Masterclass: Williams Rod Fixation for Congenital Tibial Pseudarthrosis

Key Takeaway
This masterclass guides fellows through Williams rod fixation for congenital pseudarthrosis of the tibia. We cover essential preoperative planning, precise patient positioning, and a granular, real-time breakdown of intraoperative execution, from meticulous dissection and canal preparation to rod insertion and bone grafting. Extensive pearls, pitfalls, and postoperative management strategies are discussed to ensure optimal outcomes for this challenging condition.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and to this definitive masterclass. Today, we are tackling one of the most notoriously challenging and historically frustrating conditions in pediatric orthopedics: the surgical reconstruction of congenital pseudarthrosis of the tibia (CPT) utilizing the Williams intramedullary rod. This condition, intimately associated with Neurofibromatosis Type 1 (NF1), demands not only meticulous preoperative planning and precise intraoperative execution but also a profound understanding of the underlying aberrant biology. Our ultimate goal is to achieve lasting osseous consolidation, minimize secondary angular deformity, and restore durable, functional ambulation for our young patients, thereby avoiding the devastating endpoint of amputation.

Let us begin by reviewing the fundamental patho-epidemiology of this unique disease process. Congenital pseudarthrosis of the tibia represents a pathologic fracture of a tibia that was structurally and biologically abnormal from birth. While the genetic and cellular abnormality is inherent—often linked to a mutation in the NF1 gene which encodes the tumor suppressor protein neurofibromin—the frank pseudarthrosis often only becomes clinically apparent once weight-bearing commences and mechanical stress is applied to the dysplastic bone. The local environment at the pseudarthrosis site is characterized by a thick, hamartomatous cuff of fibrous tissue. This tissue is highly cellular, aggressively osteoclastic, and profoundly anti-osteogenic, effectively strangling the underlying bone and preventing normal fracture healing.
Typically, patients present in infancy or early childhood with progressive anterolateral bowing of the tibia. This characteristic bowing, often accompanied by increasing mechanical instability, inevitably leads to a pathologic fracture if left untreated. Shortening of the involved extremity may not be immediately apparent at initial presentation but becomes rapidly progressive after the fracture occurs, driven by both bone loss at the pseudarthrosis site and growth inhibition of the adjacent physes. Pain is usually absent unless an acute fracture has just occurred, though observant parents may note a progressive limp, recurrent tripping, or a dull aching preceding the catastrophic failure of the bone.
It is absolutely crucial to inspect the skin meticulously during the initial physical examination. Over half of these patients will carry a formal diagnosis of Neurofibromatosis Type 1. You must actively search for the classic cutaneous stigmata: café-au-lait spots (irregularly shaped, hyperpigmented macules), axillary or inguinal freckling (Crowe's sign), and the presence of cutaneous or subcutaneous neurofibromas. A detailed family history regarding NF1 must be elicited. If NF1 is suspected but not previously diagnosed, immediate referral to a medical geneticist for confirmation and comprehensive counseling is highly recommended. The natural history of an established, untreated pseudarthrosis is one of relentless non-union, progressive instability, and severe limb shortening, ultimately severely impairing the child's ability to walk.
Detailed Surgical Anatomy and Biomechanics
To successfully navigate the surgical management of CPT, a masterful understanding of the distorted local anatomy is required. The tibia, our primary focus, is structurally abnormal in these patients, often presenting with cystic, sclerotic, or severely atrophic changes within its medullary canal. The pseudarthrosis itself is enveloped by the aforementioned hamartomatous fibrous tissue—which is not a true neurofibroma, but rather a hypervascular, fibromatous proliferation—typically located in the middle to distal third of the tibial diaphysis. The medullary canal architecture is critical to our operative plan; we are aiming for a perfectly straight, central path for our Williams rod. Pre-existing severe bowing, dense endosteal sclerosis, or complete obliteration of the canal can make achieving this trajectory exceptionally challenging.

