Mastering Two-Stage Hip Reimplantation for Periprosthetic Joint Infection

Key Takeaway
This masterclass guides you through two-stage hip reimplantation for periprosthetic joint infection. We cover essential preoperative planning, precise patient positioning, and meticulous intraoperative execution, from initial exposure and spacer removal to definitive acetabular and femoral component implantation. Learn critical anatomical considerations, advanced surgical techniques, and strategies to manage potential pitfalls for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the advanced discourse on one of the most formidable challenges in modern orthopedic surgery: the two-stage hip reimplantation for periprosthetic joint infection (PJI). This procedure is not merely a mechanical replacement of a compromised articulation; it is a profound biological and structural reconstruction aimed at eradicating a virulent pathogen while simultaneously restoring biomechanical function to a severely debilitated patient. As the burden of total hip arthroplasty (THA) increases globally, so too does the absolute number of PJIs, necessitating a masterful command of this salvage operation. The two-stage exchange remains the gold standard in North America for chronic PJI, offering the highest historical rates of infection eradication compared to single-stage or suppressive therapies.
To truly master this procedure, the orthopedic surgeon must first possess a deep understanding of the pathophysiology of PJI, specifically the lifecycle of the bacterial biofilm. Planktonic bacteria, once introduced into the periprosthetic space, rapidly adhere to the inert surface of the implant and undergo a phenotypic shift, secreting a protective extracellular polymeric substance (EPS). This sessile biofilm community is highly resistant to host immune responses and systemic antimicrobial therapy, rendering the implant a permanent nidus for infection. The first stage of our protocol—radical explantation of all foreign material, aggressive thorough debridement of non-viable tissue, and the insertion of an antibiotic-eluting spacer—is designed to dismantle this biofilm and deliver high local concentrations of bactericidal agents.
The epidemiology of PJI dictates that we will encounter this pathology with increasing frequency. While the infection rate following primary THA hovers between 1% and 2%, the rate following revision arthroplasty can escalate to 5% or higher. The economic burden on the healthcare system is staggering, but it is the profound morbidity inflicted upon the patient that demands our utmost clinical rigor. Patients presenting for the second stage of this protocol have already endured months of functional limitation, systemic antibiotic therapy, and psychological distress. Our objective in the reimplantation phase is to definitively close this chapter of their pathology by confirming the eradication of the pathogen and executing a flawless, durable mechanical reconstruction.
Clinically, differentiating persistent infection from the expected postoperative state of a patient with a temporary spacer is paramount. Patients with an infected primary or revision THA almost universally complain of constant, unrelenting pain, often exacerbated at rest and during the night. This is a stark contrast to the mechanical pain of aseptic loosening, which is typically activity-dependent and relieved by rest. During the inter-stage period, we must maintain a high index of suspicion for persistent infection, monitoring for delayed wound healing, chronic serous or purulent drainage, or systemic signs of inflammation. The successful execution of the second stage relies entirely on the biological success of the first stage; proceeding with reimplantation in the face of persistent infection is a catastrophic error that guarantees failure.
Detailed Surgical Anatomy and Biomechanics
The surgical anatomy encountered during a two-stage hip reimplantation is vastly different from that of a primary arthroplasty. The normal tissue planes have been obliterated by previous surgical interventions, chronic inflammation, and the subsequent fibrotic healing response. The posterolateral approach remains our workhorse due to its extensile nature and the unparalleled exposure it affords to both the acetabulum and the proximal femur. However, traversing the gluteus maximus and the fascia lata in a revision setting requires meticulous, sharp dissection. The surgeon must be prepared to encounter a dense, unyielding scar carapace that encapsulates the joint and tethers critical neurovascular structures.
The most critical anatomical consideration during the posterolateral approach is the protection of the sciatic nerve. In the setting of severe scarring, chronic inflammation, or a previously placed bulky antibiotic spacer, the normal anatomical relationships of the sciatic nerve are frequently distorted. It may be encased in scar tissue, tethered to the posterior capsule, or displaced laterally. We must be prepared to formally expose and perform a neurolysis of the nerve as it emerges deep and inferior to the piriformis muscle and courses superficial to the obturator internus. This requires careful, sharp dissection through fibrotic tissue, maintaining the hip in slight internal rotation and extension to minimize tension on the nerve during exposure.
