Master Orthopedic Board Review: Bone Tumors & Metabolic Diseases - Lymphoma, MPS, CMF | Part 11
20 Jun 2026
48 min read
37 Views
Key Takeaway
This orthopedic board review covers key bone pathologies including primary lymphoma of bone, mucopolysaccharidoses (Hurler, Morquio syndromes), chondromyxoid fibroma, and Camurati-Engelmann disease. It details clinical presentations, imaging, histology, and genetics for comprehensive exam preparation in musculoskeletal oncology and metabolic bone disorders.
Master Orthopedic Board Review: Bone Tumors & Metabolic Diseases - Lymphoma, MPS, CMF | Part 11
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
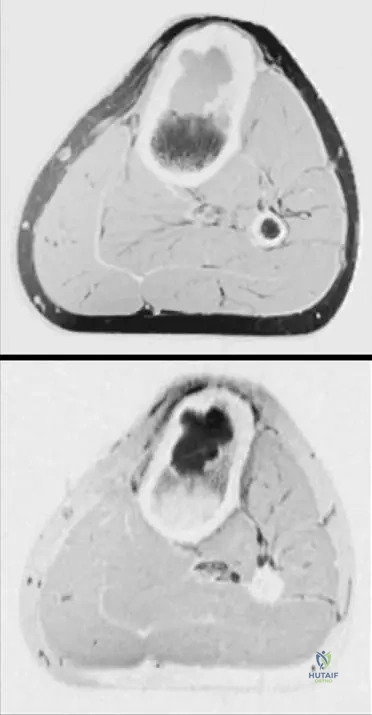
A 22-year-old male presents with chronic, mild knee pain. Radiographs reveal an eccentric, sharply circumscribed, osteolytic lesion with a sclerotic rim in the proximal tibial metaphysis.
What is the most characteristic histological finding for this lesion?
What is the most characteristic histological finding for this lesion?
Explanation
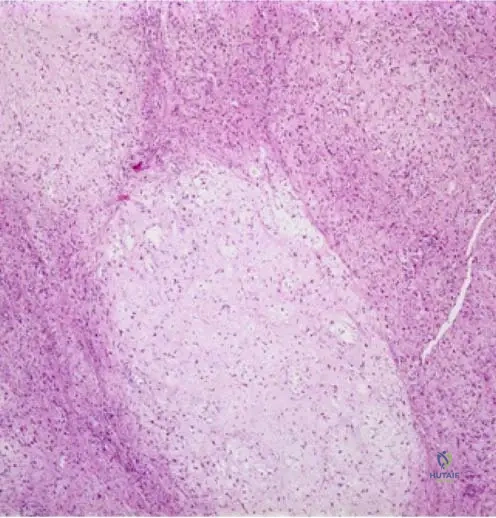
The clinical and radiographic features describe a Chondromyxoid Fibroma (CMF). Histologically, CMF is characterized by a lobular architecture with stellate or spindle cells in a myxoid background, and hypercellularity at the periphery of the lobules.
Question 2
Regarding the management of the lesion described in the previous question (Chondromyxoid Fibroma), which of the following represents the standard of care with the lowest recurrence rate while preserving joint function?
Explanation
CMF is a benign but locally aggressive tumor. Extended intralesional curettage (using a high-speed burr and/or phenol) followed by bone grafting or PMMA cementation is the standard treatment, yielding low recurrence rates.
Question 3
A 65-year-old male complains of progressive thigh pain. Radiographs demonstrate a large, permeative, moth-eaten osteolytic lesion in the femoral diaphysis with minimal periosteal reaction.
Biopsy reveals sheets of large atypical cells. Which immunohistochemical marker profile confirms the most common histological subtype of this disease?
Biopsy reveals sheets of large atypical cells. Which immunohistochemical marker profile confirms the most common histological subtype of this disease?

Explanation
Primary bone lymphoma is most commonly Diffuse Large B-Cell Lymphoma (DLBCL). The tumor cells will be positive for B-cell markers (CD20) and leukocyte common antigen (CD45), but negative for T-cell markers (CD3).
Question 4
A 55-year-old female is diagnosed with primary bone lymphoma of the proximal humerus. Staging shows no visceral or lymph node involvement. The cortex is thinned, but there is no impending fracture. What is the most appropriate initial treatment?
Explanation
Primary bone lymphoma is highly responsive to non-operative treatment. Multiagent chemotherapy (e.g., CHOP or R-CHOP) combined with radiotherapy is the standard of care, reserving surgery strictly for actual or impending pathological fractures.
Question 5
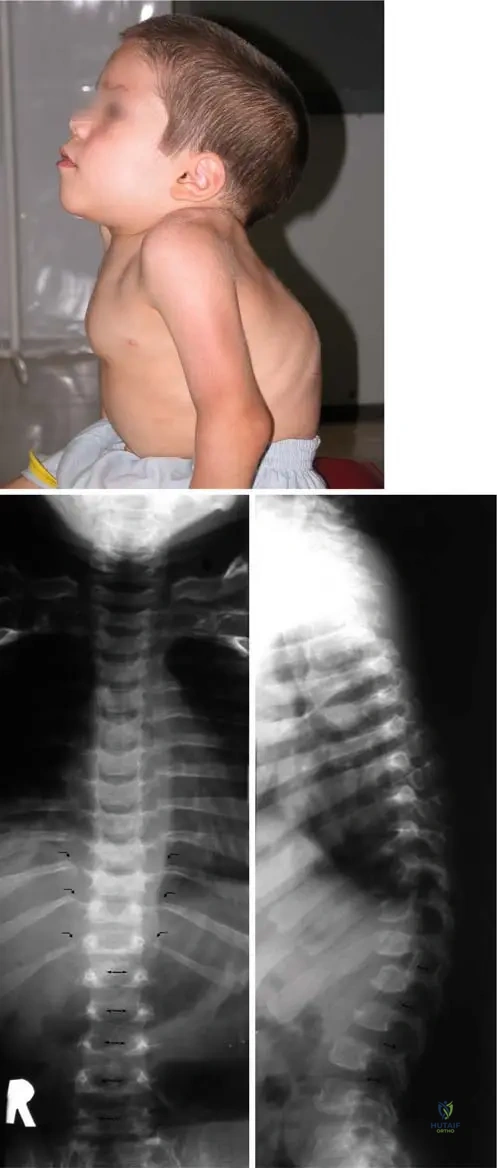
A 9-year-old boy with normal intelligence presents with short stature, severe genu valgum, and a barrel chest.
He reports recent clumsy gait and tingling in his hands. What is the most critical radiographic evaluation required immediately?
