ABOS Part I & AAOS OITE Orthopaedic Review: Shoulder, Foot, Knee MCQs | Part 22304
Key Takeaway
This module provides a comprehensive orthopaedic board review covering key topics in shoulder, foot/ankle, and knee surgery. It includes multiple-choice questions on glenohumeral dislocations, cavovarus foot deformities, meniscal biomechanics, PCL avulsions, and ACL reconstruction techniques, ideal for ABOS Part I and AAOS OITE exam preparation.
ABOS Part I & AAOS OITE Orthopaedic Review: Shoulder, Foot, Knee MCQs | Part 22304
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 84-year-old female presents after a fall onto her outstretched hand. You are asked to describe her shoulder X-ray. Which of the following views is most critical for definitively diagnosing a posterior glenohumeral dislocation when an AP view shows a 'lightbulb' sign?
Explanation
Correct Answer: C
The axillary view is the gold standard for assessing glenohumeral joint congruity and confirming the direction of dislocation (anterior or posterior). While the 'lightbulb' sign on an AP view is suggestive of posterior dislocation, it is not definitive. The Scapular Y view can indicate posterior dislocation if the humeral head is posterior to the glenoid, but it's a sagittal view. The West Point and Stryker notch views are specific for glenoid rim defects or Hill-Sachs lesions, respectively, not primary dislocation diagnosis.
Question 2
An 84-year-old woman presents with long-standing shoulder pain and weakness, with active elevation limited to 60 degrees. Her X-ray shows superior migration of the humeral head, acromial erosion, and significant glenohumeral joint space narrowing. Which of the following is the most likely diagnosis?
Explanation
Correct Answer: C
Rotator cuff arthropathy (RCA) is characterized by chronic, massive rotator cuff tears leading to superior migration of the humeral head, resulting in direct articulation between the humeral head and the acromion. This pathological contact causes secondary degenerative changes, including acromial erosion, glenohumeral joint space narrowing (typically superiorly), and often extensive osteophyte formation. Primary glenohumeral osteoarthritis usually shows concentric or inferior joint space narrowing without significant superior migration. CPPD can cause degenerative changes but not typically with this degree of superior migration. Adhesive capsulitis shows no significant radiographic findings. Seronegative spondyloarthropathies would show erosive changes, often with sacroiliitis, but not the specific pattern of RCA.
Question 3
An 84-year-old osteoporotic lady sustains a proximal humerus fracture after a low-energy fall. Her X-ray shows a fracture involving the surgical neck, greater tuberosity, and lesser tuberosity, with articular displacement. According to the Neer classification, how would you classify this fracture?
Explanation
Correct Answer: C
The Neer classification divides the proximal humerus into four anatomical parts: the humeral head (articular segment), greater tuberosity, lesser tuberosity, and humeral shaft. A fracture involving all three tuberosities and the surgical neck (which separates the head from the shaft) constitutes four distinct displaced segments, thus classifying it as a 4-part fracture. Each displaced segment (>1cm displacement or >45 degrees angulation) counts as a 'part.' A 2-part involves one displaced segment, a 3-part involves two displaced segments (e.g., head + greater tuberosity + shaft). Articular displacement is a characteristic of 4-part fractures but not a primary classification part itself. Valgus-impacted is a specific stable variant, usually 2- or 3-part.
Question 4
When reviewing the shoulder X-ray of an 84-year-old female, which radiographic finding is most indicative of severe osteoporosis, beyond just fracture presence?
Explanation
Correct Answer: C
Trabecular thinning and cortical attenuation (thinning of the outer bone layer) are direct radiographic signs of reduced bone mineral density characteristic of osteoporosis. While osteoporosis predisposes to fractures, the other options are signs of degenerative joint disease (subchondral cysts, joint space narrowing, osteophyte formation) or rotator cuff arthropathy (acromial erosion), not direct indicators of systemic bone density loss.
Question 5
An X-ray of an 84-year-old lady's shoulder shows significant inferomedial glenohumeral joint space narrowing, subchondral sclerosis, and large inferior osteophytes. There is no evidence of superior migration of the humeral head. Which diagnosis is most consistent with these findings?
Explanation
Correct Answer: C
Primary glenohumeral osteoarthritis (GHOA) typically presents with inferomedial joint space narrowing, subchondral sclerosis, and significant osteophyte formation, particularly inferiorly (humeral head and glenoid). Crucially, there is no superior migration of the humeral head, differentiating it from rotator cuff tear arthropathy. CPPD can mimic OA but often shows chondrocalcinosis. Septic arthritis would show rapid joint destruction, effusion, and possibly periarticular osteopenia, less typically prominent osteophytes. Avascular necrosis would show subchondral collapse, crescent sign, and eventual secondary OA.
Question 6
An 84-year-old lady presents with recurrent anterior glenohumeral instability. Which specialized radiographic view is most effective for visualizing a bony Bankart lesion or an anterior glenoid rim fracture?
Explanation
Correct Answer: B
The West Point axillary view is specifically designed to profile the anterior-inferior glenoid rim, making it superior for detecting bony Bankart lesions or anterior glenoid rim fractures, which are common sequelae of anterior glenohumeral dislocation. The Stryker Notch view is for Hill-Sachs lesions (posterolateral humeral head compression fracture). The Scapular Y view assesses dislocation direction. The Grashey view is a true AP. The Apical Oblique view can also show glenoid rim pathology but less specifically than West Point.
