15
Key Takeaway
An orthopedic musculoskeletal pathology review covers key conditions like atypical lipomas, osteochondromas, Ankylosing Spondylitis, and synovial chondromatosis. It includes diagnostic criteria, imaging findings (MRI, X-ray), histological features, clinical presentations, and management strategies essential for board exam preparation.
Orthopedic Board Review: Musculoskeletal Tumors, Ankylosing Spondylitis, Synovial Chondromatosis | Part 15
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 55-year-old male with long-standing ankylosing spondylitis presents with new-onset neck pain after a minor low-energy fall. His neurological exam is currently intact, and initial cervical radiographs are unrevealing.
What is the most appropriate next step in management?
Explanation
Question 2
A 45-year-old man with a history of ankylosing spondylitis presents to the emergency department after a low-energy fall. He reports new-onset neck pain but no neurologic deficits. Radiographs demonstrate an undisplaced fracture through the C5-C6 disc space. What is the most appropriate management?
Explanation
Question 3
Synovial chondromatosis is a benign nodular condition characterized by which of the following pathophysiologic mechanisms?
Explanation
Question 4
A 55-year-old woman presents with a deep thigh mass. MRI reveals a large, predominantly lipomatous tumor with thickened, nodular septa. Biopsy shows mature adipocytes with focal hyperchromatic, atypical stromal cells. Which genetic alteration is most specific for this diagnosis?
Explanation
Question 5
An 18-year-old male with multiple hereditary exostoses (MHE) is evaluated. He has multiple bony prominences around his knees and ankles. The genetic mutation associated with this condition primarily affects the synthesis of which of the following?
Explanation
Question 6
A 35-year-old male with advanced ankylosing spondylitis presents with progressive chin-on-chest deformity impairing his horizontal gaze. Preoperative evaluation determines that an extension osteotomy of the cervical spine is necessary. At which anatomical level is this osteotomy most safely and commonly performed?
Explanation
Question 7
A 42-year-old man presents with chronic knee pain and mechanical symptoms. Radiographs show multiple intra-articular calcific bodies of uniform size. What is the most appropriate management for symptomatic primary synovial chondromatosis of the knee?
Explanation
Question 8
A 62-year-old male with a 30-year history of ankylosing spondylitis presents to the emergency department with severe neck pain following a ground-level fall.
Given the rigid nature of his spine, what is the most common and characteristic cervical fracture pattern seen in this patient population?
Explanation
Question 9
A 34-year-old male with confirmed ankylosing spondylitis has persistent axial pain and morning stiffness despite maximum continuous therapy with two different nonsteroidal anti-inflammatory drugs (NSAIDs) for three months. What is the most appropriate next step in medical management?
Explanation
Question 10
Which of the following best describes the fundamental pathogenesis underlying primary synovial chondromatosis?
Explanation
Question 11
Multiple Hereditary Exostoses (MHE) is characterized by multiple osteochondromas throughout the skeleton. Mutations in the EXT1 and EXT2 genes are causative. What is the primary molecular function impaired by these mutations?
Explanation
Question 12
A 55-year-old male presents with a large, slow-growing, deep soft tissue mass in his posterior thigh. Histopathology demonstrates mature adipocytes with focal variation in cell size and hyperchromatic stromal cells.
Which molecular finding specifically differentiates an Atypical Lipomatous Tumor (ALT) from a benign lipoma?
Explanation
Question 13
Patients with advanced ankylosing spondylitis undergoing total hip arthroplasty (THA) are at a significantly higher risk for which of the following postoperative complications compared to patients with primary osteoarthritis?
Explanation
Question 14
An 18-year-old male with a known solitary osteochondroma of the proximal tibia presents with increasing localized pain and recent growth of the lesion over the past 6 months. MRI reveals a cartilage cap measuring 2.8 cm in thickness.
What is the most likely diagnosis?