He reports recent clumsy gait and tingling in his hands. What is the most critical radiographic evaluation required immediately?
Explanation
The patient has Morquio syndrome (MPS IV), characterized by normal intelligence, severe skeletal dysplasia, and marked ligamentous laxity. Odontoid hypoplasia is a hallmark, and a clumsy gait suggests cervical myelopathy from atlantoaxial instability, requiring urgent flexion-extension C-spine films or MRI.
Question 6
Which specific biochemical deficiency is responsible for the clinical presentation of Morquio A syndrome (MPS IVA)?
Explanation
Morquio A syndrome (MPS IVA) is caused by a deficiency in N-acetylgalactosamine-6-sulfatase, leading to the accumulation of keratan sulfate. Morquio B is caused by beta-galactosidase deficiency.
Question 7
A 14-year-old girl presents with severe bilateral leg pain, weakness, and a waddling gait. Radiographs display profound cortical thickening of the bilateral femoral and tibial diaphyses, sparing the epiphyses.
What is the underlying genetic mutation associated with this condition?
What is the underlying genetic mutation associated with this condition?

Explanation
The clinical and radiographic presentation is classic for Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease). This condition is inherited in an autosomal dominant pattern due to mutations in the TGFB1 gene.
Question 8
In a patient with confirmed Camurati-Engelmann disease experiencing significant, debilitating bone pain, what is the most effective first-line medical therapy?
Explanation
Systemic corticosteroids are the mainstay of medical treatment for Camurati-Engelmann disease. They are highly effective at relieving the severe bone pain and can sometimes improve the waddling gait and radiographic appearance.
Question 9
Which of the following Mucopolysaccharidoses (MPS) disorders is inherited in an X-linked recessive pattern?
Explanation
Hunter syndrome (MPS II) is the only mucopolysaccharidosis that is inherited in an X-linked recessive pattern. All other MPS disorders are inherited in an autosomal recessive manner.
Question 10
Which of the following demographic and radiographic features best distinguishes Chondromyxoid Fibroma (CMF) from Chondroblastoma?
Explanation
While both are benign cartilage tumors of young adults, CMF typically arises in the metaphysis (often eccentrically), whereas chondroblastoma almost exclusively arises in the epiphysis or apophysis.
Question 11
When evaluating a bone biopsy for a suspected primary bone lymphoma, what morphological and immunohistochemical characteristic most reliably excludes Ewing sarcoma?
Explanation
Primary bone lymphoma (typically Diffuse Large B-cell Lymphoma) strongly expresses CD45 (LCA), which distinguishes it from Ewing sarcoma. Both can sometimes stain positive for CD99, making LCA a critical differentiating marker.
Question 12
A 3-year-old child presents with coarse facial features, severe corneal clouding, hepatosplenomegaly, and a prominent thoracolumbar kyphosis (gibbus deformity). Which accumulated glycosaminoglycans are most likely to be found in the urine?
Explanation
The presentation is classic for Hurler syndrome (MPS I), caused by alpha-L-iduronidase deficiency. This leads to the accumulation and urinary excretion of both dermatan sulfate and heparan sulfate.
Question 13
A pathologist is reviewing a biopsy of an eccentric, lytic proximal tibial lesion. To confidently differentiate Chondromyxoid Fibroma (CMF) from a low-grade Chondrosarcoma, which key histological feature of CMF should be identified?
Explanation
A defining histologic feature of Chondromyxoid Fibroma is its lobular pattern with distinct hypercellularity at the periphery of the lobules. In contrast, chondrosarcomas typically show central hypercellularity within the lobules and invasive permeation of host bone.
Question 14
A patient with newly diagnosed Primary Bone Lymphoma of the femur asks about their general prognosis and presentation. Which of the following statements is most characteristic of this disease?
Explanation
A classic hallmark of Primary Bone Lymphoma is that patients frequently appear systemically well and report relatively mild pain, despite imaging that shows dramatic, permeative, "moth-eaten" bone destruction.
Question 15
A 10-year-old with Morquio syndrome requires surgical intervention for lower extremity deformity.
What is the most common lower extremity angular deformity seen in these patients?
What is the most common lower extremity angular deformity seen in these patients?
Explanation
Severe genu valgum (knock-knees) is the most common lower extremity deformity in Morquio syndrome (MPS IV), often resulting from ligamentous laxity and metaphyseal dysplasia, frequently requiring surgical correction via guided growth or osteotomy.
Question 16
In a patient with Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease), which of the following extra-appendicular manifestations is most commonly responsible for significant morbidity?
Explanation
In Camurati-Engelmann disease, hyperostosis can extend beyond the long bone diaphyses to involve the skull base. Sclerosis of the neural foramina frequently leads to entrapment neuropathies, causing hearing loss, vision loss, or facial nerve palsy.
Question 17
Which of the following radiographic findings is most characteristic of "dysostosis multiplex," the constellation of skeletal abnormalities seen in patients with Mucopolysaccharidoses?
Explanation
Dysostosis multiplex encompasses the skeletal manifestations of MPS, classically presenting with bullet-shaped hypoplastic vertebrae (leading to gibbus), oar-shaped (spatulate) ribs, J-shaped sella turcica, and thickened clavicles.
Question 18
Which of the following demographic profiles best represents the peak incidence for the development of Chondromyxoid Fibroma?
Explanation
Chondromyxoid fibroma is a rare benign tumor that predominantly affects young adults in their second and third decades of life (teens to 20s), with a slight male predominance.
Question 19
A 52-year-old male presents with a permeative lytic lesion in the distal femur. Biopsy confirms primary bone lymphoma. Which of the following staging studies is most appropriate to confirm this is a primary bone lymphoma rather than metastatic systemic lymphoma?
Explanation
To diagnose Primary Bone Lymphoma, one must rule out systemic lymphoma that has simply metastasized to bone. Staging requires a PET-CT and bone marrow biopsy; primary bone lymphoma implies the lesion is limited to the bone (with or without regional lymph node involvement) for at least 6 months.
Question 20
A 12-year-old patient with known Hurler syndrome presents for orthopedic evaluation. Which of the following upper extremity abnormalities is a hallmark finding of this specific condition?
Explanation
Patients with Hurler syndrome (MPS I) commonly develop severe joint contractures, particularly manifesting in the hands as trigger digits or a claw-hand deformity due to glycosaminoglycan deposition in the flexor tendons and joint capsules.
Question 21
A 45-year-old man presents with knee pain. Radiographs show a permeative lytic lesion in the distal femur. MRI reveals extensive marrow involvement and a large soft-tissue mass.
