ABOS Part I Orthopaedic Review: Periprosthetic, Subtrochanteric, Pilon Fractures & Management | Part 22203
Key Takeaway
This module offers a comprehensive review for ABOS Part I and AAOS OITE exams, focusing on complex lower extremity fractures. It covers periprosthetic femoral, subtrochanteric femur, and pilon fractures, detailing their classification (Vancouver, AO/OTA, Rüedi-Allgöwer), biomechanics, advanced imaging, surgical approaches, fixation strategies, and critical patient management protocols, including orthogeriatric co-management and metabolic bone health.
ABOS Part I Orthopaedic Review: Periprosthetic, Subtrochanteric, Pilon Fractures & Management | Part 22203
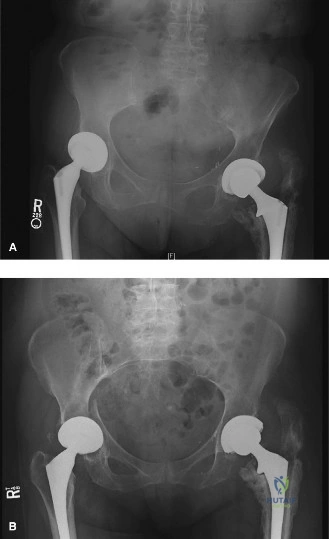
A 78-year-old female with a history of bilateral total hip arthroplasty and osteoporosis presents after a low-energy torsional injury. Initial radiographs, similar to the one shown, reveal a comminuted, spiral fracture of the right femoral shaft extending from the distal aspect of a cemented stem. The stem appears well-fixed with an intact cement mantle and no gross subsidence. Based on this initial assessment, what is the most appropriate provisional Vancouver Classification for this periprosthetic fracture?
Correct Answer: Vancouver Type B1
The Vancouver Classification system is the gold standard for periprosthetic femoral fractures, guiding prognosis and surgical strategy based on fracture location, implant stability, and bone stock. The case describes a fracture occurring around the stem, specifically extending from its distal aspect. This immediately places it into the Type B category. The critical distinction within Type B is the stability of the implant and the quality of the bone stock. The vignette explicitly states that the stem appears well-fixed with an intact cement mantle and no gross subsidence. This combination of a fracture around the stem and a stable implant is the definition of a Vancouver Type B1 fracture.
- Vancouver Type A fractures involve the trochanteric region (AG for greater trochanter, AL for lesser trochanter). This is incorrect as the fracture is in the femoral shaft, distal to the trochanters.
- Vancouver Type B2 fractures occur around a loose stem with adequate bone stock. While the fracture is around the stem, the stem is described as stable, making B2 incorrect.
- Vancouver Type B3 fractures occur around a loose stem with poor bone stock. Again, the stem is described as stable, making B3 incorrect.
- Vancouver Type C fractures occur well distal to the tip of the prosthesis. The fracture is described as extending from the distal aspect of the stem, not well distal to it, making C incorrect.
Therefore, based on the initial radiographic assessment and description of implant stability, Vancouver Type B1 is the most appropriate provisional classification.
A 65-year-old male with a history of cemented total hip arthroplasty presents with a periprosthetic femoral fracture. The fracture is located at the distal tip of the stem, similar to the case described. Which of the following biomechanical factors is most directly responsible for concentrating stress at this specific location, predisposing to fracture?
Correct Answer: The viscoelastic properties of the native bone compared to the rigid metallic stem
The case highlights that the transition zone between the rigid prosthetic stem and the more elastic native diaphyseal bone acts as a massive stress riser. This mismatch in the modulus of elasticity concentrates torsional and bending forces exactly at the tip of the prosthesis, making it a common site for periprosthetic fractures, especially with torsional injuries.
- Increased endosteal blood supply leading to localized osteolysis: The endosteal blood supply is typically compromised or obliterated by the stem and cement, not increased. Localized osteolysis can occur but is not the primary biomechanical factor for stress concentration at the tip.
- Stress shielding causing proximal femoral osteopenia: Stress shielding does lead to proximal osteopenia, weakening the bone in that region. While this is a general biomechanical alteration, the specific concentration of stress at the *distal tip* is due to the modulus mismatch, not directly the proximal osteopenia.
- Excessive periosteal stripping during the primary arthroplasty: While excessive periosteal stripping can compromise fracture healing by devascularizing the bone, it is not a direct biomechanical factor that concentrates stress at the stem tip to cause the initial fracture.
- Increased bone density at the stem tip due to load transfer: Load transfer occurs, but the effect at the tip is a stress concentration due to the material mismatch, not an increase in bone density that would prevent fracture. In fact, the opposite is true; the stress concentration makes it vulnerable.
Following initial radiographs for a suspected Vancouver B1 periprosthetic femoral fracture, a CT scan of the right lower extremity with metal artifact reduction sequence (MARS) is obtained, as shown in Figure 2. What is the most critical additional information this advanced imaging provides that plain radiographs often miss, directly impacting definitive surgical planning?
Correct Answer: Definitive evaluation of the cement mantle and subtle stem subsidence
The case explicitly states that CT imaging is critical because 'up to 20% of fractures classified as Vancouver B1 on plain radiographs are found to have loose stems intraoperatively, necessitating a shift from simple internal fixation to a complex revision arthroplasty (Vancouver B2 management).' The CT scan with MARS allows for a definitive evaluation of the cement mantle, assessment for subtle stem subsidence, and mapping of complex fracture morphology. This information is crucial for distinguishing a true B1 (stable stem) from a B2 (loose stem) preoperatively, which dictates whether internal fixation or revision arthroplasty is required.
- Accurate assessment of limb length discrepancy: While CT can contribute to this, calibrated orthogonal radiographs are typically used for templating limb length, and it's not the *most critical* additional information for B1 vs. B2 differentiation.
- Detailed visualization of the knee joint for associated injuries: A CT scan of the lower extremity would include the knee, but the primary indication for a periprosthetic hip fracture is not typically to evaluate the knee joint, unless there's specific clinical suspicion. It's not the most critical information for *definitive surgical planning* of the hip fracture itself.
- Confirmation of the patient's osteoporotic status: Osteoporosis is typically diagnosed via DEXA scan or inferred from fracture mechanism and patient history. While bone quality can be assessed on CT, it's not the primary reason for obtaining a CT in this context.
- Identification of potential deep vein thrombosis: DVT is typically diagnosed with ultrasound, not primarily with a CT scan of the lower extremity for fracture evaluation, unless a CT venogram is specifically ordered.
During the surgical exposure of a Vancouver B1 periprosthetic femoral fracture, the surgeon performs an extensile direct lateral approach. After incising the fascia lata, the vastus lateralis is identified. To preserve the primary periosteal blood supply to the femur and minimize devascularization of fracture fragments, which of the following surgical maneuvers is most appropriate?
Correct Answer: Elevate the vastus lateralis anteriorly off the lateral intermuscular septum, carefully ligating perforating vessels.