Explanation
Question 15
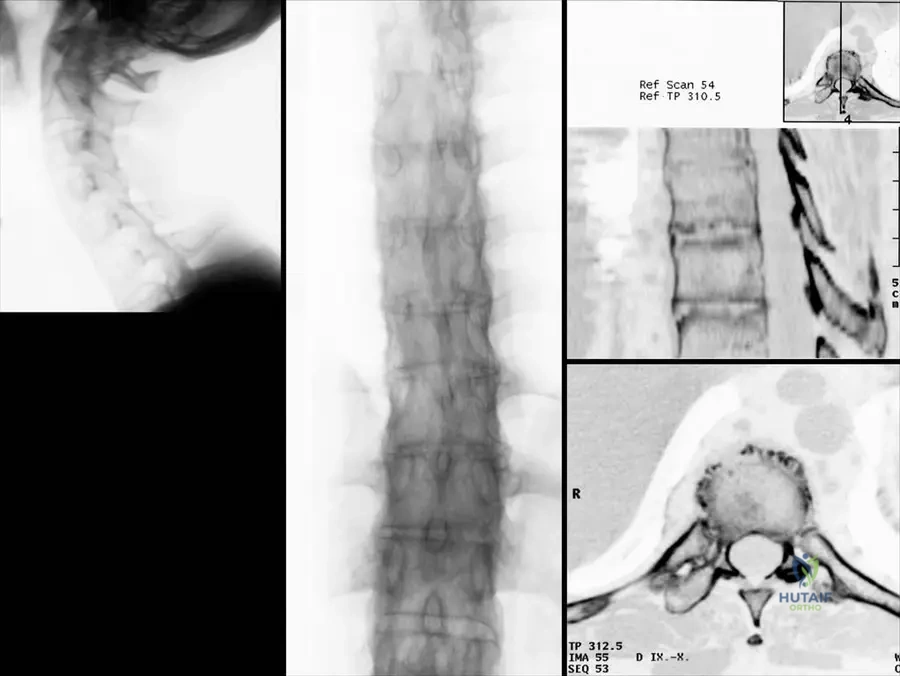
A 45-year-old male with long-standing ankylosing spondylitis presents with localized, progressive mechanical back pain. Radiographs demonstrate a destructive discovertebral lesion with surrounding reactive sclerosis. Inflammatory markers are mildly elevated.
What is the most likely diagnosis?
Explanation
Question 16
Histologically, an Atypical Lipomatous Tumor (ALT) and a Well-Differentiated Liposarcoma (WDLPS) are identical. What is the primary criterion used to differentiate these two entities in nomenclature?
Explanation
Question 17
A 55-year-old patient with long-standing ankylosing spondylitis is scheduled for orthopedic surgery under general anesthesia. Which of the following represents the most critical anesthetic challenge in this patient?
Explanation
Question 18
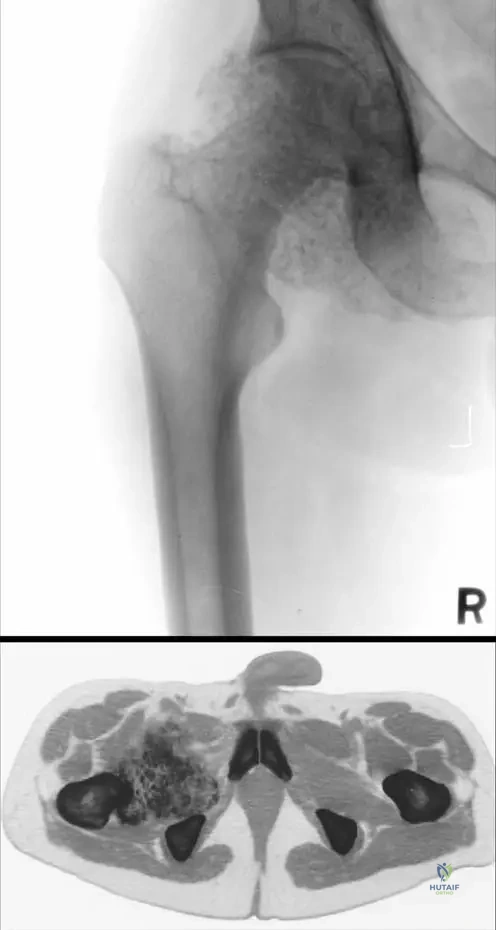
A 40-year-old male with a history of recurrent primary synovial chondromatosis of the hip presents with rapid clinical deterioration, severe pain, and extensive bony destruction on imaging.