Biopsy demonstrates sheets of large round cells. Which of the following immunohistochemical markers is most likely to be positive in this lesion?
Biopsy demonstrates sheets of large round cells. Which of the following immunohistochemical markers is most likely to be positive in this lesion?

Explanation
Primary bone lymphoma is most commonly Diffuse Large B-Cell Lymphoma (DLBCL), which stains positive for CD20 and CD45 (LCA). CD99 is typically positive in Ewing sarcoma, while cytokeratin indicates metastatic carcinoma.
Question 22
A 6-year-old child with normal intelligence presents with short stature, severe knock-knees, and a waddling gait. Radiographs reveal platyspondyly and a hypoplastic odontoid.
Which of the following enzyme deficiencies is the primary cause of this condition?
Which of the following enzyme deficiencies is the primary cause of this condition?
Explanation
The patient has Morquio syndrome (MPS IV), characterized by normal intelligence, severe skeletal dysplasia (platyspondyly, odontoid hypoplasia), and joint laxity. It is caused by a deficiency of N-acetylgalactosamine-6-sulfatase (Type A) or Beta-galactosidase (Type B).
Question 23
A 62-year-old male presents with deep, aching thigh pain. Radiographs reveal a permeative, moth-eaten lytic lesion in the femoral diaphysis. Biopsy demonstrates sheets of monotonous, small-to-medium round blue cells with prominent nucleoli and scant cytoplasm. Immunohistochemistry is strongly positive for CD20 and CD45, and negative for CD99. What is the most likely diagnosis?
Explanation
Primary bone lymphoma (most commonly Diffuse Large B-Cell Lymphoma) presents as a permeative lytic lesion in older adults. Immunohistochemistry typically shows positivity for CD45 (LCA) and B-cell markers like CD20, distinguishing it from Ewing sarcoma (CD99+) and myeloma (CD138+).
Question 24
A 6-year-old boy with normal intelligence presents with severe genu valgum, short trunk dwarfism, and a waddling gait. Radiographs reveal platyspondyly with central anterior beaking of the vertebrae and severe odontoid hypoplasia. Urine spot testing is positive for keratan sulfate. Which enzyme is most likely deficient in this patient?
Explanation
The clinical presentation of normal intelligence, severe skeletal dysplasia, atlantoaxial instability, central vertebral beaking, and keratan sulfate accumulation is classic for Morquio syndrome A (MPS IVA). This is caused by a deficiency of the enzyme galactosamine-6-sulfatase.
Question 25
A 22-year-old male presents with persistent anterior leg pain. Radiographs show an eccentric, radiolucent lesion in the proximal tibial metaphysis with a well-defined sclerotic rim.
Histological examination reveals a lobular architecture with spindle and stellate-shaped cells in a myxoid background, with osteoclast-like giant cells clustered at the lobular peripheries. What is the recommended treatment?
Histological examination reveals a lobular architecture with spindle and stellate-shaped cells in a myxoid background, with osteoclast-like giant cells clustered at the lobular peripheries. What is the recommended treatment?
Explanation
The clinical, radiographic, and histologic findings (lobular pattern, stellate cells, myxoid stroma, peripheral giant cells) are diagnostic of Chondromyxoid Fibroma (CMF). The standard treatment for this locally aggressive benign tumor is extended intralesional curettage (with a high-speed burr) and bone grafting or cementing.
Question 26
A 65-year-old male presents with deep thigh pain. Radiographs reveal a permeative, destructive lesion in the femoral diaphysis with minimal periosteal reaction.
Biopsy shows sheets of atypical lymphoid cells. Which of the following is the most likely diagnosis?
Biopsy shows sheets of atypical lymphoid cells. Which of the following is the most likely diagnosis?
Explanation
Primary bone lymphoma, most commonly diffuse large B-cell lymphoma (DLBCL), typically presents in older adults as a permeative lytic lesion with minimal periosteal reaction. Biopsy demonstrating lymphoid cells confirms the diagnosis.
Question 27
A 55-year-old man presents with severe thigh pain. Radiographs appear largely unremarkable, but MRI demonstrates extensive diaphyseal marrow replacement. Biopsy shows sheets of round cells.
Which immunohistochemical marker is most diagnostic for the most likely condition?
Which immunohistochemical marker is most diagnostic for the most likely condition?
Explanation
Primary bone lymphoma is typically a diffuse large B-cell lymphoma, which strongly expresses CD20 and CD45 (LCA). CD99 is typically positive in Ewing sarcoma, while S-100 is seen in neural tumors and chondroid lesions.
Question 28
A 6-year-old boy with short trunk dwarfism and normal intelligence presents for evaluation. Radiographs demonstrate severe platyspondyly, anterior central vertebral beaking, and odontoid hypoplasia. What is the underlying enzyme deficiency?
Explanation
The clinical picture describes Morquio syndrome (MPS IV), uniquely characterized by normal intelligence, severe platyspondyly, and odontoid hypoplasia. It is caused by a deficiency in N-acetylgalactosamine-6-sulfate sulfatase (Type IVA) or beta-galactosidase (Type IVB).
Question 29
A 22-year-old man presents with chronic knee pain. Radiographs reveal an eccentric, lytic, metaphyseal lesion with a sclerotic margin in the proximal tibia. Histology shows lobules of myxoid and chondroid tissue with multinucleated giant cells at the periphery.
What is the most appropriate definitive management?
What is the most appropriate definitive management?
Explanation
The diagnosis is Chondromyxoid fibroma (CMF), a benign but locally aggressive cartilage tumor. Simple curettage has an unacceptably high recurrence rate (up to 25-80% in older literature), making extended curettage with a high-speed burr and bone grafting the preferred treatment.
Question 30
A 10-year-old girl presents with a waddling gait, severe leg pain, and proximal muscle weakness. Radiographs demonstrate bilateral, symmetrical cortical thickening of the femoral and tibial diaphyses, sparing the epiphyses.
Which genetic mutation is associated with this condition?
Which genetic mutation is associated with this condition?

Explanation
The presentation is classic for Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease), characterized by symmetrical diaphyseal sclerosis and muscle weakness. It is an autosomal dominant condition caused by mutations in the TGFB1 gene.
Question 31
Mucopolysaccharidoses (MPS) are a group of lysosomal storage disorders. Which of the following features uniquely distinguishes Hunter syndrome (MPS II) from Hurler syndrome (MPS I)?
Explanation
Hunter syndrome (MPS II) is uniquely inherited in an X-linked recessive manner, unlike the other MPS types which are autosomal recessive. Furthermore, patients with Hunter syndrome typically do not develop the severe corneal clouding seen in Hurler syndrome.
