

Welcome, colleagues, to this definitive masterclass. Today, we are undertaking a rigorous, exhaustive exploration of a profoundly challenging yet critically important procedure in revision arthroplasty: the first stage of a two-stage exchange arthroplasty for chronic deep periprosthetic hip infection. This intervention involves the meticulous extirpation of all infected components and foreign material, radical debridement of compromised osseous and soft tissues, and the precise fabrication and insertion of a high-dose antibiotic-loaded cement spacer. This is not merely a temporizing salvage maneuver; it is the definitive foundation of a curative treatment strategy that demands uncompromising precision, profound anatomical knowledge, and an intimate understanding of microbiology and biomechanics.
Comprehensive Introduction and Patho-Epidemiology
Before we make a single incision, it is imperative to fully conceptualize the complex pathology we are addressing. Chronic deep periprosthetic joint infection (PJI) of the hip is a formidable, often insidious adversary. Unlike acute postoperative infections, which manifest rapidly with florid systemic signs, or acute hematogenous seeding in a previously asymptomatic joint, chronic infections typically present months or even years following the index arthroplasty. The infectious process has likely been established since the original surgical intervention, but due to the low virulence of the causative organism and the protective mechanisms of bacterial biofilms, classic clinical signs of sepsis are frequently conspicuously absent. Patients routinely present with insidious, non-specific mechanical hip pain as their primary, and sometimes only, symptom.
The pathogenesis of chronic PJI is fundamentally defined by the formation of a bacterial biofilm. When planktonic (free-floating) bacteria adhere to the inert surface of an orthopedic implant, they undergo a profound phenotypic shift. They begin to secrete an extracellular polymeric substance (EPS)—a dense glycocalyx matrix that firmly anchors the bacterial colony to the implant and surrounding necrotic tissue. This sessile, biofilm-encased community is highly resistant to both host immune responses (macrophages and antibodies cannot penetrate the matrix) and systemic antimicrobial therapy. The minimum inhibitory concentration (MIC) required to eradicate biofilm bacteria can be up to 1,000 times higher than that required for their planktonic counterparts, rendering systemic antibiotics virtually useless for definitive cure once a biofilm is established.
Microbiologically, chronic periprosthetic infections are most frequently driven by less virulent, commensal skin flora. Coagulase-negative Staphylococci (such as Staphylococcus epidermidis) and Cutibacterium acnes are prototypical offenders, leading to an indolent, smoldering clinical course. However, more virulent organisms, such as methicillin-resistant Staphylococcus aureus (MRSA), Enterococcus species, or Gram-negative bacilli (e.g., Pseudomonas aeruginosa), can also present chronically, particularly in immunocompromised hosts. Furthermore, the incidence of polymicrobial infections and culture-negative PJIs (often due to prior suppressive antibiotic use or fastidious organisms) is rising, complicating the diagnostic and therapeutic algorithm.
Untreated or inadequately managed, chronic periprosthetic infection invariably progresses to catastrophic failure of the reconstruction. The localized inflammatory response, mediated by host cytokines reacting to the bacterial presence, drives aggressive osteoclastogenesis. This results in progressive, massive periprosthetic osteolysis and subsequent mechanical loosening of the implants. The compromised bone stock dramatically increases the risk of periprosthetic fracture. Furthermore, the chronic inflammatory state leads to severe soft tissue contractures, persistent debilitating pain, and profound functional disability. In immunocompromised patients, the localized infection can eventually disseminate, leading to systemic sepsis and significant mortality.
Detailed Surgical Anatomy and Biomechanics