If a direct lateral (transgluteal) approach was utilized during the primary surgery or the first-stage explantation, the surgeon must be acutely aware of the superior gluteal nerve. This nerve, located approximately 3 to 5 centimeters proximal to the tip of the greater trochanter, innervates the gluteus medius, gluteus minimus, and tensor fasciae latae. Iatrogenic injury to this nerve during the proximal extension of the split will lead to catastrophic abductor insufficiency, resulting in a permanent, debilitating Trendelenburg gait and profound postoperative instability. Meticulous dissection, the avoidance of aggressive proximal retraction, and the use of stay sutures rather than heavy retractors in the proximal aspect of the wound are non-negotiable principles.
Biomechanically, the goal of the reimplantation is to restore the hip center of rotation, optimize the abductor moment arm, and equalize leg lengths. Acetabular bone loss, classified by the Paprosky system, dictates our reconstructive strategy. The safe zone for acetabular screw placement remains the posterior-superior quadrant, which avoids the external iliac vessels anteriorly and the obturator nerve and vessels inferiorly. Femoral reconstruction must address metaphyseal and diaphyseal bone loss, often necessitating the use of modular, fluted, tapered titanium stems that achieve diaphyseal fixation, bypassing proximal deficiencies by at least two cortical diameters. Restoring the native femoral offset is critical to tensioning the abductor musculature, thereby providing the necessary compressive forces across the joint to prevent postoperative dislocation.
Exhaustive Indications and Contraindications
The decision to proceed with the second stage of a two-stage reimplantation is one of the most critical junctures in the management of PJI. The primary indication for reimplantation is the definitive clinical and serological evidence that the periprosthetic infection has been eradicated following the first-stage explantation and a targeted course of systemic antibiotics. This requires a multidisciplinary approach, heavily relying on the expertise of our infectious disease colleagues. The patient must demonstrate a benign clinical exam, a well-healed surgical incision without erythema or drainage, and a progressive normalization of systemic inflammatory markers.
Contraindications to reimplantation are absolute and must be respected to prevent the devastating complication of a reinfected revision arthroplasty. Persistent or recalcitrant infection, confirmed by persistently elevated inflammatory markers, positive synovial fluid cultures, or a high synovial white blood cell count, strictly precludes the insertion of permanent components. Furthermore, patients who are medically unfit to undergo a massive reconstructive procedure, or those with an irreparably compromised soft tissue envelope that cannot provide adequate coverage for the new prosthesis, are not candidates for reimplantation. In such scenarios, salvage procedures must be considered.
To formalize the decision-making process, we rely on a rigorous protocol of preoperative testing. A minimum "antibiotic holiday" of two to four weeks is mandatory prior to joint aspiration to prevent false-negative culture results. The aspiration fluid is analyzed for cell count, differential, and extended cultures (aerobic, anaerobic, fungal, and mycobacterial). Emerging biomarkers, such as alpha-defensin and leukocyte esterase, provide additional diagnostic accuracy in equivocal cases. The Musculoskeletal Infection Society (MSIS) criteria serve as our definitive framework for confirming the absence of infection prior to proceeding to the operating theater.
| Clinical Parameter | Indications for Reimplantation | Contraindications for Reimplantation |
|---|---|---|
| Clinical Status | Healed wound, absence of rest pain, no sinus tract | Persistent drainage, erythema, severe rest pain |
| Serology (ESR/CRP) | Normalized or steadily trending downward | Persistently elevated without alternative explanation |
| Synovial Fluid (Aspiration) | WBC < 3,000 cells/µL, PMN < 80%, Negative cultures | WBC > 3,000 cells/µL, PMN > 80%, Positive cultures |
| Host Status (Cierny-Mader) | Type A or optimized Type B host | Type C host (prohibitive surgical risk) |
| Soft Tissue Envelope | Adequate viable muscle and skin coverage | Massive necrosis, inability to close over hardware |
If the evaluation reveals persistent infection, the surgeon must abort the plan for reimplantation. The appropriate course of action is a repeat first-stage procedure: removal of the current antibiotic spacer, a renewed radical debridement of all infected bone and soft tissue, and the placement of a new, freshly mixed antibiotic-laden spacer, followed by another prolonged course of culture-directed systemic antibiotics.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the blueprint for success in complex revision arthroplasty; a failure to plan is a plan to fail. Our initial assessment begins with a comprehensive medical optimization of the host. Risk factors such as diabetes mellitus, malnutrition (assessed via serum albumin and prealbumin), chronic skin lesions, and immunosuppression must be aggressively managed. A complete neurological and vascular examination is paramount, documenting any preexisting deficits, such as a partial foot drop or weak leg extensors, which will heavily influence our intraoperative approach and postoperative expectations.