Question 7
When describing the shoulder X-ray of an elderly patient, you note an apparent non-union of the acromion. Which specific view would be most crucial to confirm an os acromiale and differentiate it from an acute fracture?
Explanation
Correct Answer: C
The outlet view (or supraspinatus outlet view) is optimal for evaluating the acromial morphology, including the presence of an os acromiale, by projecting the acromion en face. An os acromiale is a developmental failure of fusion of the acromial apophyses. While other views might incidentally show it, the outlet view provides the best profile. The Zanca view is specific for the AC joint. Axillary view is for glenohumeral congruity. Transthoracic is for humeral shaft.
Question 8
A 'Grashey view' is requested for an 84-year-old female's shoulder. What is the primary purpose of this specific projection?
Explanation
Correct Answer: C
The Grashey view is a 'true AP' view of the glenohumeral joint, achieved by internally rotating the patient approximately 30-45 degrees to align the glenoid parallel to the X-ray beam. This eliminates overlap of the humeral head and glenoid, allowing for accurate assessment of joint space and articulation. While rotator cuff integrity cannot be assessed directly, its sequelae (e.g., superior migration) are better appreciated.
Question 9
On an AP internal rotation view of an 84-year-old woman's shoulder, which anatomical landmark is best visualized en face?
Explanation
Correct Answer: B
The AP internal rotation view brings the lesser tuberosity into profile, facing medially. The greater tuberosity is seen medially overlapping the humeral head. Conversely, the AP external rotation view profiles the greater tuberosity laterally.
Question 10
When reviewing an AP external rotation view of an elderly patient's shoulder, which structure is typically seen in profile laterally on the humeral head?
Explanation
Correct Answer: B
The AP external rotation view rotates the humerus externally, bringing the greater tuberosity into profile on the lateral aspect of the humeral head. The lesser tuberosity is then positioned anteriorly and medially, often superimposing on the humeral head.
Question 11
A 14-year-old male presents with bilateral cavovarus feet. On examination, you note significant plantarflexion of the first metatarsal and hindfoot varus that corrects when a 1cm block is placed under the lateral aspect of the foot, elevating the fifth metatarsal head. What is the most appropriate interpretation of this Coleman Block Test result?
Explanation
Correct Answer: B
The Coleman Block Test assesses the flexibility of the hindfoot varus component of a cavus foot. By placing a 1cm block under the lateral border of the foot (from the calcaneus to the fifth metatarsal head), the test effectively dorsiflexes and pronates the forefoot, neutralizing the effect of a plantarflexed first ray. If the hindfoot varus corrects to neutral or valgus with the block, it indicates that the hindfoot varus is flexible and compensatory for a plantarflexed first ray. This means the primary deformity is in the forefoot (plantarflexed first ray), and addressing this will correct the hindfoot. If the hindfoot varus remains uncorrected, it signifies a rigid hindfoot deformity, likely requiring a calcaneal osteotomy (e.g., Dwyer or lateralizing calcaneal osteotomy).
Question 12
Regarding the neurological examination in a patient with a suspected cavus foot, which of the following findings is most strongly associated with Charcot-Marie-Tooth (CMT) disease?
Explanation
Correct Answer: C
Charcot-Marie-Tooth (CMT) disease, particularly CMT1 (demyelinating form), is the most common hereditary neuropathy and a frequent cause of cavus foot. Classic neurological findings include slowly progressive, bilateral, and symmetric distal muscle weakness and atrophy (peroneal muscle atrophy leading to 'stork leg' appearance), sensory loss (often stocking-glove distribution), and absent or diminished deep tendon reflexes, particularly at the ankles. Upper motor neuron signs are characteristic of other neurological conditions (e.g., spinal cord lesions), while isolated or acute unilateral findings are less typical of CMT.
Question 13
A 20-year-old presents with a progressive, painful cavovarus foot deformity. Radiographs show a high arch, claw toes, and increased calcaneal pitch. Which radiographic measurement is typically increased in a cavus foot, indicating hindfoot deformity?
Explanation
Correct Answer: C
The calcaneal pitch angle (also known as the angle of inclination of the calcaneus or the calcaneal inclination angle) is formed by the intersection of a line tangent to the inferior border of the calcaneus and the floor or a line parallel to the weight-bearing surface. In a cavus foot, the calcaneus is typically more vertically oriented, resulting in an increased calcaneal pitch angle, contributing to the high arch. Meary's angle (lateral talo-first metatarsal angle) is often increased (dorsal apex angulation) due to forefoot equinus or plantarflexed first ray. The talonavicular coverage angle assesses forefoot abduction/adduction, and the Angle of Gissane (critical angle of Gissane) relates to calcaneal fractures, not primarily cavus foot morphology.
Question 14
Which of the following muscle imbalances is most commonly implicated in the development and progression of a cavus foot deformity, particularly in neuromuscular conditions?
Explanation
Correct Answer: A
The classic muscle imbalance contributing to a cavus foot is an imbalance between the tibialis anterior and peroneus longus. Weakness of the tibialis anterior (which dorsiflexes the ankle and first metatarsal) combined with overactivity or normal strength of the peroneus longus (which plantarflexes the first metatarsal) leads to a plantarflexed first ray. This plantarflexed first ray drives the forefoot equinus and subsequent compensatory hindfoot varus to achieve a plantigrade foot. While intrinsic muscle weakness contributes to claw toes, and other muscle imbalances may exist, the tibialis anterior/peroneus longus imbalance is a primary driver of the arch deformity.