The case emphasizes that the healing of a periprosthetic fracture is almost exclusively dependent on the periosteal blood supply, primarily from the perforating branches of the profunda femoris artery. Surgical approaches must strictly respect these posterior structures. The text states: 'The vastus lateralis is elevated anteriorly off the lateral intermuscular septum. Perforating vessels from the profunda femoris will be encountered piercing the septum; these must be carefully identified, ligated, or cauterized to prevent postoperative hematoma, while strictly avoiding dissection posterior to the septum to preserve the primary periosteal blood supply.'
- Aggressively strip the vastus lateralis anteriorly and posteriorly off the femur: This would lead to significant devascularization of the periosteum, directly contradicting the principle of preserving blood supply.
- Split the vastus lateralis muscle belly longitudinally in its center: While a vastus-splitting approach can be used, the text specifically states that splitting the muscle belly 'can denervate the anterior portion and cause significant bleeding,' and a subvastus or vastus-splitting approach at the *posterior border* is preferred, implying elevation rather than central splitting.
- Perform a complete circumferential periosteal stripping around the fracture site: This is a highly detrimental maneuver that would severely compromise the periosteal blood supply, drastically increasing the risk of nonunion.
- Utilize an anterior approach to avoid the vastus lateralis entirely: An extensile direct lateral approach is described as the standard for these fractures, not an anterior approach.
During the surgical procedure for the Vancouver B1 periprosthetic femoral fracture, after exposing the fracture site, the surgeon performs a critical intraoperative assessment. What is this assessment, and what is its immediate implication if a positive finding is observed?
Correct Answer: Manual 'push-pull' test of the prosthesis; if motion is detected, the diagnosis changes to Vancouver B2, requiring stem revision.
The case explicitly states: 'Once the fracture site is exposed, the most critical step of the operation occurs: the intraoperative assessment of stem stability. The surgeon must perform a manual "push-pull" test. By placing an instrument on the collar or trunnion of the prosthesis (if exposed) or by manipulating the proximal fragment, the surgeon assesses for any gross or micromotion between the stem, the cement mantle, and the proximal bone. If any motion is detected, the diagnosis changes immediately to a Vancouver B2 fracture, and the surgical plan must pivot to stem extraction and revision using a long diaphyseal-engaging stem.'
- Fluoroscopic assessment of fracture reduction; proceed with plate application if satisfactory: Fluoroscopy is used for reduction and hardware placement, but it's not the *most critical* initial intraoperative assessment for *changing the diagnosis and surgical plan* from B1 to B2.
- Measurement of cortical thickness; if less than 4mm, augment with bone graft: Cortical thickness is important for screw purchase and may influence augmentation, but it's not the primary test for stem stability.
- Assessment of periosteal integrity; if compromised, apply rhBMP-2: Periosteal integrity is important for healing, but there's no mention of a specific intraoperative test for it that would immediately change the fracture classification or primary surgical approach.
- Evaluation of fracture comminution; if severe, use a longer plate: Fracture comminution influences plate length and construct design, but it does not change the fundamental classification of B1 vs. B2.
For the Vancouver B1 periprosthetic femoral fracture, a broad, heavy-duty locking compression plate (LCP) is selected. In the proximal segment, where the intramedullary canal is occupied by the existing stem and cement, which of the following fixation strategies is most appropriate to secure the plate to the bone?
Correct Answer: Cerclage cables or wires passed circumferentially around the bone and plate, or specialized unicortical locking screws.
The case clearly outlines the fixation strategy for the proximal segment of a Vancouver B1 fracture: 'In the region of the indwelling stem, bicortical screw purchase is impossible without damaging the implant or the cement mantle, which could precipitate late loosening. Fixation here relies on cerclage cables or wires passed circumferentially around the bone and plate. Specialized cable-ready plates or cable buttons are utilized. Care must be taken using cable passers to stay strictly on the bone to avoid neurovascular injury medially. Alternatively, specialized unicortical locking screws with blunt tips can be used to engage the lateral cortex without penetrating the cement mantle.'
- Standard bicortical locking screws through the plate and stem: This is explicitly stated as impossible and damaging to the implant/cement mantle.
- Unicortical non-locking screws with washers: While unicortical screws are mentioned, they are described as *locking* screws with blunt tips, not non-locking screws with washers, which would provide less stable fixation.
- Intramedullary nailing over the existing stem: This is not feasible with an existing intramedullary stem and cement mantle.
- External fixation with pins placed proximal to the stem: External fixation is generally reserved for open fractures, highly contaminated wounds, or as a temporary measure, not as definitive fixation for a closed periprosthetic fracture around a stable stem.
To optimize the fixation construct for the Vancouver B1 periprosthetic femoral fracture, the surgeon must ensure the locking plate extends sufficiently. What is the recommended minimum overlap of the plate with the proximal stem to prevent creating a new stress riser at the end of the plate?
Correct Answer: At least two femoral cortical diameters
The case specifies the principle of construct optimization: 'To prevent a stress riser at the proximal end of the plate, the plate must overlap the proximal stem by at least two femoral diameters.' This ensures a gradual transition of stress from the plate to the bone, minimizing the risk of fracture at the plate's end.
- At least one femoral cortical diameter: This is generally considered insufficient to prevent a stress riser.
- At least three femoral cortical diameters: While more overlap might be beneficial, two diameters is the stated minimum.
- At least four femoral cortical diameters: This is excessive and not the specified minimum.
- The plate should end exactly at the stem tip: This would create a significant stress riser at the plate's end, directly adjacent to the stem, increasing the risk of refracture.
A 78-year-old female, similar to the patient in the case, undergoes surgical fixation for a Vancouver B1 periprosthetic femoral fracture. Postoperatively, she is allowed touch-down weight bearing. What is the primary rationale for allowing immediate, restricted weight bearing in such a patient with a securely fixed construct?
Correct Answer: To aid in proprioception and balance while protecting the hardware.
The case states: 'For a securely fixed Vancouver B1 fracture utilizing a long locking plate and adequate proximal/distal purchase, patients are typically allowed touch-down or flat-foot weight bearing (approximately 10-15% of body weight) immediately postoperatively. This aids in proprioception and balance while protecting the hardware from catastrophic failure.' Early, restricted weight bearing is crucial for geriatric patients to prevent complications of immobility while providing a safe mechanical environment for healing.
- To promote absolute stability and primary bone healing: Periprosthetic fractures, especially comminuted ones, are managed with principles of *relative stability* to promote secondary bone healing via callus formation, not absolute stability and primary healing.
- To prevent stress shielding of the proximal femur: Stress shielding is a long-term phenomenon related to the presence of the stem itself, not directly prevented by immediate touch-down weight bearing post-fracture fixation.
- To accelerate callus formation by inducing micromotion at the fracture site: While controlled micromotion can stimulate callus, the primary goal of immediate touch-down weight bearing is functional (proprioception, balance) and protective, not solely to induce micromotion. Excessive micromotion can lead to nonunion.
- To allow for early discharge from the hospital: While early mobilization can contribute to earlier discharge, it is a secondary benefit, not the primary rationale for the weight-bearing protocol itself. The primary rationale is patient function and hardware protection.