What is the most feared complication in this setting?
Explanation
Question 19
Which of the following describes the characteristic forearm deformity frequently observed in patients with Multiple Hereditary Exostoses (MHE)?
Explanation
Question 20
A 50-year-old male with ankylosing spondylitis presents with a severe chin-on-chest deformity, rendering him unable to look straight ahead. The primary kyphosis is located at the cervicothoracic junction. What is the surgical procedure of choice to correct this deformity?
Explanation
Question 21
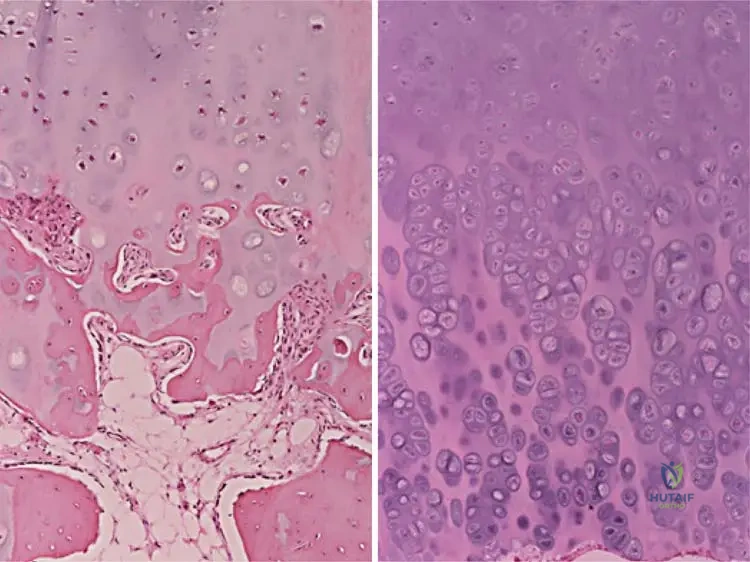
An osteochondroma is defined as a cartilage-capped exostosis.
Which of the following imaging features is pathognomonic and strictly required for the diagnosis of an osteochondroma?
Explanation
Question 22
On a standard radiograph, the presence of multiple, uniform-sized, spherical calcified loose bodies within the joint capsule of the knee strongly suggests which of the following diagnoses?
Explanation
Question 23
A 45-year-old male with long-standing ankylosing spondylitis presents after a minor fall with severe neck pain. Radiographs reveal a fracture through the C6-C7 disc space extending through the posterior elements. What is the most appropriate management?
Explanation
Question 24
A 35-year-old male presents with chronic knee pain, swelling, and mechanical catching. Radiographs show multiple intra-articular calcified bodies of uniform size.
Which of the following is the underlying pathophysiology of this condition?
Explanation
Question 25
A 16-year-old boy with multiple hereditary exostoses (MHE) is being evaluated. Which of the following characteristics is most suggestive of malignant transformation of an osteochondroma in an adult patient?
Explanation
Question 26
A 28-year-old male presents with alternating buttock pain and morning stiffness improving with activity. Radiographs reveal bilateral sacroiliitis.
Which of the following extra-articular manifestations is most commonly associated with this condition?
Explanation
Question 27
A 55-year-old male presents with a deep, slow-growing painless mass in his thigh. Biopsy reveals mature adipocytes with focal nuclear atypia and hyperchromatic stromal cells.
Which genetic abnormality is the hallmark of this lesion?
Explanation
Question 28
A 12-year-old girl is diagnosed with multiple hereditary exostoses (MHE). Radiographs show multiple bony projections with cortico-medullary continuity.
The genetic mutation responsible for this condition primarily affects the synthesis of which of the following?
Explanation
Question 29
A 42-year-old male with long-standing ankylosing spondylitis
has severe bilateral hip pain and stiffness and is scheduled for a total hip arthroplasty (THA). Which of the following is the most significant perioperative concern specific to his disease?