The proximal and distal tibial physes are vital anatomical landmarks for rod length determination, especially in our growing pediatric population. The Williams rod is uniquely designed to accommodate this growth. It is a telescoping system consisting of a female component that anchors distally (often crossing the ankle into the talus and calcaneus in very young children) and a male component that slides within it proximally. This biomechanical design is genius: it provides rigid intramedullary stabilization across the pseudarthrosis site while simultaneously allowing the male rod to passively extrude from the female receptacle as the child grows, thereby preventing the rod from tethering the physes or migrating unpredictably.

The fibula plays a highly significant, and often problematic, role in the biomechanics of the lower leg in CPT. Its involvement is highly variable; it may be independently bowed, frankly pseudarthrotic, or completely intact. An intact, thickened fibula can act as a rigid lateral tether, actively hindering our ability to achieve anatomic tibial reduction and adequate axial compression at the tibial pseudarthrosis site. In such cases, an aggressive fibular osteotomy or partial diaphyseal resection is absolutely mandatory. Conversely, if a fibular pseudarthrosis is present, it must be rigidly stabilized—typically with an intramedullary Kirschner wire or small elastic nail—to restore the lateral column of the leg and prevent progressive valgus deformity of the ankle over time.
From a neurovascular perspective, the risks are substantial. During our anterior approach along the subcutaneous border of the tibia, we must be exquisitely mindful of the anterior compartment structures. The deep peroneal nerve and the anterior tibial artery and veins lie lateral to the tibia; while our direct anterior approach is generally safe, aggressive lateral subperiosteal dissection or eccentric lateral reaming could risk devastating injury. When addressing the fibula, particularly during a proximal osteotomy or K-wire insertion, extreme caution must be exercised to avoid injury to the common peroneal nerve as it courses around the fibular neck. Furthermore, if the Williams rod is templated to cross the ankle joint, precise, dead-center alignment through the talus and calcaneus is paramount to avoid neurovascular compromise to the plantar aspect of the foot and to prevent iatrogenic subtalar stiffness or deformity.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention utilizing a Williams rod is not to be taken lightly. Nonoperative measures, such as total-contact ankle-foot orthoses (AFO) or knee-ankle-foot orthoses (KAFO), are generally reserved for the pre-fracture stage (Crawford Type I or II) to provide mechanical support, slow the progression of bowing, and postpone the need for surgery. Delaying surgery safely allows the child to grow, permitting the use of a larger diameter intramedullary rod and yielding a greater volume of autologous iliac crest bone graft. However, once a frank pseudarthrosis is established (Crawford Type IV), it will never resolve spontaneously, and operative treatment becomes absolutely indicated.
| Parameter | Indications for Williams Rod Fixation | Contraindications for Williams Rod Fixation |
|---|---|---|
| Pathology Status | Established congenital pseudarthrosis of the tibia (Crawford Type IV). | Pre-fracture anterolateral bowing without frank non-union (Relative contraindication; bracing preferred). |
| Patient Age | Generally >18-24 months (allows for sufficient canal diameter and bone graft harvest). | Infants <12 months (anatomy too small, high failure rate, bracing preferred until larger). |
| Prior Surgeries | Primary surgical intervention or revision of previously failed alternative fixations (e.g., plates, external fixators). | Active, fulminant deep osteomyelitis at the pseudarthrosis site. |
| Canal Morphology | Sufficient proximal and distal medullary canal to accept at least the smallest available Williams rod. | Completely obliterated, un-reamable canal over the entire length of the tibia (requires alternative salvage). |
| Soft Tissue Envelope | Adequate, healthy anterior skin coverage to allow for tension-free closure over the bone graft. | Severe soft tissue compromise, active ulceration, or massive skin defects requiring free flap coverage prior to bone work. |
The primary indication for the Williams rod technique is an established CPT in a child who has adequate bone stock to accept the intramedullary device. It is particularly advantageous in younger children where preservation of growth potential is critical, as the telescoping nature of the rod accommodates longitudinal growth better than static locked nailing or rigid plating. It is also an excellent option for revision cases where previous external fixation or plating has failed, provided the medullary canal can be reconstituted.
Contraindications must be strictly respected to avoid catastrophic failure. Active infection is an absolute contraindication; any history of prior infection requires a thorough workup, including inflammatory markers and potentially a pre-operative aspiration or biopsy, before proceeding with hardware implantation. Severe soft tissue compromise over the anterior tibia is a major red flag. The hamartomatous tissue resection and subsequent massive bone grafting require pristine, well-vascularized skin for coverage. If the skin is compromised, a plastic surgery consultation for a rotational or free flap is required before any osseous reconstruction is attempted. Finally, in extremely young infants, the sheer lack of physical space in the medullary canal and the inadequate volume of available autologous bone graft make this procedure highly prone to failure; these patients are best managed with rigid custom bracing until they reach an appropriate size.
Pre-Operative Planning, Templating, and Patient Positioning
Mastery of this procedure begins long before the first incision, relying heavily on exhaustive preoperative planning and precise radiographic templating. High-quality, orthogonal Anteroposterior (AP) and lateral radiographs of the entire affected tibia, including the knee and ankle joints, are non-negotiable. You must meticulously assess the morphology of the pseudarthrosis—whether it is cystic, sclerotic, or atrophic—and note the extent of the dysplastic bone involvement throughout the tibial diaphysis. Evaluate the medullary canal for widening or narrowing, as this will dictate your reaming strategy. Furthermore, assess the fibula for independent bowing or pseudarthrosis, as this will dictate whether a concurrent fibular procedure is required to achieve tibial union.