Six months after surgical fixation of a Vancouver B1 periprosthetic femoral fracture, a patient presents with progressive pain and radiographic evidence of hardware failure and lack of callus formation. The stem remains well-fixed. What is the most appropriate salvage strategy for this aseptic nonunion?
Correct Answer: Revision ORIF with decortication, autologous bone grafting, and potentially dual-plate constructs.
The case discusses the management of aseptic nonunion: 'If a patient presents with progressive pain and radiographic evidence of hardware failure or lack of callus formation at six months, intervention is required. If the stem remains well-fixed, revision plating with decortication, autologous bone grafting (e.g., from the iliac crest or using the Reamer-Irrigator-Aspirator system), and potentially dual-plate constructs are indicated.' This approach addresses the biological (nonunion) and mechanical (hardware failure) issues while preserving the stable stem.
- Non-operative management with prolonged immobilization and pain control: Non-operative management is generally reserved for very specific, non-ambulatory, or moribund patients and is associated with high complication rates. It is not appropriate for a patient with a failed surgical fixation and a stable stem.
- Immediate revision total hip arthroplasty with stem exchange: This would be indicated if the stem were loose (Vancouver B2 or B3), but the vignette explicitly states the stem remains well-fixed. Unnecessary stem revision adds significant morbidity.
- Application of an external fixator for improved stability: External fixation is typically not the definitive treatment for aseptic nonunion of a periprosthetic femoral fracture in this scenario. It's more common for open fractures or temporary stabilization.
- Aggressive surgical debridement and implant retention (DAIR): DAIR is a strategy for acute periprosthetic joint infection, not aseptic nonunion. The question specifies 'aseptic nonunion.'
The patient in the vignette has a history of osteoporosis and discontinued alendronate therapy. A critical component of her postoperative protocol, beyond surgical fixation, is the reinstitution of metabolic bone management. Which of the following best describes the recommended approach for optimizing her bone health?
Correct Answer: Consult an endocrinology or metabolic bone specialist to optimize calcium/Vitamin D and initiate appropriate pharmacological therapy.
The case emphasizes the importance of metabolic bone management: 'A critical component of the postoperative protocol is the reinstitution of metabolic bone management. Following the acute healing phase, an endocrinology or metabolic bone specialist consultation is mandatory to optimize calcium/Vitamin D levels and initiate appropriate anabolic or antiresorptive pharmacological therapy (e.g., Teriparatide or Denosumab, depending on specific indications and contraindications).' This multidisciplinary approach is essential for long-term bone health and preventing future fractures.
- Continue aspirin 81mg daily as the sole medical management for osteoporosis: Aspirin is for DVT prophylaxis and cardiovascular health, not a treatment for osteoporosis.
- Initiate high-dose Vitamin C supplementation immediately: While Vitamin C is important for collagen synthesis, it is not the primary or sole treatment for osteoporosis, which requires comprehensive management of calcium, Vitamin D, and specific pharmacological agents.
- Prescribe a short course of oral corticosteroids to reduce inflammation: Corticosteroids are known to worsen osteoporosis and are contraindicated for its management.
- Recommend strict bed rest for 3 months to allow bone consolidation: Strict bed rest is detrimental in geriatric patients, leading to numerous complications, and contradicts the principle of early mobilization for periprosthetic fractures.
The American Academy of Orthopaedic Surgeons (AAOS) guidelines emphasize an interdisciplinary approach for managing periprosthetic fractures, particularly in elderly patients. What is the primary benefit of the orthogeriatric co-management model, as highlighted in the case?
Correct Answer: It has been definitively shown to reduce time to surgery, decrease length of hospital stay, and lower the one-year mortality rate.
The case explicitly states: 'The orthogeriatric co-management model—where orthopedic surgeons and geriatricians collaboratively manage the patient from admission through discharge—has been definitively shown to reduce time to surgery, decrease length of hospital stay, and lower the one-year mortality rate in elderly patients with periprosthetic fractures.' This highlights the significant, evidence-based benefits of a comprehensive, multidisciplinary approach to these complex patients.
- It primarily focuses on reducing surgical time and blood loss during the procedure: While optimizing patient health can indirectly affect surgical parameters, the primary focus of orthogeriatric co-management is broader patient outcomes, not just intraoperative metrics.
- It ensures that all patients receive revision arthroplasty regardless of fracture type: This is incorrect. The management strategy (fixation vs. revision) is dictated by the Vancouver classification and implant stability, not by the co-management model.
- It eliminates the need for advanced imaging like CT scans: Advanced imaging remains crucial for accurate diagnosis and surgical planning, regardless of the co-management model.
- It exclusively manages the patient's psychological well-being post-injury: While psychological well-being is part of holistic care, orthogeriatric co-management encompasses a much broader range of medical, functional, and rehabilitative aspects, not exclusively psychological care.
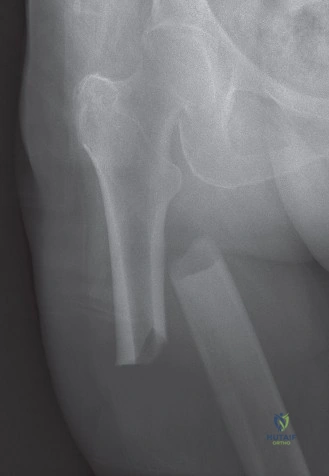
A 72-year-old female presents to the emergency department after a low-energy fall at home. She has a history of osteoporosis and has been on alendronate for 8 years. Radiographs reveal a transverse fracture of the proximal femur, approximately 3 cm distal to the lesser trochanter, with lateral cortical thickening and minimal comminution. The contralateral femur shows similar, though less pronounced, cortical changes. Given her history and radiographic findings, which of the following is the most appropriate initial management strategy for the *affected* femur?
Correct Answer: C
Explanation:
The patient's presentation is highly suggestive of an Atypical Femoral Fracture (AFF). Key features include: elderly female, prolonged bisphosphonate use (8 years of alendronate), low-energy trauma, transverse fracture pattern in the subtrochanteric region, lateral cortical thickening (a 'beaking' or 'flaring' sign), and minimal comminution. The mention of similar changes in the contralateral femur further supports the diagnosis, as AFFs are often bilateral.
- Why C is correct: The case explicitly states that Atypical Femoral Fractures (AFFs) are inherently unstable and have a high risk of complete fracture if not surgically stabilized. Prophylactic nailing of the contralateral femur is often considered if radiographic signs of an impending AFF are present due to the high rate of bilaterality. Intramedullary nailing (IMN) is the gold standard for stabilizing these fractures, providing load-sharing and robust fixation.
- Why A is incorrect: Non-operative management for AFFs is contraindicated due to their inherent instability and high risk of progression to complete fracture and nonunion.
- Why B is incorrect: While plate fixation can be used for certain subtrochanteric fractures, IMN is generally preferred for AFFs. The case states that IMN is the gold standard for most subtrochanteric fractures, and specifically mentions prophylactic nailing for incomplete AFFs. Plate fixation is typically reserved for specific situations where IMN is difficult or contraindicated, which is not the primary indication for a typical AFF.
- Why D is incorrect: While medical optimization is important, delayed fixation with prolonged skeletal traction is generally avoided for femur fractures due to the associated risks of prolonged recumbency and systemic complications, especially in elderly patients. Early stabilization is preferred.