Explanation
Question 30
A 40-year-old woman is diagnosed with primary synovial chondromatosis of the hip. She complains of progressive pain, catching, and limited range of motion. What is the recommended definitive surgical treatment to minimize recurrence?
Explanation
Question 31
A 19-year-old male presents with a painless, hard mass about the medial proximal tibia. Radiographs confirm a pedunculated osteochondroma pointing away from the joint.
He complains of occasional snapping over the mass. What is the most common non-malignant complication of an osteochondroma in this location?
Explanation
Question 32
Which of the following anatomic locations is most strongly associated with a higher risk of local recurrence and potential for dedifferentiation in atypical lipomatous tumors (ALT/WDLPS)?
Explanation
Question 33
A patient with advanced ankylosing spondylitis sustains a minimal trauma fracture of the thoracic spine.
The fracture is noted to be a completely unstable, transdiscal shear injury. Which pathological process makes the spine biomechanically susceptible to this fracture pattern?
Explanation
Question 34
A 25-year-old male with a known distal femoral osteochondroma notes recent enlargement.
An MRI is ordered. Which finding would most strongly indicate a biopsy for suspected malignant transformation?
Explanation
Question 35
How can primary synovial chondromatosis be distinguished radiographically and histologically from secondary synovial chondromatosis (such as that caused by severe osteoarthritis)?
Explanation
Question 36
A 55-year-old man with a long-standing history of ankylosing spondylitis presents to the emergency department after a low-energy fall. He complains of severe neck pain but has normal neurology. CT scan reveals a transverse fracture through the C6-C7 disc space extending through the posterior elements. What is the most appropriate management for this injury?
Explanation
Question 37
A 28-year-old man presents with chronic lower back pain and morning stiffness lasting over an hour. Radiographs of the sacroiliac joints are unremarkable.
What is the earliest MRI finding of sacroiliitis in patients with this condition?
Explanation
Question 38
A 45-year-old male with severe hip pain secondary to ankylosing spondylitis is scheduled for a total hip arthroplasty (THA). Compared to a patient with primary osteoarthritis, this patient is at a significantly higher risk for which of the following postoperative complications?
Explanation
Question 39
A 16-year-old boy presents with a painless, hard mass around his distal femur. Imaging shows a sessile lesion with cortico-medullary continuity with the host bone.
The pathogenesis of this condition is most commonly associated with a mutation in a gene responsible for the synthesis of which of the following?
Explanation
Question 40
A 60-year-old woman presents with a slowly enlarging, painless mass deep in her right thigh. Biopsy reveals mature adipocytes with focal cellular atypia and hyperchromatic stromal cells.
Which of the following genetic abnormalities is most characteristic of this tumor?
Explanation
Question 41
A 40-year-old man presents with chronic knee pain, swelling, and mechanical locking. Radiographs show multiple, uniform, calcified loose bodies within the joint capsule.
What is the underlying pathophysiology of this primary condition?
Explanation
Question 42
When evaluating a patient with multiple intra-articular loose bodies, which of the following radiographic features best differentiates primary synovial chondromatosis from secondary synovial chondromatosis?
Explanation
Question 43
A 35-year-old man with a known history of an asymptomatic distal femur osteochondroma presents with new-onset pain and enlargement of the mass. An MRI is obtained. Which of the following findings is most predictive of malignant transformation to a secondary chondrosarcoma?
Explanation
Question 44
A 60-year-old male with long-standing ankylosing spondylitis presents with localized, severe back pain. Radiographs demonstrate a destructive intervertebral disc lesion with endplate sclerosis and adjacent pseudarthrosis. What is the eponymous term for this lesion?
Explanation
Question 45
Which of the following best explains why an "atypical lipomatous tumor" and a "well-differentiated liposarcoma" are classified differently despite having identical histological features?
Explanation
Question 46
A 12-year-old girl is found to have a pedunculated bony mass on her proximal tibia that points away from the joint line.
Which of the following best describes the embryologic/developmental origin of this lesion?