Question 15
When examining a child with a suspected progressive cavus foot, what is the most critical component of the initial evaluation to determine etiology?
Explanation
Correct Answer: A
A progressive cavus foot, especially in a child, is highly suggestive of an underlying neurological condition (e.g., Charcot-Marie-Tooth disease, Friedreich's ataxia, spinal dysraphism). Therefore, a detailed family history for similar conditions and a thorough neurological examination are paramount to identify the underlying etiology. The neurological exam should include evaluation of muscle strength, sensation, reflexes, and coordination. Shoe wear, activity levels, gait analysis, and pressure mapping are valuable for characterizing the deformity and its biomechanical impact but are secondary to identifying the primary cause.
Question 16
A patient presents with a rigid cavus foot and chronic lateral ankle instability. You determine the hindfoot varus is rigid and irreducible. Which surgical procedure is most appropriate for correcting the hindfoot deformity in this scenario?
Explanation
Correct Answer: C
For a rigid hindfoot varus, a calcaneal osteotomy is often required. The Dwyer osteotomy (lateral closing wedge osteotomy of the calcaneus) is a well-established procedure to correct a rigid hindfoot varus by removing a wedge of bone from the lateral aspect of the calcaneus, effectively rotating the tuberosity into valgus. Subtalar arthrodesis might be considered for severe, symptomatic, arthritic, or recalcitrant deformities, but an osteotomy preserves joint motion if possible. The other options address forefoot or soft tissue components, not primarily rigid hindfoot varus.
Question 17
During a physical examination of a cavus foot, you observe significant clawing of the lesser toes. This deformity is primarily caused by:
Explanation
Correct Answer: C
Claw toe deformities (hyperextension of the MTP joint, flexion of the PIP and DIP joints) in a cavus foot primarily result from an imbalance where the strong extrinsic flexor muscles (flexor digitorum longus and brevis) overpower the weak intrinsic foot muscles (lumbricals and interossei). The intrinsic muscles are responsible for stabilizing the MTP joints in a neutral position and assisting in toe extension. Their weakness allows the extrinsic flexors to pull the toes into the characteristic clawed position.
Question 18
Which of the following is considered a key differentiating factor between a 'flexible' and 'rigid' cavus foot during clinical examination?
Explanation
Correct Answer: B
The ability to passively correct the forefoot and hindfoot deformities is the fundamental differentiator between a flexible and rigid cavus foot. A flexible deformity can be manually corrected to a plantigrade position, indicating that soft tissue releases or tendon transfers may suffice, or that the deformity is driven by a flexible primary deformity (e.g., plantarflexed first ray). A rigid deformity resists passive correction, often necessitating osteotomies or arthrodesis to achieve correction. Callosities, ankle sprains, and plantar fasciitis are common symptoms but do not directly define flexibility or rigidity. Age can be a factor in progression but not a direct measure of rigidity.
Question 19
A 7-year-old child presents with a progressive, unilateral cavus foot. This finding should immediately raise suspicion for which of the following etiologies?
Explanation
Correct Answer: C
While most neurological causes of cavus foot (like CMT and Friedreich's ataxia) are typically bilateral and often symmetric, a unilateral or markedly asymmetric progressive cavus foot strongly suggests an underlying acquired neurological cause, such as a spinal cord tumor, tethered cord syndrome, poliomyelitis, or other localized neurological pathology. It warrants urgent neurological imaging (e.g., MRI of the spine) to rule out compressive or developmental lesions. Idiopathic cavus feet are usually bilateral, and hereditary neuropathies like CMT are systemic and bilateral.
Question 20
In a cavus foot patient with a flexible plantarflexed first ray, what is the biomechanical consequence of attempting to bring the foot flat on the ground during gait?
Explanation
Correct Answer: D
A plantarflexed first ray means the first metatarsal head is lower than the other metatarsal heads. To bring the entire forefoot to the ground, the hindfoot must excessively supinate or invert, resulting in a compensatory hindfoot varus. This creates the characteristic cavovarus deformity. The midtarsal joint also supinates. This mechanism explains why correcting the plantarflexed first ray can resolve the hindfoot varus in flexible cases.
Question 21
Regarding the collagenous architecture of the menisci, which of the following statements most accurately describes the predominant fiber orientation in the main body of the meniscal substance, critical for its biomechanical function?
Explanation
Correct Answer: B
The menisci are primarily composed of type I collagen, with the vast majority (90-95%) of the fibers arranged circumferentially. These longitudinal fibers are crucial for converting vertical compressive loads into 'hoop stresses,' which are then resisted by the integrity of the circumferential fibers, allowing the meniscus to transmit load efficiently and protect articular cartilage. Radial fibers, though fewer, act as 'tie-ropes' to prevent extrusion of the circumferential fibers.
Question 22
Which meniscal structure is considered a secondary stabilizer to anterior tibial translation, particularly in the ACL-deficient knee?
Explanation
Correct Answer: A
The posterior horn of the medial meniscus plays a significant role as a secondary stabilizer to anterior tibial translation. Its posterior root attachment resists anterior displacement of the meniscus itself, and its intact structure prevents excessive anterior translation of the tibia relative to the femur, especially when the ACL is deficient. The posterior horn of the lateral meniscus also contributes but to a lesser degree than the medial.