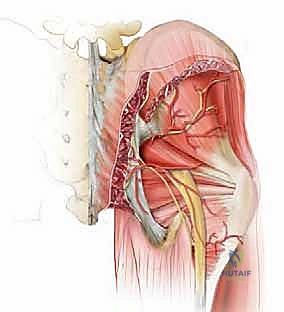
Mastery of the surgical anatomy is paramount when navigating a chronically infected, multiply operated hip. The normal tissue planes are invariably obliterated by dense, vascularized scar tissue and chronic inflammatory phlegmon. We typically utilize an extensile posterior approach, incorporating prior incisions to prevent devascularization of the skin flaps. The superficial dissection involves incising the fascia lata and splitting the gluteus maximus in line with its fibers. The gluteus maximus, innervated by the inferior gluteal nerve, must be carefully mobilized to expose the deeper structures.
The deep dissection is where the anatomical challenge truly begins. The short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus, and quadratus femoris) are often scarred directly to the posterior capsule or the implant itself. The sciatic nerve, exiting the greater sciatic foramen inferior to the piriformis (in classic anatomy), is at extreme risk during this exposure. The nerve may be encased in scar tissue, displaced by heterotopic ossification, or tethered by previous suture material. A meticulous, systematic identification of the sciatic nerve—often starting proximally at the sciatic notch and tracing it distally—is mandatory before any aggressive retractor placement or capsular release is performed.
Vascular anatomy must also be respected, particularly the medial femoral circumflex artery (MFCA), though in the setting of radical debridement for chronic infection, the primary goal is eradication of necrotic tissue, which may necessitate sacrifice of some collateral circulation. When addressing the acetabulum, the surgeon must be acutely aware of the intrapelvic vascular structures. Medial migration of an infected acetabular component can place the external iliac vessels and the obturator neurovascular bundle at imminent risk during extraction. Preoperative advanced imaging is critical to identify any intrapelvic cement or implant protrusion that dictates a highly modified, potentially combined intra- and extra-pelvic extraction approach.
The biomechanics of the antibiotic-loaded spacer are central to the success of the two-stage exchange. Historically, the first stage concluded with a resection arthroplasty (Girdlestone procedure), leaving the patient with profound limb shortening, instability, and massive dead space that complicated the eventual reimplantation. The advent of articulating antibiotic spacers revolutionized this paradigm. An articulating spacer (resembling a crude total hip arthroplasty) maintains soft tissue tension, preserves the abductor mechanism length-tension relationship, and prevents severe capsular contracture. Biomechanically, it allows for limited articulation and partial weight-bearing, dramatically improving patient function and psychological well-being between stages. Crucially, the spacer manages the dead space and acts as a local drug delivery system, providing high-dose, burst-release elution of antibiotics directly into the local environment at concentrations far exceeding systemic toxicity thresholds.
Exhaustive Indications and Contraindications
The decision to proceed with a two-stage exchange arthroplasty is governed by strict clinical criteria. It remains the absolute gold standard in North America for the management of chronic PJI. The primary indication is a confirmed chronic periprosthetic infection (typically defined as symptom onset >4 weeks post-operatively or >4 weeks of symptoms in hematogenous seeding) where the biofilm has fully matured. It is definitively indicated when a draining sinus tract is present communicating with the joint space, which represents a pathognomonic sign of deep infection and absolute failure of the current implant construct.