Explanation
Question 47
A 45-year-old patient with known, long-standing primary synovial chondromatosis of the hip returns with rapidly progressive pain. Advanced imaging is ordered. Which of the following MRI findings is the most reliable indicator of malignant transformation to a synovial chondrosarcoma?
Explanation
Question 48
A 50-year-old man with ankylosing spondylitis presents with a severe chin-on-chest deformity, preventing forward gaze. He is scheduled for a corrective spinal osteotomy. Which of the following anatomical levels is the safest and most optimal site for a pedicle subtraction osteotomy (PSO) to correct this cervicothoracic kyphosis?
Explanation
Question 49
A 10-year-old boy with Multiple Hereditary Exostoses (MHE) is being evaluated for progressive forearm deformity. Which of the following represents the most classic pattern of forearm deformity seen in this syndrome?
Explanation
Question 50
When evaluating an intramuscular lipomatous tumor of the thigh on MRI, which of the following features is most suggestive of an Atypical Lipomatous Tumor (ALT) rather than a simple benign lipoma?
Explanation
Question 51
A 65-year-old patient with end-stage ankylosing spondylitis presents with a restrictive pattern on pulmonary function tests. The patient denies any history of smoking or primary pulmonary disease. This restrictive lung physiology is primarily due to ankylosis of which of the following structures?
Explanation
Question 52
Which of the following is considered the standard surgical management for a symptomatic patient with primary synovial chondromatosis of the knee to minimize the risk of recurrence?
Explanation
Question 53
An 18-year-old runner with a known sessile osteochondroma on the proximal medial tibia complains of recent focal pain and swelling directly over the lesion. Imaging reveals a fluid-filled sac overlying the cartilage cap with no increase in cap thickness. What is the most likely diagnosis?
Explanation
Question 54
A 70-year-old man with ankylosing spondylitis suffers a hyperextension injury to his cervical spine resulting in a fracture.
Due to the altered biomechanics of the ankylosed spine, this patient is at uniquely high risk for which of the following acute complications?
Explanation
Question 55
A 52-year-old man is diagnosed with an atypical lipomatous tumor (ALT) in the anterior compartment of his thigh. There is no evidence of metastasis. What is the most appropriate surgical treatment approach?
Explanation
Question 56
A 28-year-old male with multiple hereditary exostoses presents with a newly enlarging mass around his right knee.
MRI shows an osteochondroma with a cartilaginous cap. What cartilage cap thickness on MRI is most highly suggestive of secondary malignant transformation to chondrosarcoma in an adult?
Explanation
Question 57
A 45-year-old male with severe ankylosing spondylitis is planning to undergo a corrective spinal osteotomy for rigid cervicothoracic kyphosis.
Which of the following clinical parameters is most useful for calculating the exact amount of sagittal correction required preoperatively?

Explanation
Question 58
Primary synovial chondromatosis of the knee in a 40-year-old male is best described by which of the following histological processes?
Explanation
Question 59
A 55-year-old female presents with a deep-seated intramuscular thigh mass. Biopsy reveals an atypical lipomatous tumor.
Which of the following genetic alterations is diagnostic for this specific lesion?
Explanation
Question 60
A 35-year-old male with ankylosing spondylitis is scheduled for a total hip arthroplasty (THA) due to severe bilateral hip involvement. He is at significantly increased risk for which of the following postoperative complications compared to patients with primary osteoarthritis?
Explanation
Question 61
Multiple hereditary exostoses (MHE) is an autosomal dominant condition linked to mutations in EXT1 and EXT2. These genes encode for glycosyltransferases primarily involved in the synthesis of which of the following?
Explanation
Question 62
A 62-year-old man with ankylosing spondylitis sustains a seemingly minor cervical spine fracture after a ground-level fall.
He presents with delayed, rapidly progressive quadriparesis 24 hours after admission despite a stable and immobilized fracture pattern. What is the most likely cause?
Explanation
Question 63
A 45-year-old patient with a long-standing history of multiple loose bodies in the hip joint diagnosed as primary synovial chondromatosis presents with sudden onset of severe rest pain and rapid swelling.
What is the most feared complication that must be ruled out?