FIG 1A • Preoperative radiograph: Pelvis (AP view) demonstrating an antibiotic spacer in situ with significant acetabular bone loss.

FIG 1B • Preoperative radiograph: AP view of the femur, crucial for assessing diaphyseal bone quality and spacer fixation.

FIG 1D • Preoperative radiograph: Iliac oblique view, utilized to evaluate the integrity of the posterior column.
Radiographic assessment requires a high-quality series of plain films, including an anteroposterior (AP) view of the pelvis, an AP and lateral view of the full length of the femur, and Judet views if acetabular column compromise is suspected. Computed Tomography (CT) scans with metal artifact reduction sequences (MARS) are invaluable for quantifying the exact magnitude and morphology of acetabular and femoral bone defects. These imaging modalities allow us to classify the bone loss and anticipate the necessity for specialized reconstructive implants, such as highly porous metal augments, cup-cage constructs, or modular diaphyseal-fitting femoral stems.

FIG 2 • Preoperative templating is essential to determine the diameter and length of the implant, restoring the center of rotation and leg length.
Careful preoperative templating is absolutely essential. We utilize digital templating software to predict implant size, length, and necessary offset. The contralateral, uninfected hip often serves as our template for restoring the native center of rotation and equalizing leg lengths. We must ensure that our selected femoral implant can bypass any cortical defects or stress risers by a minimum of two cortical diameters to prevent periprosthetic fractures. Furthermore, the surgeon must ensure that a wide array of specialized revision instruments, explantation tools, and backup implant systems are physically present in the operating room prior to the induction of anesthesia.
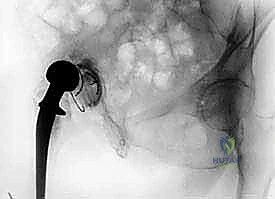
FIG 3 • Patient positioned securely in the lateral decubitus position, ensuring strict verticality of the pelvis.
Patient positioning is a critical first step that must be performed under the direct, unyielding supervision of the attending surgeon. The patient is placed in the lateral decubitus position utilizing robust anterior and posterior supports, such as a pegboard or a rigid beanbag system. Crucially, the pelvis must be perfectly vertical and orthogonal to the floor. Any unrecognized tilt or roll of the pelvis will directly translate into the malpositioning of the acetabular component, leading to altered biomechanics, impingement, and a high risk of postoperative dislocation. The operative leg is draped completely free to allow for a full, unrestricted range of motion during the procedure, which is vital for trial reduction and rigorous stability testing.
Step-by-Step Surgical Approach and Fixation Technique
With the patient prepped, draped, and the preoperative plan confirmed, we commence the surgical execution. We utilize the posterior approach, meticulously excising the previous surgical scar to access healthy dermal edges. The deep dissection proceeds through the subcutaneous fat to the fascia lata, which is incised in line with the skin incision. At this juncture, the surgeon encounters the dense fibrotic capsule typical of the inter-stage hip.