Question 23
The primary blood supply to the menisci in adults is derived from which arterial network?
Explanation
Correct Answer: A
The primary blood supply to the menisci in adults originates from branches of the inferior genicular arteries (medial and lateral), which form a perimeniscal plexus. This plexus supplies the outer 10-30% of the meniscal tissue, creating the well-known 'red-red' (vascular), 'red-white' (partially vascular), and 'white-white' (avascular) zones.
Question 24
What is the primary role of radial 'tie' fibers within the meniscal substance?
Explanation
Correct Answer: C
While the circumferential fibers bear the hoop stresses, the relatively fewer radial 'tie' fibers act like 'sutures' or 'staples,' connecting the circumferential bundles. Their critical role is to resist meniscal extrusion by preventing the outward bulging and separation of the circumferential fibers under compressive loads, thus maintaining the meniscus's integrity and function.
Question 25
Which meniscal root attachment is considered stronger and has a higher load-to-failure threshold?
Explanation
Correct Answer: C
The posterior horn of the medial meniscus root attachment is biomechanically the strongest, resisting high loads and contributing significantly to posterior stability. Disruption of this root attachment effectively renders the medial meniscus non-functional, leading to biomechanical consequences similar to a total meniscectomy.
Question 26
Loss of meniscal function due to injury or meniscectomy is most directly linked to an increased incidence of:
Explanation
Correct Answer: D
The menisci play a crucial role in load transmission, distributing axial loads over a larger surface area, and thereby reducing peak contact stresses on the articular cartilage. Loss of meniscal function, whether from injury or surgical removal, significantly increases peak contact pressures on the tibial and femoral condyles, leading to progressive degeneration and an increased incidence of tibiofemoral osteoarthritis.
Question 27
The integrity of the posterior root of the medial meniscus is critical because its avulsion effectively leads to:
Explanation
Correct Answer: C
The posterior root attachment of the medial meniscus is essential for anchoring the meniscus and maintaining its circumferential integrity. An avulsion of this root disrupts the 'hoop stress' mechanism, leading to significant medial meniscal extrusion from the joint line. This extrusion effectively renders the meniscus dysfunctional, markedly increasing contact pressures on the medial tibial cartilage, similar to a total meniscectomy, and accelerating osteoarthritic changes.
Question 28
During full knee extension, what percentage of the compressive load across the knee joint is transmitted through the menisci?
Explanation
Correct Answer: C
The menisci transmit a significant portion of the compressive load across the tibiofemoral joint. In full extension, they transmit approximately 50-70% of the load. This percentage increases with flexion, with some studies suggesting up to 85% of load transmission through the menisci in deeper flexion.
Question 29
Which clinical scenario would most strongly suggest an irreparable meniscal tear requiring partial meniscectomy rather than repair?
Explanation
Correct Answer: C
A chronic, complex degenerative tear in the avascular 'white-white zone' of an older patient has the least potential for successful repair. The lack of blood supply, the degenerative nature of the tissue, and the patient's age all contribute to poor healing prospects. In such cases, partial meniscectomy to remove the unstable, symptomatic fragment is typically performed.
Question 30
What is the functional consequence of meniscal extrusion beyond the tibiofemoral joint line?
Explanation
Correct Answer: C
Meniscal extrusion, where the meniscus displaces outward from the tibiofemoral joint space, indicates a loss of its critical 'hoop stress' function. This significantly reduces the meniscus's ability to transmit loads and increase contact area. As a result, peak contact pressures on the articular cartilage increase substantially, accelerating cartilage degeneration and increasing the risk of osteoarthritis.
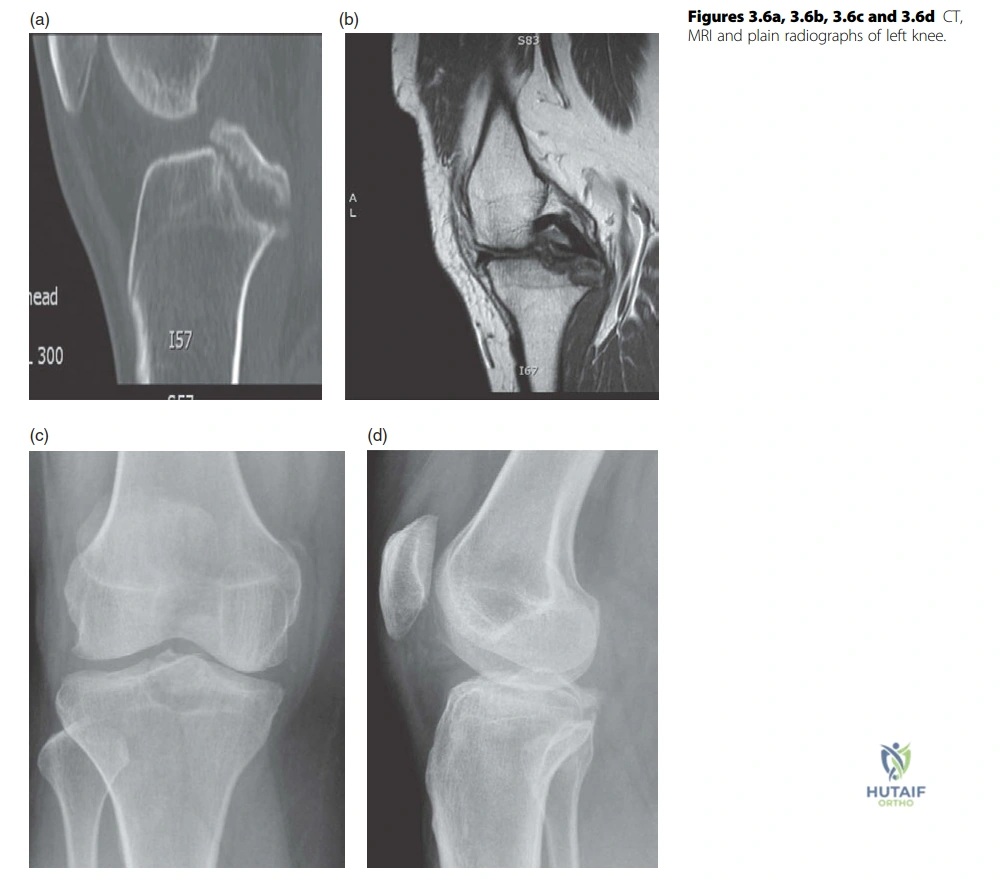
Question 31
A 26-year-old rugby player presents after an awkward fall onto his left knee. Radiographs and MRI, as shown in the provided image, reveal cortical disruption at the PCL insertion with a displaced avulsed fragment. What is the most appropriate initial surgical management for this specific injury?