- Why E is incorrect: Total hip arthroplasty is not indicated for an acute subtrochanteric femur fracture, even in osteoporotic bone. It is a reconstructive procedure for hip joint pathology (e.g., severe arthritis, femoral head AVN/fracture) and would not address the diaphyseal fracture.
A 35-year-old male sustains a high-energy subtrochanteric femur fracture after a motor vehicle collision. On initial clinical examination and radiographic assessment, the orthopedic surgeon notes significant displacement of the fracture fragments. Which of the following describes the characteristic deforming forces acting on the *proximal* fragment in a typical subtrochanteric femur fracture?
Correct Answer: C
Explanation:
The teaching case explicitly details the powerful muscular attachments and their deforming forces on subtrochanteric fracture fragments. Understanding these forces is critical for achieving successful reduction.
- Why C is correct: The case states: "The net effect of these opposing forces is often a characteristic deformity: flexion, abduction, and external rotation of the proximal fragment, with adduction and shortening of the distal fragment." Specifically, the iliopsoas muscle inserts onto the lesser trochanter, causing flexion of the proximal fragment. The gluteus medius and minimus insert onto the greater trochanter, inducing abduction. The external rotators (piriformis, obturators, gemelli, quadratus femoris) also contribute to external rotation of the proximal segment.
- Why A, B, D, and E are incorrect: These options do not accurately reflect the combined deforming forces described in the case for the proximal fragment. Extension is not a primary deforming force on the proximal fragment; rather, flexion is. Adduction and internal rotation are typically forces acting on the distal fragment, not the proximal. The forces are rarely balanced, leading to significant displacement.
A 58-year-old male presents with a comminuted subtrochanteric femur fracture (AO/OTA 32-A3) after a fall from a ladder. During pre-operative planning, a CT scan reveals significant medial cortical comminution. The surgeon plans for intramedullary nailing. Based on the biomechanical principles outlined in the case, what is the most critical consideration regarding this medial comminution?
Correct Answer: C
Explanation:
The teaching case emphasizes the biomechanical challenges posed by subtrochanteric fractures, particularly the impact of comminution.
- Why C is correct: The case states under 'Impact of Comminution': "Loss of medial cortical support significantly increases the load on the implant, contributing to implant fatigue and failure if not adequately supported biomechanically. The restoration of medial cortical contact, either directly or indirectly, is critical for load sharing and long-term implant survival." This highlights the crucial role of the medial cortex in sharing compressive loads and protecting the implant from excessive bending stresses.
- Why A is incorrect: While extensive soft tissue stripping during open reduction can compromise periosteal circulation, medial comminution itself does not primarily affect the overall vascular supply to the fracture site in a way that is distinct from other comminuted fractures. The primary concern with medial comminution is biomechanical load sharing.
- Why B is incorrect: The presence of comminution, especially in the subtrochanteric region, generally favors the use of a *long* intramedullary nail to span the entire femoral shaft and protect against distal stress risers or iatrogenic fractures, not a shorter nail.
- Why D is incorrect: While significant comminution can be challenging, IMN remains the gold standard for most subtrochanteric fractures, even comminuted ones. Adjunctive techniques like blocking screws can help achieve reduction and stability. Plate fixation is reserved for specific indications, not simply comminution.
- Why E is incorrect: Medial comminution itself does not inherently increase the likelihood of nerve injury during a lateral surgical approach. Nerve injury is a rare complication related to direct trauma during the approach or screw insertion, not specifically due to medial comminution.
A 48-year-old male presents with a subtrochanteric femur fracture after a fall from a height. Pre-operative radiographs are obtained, including the image below. The surgical team is planning for intramedullary nailing. Which of the following pre-operative planning steps is most crucial for determining the appropriate nail length and diameter?
Correct Answer: C
Explanation:
The question asks about the most crucial pre-operative planning step for determining nail length and diameter, specifically in the context of the provided image showing a subtrochanteric fracture.
- Why C is correct: The case explicitly states under 'Implant Selection and Templating': "Templating with contralateral hip films helps estimate nail length and diameter. The nail should ideally extend to within 1-2 cm of the epiphyseal plate of the distal femur." This is a direct and essential step for accurate implant sizing.
- Why A is incorrect: Reviewing anticoagulant use is crucial for surgical safety (bleeding risk) but does not directly determine nail length or diameter.
- Why B is incorrect: Obtaining a CT scan with 3D reconstructions is highly recommended for comminuted fractures to delineate fracture patterns and identify issues with nail entry or length. While it helps understand the fracture, templating with contralateral films is the primary method for *estimating* the overall nail length and diameter needed for the entire femur.
- Why D is incorrect: A comprehensive neurological examination is part of the overall patient assessment to rule out concomitant injuries but does not directly influence nail sizing.
- Why E is incorrect: Consulting anesthesia for pain management is vital for patient comfort and early mobilization but is not a step for determining implant dimensions.
During the surgical fixation of a subtrochanteric femur fracture, the surgeon encounters difficulty achieving and maintaining reduction of the proximal fragment, which remains significantly flexed and abducted despite longitudinal traction. Which of the following intra-operative maneuvers or adjunctive techniques is most appropriate to address this specific reduction challenge?
Correct Answer: C
Explanation:
The question describes a common and challenging scenario in subtrochanteric fracture fixation: difficulty reducing the proximal fragment's characteristic flexion and abduction deformity.
- Why C is correct: The case specifically addresses this under 'Reduction - Addressing Proximal Fragment Deformity': "Flexion: The proximal fragment is often flexed by the iliopsoas. This can be counteracted by increasing hip flexion (if on a radiolucent table), placing a bolster under the buttock, or using a femoral distractor. Abduction/External Rotation: Reduced by adducting and internally rotating the entire limb. A large Schanz pin placed in the proximal fragment and used as a joystick can also aid in reduction." Using a Schanz pin as a joystick provides direct control over the proximal fragment, and a bolster can help counteract iliopsoas flexion.
- Why A is incorrect: While an external fixator can provide powerful reduction capabilities, applying it only to the distal fragment would not directly address the flexion and abduction of the proximal fragment. A fixator spanning the fracture would be more effective, but a Schanz pin is a more direct and less invasive method for joystick control of the proximal fragment.
- Why B is incorrect: Increasing reaming diameter facilitates nail passage but does not directly aid in reducing a significantly flexed and abducted proximal fragment. It's a step *after* reduction.
- Why D is incorrect: Cerclage wires are used for highly comminuted patterns to achieve reduction, but they require open exposure and can compromise periosteal blood supply. They are not the primary or most appropriate technique for correcting the specific flexion/abduction deformity of the proximal fragment, which is better managed with direct manipulation or joystick techniques.
- Why E is incorrect: A distal femoral osteotomy is a complex procedure for correcting malunion or deformity in the distal femur and is not an appropriate intra-operative maneuver for reducing an acute subtrochanteric fracture.
A 65-year-old male undergoes intramedullary nailing for a subtrochanteric femur fracture. Post-operatively, he experiences persistent pain at the greater trochanteric entry site, which is exacerbated by hip abduction and external rotation. Radiographs confirm appropriate nail placement and fracture healing. What is the most likely cause of his persistent pain?