Furthermore, a two-stage exchange is indicated in cases where prior attempts at debridement, antibiotics, and implant retention (DAIR) have failed. It is also the procedure of choice when dealing with highly virulent, multidrug-resistant organisms (e.g., MRSA, VRE), atypical organisms (fungal or mycobacterial infections), or when the infecting organism remains unidentified preoperatively, precluding the targeted antibiotic therapy required for a single-stage exchange. Additionally, if the soft tissue envelope is severely compromised, requiring a period of healing and potential flap coverage before definitive reimplantation, the two-stage approach provides the necessary temporal window.
Contraindications, while relatively few, are absolute when present. The most profound contraindication is a patient who is medically unfit to survive two major surgical interventions. In patients with severe cardiovascular, pulmonary, or advanced systemic disease, the physiological insult of radical debridement, massive blood loss, and prolonged anesthesia may be fatal. In such cases, chronic suppressive antibiotic therapy or a definitive resection arthroplasty may be the only viable, albeit palliative, options. Another critical contraindication is the absolute lack of reconstructable bone stock or an irreparable abductor mechanism, where a second-stage reimplantation would be biomechanically impossible. In these extreme scenarios, a definitive Girdlestone resection or even proximal femoral replacement/amputation must be considered.
| Indication/Contraindication Category | Specific Clinical Scenarios | Rationale / Management Strategy |
|---|---|---|
| Absolute Indications | Chronic PJI (>4 weeks), Draining sinus tract, Failed prior DAIR procedure. | Biofilm maturation necessitates complete implant removal. Sinus tract indicates established, uncontainable local sepsis. |
| Relative Indications | Highly virulent/resistant organisms (MRSA, VRE), Culture-negative PJI, Compromised soft tissue envelope. | High risk of failure with 1-stage. 2-stage allows for local high-dose antibiotic delivery and soft tissue optimization prior to reimplantation. |
| Absolute Contraindications | Medically unstable patient (ASA 4/5 with high perioperative mortality risk), Non-ambulatory baseline. | The physiological burden of two massive surgeries outweighs the benefit. Consider suppressive antibiotics or permanent resection arthroplasty. |
| Relative Contraindications | Massive, un-reconstructable pelvic or femoral bone loss, Irreparable abductor deficiency. | If stage 2 is anatomically impossible, stage 1 spacer insertion may lead to chronic spacer retention, which carries high complication rates. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the absolute foundation of success in revision surgery for infection. The clinical evaluation must be exhaustive. A detailed history should focus on the chronicity of pain, episodes of wound drainage, prior surgical interventions, and any history of systemic bacteremia. The physical examination must assess gait, leg length discrepancy, and the integrity of the soft tissue envelope. Crucially, a comprehensive neurovascular examination must be documented preoperatively; pre-existing neuropathies (especially peroneal or sciatic) must be identified to avoid misattribution of postoperative deficits.
Laboratory investigations and joint aspiration are the cornerstones of diagnosis. Erythrocyte Sedimentation Rate (ESR) and C-reactive Protein (CRP) are the primary screening tools. According to the Musculoskeletal Infection Society (MSIS) criteria, elevated serum inflammatory markers prompt a mandatory joint aspiration. The synovial fluid must be analyzed for a cell count and differential; a synovial white blood cell (WBC) count >3,000 cells/µL or >80% polymorphonuclear leukocytes (PMNs) is highly indicative of chronic PJI. The fluid must be sent for aerobic, anaerobic, fungal, and acid-fast bacilli cultures. Crucially, the patient must undergo an "antibiotic holiday"—complete cessation of all antimicrobial therapy for a minimum of 2 to 4 weeks prior to aspiration—to maximize the yield of the cultures and avoid false negatives.
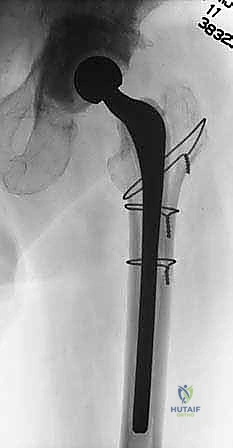
Imaging is essential for both diagnosis and surgical strategy. Standard radiographs may demonstrate subtle signs of infection such as periosteal reaction, endosteal scalloping, or rapid, aggressive osteolysis.