Templating the Williams rod requires careful attention to both diameter and length. The system utilizes a female coupling that remains anchored distally and a male coupling that acts as the proximal telescoping segment. The diameter is dictated by the narrowest portion of the healthy medullary canal adjacent to the pseudarthrosis; we always aim for the largest diameter that can be safely inserted to maximize bending stiffness and rotational stability. Length determination is highly dependent on the child's age and the location of the pseudarthrosis. In younger children (typically under 8 years) or those with a very distal pseudarthrosis, the female component must cross the ankle and subtalar joints, anchoring securely into the calcaneus to provide adequate distal fixation. In older children with sufficient distal tibial bone stock, the rod can be contained entirely within the tibia. You must accurately calculate the anticipated length of the dysplastic tibia to be resected (usually 1 to 3 cm) and subtract this from your overall rod length measurement.

Patient positioning is paramount for optimal surgical access, unhindered fluoroscopy, and the prevention of intraoperative complications. The procedure demands a general anesthetic. We invariably begin by harvesting the autologous iliac crest bone graft before positioning the patient for the tibial reconstruction. For smaller children, this is done in the lateral decubitus position to access the posterior iliac crest, which yields a higher volume of rich cancellous bone. For larger children, the anterior iliac crest is accessed in the supine position with a small bump under the ipsilateral hip.
Once the graft is harvested and safely stored on the back table, the patient is positioned completely supine. The entire affected lower extremity, from the midthigh down to the toes, is prepped and draped in a sterile fashion. A sterile thigh tourniquet is applied high on the thigh to ensure a bloodless field during the meticulous resection of the hamartoma. Crucially, the C-arm must be positioned to obtain true AP and lateral views of the entire tibia, ankle, and foot without requiring the surgical team to reposition the patient's leg. The foot must remain freely mobile for intraoperative manipulation; this is essential to maintain neutral alignment during the trans-calcaneal insertion of the rod, preventing iatrogenic equinus or valgus deformities.
Step-by-Step Surgical Approach and Fixation Technique
We now transition to the operative execution. The tourniquet is inflated to 250-300 mmHg. A longitudinal incision, typically 6 to 8 cm in length, is made directly over the anterior subcutaneous border of the tibia, centered over the apex of the pseudarthrosis. The dissection is carried sharply down through the subcutaneous tissue directly to the bone.