Question 32
A 50-year-old woman is diagnosed with localized diffuse large B-cell primary lymphoma of the distal femur. There is no cortical breakthrough and no impending fracture. What is the most appropriate initial management?
Explanation
Primary bone lymphoma is highly responsive to non-operative treatment. Standard of care includes systemic multi-agent chemotherapy (such as CHOP) combined with local involved-field radiation therapy, reserving surgery strictly for impending or actual pathologic fractures.
Question 33
An intraoperative frozen section of a lytic femoral lesion in a 55-year-old male demonstrates sheets of small round blue cells. The pathologist suspects primary bone lymphoma. What is the most critical step regarding the handling of the remaining biopsy specimen to confirm this diagnosis?
Explanation
Fresh tissue is required for flow cytometry and cytogenetic analysis, which are essential for definitively diagnosing and subtyping lymphoma. Putting the entire sample in formalin or decalcifying it will destroy cell surface markers needed for flow cytometry.
Question 34
A 48-year-old male presents with knee pain. Imaging reveals a diaphyseal permeative lesion in the distal femur. A biopsy is performed, and immunohistochemistry is positive for CD20 and CD45, and negative for CD99 and CD138. What is the most likely diagnosis?
Explanation
The immunohistochemical profile of primary bone lymphoma (usually Diffuse Large B-Cell Lymphoma) is positive for CD45 (Leukocyte Common Antigen) and CD20 (B-cell marker). Ewing sarcoma is CD99 positive, while multiple myeloma is CD138 positive.
Question 35
A 60-year-old female is diagnosed with primary diffuse large B-cell lymphoma of the proximal humerus without cortical breakthrough or impending fracture. What is the gold standard initial treatment?
Explanation
Primary bone lymphoma is highly sensitive to chemotherapy and radiation. Surgery is strictly reserved for actual or impending pathologic fractures, not for primary local tumor control.
Question 36
A 50-year-old male presents with insidious thigh pain. Radiographs appear largely normal, but an MRI is obtained.
Which of the following MRI features is considered classic for primary bone lymphoma?
Which of the following MRI features is considered classic for primary bone lymphoma?
Explanation
A hallmark of primary bone lymphoma is massive marrow involvement and soft tissue extension through cortical channels, producing minimal to no gross cortical bone destruction on plain radiographs.
Question 37
A 6-year-old boy with a known diagnosis of Morquio syndrome (MPS IV) presents for orthopedic evaluation. Which of the following screening examinations is most critical to prevent a catastrophic complication in this patient?
Explanation
Morquio syndrome is classically associated with odontoid hypoplasia and ligamentous laxity, leading to severe atlantoaxial instability. Flexion-extension C-spine radiographs are critical to screen for impending cervical myelopathy.
Question 38
While most mucopolysaccharidoses (MPS) are inherited in an autosomal recessive pattern, which of the following is inherited in an X-linked recessive manner?
Explanation
Hunter syndrome (MPS II) is the only mucopolysaccharidosis with an X-linked recessive inheritance pattern. All other MPS disorders are autosomal recessive.
Question 39
A 4-year-old girl is being evaluated for skeletal dysplasia. A hand radiograph is obtained.
What is the classic finding demonstrated in the hands of patients with Hurler syndrome (MPS I)?
What is the classic finding demonstrated in the hands of patients with Hurler syndrome (MPS I)?
Explanation
Dysostosis multiplex is the constellation of radiographic findings in MPS. In the hand, this typically presents as bullet-shaped phalanges and proximal pointing of the metacarpals.
Question 40
Morquio A syndrome (MPS IVA) is primarily caused by a deficiency in which of the following enzymes?
Explanation
Morquio A syndrome results from a deficiency of galactose-6-sulfatase (GALNS), leading to the accumulation of keratan sulfate and chondroitin-6-sulfate. Alpha-L-iduronidase is deficient in Hurler syndrome.
Question 41
What is the characteristic spinal deformity finding associated with Hurler syndrome (MPS I)?
Explanation
Hurler syndrome typically presents with anteroinferior beaking of the vertebral bodies, leading to thoracolumbar kyphosis. In contrast, Morquio syndrome classically presents with central anterior beaking.
Question 42
A biopsy of an eccentric, lytic metaphyseal lesion in a 25-year-old male shows a lobular architecture with stellate and spindle-shaped cells in a myxoid and chondroid background. Multinucleated giant cells are present at the lobular periphery. What is the diagnosis?
Explanation
The histological hallmark of Chondromyxoid fibroma (CMF) is its lobular pattern of stellate/spindle cells in a myxochondroid background, with hypercellular fibrous septa containing osteoclast-like giant cells at the periphery of the lobules.
Question 43
What is the most common anatomic location for the presentation of a Chondromyxoid fibroma (CMF)?
Explanation
CMF most commonly occurs in the lower extremities, particularly around the knee. The proximal tibia metaphysis is the single most common location, accounting for a large percentage of cases.
Question 44
A 20-year-old male presents with chronic pain below the knee. A radiograph is obtained.
Which radiographic description best characterizes this lesion, consistent with Chondromyxoid fibroma?
Which radiographic description best characterizes this lesion, consistent with Chondromyxoid fibroma?
Explanation
CMF typically presents as an eccentric, geographic, osteolytic lesion in the metaphysis with a well-defined, scalloped sclerotic margin. Intralesional calcification is rarely visible on plain radiographs.
Question 45
Which of the following histological features is most useful in differentiating a Chondroblastoma from a Chondromyxoid fibroma?
Explanation
Chondroblastoma is characterized by chondroblasts with grooved "coffee-bean" nuclei and fine, pericellular "chicken-wire" calcifications. CMF features a myxoid background and lacks both the grooved nuclei and typical chicken-wire calcification.
Question 46
A 10-year-old child presents with a waddling gait, severe leg muscle weakness, and chronic deep thigh pain. Radiographs demonstrate bilateral symmetrical cortical thickening of the diaphyseal regions of the femur and tibia, sparing the epiphyses. What is the most likely diagnosis?
Explanation
Progressive diaphyseal dysplasia (Camurati-Engelmann disease) presents with bilateral, symmetrical diaphyseal cortical thickening, leg pain, and proximal muscle weakness resulting in a waddling gait.
Question 47
Which genetic mutation is responsible for Progressive diaphyseal dysplasia (Camurati-Engelmann disease)?
Explanation
Camurati-Engelmann disease is an autosomal dominant condition caused by mutations in the TGFB1 (Transforming Growth Factor Beta 1) gene, which leads to increased bone formation.