Above: Radiograph demonstrating a sinus tract extending through the lateral cortex, a pathognomonic sign of chronic, uncontrolled deep infection.

Above: Radiograph showing extensive periosteal reaction and a sinus tract through the posteromedial cortex, indicating aggressive osteomyelitis secondary to the implant.
Advanced imaging, including CT scans with metal artifact reduction, is often utilized to quantify bone loss, assess component fixation, and critically, to identify any intrapelvic cement or medial wall defects that could lead to catastrophic vascular injury during acetabular extraction.
Above: Preoperative templating and advanced imaging are critical to anticipate bone defects and plan the dimensions of the articulating spacer.
Patient positioning must facilitate extensile exposure and intraoperative fluoroscopy. We position the patient in the lateral decubitus position on a radiolucent table, utilizing a rigid pelvic positioner or beanbag. The pelvis must be perfectly perpendicular to the floor to ensure accurate assessment of component version during spacer insertion. All pressure points, particularly the contralateral peroneal nerve at the fibular head and the axilla, must be meticulously padded. The operative leg is draped completely free to allow for extreme ranges of motion necessary for component dislocation and extraction. Intraoperative fluoroscopy must be readily available and its trajectory confirmed prior to making the incision, as it will be heavily relied upon to confirm complete cement removal and optimal spacer seating.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach begins with the excision of any previous surgical scars and, critically, the en bloc excision of any established sinus tracts down to the fascial layer. We utilize a standard posterior approach, splitting the gluteus maximus and meticulously identifying and protecting the sciatic nerve, which is frequently encased in dense perineural fibrosis.

Above: Careful isolation and protection of the sciatic nerve during the deep exposure, navigating through dense scar tissue.
Once the joint is accessed, the hip is dislocated. If the hip cannot be safely dislocated due to severe contracture or protrusio, the femoral neck of the implant or the native bone may need to be transected in situ.
The extraction of the infected components must be methodical to preserve remaining bone stock. The femoral component is addressed first. Loose stems can often be extracted with a slap hammer. However, well-fixed, fully porous-coated stems or well-fixed cemented stems present a significant challenge. We frequently employ an Extended Trochanteric Osteotomy (ETO) to facilitate safe extraction of the stem and cement mantle without causing an uncontrolled diaphyseal fracture.

Above: Utilizing specialized extraction instrumentation to remove a well-fixed femoral component after adequate exposure is achieved.
Above: Complete removal of the femoral stem, revealing the compromised endosteal canal that will require aggressive debridement.
Acetabular extraction follows. Well-fixed porous shells are carefully explanted using curved osteotomes or specialized explant systems (e.g., Explant, Zimmer) to minimize damage to the acetabular rim and columns.
Following complete hardware removal, the most critical phase of the operation commences: the radical debridement. This must be executed with oncologic principles—a "tumor-like" resection of all infected, necrotic, and devascularized tissue. A complete synovectomy is performed. The acetabulum is reamed to bleeding, healthy subchondral bone. The femoral canal is aggressively reamed using flexible reamers to remove the infected endosteal membrane, followed by thorough brushing.
Above: Aggressive debridement of the acetabulum using hemispherical reamers to expose bleeding, viable bone.

Above: Preparation of the femoral canal, ensuring all necrotic endosteal tissue and residual cement are meticulously eradicated.
The entire surgical field is then subjected to high-volume pulsatile lavage using a minimum of 6 to 9 liters of normal saline, often supplemented with dilute betadine or chlorhexidine solutions, to mechanically disrupt any remaining biofilm.
With the debridement complete, we turn to the fabrication of the articulating antibiotic-loaded cement spacer. We utilize high-viscosity polymethylmethacrylate (PMMA) bone cement (e.g., Palacos or Simplex). The cement is hand-mixed (vacuum mixing is avoided to increase porosity and enhance antibiotic elution) with high doses of heat-stable antibiotics. A standard regimen involves adding 3 to 4 grams of Vancomycin and 3.6 to 4.8 grams of Tobramycin per 40-gram bag of cement. This high ratio intentionally compromises the mechanical strength of the cement to maximize the surface area for rapid, burst-release antibiotic elution.

Above: Hand-mixing the PMMA bone cement with high-dose, broad-spectrum powdered antibiotics.

Above: The doughy antibiotic-loaded cement is prepared for insertion into the specialized silicone molds.
The doughy cement is placed into specialized silicone molds (such as the PROSTALAC system) that contain a central stainless steel endoskeleton for structural support.
The spacer components are then inserted. The femoral spacer is seated into the prepared canal, ensuring appropriate version and height to restore leg length and soft tissue tension. The acetabular spacer is molded directly into the reamed acetabulum, often utilizing a trial head to create a congruent articulating surface.