Correct Answer: D
Explanation:
The question describes a patient with persistent pain at the greater trochanteric entry site after IMN for a subtrochanteric fracture, with confirmed fracture healing and appropriate nail placement.
- Why D is correct: The case lists 'Pain at Greater Trochanteric Entry Site' as a common complication (10-20% incidence) and attributes it to "Nail prominence, irritation of the gluteus medius/trochanteric bursa." This perfectly matches the patient's symptoms and the location of pain.
- Why A is incorrect: While piriformis fossa entry (historically) could lead to AVN, modern trochanteric entry nails are designed to avoid this. Furthermore, AVN of the femoral head would typically present with groin pain and radiographic changes in the femoral head, not specifically trochanteric pain, and the question states appropriate nail placement.
- Why B is incorrect: Distal locking screw irritation would cause pain in the distal thigh, not at the greater trochanter.
- Why C is incorrect: The question states that radiographs confirm "fracture healing," ruling out nonunion as the cause of the current pain.
- Why E is incorrect: DVT would typically present with leg swelling, pain (often calf), warmth, and tenderness, not localized pain at the greater trochanteric entry site.
A 55-year-old female presents with a subtrochanteric femur fracture (AO/OTA 32-A3.3, reverse obliquity pattern). She has a wide medullary canal, and pre-operative templating suggests that even the largest available intramedullary nail would not provide adequate canal fill. The surgeon is concerned about the stability of IMN in this specific fracture pattern. Based on the case, which of the following fixation methods would be a more appropriate alternative in this scenario?
Correct Answer: C
Explanation:
The question describes a specific scenario where IMN might be suboptimal: a reverse obliquity fracture with a wide medullary canal, leading to concerns about adequate canal fill and stability with IMN.
- Why C is correct: The case discusses the 'Role of Plate Osteosynthesis' and states: "Plate fixation (e.g., LCP, LISS) is reserved for specific situations where IMN is difficult or contraindicated. These include: ...Extremely wide medullary canals where an IMN would not provide adequate fill. ...Certain reverse obliquity patterns (AO/OTA 32-A3.3) where IMN may allow medial displacement of the distal fragment, although controversy exists, and blocking screws with IMN can address this." This scenario combines both a wide canal and a reverse obliquity pattern, making plate osteosynthesis a more appropriate alternative.
- Why A is incorrect: External fixation is generally used for temporary stabilization, especially in polytrauma, or for complex open fractures, but rarely as definitive treatment for a closed subtrochanteric fracture due to high complication rates and functional limitations.
- Why B is incorrect: Dynamic hip screws (DHS) are primarily used for intertrochanteric fractures and are generally not recommended for subtrochanteric fractures due to high rates of failure and cutout, as they are not designed to withstand the high bending and torsional forces in this region.
- Why D is incorrect: Non-operative management is almost universally contraindicated for displaced subtrochanteric fractures due to the high risk of nonunion, malunion, and systemic complications.
- Why E is incorrect: While exchange nailing with a larger diameter nail is a strategy for nonunion, it's not a primary fixation method for an acute fracture with an *initially* wide canal where even standard large nails are insufficient. Custom-made nails are not a routine primary option.
A 28-year-old male sustains a comminuted subtrochanteric femur fracture. During intramedullary nailing, the surgeon notes that the nail consistently tends to drift into varus, despite careful reaming and initial reduction attempts. To optimize reduction and prevent malalignment, the surgeon decides to use an adjunctive technique. Which of the following techniques, as described in the case, would be most effective in guiding the nail into the desired anatomical reduction and preventing varus angulation?
Correct Answer: C
Explanation:
The question describes a specific intra-operative challenge: the nail drifting into varus despite initial reduction efforts, and asks for the most effective adjunctive technique to guide the nail and prevent malalignment.
- Why C is correct: The case specifically discusses 'Blocking Screws (Poller Screws)' under 'Adjunctive Techniques': "These are strategically placed screws (typically unicortical) that block the nail path, guiding it into the desired anatomical reduction. They are particularly useful for correcting varus-valgus and anterior-posterior angulation, especially in fractures with significant comminution or those tending towards malalignment. Evidence supports their use in optimizing reduction and preventing malunion." This directly addresses the problem of varus drift.
- Why A is incorrect: While an external fixator can aid in reduction, it's a more extensive intervention and not the most direct or specific method for *guiding the nail* and preventing varus drift during IMN insertion.
- Why B is incorrect: Cerclage wires are used for achieving reduction in highly comminuted patterns, but they require open exposure and can compromise periosteal blood supply. They are not primarily used to *guide the nail* or prevent specific angulation during nail insertion in the same way blocking screws are.
- Why D is incorrect: Limited open reduction with clamps is a direct reduction technique if closed methods fail, but it's not an adjunctive technique for *guiding the nail* once it's being inserted. Blocking screws work in conjunction with the nail.
- Why E is incorrect: Reaming to a larger diameter might provide more space for the nail, but it does not inherently *guide* the nail or prevent it from drifting into varus. In fact, excessive reaming without proper guidance could worsen malalignment.
A 70-year-old male undergoes intramedullary nailing for a subtrochanteric femur fracture. Post-operatively, the surgeon prescribes a rehabilitation protocol. Given the patient's age and the nature of the injury, which of the following weight-bearing strategies is generally recommended for a stable IMN construct in the immediate post-operative period (Day 0-7)?
Correct Answer: C
Explanation:
The question asks about the recommended immediate post-operative weight-bearing status for a stable IMN construct of a subtrochanteric femur fracture.
- Why C is correct: The case states under 'Immediate Post-Operative Period (Day 0-7) - Weight-Bearing (WB) Status': "Protected Weight-Bearing (PWB) or Touch-Down Weight-Bearing (TDWB): For most stable IMN constructs, early protected weight-bearing is initiated. This typically involves 10-25% body weight, emphasizing touch-down to maintain proprioception and stimulate healing without overloading the implant." This aligns perfectly with the recommended protocol.
- Why A is incorrect: Full weight-bearing immediately post-op, even with a stable IMN, is generally too aggressive and risks implant failure or loss of reduction, especially in an elderly patient with potentially compromised bone quality.
- Why B is incorrect: Non-weight-bearing for 6 weeks is overly cautious for most stable IMN constructs and can lead to complications of prolonged immobility, such as muscle atrophy, joint stiffness, and DVT. It is reserved for highly unstable fixation or severe osteoporosis.
- Why D is incorrect: Continuous passive motion (CPM) is primarily used for knee rehabilitation and is not universally indicated for hip fractures. More importantly, it doesn't address the weight-bearing status.
- Why E is incorrect: Progressive weight-bearing starting with 50% body weight on day 1 is generally too aggressive for immediate post-operative management of a subtrochanteric fracture, even with a stable IMN. The initial phase is typically 10-25% body weight.
A 40-year-old male presents with a subtrochanteric femur fracture (AO/OTA 32-A1) after a motorcycle accident. He is otherwise healthy. The surgeon plans for intramedullary nailing. During the procedure, the image below is obtained. Based on the current literature and guidelines, which of the following statements regarding the choice of intramedullary nail is most accurate for this fracture?