Question 48
A patient with suspected Camurati-Engelmann disease undergoes radiographic evaluation.
What is the hallmark radiographic feature seen in this condition?
What is the hallmark radiographic feature seen in this condition?
Explanation
The hallmark of Camurati-Engelmann disease is symmetrical cortical thickening and sclerosis of the diaphysis of long bones, which begins mid-shaft and progresses toward, but spares, the metaphyses and epiphyses.
Question 49
What is the most effective medical treatment to alleviate the severe bone pain and improve muscle weakness in patients with Progressive diaphyseal dysplasia (Camurati-Engelmann disease)?
Explanation
Systemic glucocorticoids are the mainstay of medical treatment for Camurati-Engelmann disease, proven to effectively reduce bone pain, decrease cortical thickening, and improve muscle strength.
Question 50
A 35-year-old patient undergoes curettage of a pathologically confirmed Chondromyxoid fibroma of the proximal tibia. What is the standard management to minimize the risk of local recurrence while preserving joint function?
Explanation
Because CMF has a local recurrence rate of up to 25% with simple curettage alone, extended curettage with a high-speed burr and local adjuvants (phenol, argon beam, or cryotherapy) is the standard of care to minimize recurrence.
Question 51
A 5-year-old child with Hunter syndrome (MPS II) is scheduled for elective bilateral hip osteotomies. Which of the following is the most critical perioperative consideration for the anesthesia team?
Explanation
Patients with MPS (especially Hurler and Hunter syndromes) accumulate glycosaminoglycans in their upper airway tissues (macroglossia, stiff tissues) and have a short neck, making them extremely difficult to intubate and at high risk for perioperative airway loss.
Question 52
A 55-year-old male presents with deep, aching thigh pain. Radiographs show a mottled, permeative lytic lesion in the femoral diaphysis. MRI reveals extensive bone marrow replacement and a large soft tissue mass, but with remarkable preservation of the cortical bone structure.
Which of the following immunohistochemical marker profiles is most characteristic of the suspected diagnosis?
Which of the following immunohistochemical marker profiles is most characteristic of the suspected diagnosis?
Explanation
The clinical and radiographic presentation with a large soft-tissue mass but minimal cortical destruction is classic for Primary Bone Lymphoma (typically Diffuse Large B-Cell Lymphoma). DLBCL is characteristically positive for B-cell markers (CD20) and Leukocyte Common Antigen (CD45), but negative for T-cell markers (CD3).
Question 53
A 4-year-old boy presents with severe thoracolumbar kyphosis, coarse facial features, and corneal clouding. Radiographs of the spine demonstrate anterior inferior vertebral beaking. Which of the following metabolic defects is the underlying cause of this patient's condition?
Explanation
Anterior inferior vertebral beaking, coarse facial features, and corneal clouding are classic for Hurler syndrome (MPS I), an autosomal recessive disorder caused by a deficiency of alpha-L-iduronidase. Hunter syndrome (MPS II) presents similarly but is X-linked and lacks corneal clouding, while Morquio syndrome (MPS IV) features anterior central (middle) vertebral beaking.
Question 54
A 25-year-old female undergoes a biopsy for a painful, eccentric, osteolytic lesion in the proximal tibial metaphysis with a well-defined sclerotic margin.
Histological analysis shows stellate cells in a myxoid background with osteoclast-like giant cells at the periphery of lobules. What is the most common genetic alteration associated with this tumor?
Histological analysis shows stellate cells in a myxoid background with osteoclast-like giant cells at the periphery of lobules. What is the most common genetic alteration associated with this tumor?
Explanation
The lesion is a Chondromyxoid Fibroma (CMF), which frequently involves a rearrangement of chromosome 6q25, leading to promoter swapping and upregulation of the GRM1 (glutamate receptor 1) gene. This mutation is found in up to 80% of CMF cases.
Question 55
A 10-year-old child presents with a waddling gait, severe leg pain, and generalized muscle weakness. Radiographs demonstrate symmetrical cortical thickening and sclerosis of the diaphyseal regions of the bilateral femurs and tibiae, sparing the epiphyses.
Which of the following medical treatments has been shown to be most effective in alleviating the pain and improving motor function in this condition?
Which of the following medical treatments has been shown to be most effective in alleviating the pain and improving motor function in this condition?
Explanation
The patient has Camurati-Engelmann disease (Progressive Diaphyseal Dysplasia). Systemic corticosteroids are the mainstay of medical treatment, significantly reducing bone pain, improving waddling gait, and sometimes reversing the radiographic abnormalities.
Question 56
A 6-year-old boy with a known diagnosis of Morquio syndrome (MPS IV) presents for an orthopedic evaluation. He has pronounced genu valgum and a short trunk.
Which of the following is the most critical screening evaluation required before he undergoes any elective surgical procedure?
Which of the following is the most critical screening evaluation required before he undergoes any elective surgical procedure?
Explanation
Patients with Morquio syndrome have a high incidence of odontoid hypoplasia and ligamentous laxity, leading to atlantoaxial instability. Flexion-extension cervical radiographs (and often an MRI) are mandatory prior to general anesthesia to prevent catastrophic spinal cord injury during intubation.
Question 57
Primary Bone Lymphoma is most frequently treated with which of the following regimens, assuming there is no impending pathologic fracture?
Explanation
Primary Bone Lymphoma is highly responsive to systemic therapy, and surgical resection is rarely indicated unless needed for stabilization of an impending or actual fracture. The standard of care is multi-agent chemotherapy (R-CHOP for DLBCL) usually combined with consolidative radiation therapy to the affected bone.
Question 58
Which specific glycosaminoglycan (GAG) is predominantly accumulated and excreted in the urine of patients with Morquio syndrome (MPS IV)?
Explanation
Morquio syndrome (MPS IV) is characterized by the inability to degrade keratan sulfate due to deficiency in either N-acetylgalactosamine-6-sulfatase (Type A) or beta-galactosidase (Type B). Hurler and Hunter syndromes typically show elevated heparan and dermatan sulfate.
Question 59
A 28-year-old male is diagnosed with a chondromyxoid fibroma of the proximal tibia after an incisional biopsy. He is neurologically intact with a stable knee joint. Which of the following is the most appropriate definitive surgical management?
Explanation
Chondromyxoid fibroma is a benign but locally aggressive cartilaginous tumor. The standard of care to minimize recurrence while preserving joint function is extended intralesional curettage with the use of a high-speed burr, followed by bone grafting or cementation.