Above: The fabricated articulating spacer is carefully extracted from the silicone mold.

Above: Insertion of the femoral component of the articulating spacer into the debrided femoral canal.

Above: Ensuring appropriate seating and version of the femoral spacer to optimize biomechanical stability.

Above: Final reduction of the articulating spacer, confirming stability, range of motion, and adequate soft tissue tensioning.
Once the cement has fully polymerized, the hip is reduced, and stability is meticulously assessed. The wound is closed in multiple layers over deep subfascial drains to manage the anticipated postoperative hematoma and dead space.

Above: Layered, watertight closure of the soft tissue envelope is crucial to prevent postoperative sinus tract formation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the first stage of a two-stage exchange is fraught with potential complications due to the severely compromised nature of the host tissues and the inherent biomechanical limitations of cement spacers. Spacer dislocation is one of the most frequent mechanical complications, occurring in 5% to 15% of cases. This instability is driven by massive bone loss, abductor mechanism insufficiency, and the imperfect geometry of the handcrafted spacer. Management of a dislocated spacer typically involves an initial attempt at closed reduction under conscious sedation. If closed reduction fails or the spacer is chronically unstable, open revision of the spacer is mandated to prevent devastating soft tissue contractures and damage to the remaining bone stock.
Intraoperative periprosthetic fractures are a significant risk during both the extraction of well-fixed implants and the aggressive reaming required for debridement. The incidence ranges from 3% to 10%. Cortical perforations or non-displaced linear fractures recognized intraoperatively must be immediately bypassed with the stem of the spacer and frequently augmented with cerclage wiring or strut allografts. Failure to address these fractures can lead to catastrophic failure of the spacer construct, severe pain, and the inability to mobilize the patient between stages.
The most devastating complication is the failure to eradicate the infection, which occurs in approximately 10% to 15% of two-stage exchanges. Persistent infection is typically heralded by persistently elevated inflammatory markers, chronic wound drainage, or a positive aspiration prior to the planned second stage. Salvage management in this scenario requires a complete repetition of the first stage: removal of the spacer, a secondary radical debridement, and insertion of a new antibiotic-loaded spacer with an adjusted antimicrobial profile based on updated cultures. In hosts with severely compromised immune systems or un-reconstructable bone loss, salvage may ultimately necessitate a permanent Girdlestone resection arthroplasty or, rarely, hip disarticulation.
Systemic toxicity from the high-dose local antibiotics is a rare but documented complication. Acute kidney injury (AKI) secondary to massive aminoglycoside (Tobramycin/Gentamicin) or Vancomycin elution can occur, particularly in elderly patients with pre-existing renal impairment. The incidence of clinically significant AKI is low (<3%), but it necessitates rigorous postoperative monitoring of serum creatinine and potentially serum antibiotic trough levels, requiring prompt collaboration with nephrology and infectious disease specialists if renal function deteriorates.
| Complication | Estimated Incidence | Primary Cause / Risk Factor | Salvage / Management Strategy |
|---|---|---|---|
| Spacer Dislocation | 5% - 15% | Abductor deficiency, severe bone loss, improper spacer sizing/version. | Closed reduction. If unstable, open revision and exchange of the spacer construct. |
| Periprosthetic Fracture | 3% - 10% | Aggressive extraction of fixed stems, compromised osteoporotic bone. | Intraoperative cerclage wiring, bypass with a longer spacer stem, restricted weight-bearing. |
| Persistent Infection | 10% - 15% | Inadequate debridement, retained cement/biofilm, highly resistant organisms. | Repeat Stage 1 (spacer exchange), prolonged IV antibiotics. Consider permanent resection if unresolvable. |
| Acute Kidney Injury (AKI) | 1% - 3% | Systemic absorption of high-dose local aminoglycosides/vancomycin. | Aggressive IV hydration, nephrology consult, monitor |
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding resection-arthroplasty-and-spacer-insertion