Correct Answer: C
Explanation:
The question asks about the most accurate statement regarding the choice of intramedullary nail for a subtrochanteric femur fracture, referencing the provided image of an IMN.
- Why C is correct: The case states under 'Summary of Key Literature / Guidelines - Reamed vs. Unreamed Nailing': "Reamed intramedullary nailing typically allows for insertion of a larger diameter nail, improving bone-implant contact and construct stability, with good union rates. While concerns about fat embolization exist, modern reaming techniques have minimized this risk." This makes reamed nailing the generally preferred method.
- Why A is incorrect: The case states under 'Long vs. Short Nails': "For subtrochanteric fractures, particularly those with comminution or extension into the diaphysis, long intramedullary nails extending to the distal femoral metaphysis are generally recommended. This approach reduces the risk of distal femoral shaft fractures above the tip of a short nail, providing a more robust construct and protecting the entire diaphyseal segment." Therefore, a long nail is generally preferred.
- Why B is incorrect: The case states under 'Trochanteric Entry Nails': "Modern trochanteric entry nails are generally preferred over piriformis entry nails. Studies have shown that trochanteric entry is associated with a lower risk of iatrogenic avascular necrosis of the femoral head and easier insertion due to better alignment with the femoral canal, without compromising stability."
- Why D is incorrect: While unreamed nailing has theoretical advantages regarding fat embolization and periosteal blood flow, the case indicates that reamed nailing is generally preferred due to superior stability from larger diameter nails and improved cortical contact, with minimized risks from modern reaming techniques.
- Why E is incorrect: The case clearly states under 'Intramedullary Nailing as the Gold Standard': "Extensive literature consistently supports antegrade intramedullary nailing (IMN) as the gold standard for nearly all subtrochanteric femur fractures. This is primarily due to its load-sharing characteristics, high biomechanical stability, and minimally invasive nature compared to plate osteosynthesis."
A 68-year-old female with a history of chronic kidney disease and poorly controlled diabetes sustains a subtrochanteric femur fracture. She is medically unstable with severe sepsis and decompensated cardiac failure. The orthopedic team is considering surgical intervention. Based on the case, which of the following is an absolute contraindication to immediate operative management?
Correct Answer: C
Explanation:
The question asks for an absolute contraindication to immediate operative management, given a patient with a subtrochanteric fracture and severe medical comorbidities.
- Why C is correct: The case explicitly lists under 'Contraindications for Operative Management': "Absolute contraindications to surgical intervention are rare and generally relate to the patient's overall physiological status rather than the fracture pattern itself. Medically unstable patient: A patient with severe, uncorrectable medical comorbidities (e.g., severe sepsis, decompensated cardiac failure) where the risks of anesthesia and surgery outweigh the benefits of fracture fixation. Such cases require medical stabilization, potentially followed by delayed surgery, or palliation." This perfectly matches the patient's described condition.
- Why A is incorrect: A comminuted fracture pattern is an indication for operative management, not a contraindication, due to its inherent instability.
- Why B is incorrect: A history of prolonged bisphosphonate use is a risk factor for atypical femoral fractures (AFFs), which are a strong indication for surgical fixation, not a contraindication.
- Why D is incorrect: The need for a long intramedullary nail is a surgical planning detail, not a contraindication to surgery itself.
- Why E is incorrect: Advanced age is not an absolute contraindication to surgery. While it often correlates with comorbidities, the decision for surgery is based on physiological status and fracture stability, not age alone. Many elderly patients undergo successful subtrochanteric fracture fixation.
A 42-year-old male construction worker presents to the trauma center with a high-energy pilon fracture after a 15-foot fall. His medical history includes daily tobacco use (1 pack/day x 20 years), poorly controlled Type 2 Diabetes Mellitus (HbA1c 8.4%), and a BMI of 32. Given these comorbidities, which of the following is the MOST significant immediate concern for the orthopedic surgeon regarding the timing and approach to definitive surgical management?
Correct Answer: C
The patient's history of daily tobacco use and poorly controlled Type 2 Diabetes Mellitus are critical factors that significantly impair soft tissue healing and elevate the risk of postoperative complications, particularly wound dehiscence, deep surgical site infection, delayed union, and nonunion. Nicotine is a potent vasoconstrictor, diminishing microvascular perfusion, while carbon monoxide reduces oxygen delivery. Hyperglycemia impairs leukocyte function, increasing infection susceptibility. These factors, combined with the severe Tscherne Grade III closed soft tissue injury described in the case, make a staged approach (Span, Scan, and Plan) absolutely paramount. Delaying definitive open reduction and internal fixation (ORIF) allows the soft tissue envelope to recover, edema to resolve, and patient comorbidities to be optimized, thereby drastically reducing the risk of catastrophic wound complications.
Option A is incorrect because while high-energy trauma and immobility do increase DVT risk, it is a general trauma concern managed with standard protocols and not the primary immediate concern dictating the timing of definitive fracture fixation in the context of severe soft tissue injury and comorbidities.
Option B is incorrect because while a high BMI does add mechanical stress, the immediate concern for hardware failure is secondary to the more pressing issues of soft tissue viability and infection risk, which directly impact the ability to perform definitive surgery safely.
Option D is incorrect because while chronic nicotine use can influence pain perception and management, it is not the most significant immediate concern dictating the surgical strategy for a pilon fracture with severe soft tissue compromise.
Option E is incorrect because while intraoperative glucose management is important, it is typically handled by the anesthesia team and does not fundamentally alter the orthopedic surgeon's decision-making regarding the timing of definitive fixation in the face of severe soft tissue injury and systemic comorbidities.
During the initial assessment of the patient's right lower extremity, intracompartmental pressure monitoring is performed due to equivocal clinical findings. The anterior compartment pressure is 42 mmHg, lateral is 38 mmHg, superficial posterior is 35 mmHg, and deep posterior is 45 mmHg. The patient's diastolic blood pressure is 85 mmHg. Based on these findings and the immediate management decision described in the case, what is the MOST appropriate next step?
Correct Answer: D
The case explicitly states that the delta pressure (Diastolic BP minus Compartment Pressure) for the deep posterior compartment is 40 mmHg (85 - 45 = 40) and for the anterior compartment is 43 mmHg (85 - 42 = 43). While these values hover near the generally accepted threshold of 30 mmHg for fasciotomy, the case also states, 'A decision is made to proceed with immediate spanning external fixation to restore length and alignment, which often significantly decreases intracompartmental pressures by reducing the volumetric mismatch caused by the shortened, displaced fracture.' This highlights a critical principle in high-energy fractures: restoring length and alignment with an external fixator can decompress the compartments by increasing the volume available for the swollen tissues, often obviating the need for fasciotomy. This is a common and appropriate initial management strategy for equivocal compartment syndrome in the setting of a severely displaced fracture.
Option A is incorrect because while the pressures are elevated, the delta pressures are not definitively below 30 mmHg, and the case describes a specific decision to first apply an external fixator, which can resolve the issue without fasciotomy.