Question 60
A 12-year-old girl with a history of recurrent ear infections and progressive hearing loss develops a waddling gait and aching pain in her legs. Radiographs demonstrate marked symmetric endosteal and periosteal thickening of the long bone diaphyses.
This condition is most commonly caused by a mutation in which of the following genes?
This condition is most commonly caused by a mutation in which of the following genes?
Explanation
The clinical and radiographic picture represents Camurati-Engelmann disease (progressive diaphyseal dysplasia). It is inherited in an autosomal dominant pattern and is caused by mutations in the TGFB1 (Transforming Growth Factor Beta 1) gene, leading to increased bone formation.
Question 61
When evaluating a patient with Mucopolysaccharidosis Type I (Hurler syndrome), which of the following hand/wrist manifestations is most commonly encountered and often necessitates surgical intervention?
Explanation
Carpal tunnel syndrome is extremely common in patients with MPS (especially types I, II, and V) due to the deposition of glycosaminoglycans within the flexor tenosynovium and flexor retinaculum. Prophylactic or early surgical release is frequently required to prevent irreversible median nerve damage.
Question 62
A 68-year-old female presents with a pathological fracture of the proximal femur. Pre-operative imaging showed a permeative lytic lesion.
Frozen section during stabilization reveals sheets of round blue cells. Immunohistochemistry later returns positive for CD20 and PAX5. In managing her fracture, which of the following statements regarding the integration of radiotherapy is correct?
Frozen section during stabilization reveals sheets of round blue cells. Immunohistochemistry later returns positive for CD20 and PAX5. In managing her fracture, which of the following statements regarding the integration of radiotherapy is correct?
Explanation
For pathological fractures secondary to primary bone lymphoma, surgical stabilization is required. Adjuvant radiotherapy is typically part of the treatment protocol but significantly increases the risk of delayed union, nonunion, and hardware failure.
Question 63
Which of the following is a key distinguishing histological feature between Chondromyxoid Fibroma (CMF) and Chondroblastoma?
Explanation
Histologically, CMF displays a characteristic lobular architecture with hypercellular peripheries containing spindle/stellate cells and osteoclast-like giant cells, and hypocellular myxoid centers. Chondroblastoma features sheet-like arrangements of chondroblasts, 'chicken-wire' calcifications, and lacks this specific lobular architecture.
Question 64
A 50-year-old patient undergoes an MRI for a suspected Primary Bone Lymphoma of the humerus. Which of the following MRI characteristics is most typically associated with this malignancy?
Explanation
Primary bone lymphoma classically demonstrates low to intermediate signal on T1-weighted imaging with an extensive marrow and soft tissue component. A hallmark feature is the relative preservation of the cortical bone despite the large size of the marrow and soft tissue masses.
Question 65
A pediatric patient with suspected Mucopolysaccharidosis undergoes diagnostic testing. Which of the following confirms the definitive diagnosis and specific subtype of the MPS?
Explanation
While urinary GAG levels are an excellent screening test, the definitive diagnosis and subtyping of Mucopolysaccharidoses require the measurement of specific lysosomal enzyme activities in leukocytes, cultured skin fibroblasts, or plasma.
Question 66
In Chondromyxoid Fibroma, approximately 20% of cases may be complicated by secondary changes that can obscure the primary diagnosis on small biopsy samples. What is this common secondary histological finding?
Explanation
Secondary aneurysmal bone cyst (ABC) changes can occur in approximately 20% of Chondromyxoid Fibromas. This can lead to misdiagnosis if a limited biopsy only samples the cystic, blood-filled spaces of the ABC component.
Question 67
A 3-year-old boy presents with coarse facial features, hepatosplenomegaly, and joint stiffness. His mother reports that her brother died in childhood of a similar condition. The patient has clear corneas. What is the inheritance pattern of this specific mucopolysaccharidosis?
Explanation
The clinical picture describes Hunter syndrome (MPS II), which is distinguished from Hurler syndrome by clear corneas and its inheritance pattern. Hunter syndrome is the only mucopolysaccharidosis that is X-linked recessive; all others are autosomal recessive.
Question 68
Primary bone lymphoma can easily be confused with chronic osteomyelitis clinically and radiographically. Which of the following histological stains is most helpful in highlighting the characteristic dense connective tissue framework surrounding the malignant cells in lymphoma?
Explanation
Reticulin staining in primary bone lymphoma characteristically demonstrates a dense, intertwining network of reticulin fibers surrounding individual lymphoma cells. PAS is positive in Ewing sarcoma, while Toluidine blue highlights mucin/cartilage.
Question 69
Which of the following joint abnormalities is a classic orthopedic manifestation in patients with Morquio syndrome (MPS IV) as a result of primary epiphyseal dysplasia and ligamentous laxity?
Explanation
Morquio syndrome (MPS IV) is highly associated with ligamentous laxity and severe genu valgum (knock-knees), which often requires surgical correction (such as guided growth or osteotomies) to maintain ambulation.
Question 70
In the context of Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease), which of the following regions of the skeleton is characteristically SPARED from the hyperostotic process?
Explanation
Camurati-Engelmann disease typically features bilateral, symmetrical cortical thickening and sclerosis of the diaphyses of the long bones. The metaphyses may be involved as the disease progresses, but the epiphyses are classically spared.
Question 71
A 21-year-old male with an eccentric, sharply circumscribed, osteolytic lesion in the proximal tibia is diagnosed with Chondromyxoid Fibroma. Radiographically, what is the typical character of the periosteal reaction associated with this lesion?
Explanation
Chondromyxoid Fibroma is a benign lesion (Lodwick Type 1A or 1B) that typically causes geographic bone destruction with a sclerotic inner margin. It expands the cortex but typically lacks aggressive periosteal reactions (like onion-skinning or sunburst) unless complicated by a pathological fracture.
Question 72
A 55-year-old male presents with deep, aching pain in his distal femur. Radiographs reveal a permeative, moth-eaten osteolytic lesion. MRI demonstrates a large, associated soft-tissue mass, yet there is minimal cortical destruction. A biopsy confirms Primary Bone Lymphoma (diffuse large B-cell subtype). What is the preferred initial treatment for this condition?
Explanation
Primary bone lymphoma (PBL) is highly responsive to chemo-radiation. The standard of care is multiagent chemotherapy (such as R-CHOP) with or without consolidation involved-field radiotherapy, avoiding extensive surgery unless required for impending fractures.
Question 73
A 6-year-old child presents with short-trunk dwarfism, knock knees, and a barrel chest, but possesses normal intelligence. Cervical spine radiographs reveal atlantoaxial instability. A diagnosis of Morquio syndrome (MPS IV Type A) is suspected. Which specific lysosomal enzyme is deficient in this patient?