Explanation
Correct Answer: C
The case explicitly states the candidate's proposed treatment for this patient: "I would offer this patient reattachment of the PCL avulsion through open procedure." This indicates that for a displaced PCL avulsion, direct open reattachment of the bone fragment is the preferred surgical approach. Non-operative management is typically reserved for non-displaced or minimally displaced avulsions. Arthroscopic PCL reconstruction with allograft or PCL repair is generally indicated for mid-substance tears or chronic instability, not acute bony avulsions where direct reattachment is feasible. Staged procedures or debridement are not the primary initial management for a displaced bony avulsion.
Question 32
During a posterior approach to the knee for open reattachment of a PCL avulsion, the popliteal vessels are displaced laterally. Which of the following neurovascular structures is most directly at risk of injury during this maneuver, particularly if ligation of the middle geniculate and superior medial geniculate vessels is required?
Explanation
Correct Answer: E
The case states, "Popliteal vessels are displaced laterally and this usually requires ligation of middle geniculate and superior medial geniculate vessels." The middle and superior medial geniculate vessels are branches of the popliteal artery. Therefore, the maneuver of displacing the popliteal vessels and ligating these specific branches directly involves the popliteal artery, placing it at the most direct risk of injury during this particular step. While the tibial nerve (which lies posterior to the popliteal vein) and other nerves (common peroneal, sural, small saphenous) are generally at risk during a posterior approach, the question specifically highlights the manipulation of the popliteal vessels and ligation of its branches, making the popliteal artery the most pertinent answer in this context.
Question 33
The candidate correctly describes several indications for a posterior approach to the knee. Which of the following conditions would generally not be considered a primary indication for a posterior approach as outlined in the case?
Explanation
Correct Answer: D
The case lists the indications for a posterior approach to the knee, which include: removal of popliteal cysts and neoplasms, posterior synovectomy, open reduction and internal fixation of posterior tibial plateau shear fractures, fixation of bone avulsions associated with a PCL injury, and repair of posterior vascular injuries. Arthroscopic meniscal repair, even for a posterior horn tear, is typically performed arthroscopically through standard portals, not via an open posterior approach as described for these more extensive procedures.
Question 34
During a single-bundle ACL reconstruction on a right knee, the examiner emphasizes the importance of anatomical and isometric tunnel placement. Based on the principles discussed in the case, what is the optimal clock face position for the femoral tunnel to replace the posterolateral bundle?
Explanation
Correct Answer: C
The case explicitly states, "For the femoral tunnel the isometric point lies at about 10 to 10.30 o’clock for right knee and 1.30 to 2 for left knee." The aim in single-bundle reconstruction is to place the tunnel at the footprint of the posterolateral bundle of the ACL, which is considered important to replace. Therefore, 10 to 10:30 o'clock is the optimal position for a right knee.
Question 35
A surgeon performing a single-bundle ACL reconstruction places the femoral tunnel too anteriorly, on the "resident's ridge." According to the case discussion, what is the most likely clinical consequence of this technical error?
Explanation
Correct Answer: C
The case clearly states, "The most common mistake is to place femoral tunnel too anterior or ‘resident’s ridge’. This restricts flexion of the knee and may result in elongation of graft." Conversely, too posterior tunnel placement results in excessive tightening of the graft when the knee is extended. Therefore, an anterior femoral tunnel leads to a restriction of knee flexion.
Question 36
A 35-year-old active patient requires ACL reconstruction and expresses significant concern about developing anterior knee pain post-operatively. Based on the information provided in the case, which autograft choice would be more likely to lead to this specific donor site morbidity?
Explanation
Correct Answer: A
The case discusses the donor site morbidities of BPTB and hamstring grafts. It states that the BPTB graft "has donor site morbidity which includes anterior knee pain in 30–50%, patellar tendonitis 3–5%, patellar fracture and patella baja." In contrast, the hamstring graft "has less donor site morbidity." Therefore, a BPTB graft is more likely to cause anterior knee pain post-operatively compared to a hamstring graft.