Option B is incorrect because while serial examinations are always important, the pressures are significantly elevated, and a more active intervention (external fixation) is indicated to address the underlying cause of the pressure elevation (volumetric mismatch due to fracture displacement).
Option C is incorrect because mannitol and elevation are adjunctive measures for compartment syndrome but are not definitive treatments, especially in the setting of a displaced fracture causing the pressure elevation.
Option E is incorrect because while vascular assessment is paramount, the case states 'palpable but bounding dorsalis pedis and posterior tibial pulses' and 'Capillary refill in the digits is brisk.' Angiography is reserved for cases with signs of vascular compromise, which are not present here.
The patient's initial clinical examination reveals extensive fracture blisters, including both clear fluid-filled and hemorrhagic types, over the anterior and medial aspects of the distal tibia. The injury is classified as a Tscherne Grade III closed soft tissue injury. Which of the following statements accurately reflects the implications of these findings for definitive surgical planning?
Correct Answer: B
The case explicitly states, 'The presence of hemorrhagic blisters signifies a more severe soft tissue insult and strictly precludes any immediate surgical incisions through these zones.' Hemorrhagic blisters indicate a deeper cleavage plane involving the dermal vascular plexus, signifying significant dermal compromise. Tscherne Grade III closed soft tissue injuries are characterized by severe skin contusion, extensive subcutaneous degloving, and impending compartment syndrome, all of which necessitate a delay in definitive surgery to allow for soft tissue recovery. Operating through compromised skin significantly increases the risk of wound dehiscence, infection, and flap necrosis.
Option A is incorrect because even clear fluid-filled blisters indicate dermo-epidermal separation and significant edema, which, in the context of a high-energy pilon fracture and Tscherne Grade III injury, still necessitates a delay in definitive fixation. The severity of the overall soft tissue injury, not just the blister type, dictates the staged approach.
Option C is incorrect because Tscherne classification primarily assesses soft tissue injury severity, which has a profound impact on wound complication rates, infection, and the timing of surgery, rather than directly impacting bone healing in isolation.
Option D is incorrect because fracture blisters, especially hemorrhagic ones, are not benign. Incising and debriding them immediately prior to definitive ORIF would be detrimental, as it would create an open wound in compromised tissue, increasing infection risk and hindering wound healing.
Option E is incorrect because the case states that the soft tissue envelope typically requires 10 to 21 days to recover sufficiently, with the 'wrinkle sign' being the definitive indicator. 3-5 days is generally too short for severe Tscherne Grade III injuries.
Following the application of a spanning external fixator, a high-resolution Computed Tomography (CT) scan is obtained for detailed preoperative planning. Review the provided axial CT image of the distal tibia.
Based on the image and the case description, which of the following fracture fragments is MOST clearly demonstrated and described as being significantly impacted proximally into the metaphyseal void?

Correct Answer: D
The case description explicitly states, 'The CT scan clearly delineates a large, central die-punch fragment that is impacted 15 millimeters proximally into the metaphyseal void.' The axial CT image provided shows significant comminution of the articular surface, with a large central fragment driven proximally. This central impaction is a hallmark of high-energy pilon fractures and is critical to identify for surgical planning, as it requires elevation and bone grafting.
Option A is incorrect because while a posterolateral (Volkmann) fragment may be present (and is mentioned in the case as part of the Topliss three-fragment pattern), the case specifically highlights the central die-punch fragment as being significantly impacted proximally.
Option B is incorrect because the medial malleolar fragment is typically an avulsion or shear fracture of the medial column, not a centrally impacted fragment.
Option C is incorrect because the anterolateral (Chaput) fragment is a peripheral articular fragment, often displaced, but not typically described as being impacted centrally into the metaphyseal void.
Option E is incorrect because the fibular fracture is a separate injury of the lateral column and is not part of the tibial articular surface impaction.
The initial radiographic series for this 42-year-old male with a high-energy pilon fracture reveals a highly comminuted, complete articular fracture of the distal tibia. Specific findings include significant metaphyseal comminution with varus collapse, a fibula fracture at the level of the syndesmosis, proximal talar migration, a central die-punch fragment, a fractured medial malleolus with vertical extension, and gross displacement of the anterolateral (Chaput) fragment. Which of the following AO/OTA classifications BEST describes this injury?
Correct Answer: D
The case explicitly states, 'Utilizing the more comprehensive AO/OTA classification, the fracture is designated as a 43-C3.' The '43' denotes the distal tibia segment. The 'C' indicates a complete articular fracture, meaning the articular surface is completely separated from the diaphysis. The '3' specifies that both the articular surface and the metaphyseal region are multifragmentary. This aligns perfectly with the description of a 'highly comminuted, complete articular fracture of the distal tibia' with 'significant metaphyseal comminution' and 'proximal talar migration,' indicating a severe, multifragmentary injury involving both the articular surface and the metaphysis.
Option A (43-A3) represents an extra-articular fracture of the distal tibia, which is incorrect as the case describes a complete articular fracture.
Option B (43-B1) represents a partial articular fracture, which is incorrect as the case describes a complete articular fracture.
Option C (43-C1) represents a complete articular fracture with simple metaphyseal involvement, which is incorrect as the case describes multifragmentary metaphyseal comminution.
Option E (44-C2) refers to a fracture of the ankle (malleolar region) and is not the primary classification for a pilon fracture of the distal tibia (43).
The patient's pilon fracture is classified as a Rüedi-Allgöwer Type III. This classification, along with the AO/OTA 43-C3 designation, underscores the extreme complexity of the injury. Which of the following statements accurately describes the key characteristic of a Rüedi-Allgöwer Type III pilon fracture?
Correct Answer: C
The case explicitly states, 'Under the Rüedi-Allgöwer system, this injury is classified as a Type III fracture. This indicates a highly comminuted articular surface with significant metaphyseal impaction and displacement of the major weight-bearing columns.' This definition perfectly matches the description of the patient's severe pilon fracture, characterized by extensive articular and metaphyseal damage.
Option A is incorrect as it describes a Rüedi-Allgöwer Type I fracture, which is a simple, non-displaced articular fracture.
Option B is incorrect as it describes a Rüedi-Allgöwer Type II fracture, which involves significant displacement of a major articular fragment but typically less comminution than Type III.
Option D is incorrect as Rüedi-Allgöwer classification specifically addresses intra-articular fractures of the distal tibia, not extra-articular ones.
Option E is incorrect as a pilon fracture involves the tibial plafond, not just the medial malleolus in isolation.
Fourteen days after initial external fixation, the patient's soft tissue envelope shows significant improvement, with resolution of edema and a positive 'wrinkle sign.' Definitive reconstruction is planned using a dual incision strategy. The primary approach is an anterolateral incision. Which of the following describes the correct internervous plane for this approach and a critical nerve to protect?
Correct Answer: B
The case explicitly states, 'The deep dissection utilizes the internervous plane between the extensor digitorum longus (innervated by the deep peroneal nerve) and the peroneus tertius.' It also highlights the critical need for 'meticulous identification and protection of the superficial peroneal nerve, which frequently crosses the operative field from medial to lateral in the distal third of the leg.' This accurately describes the anatomical considerations for the anterolateral approach to the distal tibia.