The first critical step is the radical excision of the pseudarthrosis and its surrounding hamartomatous tissue. This is not a simple fracture takedown; it is akin to a marginal tumor resection. The thickened, fibrous periosteum—which is biologically active and anti-osteogenic—must be meticulously excised completely around the circumference of the bone at the non-union site. We use a combination of sharp dissection, curettes, and rongeurs to resect 1 to 2 cm of the abnormal, sclerotic bone ends until we reach healthy, bleeding, punctate cortical bone both proximally and distally. If significant angular deformity persists after this excision, a formal corrective osteotomy of the proximal or distal segment may be required to allow a straight rod to pass centrally within the medullary canal.

Next, we prepare the medullary canal. In CPT, the canal is often obliterated by dense endosteal sclerosis. We utilize sequential rigid reamers, starting with a small drill bit or a high-speed burr, to carefully open the canal both proximally and distally. This must be done under strict fluoroscopic guidance to avoid eccentric reaming or iatrogenic cortical perforation. The canal is over-reamed by 0.5 to 1.0 mm greater than the templated diameter of the Williams rod to allow for smooth insertion without excessive hoop stresses that could split the dysplastic bone.


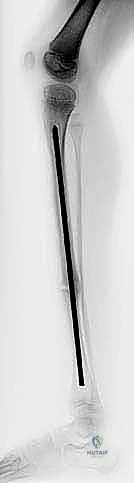
Rod insertion begins with the distal segment. If the plan dictates crossing the ankle, the foot is held in strict neutral dorsiflexion and neutral heel alignment. A guide pin is passed antegrade through the distal tibial segment, across the center of the talar dome, and out through the plantar aspect of the calcaneus. The female component of the Williams rod is then introduced retrograde over this guide wire, passing from the plantar aspect of the foot, through the calcaneus and talus, and into the distal tibial segment until the proximal end of the female receptacle is flush with the resection site.


The male component of the rod is then inserted antegrade into the proximal tibial segment. This requires careful manipulation to ensure it travels centrally up the medullary canal toward the proximal tibial physis, stopping just short of the growth plate. Once both components are independently seated, the critical step of docking occurs. The proximal tibial segment (containing the male rod) is manipulated to align with the distal segment. The male rod is then advanced distally so that it slides perfectly into the female receptacle.


At this juncture, we must address the fibula. If the fibula is intact and preventing axial compression at the tibial pseudarthrosis site, a separate lateral incision is made, and a 1 cm segment of the fibular diaphysis is resected. If the fibula is pseudarthrotic, it is opened, the fibrous tissue is excised, and it is stabilized with a retrograde intramedullary K-wire. With the fibula addressed, robust axial compression is applied across the tibial pseudarthrosis site. The telescoping nature of the Williams rod allows the bone ends to intimately impact against one another.


The final, and arguably most biologically important, step is the bone grafting. The previously harvested autologous iliac crest bone graft is meticulously packed around the entire circumference of the tibial docking site. We aim for a voluminous, 360-degree biological fusion mass. The tourniquet is deflated, meticulous hemostasis is achieved, and the wound is closed in layers. It is imperative that the skin closure is completely tension-free over the massive bone graft to prevent wound necrosis and subsequent deep infection.