Question 37
While discussing the potential complications of a hamstring four-strand autograft for ACL reconstruction, the candidate mentions hamstring weakness. What other specific nerve injury is cited in the case as a potential donor site morbidity associated with hamstring graft harvest?
Explanation
Correct Answer: D
The case explicitly lists the potential complications of hamstring graft harvest, stating, "It can also result in hamstring weakness and saphenous nerve injury." The saphenous nerve runs in close proximity to the hamstring tendons during harvest, making it susceptible to injury.
Question 38
The case focuses on the treatment of a PCL avulsion injury. How does the initial surgical management described for this specific injury typically differ from the management of a chronic mid-substance PCL tear?
Explanation
Correct Answer: B
The case describes the treatment for a PCL avulsion as "reattachment of the PCL avulsion through open procedure." This implies direct fixation of the avulsed bone fragment back to its origin. In contrast, a chronic mid-substance PCL tear, where the ligament itself is torn and not amenable to direct repair, typically requires a formal PCL reconstruction using a graft (autograft or allograft) to recreate the ligament. Therefore, avulsions are often treated with direct reattachment, while mid-substance tears require reconstruction.
Question 39
During an arthroscopic ACL reconstruction, after careful assessment, the surgeon notes that abnormally narrow intercondylar notch correlates with increased incidence of ACL tears. If impingement on the lateral femoral condyle is identified despite correct tunnel placement, what additional surgical step is indicated according to the case?
Explanation
Correct Answer: C
The case explicitly addresses this scenario: "Careful assessment of notch should be done prior to graft insertion using a pin to ensure no impingement on lateral femoral condyle. The presence of impingement with correct placement of tunnels necessitates notchplasty of the anterior portion of lateral femoral condyle." This procedure aims to widen the notch to prevent graft impingement, which can lead to graft failure.
Question 40
When performing a posterior approach to the knee, the candidate describes the relative anatomical positions of key neurovascular structures in the popliteal fossa. From deepest to most superficial, what is the correct order of the popliteal artery, popliteal vein, and tibial nerve?
Explanation
Correct Answer: A
The case describes the anatomical relationship of these structures in the popliteal fossa: "The tibial nerve lies posterior to the popliteal vein which in turn is superficial to popliteal artery." This means the popliteal artery is the deepest structure, followed by the popliteal vein, and then the tibial nerve is the most superficial of these three structures.
Question 41
A 72-year-old female presents with pseudoparalysis of the shoulder and advanced cuff tear arthropathy. A reverse total shoulder arthroplasty (rTSA) is planned. Which of the following best describes the biomechanical principle of a standard Grammont-style reverse shoulder arthroplasty?
Explanation
Question 42
A 24-year-old football player sustains a hyperplantarflexion injury to his midfoot. Radiographs demonstrate a 'fleck sign' in the first intermetatarsal space. The torn ligament responsible for this finding originates from and attaches to which of the following structures?
Explanation
Question 43
A 21-year-old female soccer player undergoes primary anterior cruciate ligament (ACL) reconstruction. During the healing process, the graft requires a robust blood supply to properly undergo ligamentization. What is the primary arterial supply to the native ACL?
Explanation
Question 44
A 28-year-old male with recurrent anterior shoulder instability is noted to have a 25% anterior glenoid bone loss and an engaging Hill-Sachs lesion. If a Remplissage procedure were to be performed in conjunction with an arthroscopic Bankart repair for a smaller glenoid defect, which of the following best describes the Remplissage technique?
Explanation
Question 45
A 45-year-old female presents with a painful bunion deformity. Weight-bearing radiographs reveal a hallux valgus angle (HVA) of 28 degrees and an intermetatarsal angle (IMA) of 12 degrees. There is no hypermobility of the first tarsometatarsal joint. Which of the following is the most appropriate surgical indication for a distal chevron osteotomy?
Explanation
Question 46
During a total knee arthroplasty (TKA) on a 68-year-old female with a severe 25-degree valgus deformity, extensive lateral releases are required to balance the knee. Postoperatively, she exhibits a foot drop. Which of the following is the most likely cause of this complication?
Explanation
Question 47
A 35-year-old manual laborer sustains a Type III acromioclavicular (AC) joint separation. The coracoclavicular (CC) ligaments are completely ruptured. Which of the following describes the correct anatomic orientation of the native CC ligaments?
Explanation
Question 48
A 32-year-old male sustains a Hawkins Type II talar neck fracture. He is at significant risk for avascular necrosis (AVN) of the talar body. What is the primary blood supply to the talar body that is disrupted in this injury?
Explanation
Question 49
A 19-year-old male presents to the emergency department after a twisting injury to his knee while skiing. MRI confirms an acute, isolated rupture of the anterior cruciate ligament (ACL). Which of the following meniscal injuries is statistically most likely to be associated with this acute tear?
Explanation
Question 50
A 22-year-old cyclist falls and sustains a displaced midshaft clavicle fracture. Which of the following represents an absolute indication for operative fixation of this fracture?
Explanation
Question 51
A 45-year-old roofer falls from a ladder and sustains an intra-articular calcaneus fracture. You are reviewing his CT scan to determine the Sanders classification. Which specific imaging plane is used to define the Sanders classification?