Option A is incorrect because the plane between the Tibialis Anterior and Extensor Hallucis Longus is more medial, and the saphenous nerve is on the medial side of the leg, not typically at risk in the anterolateral approach.
Option C is incorrect because the plane between the Peroneus Longus and Brevis is more lateral and posterior, and while the deep peroneal nerve is important, the superficial peroneal nerve is more directly at risk with the skin incision and initial dissection of the anterolateral approach.
Option D is incorrect because this describes a posterior approach, and the sural nerve is lateral.
Option E is incorrect because this describes a posterior approach, and the posterior tibial nerve is in the deep posterior compartment.
The definitive reconstruction of this high-energy pilon fracture follows a specific, sequential algorithm. After the fibula is addressed, attention is turned to the articular surface. Which of the following sequences represents the MOST appropriate order for reducing the articular fragments of the distal tibia, as described in the case?
Correct Answer: C
The case explicitly states the reduction sequence: 'The reduction proceeds from the periphery to the center. The anterolateral (Chaput) fragment is mobilized and reduced to the reconstructed fibula. The posterolateral (Volkmann) fragment is then reduced... Once the peripheral rim is re-established, the central die-punch fragments are elevated.' This 'periphery to center' approach is a fundamental principle in pilon fracture reconstruction, using the intact fibula as a template for the lateral column and then building the articular surface outwards from there, finally addressing the central impaction.
Options A, B, D, and E are incorrect because they do not follow the described 'periphery to center' reduction strategy, nor do they align with the specific sequence outlined in the case, which prioritizes reducing the peripheral fragments (Chaput, Volkmann) to the fibula before addressing the central impaction.
A 42-year-old male presents with a high-energy pilon fracture, classified as Rüedi-Allgöwer Type III and AO/OTA 43-C3. The initial management involves a spanning external fixator. The patient's soft tissues are severely compromised, with extensive edema and hemorrhagic fracture blisters. The definitive reconstruction is planned for 14 days post-injury, once the 'wrinkle sign' is positive. What is the primary biomechanical and biological imperative for maintaining a minimum skin bridge of 7 centimeters between the planned anterolateral and posteromedial incisions?
Correct Answer: C
The case explicitly states, 'It is an absolute biomechanical and biological imperative that a minimum skin bridge of 7 centimeters is maintained between the two incisions to preserve the delicate angiosomal blood supply and prevent catastrophic skin necrosis.' This highlights the critical importance of respecting the soft tissue vascularity, especially in high-energy injuries with compromised envelopes. Inadequate skin bridges can lead to ischemia and necrosis of the intervening skin, resulting in devastating wound complications.
Option A is incorrect because while implant placement is a consideration, the primary reason for the skin bridge is biological (vascularity), not purely mechanical space.
Option B is incorrect because nerve entrapment is not the primary concern for maintaining a skin bridge; rather, it's the vascularity of the skin itself.
Option D is incorrect because while tension-free closure is always desired, the 7 cm rule is specifically about preserving blood supply to the skin bridge, not just distributing tension.
Option E is incorrect because heterotopic ossification is a concern in some trauma cases, but it is unrelated to the specific requirement for a minimum skin bridge in dual incision approaches for pilon fractures.
The patient's initial radiographs show a highly comminuted, complete articular fracture of the distal tibia with significant metaphyseal comminution and varus collapse. The fibula is fractured at the level of the syndesmosis, and the talus is proximally migrated. The CT scan further delineates a large, central die-punch fragment impacted 15 millimeters proximally. Based on these findings, which of the following comparative pathologies is LEAST likely to present with a similar degree of central articular impaction and metaphyseal comminution?
Correct Answer: B
The case's differential diagnosis table clearly distinguishes between pilon fractures and trimalleolar ankle fractures. For trimalleolar ankle fractures, it states, 'Articular involvement is peripheral, lacking central impaction.' In contrast, pilon fractures are characterized by 'Complete articular involvement, metaphyseal comminution, central die-punch fragments, proximal talar migration.' Therefore, a trimalleolar ankle fracture is the least likely to present with the central articular impaction and metaphyseal comminution seen in this pilon fracture.
Option A (high-energy talar body fracture) can involve significant comminution and impaction within the talus itself, which is a different bone but can be a high-energy injury with complex articular involvement.
Option C (distal tibial shaft fracture with intra-articular extension) can have an articular split, but the primary fracture is diaphyseal/metaphyseal, and while it extends into the joint, it typically lacks the profound central impaction and comminution characteristic of a pilon.
Option D (severe calcaneal fracture with joint depression) is a high-energy hindfoot injury that frequently involves significant impaction and depression of the subtalar joint articular surface, making it similar in concept of articular impaction, though in a different bone.
Option E (a high-energy pilon fracture) is the exact pathology described in the case and is characterized by central articular impaction and metaphyseal comminution.
The patient's definitive reconstruction involves a dual incision strategy, including a posteromedial approach to address the posterior malleolar extension and the medial column. Which of the following describes the correct internervous plane for the deep dissection of this posteromedial approach and the neurovascular structures to protect?
Correct Answer: D
The case explicitly states for the posteromedial approach: 'The saphenous nerve and vein are protected anteriorly. The deep dissection proceeds between the posterior tibial tendon and the flexor digitorum longus, allowing access to the posterior aspect of the medial malleolus and the Volkmann fragment.' This accurately describes the internervous plane and the key neurovascular structures to protect during this approach.
Option A is incorrect as this describes an anterior approach.
Option B is incorrect as this describes a lateral approach.
Option C is incorrect because while the Flexor Digitorum Longus and Flexor Hallucis Longus are in the deep posterior compartment, the primary internervous plane for the posteromedial approach is between the Posterior Tibial Tendon and the Flexor Digitorum Longus. The sural nerve is lateral.
Option E is incorrect because while the Gastrocnemius and Soleus are posterior, the approach for the distal tibia is typically deeper, and the posterior tibial nerve and artery are deep to the flexor tendons, not directly between the gastrocnemius and soleus for this specific approach to the medial malleolus/Volkmann fragment.
Radiographs confirm a displaced fracture above the anterior flange of the femoral component. The femoral component shows no signs of loosening. According to the Rorabeck classification, this is a Type II fracture. Which of the following factors makes retrograde intramedullary nailing CONTRAINDICATED in this specific scenario?
Radiographs demonstrate a fracture around the stem with visible subsidence of the implant, but adequate proximal bone stock is noted. According to the Vancouver Classification, what is the most appropriate treatment?
) is obtained to evaluate the articular comminution. A large, displaced posterolateral articular fragment (Volkmann's fragment) is identified. Which ligamentous structure remains attached to this specific fragment?
What is the most common complication associated with an entry point that is too lateral on the greater trochanter during this procedure?
Which nerve is at greatest risk of iatrogenic injury during the superficial dissection of the anterolateral approach to the distal tibia?
When reconstructing the articular surface, the surgeon typically identifies three primary articular fragments. Which structure attaches to the anterolateral (Chaput) fragment?
None