Complications, Incidence Rates, and Salvage Management
Despite flawless surgical technique, the complication rate in the treatment of congenital pseudarthrosis of the tibia remains notoriously high. The underlying genetic and biological defects mean that these bones possess a profound reluctance to heal. Parents must be extensively counseled preoperatively that multiple surgical interventions are the statistical norm, not the exception, and that the road to skeletal maturity is fraught with potential setbacks.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Persistent Nonunion | 20% - 40% | Incomplete hamartoma resection, inadequate bone graft, premature weight-bearing, severe NF1 phenotype. | Revision surgery with repeat radical resection, BMP-2 application, massive structural allograft/autograft, or conversion to Ilizarov bone transport. |
| Rod Migration / Extrusion | 15% - 25% | Failure of the telescoping mechanism, rod too short, distal migration through the calcaneus due to osteopenia. | Hardware revision; if distal extrusion occurs, the rod must be advanced proximally or replaced. May require custom shoe wear modifications. |
| Ankle Valgus Deformity | 30% - 50% | Unaddressed fibular pseudarthrosis, proximal migration of the lateral malleolus, asymmetric distal tibial physeal growth. | Distal tibial medial hemiepiphysiodesis (guided growth), supramalleolar corrective osteotomy, or fibular lengthening procedures. |
| Refracture | 25% - 35% | Premature hardware removal, failure to maintain long-term bracing, stress riser at the end of the rod. | Immediate re-institution of non-weight-bearing cast. Often requires revision intramedullary nailing with a larger/longer device and repeat bone grafting. |
| Deep Surgical Infection | 5% - 10% | Tension on the skin closure over massive bone graft, poor vascularity of the dysplastic soft tissue envelope. | Aggressive operative debridement, hardware retention (if stable) or removal (if loose/biofilm present), culture-directed IV antibiotics, potential flap coverage. |
Persistent nonunion is the most dreaded complication. If the bone fails to consolidate within 6 to 9 months, or if hardware failure occurs prior to union, revision surgery is mandatory. Salvage techniques often involve a more aggressive resection, the off-label use of recombinant human Bone Morphogenetic Protein-2 (rhBMP-2) to stimulate osteoinduction, or the application of a circular external fixator (Ilizarov method) for compression or bone transport.
Ankle valgus is an insidious complication that often develops years after a successful tibial union. It is primarily driven by a persistent fibular pseudarthrosis that allows the lateral malleolus to migrate proximally, removing the lateral buttress of the talus. This highlights the absolute necessity of addressing the fibula during the index procedure. If valgus develops, it must be aggressively managed with guided growth (medial hemiepiphysiodesis) or a formal supramalleolar osteotomy to prevent long-term joint degeneration.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following Williams rod fixation is exceptionally conservative and requires immense dedication from both the patient and the family. The biological healing of a CPT is measured in months and years, not weeks. Immediately postoperatively, the patient is placed in a sterile, well-padded, long-leg bent-knee cast. The patient is made strictly non-weight-bearing on the operative extremity. This initial cast is typically maintained for 6 to 8 weeks to allow for initial soft tissue healing and the very early stages of graft incorporation.
Following the initial casting phase, the patient is transitioned to a custom-molded, clamshell-style knee-ankle-foot orthosis (KAFO) or a rigid ankle-foot orthosis (AFO), depending on the level of the pseudarthrosis and the stability of the fixation. Radiographs are obtained at 4-week intervals to meticulously monitor the incorporation of the bone graft and the progression of the union. Weight-bearing is advanced at a glacial pace. Touch-down weight-bearing may be initiated only when there is definitive radiographic evidence of bridging callus across at least three cortices, which rarely occurs before the 3-month mark.
It is a fundamental tenet of CPT management that the affected limb must remain continuously braced until the child reaches skeletal maturity. Even after solid radiographic union is achieved, the dysplastic bone remains highly susceptible to refracture. The intramedullary rod is generally left in place permanently; hardware removal is explicitly contraindicated unless the rod is causing severe soft tissue irritation, has broken, or has migrated to a degree that it threatens skin integrity or joint function. The family must understand that the brace is as crucial to the long-term success of the procedure as the surgery itself.
Summary of Landmark Literature and Clinical Guidelines
The evolution of CPT management has been shaped by several key contributors and landmark studies. The original description of the telescoping rod technique by Williams revolutionized the approach, providing a biomechanical solution that respected the need for longitudinal growth while maintaining continuous intramedullary stability. His early case series demonstrated a marked improvement in union rates compared to historical plating or casting techniques.
Subsequent work by Crawford established the widely utilized classification system for CPT, which remains critical for prognosticating the natural history and guiding the timing of surgical intervention. Crawford's Type IV (frank pseudarthrosis) remains the absolute indication for the aggressive surgical approach detailed in this chapter. More recently, the work of Paley and others has emphasized the concept of the "cross-union." Paley advocates for not only achieving union of the tibia but intentionally creating a synostosis between the tibia and the fibula at the pseudarthrosis site to massively increase the cross-