Explanation
Question 64
What is the most definitive pathognomonic radiographic and histologic feature of an osteochondroma?
Explanation
Question 65
First-line medical therapy for a patient with severe ankylosing spondylitis who experiences persistent axial symptoms despite continuous, maximized use of NSAIDs involves targeted inhibition of which of the following cytokines?
Explanation
Question 66
A 60-year-old male is diagnosed with an atypical lipomatous tumor (ALT) in the deep posterior compartment of the thigh. There is no clinical or radiographic evidence of dedifferentiation. What is the most appropriate surgical treatment?
Explanation
Question 67
Which of the following clinical or pathologic features best distinguishes primary synovial chondromatosis from secondary synovial chondromatosis?
Explanation
Question 68
A 22-year-old male with a known, untreated osteochondroma of the distal posterior femur complains of a new, expanding pulsatile mass in the popliteal fossa and severe calf claudication. What is the most likely diagnosis?
Explanation
Question 69
A 24-year-old male complains of severe morning stiffness and inflammatory back pain. Plain radiographs of the pelvis are completely negative for sacroiliitis.
Which MRI sequence is most sensitive for detecting the early, active inflammatory phase of sacroiliitis in suspected ankylosing spondylitis?
Explanation
Question 70
Which of the following best describes the typical fracture pattern seen in the cervical spine of a patient with advanced ankylosing spondylitis following a low-energy fall?
Explanation
Question 71
A 16-year-old male presents with a painless, palpable mass about the distal femur.
Which radiographic finding is considered pathognomonic for this lesion?
Explanation
Question 72
A 50-year-old male with long-standing ankylosing spondylitis presents with progressive weakness in both lower extremities following a minor ground-level fall. CT of the cervical spine reveals a completely displaced, extension-distraction fracture at C6-C7. Which of the following is the most likely additional complication seen in this demographic?
Explanation
Question 73
A 55-year-old male presents with a large, slow-growing, deep-seated mass in the posterior thigh.
Biopsy demonstrates mature adipocytes with focal nuclear atypia. Which genetic alteration is most characteristic of this lesion?

Explanation
Question 74
Which clinical feature most reliably distinguishes Primary Synovial Chondromatosis from Secondary Synovial Chondromatosis?
Explanation
Question 75
A 12-year-old boy with multiple hereditary exostoses (MHE) is evaluated for bilateral knee bumps. The underlying genetic defect in this condition primarily impairs which of the following cellular processes?
Explanation
Question 76
A 35-year-old male with severe ankylosing spondylitis requires bilateral total hip arthroplasties (THA) for end-stage auto-fusion of his hips. Postoperatively, this patient is at the highest risk for which of the following complications?
Explanation
Question 77
A 25-year-old male with a known sessile osteochondroma of the proximal tibia reports a recent onset of pain and rapid growth of the mass. An MRI is obtained. Which finding most strongly suggests malignant transformation?
Explanation
Question 78
A 45-year-old male with ankylosing spondylitis presents with a severe fixed, forward-flexed posture. He reports difficulty looking straight ahead. He wishes to undergo surgical deformity correction. What is the most appropriate surgical intervention to correct his sagittal imbalance?
Explanation
Question 79
Which joint is most frequently affected by primary synovial chondromatosis?
Explanation
Question 80
A patient with undiagnosed ankylosing spondylitis is most likely to present with which of the following extra-articular manifestations prior to definitive spinal fusion?
Explanation
Question 81
An incidental cartilaginous lesion is identified in the proximal humerus of a 50-year-old female. Which of the following MRI findings differentiates a low-grade chondrosarcoma from a benign enchondroma?
Explanation
Question 82
A 30-year-old female is diagnosed with symptomatic primary synovial chondromatosis of the knee. What is the most appropriate initial surgical management?
Explanation
Question 83
A 22-year-old male presents with a painless mass about his distal femur. Radiographs demonstrate a pedunculated exostosis pointing away from the joint.
Which of the following gene mutations and corresponding molecular mechanisms is most likely responsible for this condition?