Explanation
Question 52
A 30-year-old male is brought to the trauma bay after a high-speed motorcycle collision. He has a grossly unstable knee with multi-ligamentous injury (KD-III). After reduction, his distal pulses are palpable, but his Ankle-Brachial Index (ABI) is 0.8. What is the most appropriate next step in management?
Explanation
Question 53
A 22-year-old collegiate baseball pitcher presents with vague shoulder pain and decreased throwing velocity. Physical examination reveals Glenohumeral Internal Rotation Deficit (GIRD) of 25 degrees compared to the contralateral side. What is the primary anatomic pathology responsible for this physical finding?
Explanation
Question 54
A 55-year-old male sustains an acute Achilles tendon rupture while playing tennis. He is treated non-operatively in a functional rehabilitation brace. Most Achilles tendon ruptures occur in a hypovascular 'watershed' zone. Where is this zone anatomically located?
Explanation
Question 55
A 17-year-old female presents with recurrent lateral patellar dislocations. An MPFL (medial patellofemoral ligament) reconstruction is planned. To ensure isometric graft function, the femoral tunnel must be placed at Schottle's point. Where is this point located radiographically?
Explanation
Question 56
A 48-year-old construction worker presents with deep, aching shoulder pain. MR arthrogram demonstrates a Type II SLAP tear. Given his age and occupation, which of the following treatments has been shown to provide the most reliable return to work and pain relief?
Explanation
Question 57
A 60-year-old overweight female complains of medial foot pain and a collapsed arch. On examination, she has a flexible pes planus deformity and cannot perform a single-leg heel rise. Which of the following is the standard surgical treatment for this Stage II posterior tibial tendon dysfunction (PTTD)?
Explanation
Question 58
A 45-year-old male sustains a Schatzker Type II tibial plateau fracture after a fall from a height. This fracture pattern involves a split-depression of the lateral plateau. What is the most frequently associated soft tissue injury that should be evaluated during surgical fixation?
Explanation
Question 59
A 50-year-old male presents with acute shoulder pain and weakness after attempting to catch a falling heavy box.
Physical examination reveals a positive Bear-Hug test. Which of the following muscles is most likely injured?
Explanation
Question 60
A 70-year-old male presents with severe shoulder pain and an inability to actively elevate his arm above 40 degrees. Radiographs demonstrate superior migration of the humeral head with severe glenohumeral osteoarthritis. A subsequent MRI confirms a massive, retracted, irreparable tear of the supraspinatus and infraspinatus tendons with fatty infiltration. Which of the following is the most appropriate surgical management?
Explanation
Question 61
A 24-year-old male undergoes arthroscopic anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Postoperatively, he achieves full extension but complains of severe stiffness and restricted flexion, with a firm endpoint at 90 degrees. What is the most likely technical error responsible for this complication?
Explanation
Question 62
A 55-year-old poorly controlled diabetic male presents with a painless, erythematous, and significantly swollen left foot. He is afebrile with bounding pedal pulses. Radiographs show soft tissue swelling, periarticular debris, and early subluxation of the tarsometatarsal joints. What is the most appropriate initial management?
Explanation
Question 63
A 21-year-old collegiate rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals 28% bone loss of the anteroinferior glenoid. Which of the following surgical procedures is most appropriate to prevent recurrent dislocation?
Explanation
Question 64
A patient presents with posterolateral knee pain and instability after a hyperextension injury. On physical examination, the dial test shows 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side, but symmetric rotation at 90 degrees of flexion. Which structure is most likely injured?
Explanation
Question 65
During closed reduction of a subtle Lisfranc injury in a 30-year-old male, the surgeon notes widening between the medial and middle cuneiforms. The Lisfranc ligament provides crucial stability to the midfoot. What are the true anatomical attachments of the Lisfranc ligament?
Explanation
Question 66
An orthopedic surgeon is performing a deltoid-splitting approach for an open rotator cuff repair. To avoid denervating the anterior deltoid, the split must not extend too far distally. What is the approximate safe distance from the lateral edge of the acromion before risking injury to the axillary nerve?
Explanation
Question 67
A 55-year-old female undergoes MRI of the knee showing a complete radial tear adjacent to the posterior root attachment of the medial meniscus. If left untreated, the biomechanical consequence of this specific tear is most equivalent to which of the following?
Explanation
Question 68
A 42-year-old male presents with a palpable gap in his posterior ankle following a sudden acceleration while playing tennis. He is diagnosed with an acute Achilles tendon rupture. The tear occurred in the 'watershed' area of the tendon. How far proximal to the calcaneal insertion is this zone typically located?
Explanation
Question 69
A 28-year-old professional volleyball player presents with insidious onset posterior shoulder pain. Examination reveals profound weakness in external rotation, but normal forward elevation and abduction. An MRI shows an isolated paralabral cyst in the spinoglenoid notch. Which nerve is compressed, and which muscle is consequently affected?
Explanation
Question 70
A 16-year-old female requires medial patellofemoral ligament (MPFL) reconstruction for recurrent lateral patellar dislocations. Intraoperative fluoroscopy is used to determine the anatomic femoral attachment of the MPFL (Schottle's point). Where is this point located radiographically?