Explanation
Morquio A syndrome (MPS IVA) is caused by a deficiency of the enzyme galactose-6-sulfatase. It is characterized by severe skeletal dysplasia, normal intelligence, and significant cervical spine instability due to odontoid hypoplasia.
Question 74
A 25-year-old female undergoes a biopsy of an eccentric, lytic metaphyseal lesion in her proximal tibia. The pathologist diagnoses a Chondromyxoid Fibroma (CMF). Which of the following is the defining histological hallmark of this tumor?
Explanation
CMF is characterized microscopically by a distinct lobular architecture featuring hypocellular, myxoid or chondroid centers and hypercellular peripheries containing spindle cells and osteoclast-like giant cells. This biphasic pattern is essential for diagnosis.
Question 75
A 45-year-old male presents with night sweats, fever, and thigh pain. Radiographs show a permeative diaphyseal lesion mimicking osteomyelitis.
Which MRI feature most strongly suggests a diagnosis of primary bone lymphoma over acute osteomyelitis?
Which MRI feature most strongly suggests a diagnosis of primary bone lymphoma over acute osteomyelitis?
Explanation
A classic imaging hallmark of primary bone lymphoma is the presence of a large soft-tissue mass that extends outward from the bone with surprisingly little cortical destruction. Osteomyelitis typically shows distinct cortical breakdown, abscesses, or cloacae.
Question 76
A 2-year-old boy presents with corneal clouding, coarse facial features, severe kyphosis, and progressive intellectual disability. Urinary tests reveal high levels of dermatan sulfate and heparan sulfate. What is the inheritance pattern and deficient enzyme for this condition?
Explanation
The patient has Hurler syndrome (MPS I), which is inherited in an autosomal recessive manner and caused by a deficiency in alpha-L-iduronidase. It presents with severe systemic manifestations, including corneal clouding and cognitive decline.
Question 77
A 4-year-old boy presents with joint stiffness, nodular skin lesions over his scapulae, and behavioral issues. Physical exam reveals clear corneas and hepatosplenomegaly. Which inheritance pattern differentiates this specific mucopolysaccharidosis from the others?
Explanation
This clinical picture is typical of Hunter syndrome (MPS II), which is distinguished by clear corneas and unique nodular skin lesions. Unlike all other mucopolysaccharidoses (which are autosomal recessive), Hunter syndrome is X-linked recessive.
Question 78
A 30-year-old presents with chronic knee pain. Imaging reveals the following lesion.
Biopsy confirms a benign cartilaginous tumor. What is the most common anatomical site for this specific tumor type?
Biopsy confirms a benign cartilaginous tumor. What is the most common anatomical site for this specific tumor type?
Explanation
Chondromyxoid fibroma (CMF) is a rare benign primary bone tumor. While it can occur in various bones, it has a strong predilection for the long bones of the lower extremity, specifically the proximal tibial metaphysis.
Question 79
A 10-year-old boy presents with severe bilateral leg pain, fatigability, and a waddling gait. Radiographs show symmetrical cortical thickening of the femoral and tibial diaphyses, sparing the epiphyses.
What is the underlying genetic mutation responsible for this progressive diaphyseal dysplasia (Camurati-Engelmann disease)?
What is the underlying genetic mutation responsible for this progressive diaphyseal dysplasia (Camurati-Engelmann disease)?
Explanation
Camurati-Engelmann disease (Progressive Diaphyseal Dysplasia) is an autosomal dominant condition caused by mutations in the TGFB1 gene. This leads to increased transforming growth factor-beta 1 activity, stimulating excessive bone formation at the diaphyses.
Question 80
A 7-year-old child with Morquio syndrome presents to the orthopedic clinic with increasing clumsiness, hyperreflexia, and a positive Babinski sign.
What is the primary etiology of the neurologic deterioration in this patient?
What is the primary etiology of the neurologic deterioration in this patient?
Explanation
Morquio syndrome (MPS IV) is classically associated with hypoplasia or absence of the odontoid process. Combined with ligamentous laxity, this causes severe atlantoaxial instability, leading to cervical myelopathy if left untreated.
Question 81
When working up a 60-year-old patient with a newly diagnosed primary bone lymphoma of the humerus, which staging study is absolutely essential and distinguishes the workup of this disease from that of primary bone sarcomas (e.g., osteosarcoma)?
Explanation
Primary bone lymphoma requires accurate hematologic staging to ensure there is no systemic involvement. A whole-body PET-CT and a unilateral or bilateral bone marrow aspirate/biopsy are standard to rule out widespread systemic lymphoma.
Question 82
A 28-year-old patient undergoes surgical treatment for a progressively painful, biopsy-proven chondromyxoid fibroma in the distal femur. What is the standard surgical management that offers the lowest recurrence rate while preserving the joint?
Explanation
Chondromyxoid fibromas are locally aggressive benign tumors (Campanacci stage 2 or 3). The standard of care is extended intralesional curettage using a high-speed burr, often followed by local adjuvants (phenol, cryotherapy) and bone grafting or cementing, which significantly reduces the recurrence rate compared to simple curettage.
Question 83
A 5-year-old with suspected mucopolysaccharidosis undergoes a skeletal survey. Dysostosis multiplex is confirmed.
Which classic vertebral radiographic finding differentiates Hurler syndrome from Morquio syndrome?
Which classic vertebral radiographic finding differentiates Hurler syndrome from Morquio syndrome?
Explanation
In the mucopolysaccharidoses, vertebral body shape helps differentiate syndromes. Hurler syndrome typically features anterior-inferior beaking of the vertebral bodies, whereas Morquio syndrome characteristically demonstrates central anterior beaking.
Question 84
A 55-year-old male was successfully treated for primary bone lymphoma of the distal femur 8 years ago using R-CHOP chemotherapy and localized radiation therapy (45 Gy). He now presents with a new onset of severe knee pain at rest and an aggressive, destructive lytic lesion on radiographs. What is the most likely diagnosis?
Explanation
A new, aggressive, destructive bone lesion arising in the field of prior radiation (usually >5 years post-exposure) is highly suspicious for a radiation-induced secondary sarcoma, most commonly osteosarcoma, fibrosarcoma, or undifferentiated pleomorphic sarcoma.
Question 85
A patient with Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease) presents with severe, debilitating pain in the lower extremities.
Which of the following pharmacological treatments is considered first-line and highly effective for reducing bone pain and improving gait in these patients?
Which of the following pharmacological treatments is considered first-line and highly effective for reducing bone pain and improving gait in these patients?