Explanation
Question 84
A 45-year-old male presents with worsening knee pain and swelling after years of stable, mild discomfort. Radiographs reveal multiple uniformly sized periarticular calcified bodies.
MRI demonstrates a new, large, non-calcified soft tissue mass invading the adjacent femur. What is the most likely diagnosis of this new lesion?
Explanation
Question 85
A 55-year-old female undergoes a core needle biopsy of a deep, 10-cm intramuscular thigh mass.
Histology shows mature adipocytes with focal nuclear atypia. Which of the following molecular markers is most specific for distinguishing this lesion from a benign lipoma?
Explanation
Question 86
A 60-year-old man with a 30-year history of ankylosing spondylitis presents with localized, progressive thoracolumbar back pain. Radiographs demonstrate an established bamboo spine with a localized, destructive radiolucent cleft at the T11-T12 disc space with sclerotic margins. What is the most appropriate initial management for this specific radiographic finding?
Explanation
Question 87
A 48-year-old man with ankylosing spondylitis presents with a severe chin-on-chest deformity, significantly impairing his horizontal gaze and ability to eat.
A surgical correction is planned. At which anatomic level is an extension osteotomy most safely and effectively performed to correct this specific deformity?
Explanation
Question 88
A 40-year-old male with ankylosing spondylitis presents with localized, worsening back pain and progressive kyphosis. Radiographs reveal a focal destructive discovertebral lesion with surrounding sclerotic margins. What is the most likely diagnosis?
Explanation
Question 89
A 35-year-old male with severe ankylosing spondylitis is scheduled for bilateral total hip arthroplasty due to disabling hip ankylosis. What is the most appropriate perioperative intervention to mitigate a highly prevalent postoperative complication in this population?
Explanation
Question 90
A 50-year-old female with a 10-year history of primary synovial chondromatosis of the knee presents with rapid worsening of pain, significant new swelling, and restricted motion. MRI demonstrates aggressive soft tissue expansion and new marrow invasion. What is the most likely cause of her acute deterioration?
Explanation
Question 91
A 15-year-old male presents with multiple painless, bony bumps around his knees and wrists. Radiographs reveal multiple pedunculated lesions growing away from the adjacent joints. Genetic testing is ordered. What is the underlying biochemical consequence of the most likely genetic mutation?

Explanation
Question 92
A 60-year-old male presents with a deep, painless, slow-growing 10 cm mass in the posterior thigh. Core needle biopsy shows mature adipose tissue with scattered focal atypia and hyperchromatic stromal cells. Which molecular finding confirms the diagnosis of an atypical lipomatous tumor rather than a benign lipoma?
Explanation
Question 93
A 30-year-old male with a known solitary sessile osteochondroma of the distal femur presents with new-onset, progressive pain at the site. Which of the following MRI findings is most indicative of malignant transformation in a skeletally mature patient?
Explanation
Question 94
A 45-year-old male with severe ankylosing spondylitis presents with a fixed chin-on-chest deformity, severely limiting his forward horizontal gaze and ability to eat. An extension osteotomy is planned for correction. Which anatomical level is generally considered the safest and most effective for this procedure?
Explanation
Question 95
A 40-year-old female presents with chronic catching and locking in her right hip. Radiographs demonstrate numerous uniform, intra-articular calcified loose bodies. What is the definitive surgical management required to minimize the risk of recurrence?
Explanation
Question 96
A 55-year-old male with long-standing ankylosing spondylitis suffers a minor mechanical fall and sustains a transdiscal fracture at the T10-T11 level. Why do spinal fractures in this patient population carry an exceptionally high risk of neurologic compromise?
Explanation
Question 97
A general surgeon performs an unplanned excisional biopsy of an atypical lipomatous tumor located deep in the anterior thigh using a transverse incision. How does this initial approach primarily complicate the definitive orthopedic oncology management?
Explanation
Question 98
Pathological evaluation of a solitary sessile mass resected from the proximal humerus of a 14-year-old boy reveals host trabecular bone merging with a superficial cartilage cap. Which histologic feature of the cartilage cap characterizes it as a classic benign osteochondroma?
Explanation
None