Explanation
Question 71
A 62-year-old female presents with severe pain and stiffness at the base of her great toe. Radiographs demonstrate end-stage hallux rigidus (Coughlin Grade 4). She elects to undergo a first metatarsophalangeal (MTP) joint arthrodesis. What is the optimal position for fusing the first MTP joint?
Explanation
Question 72
A 34-year-old bodybuilder feels a sudden 'pop' and tearing sensation in his anterior chest/shoulder while performing a heavy bench press. Examination reveals loss of the anterior axillary fold. If surgical repair is pursued, where is the most common site of failure that requires reattachment?
Explanation
Question 73
During a total knee arthroplasty (TKA), the surgeon checks the gap balancing. The knee is stable and symmetric in full extension, but tight in both medial and lateral compartments at 90 degrees of flexion. Which of the following adjustments is the most appropriate next step to correct this mismatch?
Explanation
Question 74
A 22-year-old basketball player sustains a fracture at the base of the fifth metatarsal. Radiographs show a transverse fracture at the metaphyseal-diaphyseal junction (Zone 2), extending into the fourth-fifth intermetatarsal facet. What is the primary reason this specific fracture is at a high risk for nonunion?
Explanation
Question 75
A 28-year-old male sustains a severe traction injury to his right shoulder in a motorcycle accident. Examination reveals a completely flail arm, laterally displaced scapula, and massive swelling. Radiographs show a displaced clavicle fracture and acromioclavicular separation. This constellation of findings (scapulothoracic dissociation) carries the highest risk for which of the following concomitant injuries?
Explanation
Question 76
A 25-year-old male twists his knee while playing soccer. His radiograph shows an elliptic bone fragment avulsed from the lateral tibial plateau, distal to the joint line. This 'Segond fracture' is considered pathognomonic for an anterior cruciate ligament (ACL) tear. Which structural avulsion is responsible for this radiographic finding?
Explanation
Question 77
A 45-year-old roofer falls from a height and sustains an intra-articular calcaneus fracture. The Sanders classification is commonly used for surgical planning. On which specific radiographic view and anatomical landmark is the Sanders classification based?
Explanation
Question 78
A 45-year-old recreational tennis player presents with persistent anterior shoulder pain and clicking. An MRI arthrogram reveals a Type II SLAP (Superior Labrum Anterior and Posterior) tear. After 6 months of failed physical therapy, surgery is planned. What is the most appropriate surgical treatment for this patient?
Explanation
Question 79
A 30-year-old male sustains a high-energy knee dislocation (KD-III). The knee is reduced in the emergency department. His foot is warm, but pedal pulses are asymmetrical. An Ankle-Brachial Index (ABI) is measured. At what ABI threshold is a CT angiogram (CTA) strictly indicated to rule out a popliteal artery injury?
Explanation
Question 80
In reverse total shoulder arthroplasty, how does the design fundamentally alter the glenohumeral joint's biomechanics compared to a native shoulder to compensate for a deficient rotator cuff?
Explanation
Question 81
A 25-year-old athlete sustains a direct blow to the anteromedial tibia. Examination reveals 15 degrees of increased external rotation of the tibia compared to the contralateral side at both 30 degrees and 90 degrees of knee flexion. Which of the following injury patterns is most likely present?
Explanation
Question 82
A 21-year-old collegiate basketball player sustains an acute diaphyseal-metaphyseal junction fracture of the fifth metatarsal. He wishes to return to play as safely and quickly as possible. What is the most appropriate management?
Explanation
Question 83
During reconstruction of the medial patellofemoral ligament (MPFL) for recurrent patellar instability, the femoral attachment must be anatomically placed to avoid altering joint kinematics. Where is the native femoral origin of the MPFL located?
Explanation
Question 84
A 28-year-old male volleyball player presents with insidious onset of posterior shoulder pain and isolated weakness in external rotation. An MRI reveals a paralabral cyst. Where is this cyst most likely located, and what nerve is compressed?
Explanation
Question 85
A 24-year-old female sustains a severe midfoot twisting injury. Radiographs show a widened space between the bases of the 1st and 2nd metatarsals with no obvious avulsion fractures. MRI confirms a complete tear of the Lisfranc ligament. What is the most appropriate surgical treatment?
Explanation
Question 86
An 18-year-old skier sustains a twisting injury to the knee. An AP radiograph demonstrates a small vertical avulsion fracture of the lateral tibial plateau. Which of the following intra-articular injuries is most highly associated with this radiographic finding?
Explanation
Question 87
A 22-year-old male presents with recurrent anterior shoulder dislocations. A 3D CT scan reveals a 25 percent defect of the anterior glenoid rim. What is the most appropriate surgical procedure to restore lasting stability?
Explanation
Question 88
A 30-year-old male sustains a Hawkins Type III talar neck fracture following a motor vehicle collision. Which of the following radiographic findings at 6 to 8 weeks post-injury would indicate a good prognosis regarding the vascularity of the talar body?
Explanation
Question 89
A 55-year-old woman presents with acute medial knee pain after a deep squat. MRI reveals a complete posterior root tear of the medial meniscus with 4 mm of meniscal extrusion. What is the biomechanical consequence of leaving this tear untreated?
Explanation
Question 90
A 48-year-old construction worker presents with chronic anterior shoulder pain exacerbated by heavy lifting. MRI arthrogram shows a Type II SLAP tear. Six months of physical therapy has failed to provide relief. What is the surgical treatment of choice?
Explanation
None