TECH FIG 1A • Incising the anterior femoral capsule with electrocautery to allow exposure and mobilization of the proximal femur.
The immediate priority is the identification and protection of the sciatic nerve. With the hip placed in slight internal rotation and extension, we carefully dissect through the scar tissue overlying the short external rotators. If the anatomy is heavily distorted, formal neurolysis is performed, tracing the nerve from the greater sciatic notch distally. Once the nerve is protected, the gluteus maximus tendon is often released from its femoral insertion to facilitate adequate mobilization of the proximal femur. The remnants of the short external rotators and the thick posterior capsule are incised as a single, robust composite flap and tagged with heavy, non-absorbable sutures for later repair.

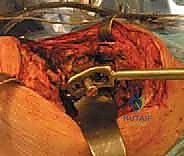
TECH FIG 2A • Exposure of the articulating antibiotic spacer prior to extraction.

TECH FIG 2B • Careful extraction of the femoral spacer, ensuring minimal destruction of the remaining host bone.

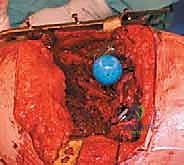
TECH FIG 2C • The acetabular void following the removal of the spacer and initial debridement of the pseudocapsule.
Removal of the antibiotic spacer is the next critical hurdle. If an articulating spacer was utilized, it is dislocated with gentle traction and rotation. The extraction of the femoral and acetabular cement mantles must be performed with extreme caution to preserve the remaining, often fragile, host bone. We utilize specialized cement extraction tools, osteotomes, and occasionally high-speed burrs. If the femoral cement mantle is deeply interdigitated and resists removal, an Extended Trochanteric Osteotomy (ETO) must be strongly considered to prevent catastrophic intraoperative fracturing of the femoral shaft. Once all foreign material is removed, the acetabulum and femoral canal are subjected to a final, rigorous debridement of any residual necrotic tissue or pseudomembrane, followed by copious pulsatile lavage.
TECH FIG 3A • Sequential reaming of the acetabulum to achieve bleeding, viable host bone.

TECH FIG 3B • Assessment of the acetabular defect morphology to determine the need for augments or bone graft.

TECH FIG 3C • Impaction of the highly porous, multi-hole acetabular shell into the prepared bed.

TECH FIG 3D • Placement of supplemental screws in the posterior-superior quadrant to ensure absolute initial stability.
Acetabular reconstruction begins with concentric reaming to expose bleeding, viable subchondral bone. In the setting of severe bone loss (Paprosky Types II and III), we frequently utilize highly porous, trabecular metal multi-hole shells that provide excellent initial friction fit and promote rapid osseointegration. If uncontained defects are present, trabecular metal augments are shaped and secured to the host bone to reconstruct the columns and provide a stable foundation for the hemispherical shell. The shell is impacted into the targeted orientation (typically 40 degrees of abduction and 20 degrees of anteversion), and multiple screws are placed into the posterior-superior safe zone to achieve rigid, absolute mechanical stability.
TECH FIG 4A • Preparation of the femoral canal utilizing sequential flexible reamers to bypass proximal defects.

TECH FIG 4B • Broaching the proximal femur to accommodate the metaphyseal segment of the revision stem.

TECH FIG 4C • Insertion of the trial modular femoral stem, allowing independent adjustment of version and offset.
TECH FIG 4D • Trial reduction of the hip joint to meticulously assess soft tissue tension and stability.

TECH FIG 4E • Assessing stability through a full range of motion, specifically testing for posterior escape in flexion and internal rotation.
Femoral reconstruction is dictated by the quality of the diaphyseal bone. We typically employ a modular, fluted, tapered titanium stem. The diaphysis is progressively reamed until firm cortical chatter is achieved, ensuring axial and rotational stability of the distal segment. The proximal segment is then prepared to restore the appropriate version, offset, and leg length. A trial reduction is performed. The hip is
Clinical & Radiographic Imaging Archive