Explanation
Systemic corticosteroids (e.g., prednisone) are uniquely effective in Camurati-Engelmann disease. They not only provide dramatic relief of bone pain and muscle weakness but can also partially reverse the radiographic diaphyseal thickening.
Question 86
While Chondromyxoid Fibroma (CMF) and Chondroblastoma are both rare, benign cartilaginous bone tumors, they have distinct classic presentations. Which feature best differentiates CMF from chondroblastoma clinically and radiographically?
Explanation
The location of the tumor is a key differentiating feature. Chondroblastoma characteristically arises in the epiphysis (or apophysis) of long bones, whereas Chondromyxoid Fibroma is classically found in the metaphysis.
Question 87
A 48-year-old patient presents with a destructive diaphyseal lesion.
A core needle biopsy is taken, but the initial histology shows significant 'crush artifact' among the small round blue cells. Which adjunctive test on the fresh tissue sample is most reliable to confirm a suspected diagnosis of Primary Bone Lymphoma?
A core needle biopsy is taken, but the initial histology shows significant 'crush artifact' among the small round blue cells. Which adjunctive test on the fresh tissue sample is most reliable to confirm a suspected diagnosis of Primary Bone Lymphoma?
Explanation
Lymphoma cells are extremely fragile and prone to 'crush artifact' on standard needle biopsy, obscuring cellular architecture. Submitting fresh tissue in saline for flow cytometry is highly reliable for identifying the clonal B-cell or T-cell populations characteristic of lymphoma.
Question 88
An 8-year-old child presents with normal intelligence but severe skeletal dysplasia, macrocephaly, coarse facial features, and dense corneal clouding. Laboratory tests show elevated urinary dermatan sulfate only. A diagnosis of Maroteaux-Lamy syndrome (MPS VI) is made. Which enzyme is deficient in this condition?
Explanation
Maroteaux-Lamy syndrome (MPS VI) is caused by a deficiency in arylsulfatase B. It is characterized by severe skeletal manifestations (dysostosis multiplex) and corneal clouding, but notably preserves normal intellectual function.
Question 89
A 45-year-old male presents with deep right thigh pain. Radiographs demonstrate a subtle permeative diaphyseal lesion with minimal cortical destruction. However, MRI reveals extensive marrow replacement and a large soft tissue mass. Biopsy confirms primary bone lymphoma (diffuse large B-cell). What is the most appropriate initial treatment for this patient?
Explanation
Primary bone lymphoma is highly sensitive to chemotherapy and radiation. Systemic chemoradiation (e.g., R-CHOP) is the standard of care, and surgical intervention is strictly reserved for impending or actual pathologic fractures.
Question 90
A 6-year-old boy presents with short-trunk dwarfism, knock knees, and normal intelligence. Radiographs demonstrate platyspondyly with central anterior beaking.
What is the most life-threatening orthopedic complication associated with this specific metabolic disorder?
What is the most life-threatening orthopedic complication associated with this specific metabolic disorder?
Explanation
The clinical and radiographic presentation is classic for Morquio syndrome (MPS IV). The most life-threatening complication is cervical myelopathy secondary to atlantoaxial instability from odontoid hypoplasia, which warrants prompt screening.
Question 91
An 18-year-old female presents with chronic dull knee pain. Radiographs show an eccentric, radiolucent, sharply marginated metaphyseal lesion in the proximal tibia.
Which of the following best describes the classic histologic appearance of this tumor?
Which of the following best describes the classic histologic appearance of this tumor?
Explanation
Chondromyxoid fibroma (CMF) is characterized histologically by a distinct lobular architecture. It features lobules of myxoid and chondroid tissue containing stellate cells, which are separated by highly cellular fibrous septa with osteoclast-like giant cells.
Question 92
A 12-year-old girl presents with deep leg pain, easy fatigability, and a waddling gait. Radiographs reveal bilateral, symmetric cortical thickening and sclerosis of the femoral and tibial diaphyses, sparing the epiphyses.
A mutation in which of the following genes is primarily responsible for this condition?
A mutation in which of the following genes is primarily responsible for this condition?
Explanation
The clinical and radiographic presentation is diagnostic of progressive diaphyseal dysplasia (Camurati-Engelmann disease). This autosomal dominant condition is caused by a mutation in the TGFB1 gene, leading to increased bone formation.
Question 93
A 55-year-old female presents with a destructive osteolytic lesion in the proximal humerus associated with a soft tissue mass. Following a biopsy, she is diagnosed with primary bone lymphoma. Which of the following imaging features is considered highly characteristic of this malignancy?
Explanation
A classic imaging hallmark of primary bone lymphoma is an MRI demonstrating extensive bone marrow infiltration that is disproportionately large compared to the minimal cortical destruction seen on plain radiographs.
Question 94
A 4-year-old boy presents with coarse facial features, joint contractures, hepatosplenomegaly, and clear corneas. His mother notes that his maternal uncle had similar clinical features and passed away in his teens. Radiographs demonstrate anterior inferior vertebral body beaking. Which of the following is the deficient enzyme in this patient's condition?
Explanation
The patient has Hunter syndrome (MPS II), distinguished from Hurler syndrome by clear corneas and an X-linked recessive inheritance pattern (maternal uncle affected). It is caused by a deficiency in iduronate-2-sulfatase.
Question 95
When distinguishing a chondromyxoid fibroma (CMF) from a chondroblastoma based on clinical and histologic criteria, which of the following features is most indicative of CMF?
Explanation
CMF typically presents as an eccentric metaphyseal lesion with lobular architecture consisting of myxoid and chondroid zones. Chondroblastomas are classically epiphyseal and feature 'chicken-wire' calcifications.
Question 96
A 60-year-old man undergoes a biopsy for a permeative lesion of the proximal femur.
Histology demonstrates sheets of large, atypical mononuclear cells with prominent nucleoli. Immunohistochemistry is strongly positive for CD20 and CD45, but negative for CD99 and CD138. What is the most appropriate next step in systemic evaluation?
Histology demonstrates sheets of large, atypical mononuclear cells with prominent nucleoli. Immunohistochemistry is strongly positive for CD20 and CD45, but negative for CD99 and CD138. What is the most appropriate next step in systemic evaluation?
Explanation
The CD20 and CD45 positivity confirms diffuse large B-cell lymphoma (primary bone lymphoma), while negative CD138 rules out multiple myeloma and negative CD99 makes Ewing sarcoma unlikely. Staging via PET/CT is the standard next step.
None

Medically Verified Content by
Prof. Dr. Mohammed Hutaif Clinic
Consultant Orthopedic & Spine Surgeon