Mastering Below-Knee Amputation: An Intraoperative Masterclass for Complex Lower Extremity Tumors
Key Takeaway
This masterclass details below-knee amputation for extensive lower extremity tumors. We cover comprehensive anatomy, meticulous preoperative planning, and granular intraoperative execution, emphasizing precise neurovascular management, optimal flap creation, and robust myodesis. Learn critical pearls, pitfalls, and post-operative rehabilitation strategies to achieve functional outcomes and prevent complications.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater for an exhaustive exploration of a foundational yet highly nuanced orthopedic oncology procedure: the below-knee amputation (BKA). While the modern era of orthopedic oncology heavily emphasizes limb salvage, extirpative surgery remains an indispensable pillar of our armamentarium. This procedure is not merely the removal of a diseased limb; it is a meticulously orchestrated reconstructive effort. The ultimate objective is to achieve wide, negative oncologic margins while simultaneously engineering a highly functional, durable residual limb that seamlessly interfaces with modern prosthetic technology.
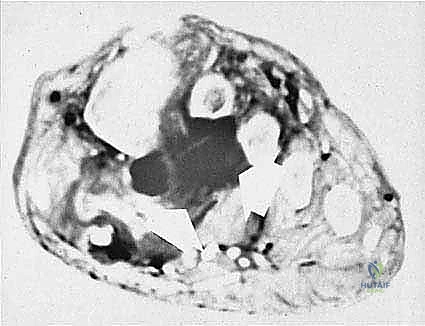
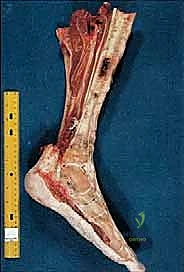
Our index case today involves a patient presenting with an extensive, high-grade sarcoma encompassing the distal leg, ankle, and foot. In such scenarios, the patho-epidemiology of the lesion dictates our surgical strategy. High-grade soft tissue sarcomas and primary bone tumors in the distal extremity often exhibit insidious microscopic extension along fascial planes and neurovascular bundles. When these tumors invade critical structures such as the posterior tibial neurovascular bundle or the plantar aponeurosis, attempts at limb salvage frequently result in a severely compromised, insensate, and painful appendage that is functionally inferior to a well-executed amputation.
The paradigm shift in modern amputation surgery relies heavily on the profound advancements in prosthetic design, including dynamic response feet, osseointegration, and advanced socket interfaces. A meticulously constructed BKA provides this patient with a far superior trajectory for an active, pain-free life compared to a marginal limb salvage fraught with the risks of local recurrence, chronic infection, and non-union. Therefore, we approach this amputation with the same reconstructive zeal and precision as we would a complex free flap or endoprosthetic reconstruction.

Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the lower extremity's compartmental anatomy is the bedrock of a successful oncologic amputation. Precision during dissection is paramount not only for achieving negative margins but also for preserving the delicate vascular supply to the fasciocutaneous flaps and preventing debilitating postoperative neuromas. The leg is rigidly divided into four distinct compartments by unyielding fascial septa: the anterior, lateral, superficial posterior, and deep posterior compartments.
Anterior and Lateral Compartments
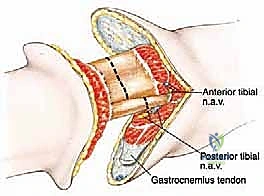
The anterior compartment houses the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius muscles. Deep within this compartment, intimately applied to the interosseous membrane, lies the anterior tibial artery and vein, accompanied by the deep peroneal nerve. These structures must be meticulously identified, individually ligated, and the nerve subjected to traction neurectomy to prevent symptomatic neuroma formation at the anterior distal tibia. The lateral compartment contains the peroneus longus and brevis muscles, along with the superficial peroneal nerve, which typically pierces the deep fascia in the distal third of the leg. This nerve must also be cleanly transected and allowed to retract into the proximal muscle belly.
Superficial and Deep Posterior Compartments
The superficial posterior compartment is the critical workhorse for our soft tissue reconstruction. It contains the gastrocnemius, soleus, and plantaris muscles. The gastrocnemius, with its robust vascular supply from the sural arteries, forms the bulk of the long posterior flap. Our target resection level is typically at the musculocutaneous junction of the gastrocnemius, which provides superior, highly vascularized soft tissue padding over the distal tibial stump. The deep posterior compartment contains the tibialis posterior, flexor digitorum longus, and flexor hallucis longus. Crucially, it houses the posterior tibial and peroneal vessels, along with the tibial nerve. The integrity of the posterior tibial artery is the absolute prerequisite for the viability of the long posterior flap.
Osteology and Biomechanics
The osteology of the tibia and fibula directly influences prosthetic biomechanics. The anterior crest of the tibia is largely subcutaneous; leaving a sharp anterior cortical edge will inevitably lead to skin breakdown and prosthetic intolerance. Therefore, rigorous beveling of the anterior and medial tibial cortices is mandatory. The fibula must be resected approximately 4 to 5 centimeters proximal to the tibial osteotomy. This differential length prevents the fibula from becoming a distal weight-bearing point, creating a conical, tapered stump that facilitates optimal volume containment within a total-contact prosthetic socket.
Exhaustive Indications and Contraindications
The decision to proceed with a major limb amputation is never taken lightly and requires a multidisciplinary consensus involving orthopedic oncology, medical oncology, radiation oncology, and musculoskeletal radiology. The indications for a below-knee amputation in the setting of complex lower extremity tumors are well-defined but require careful patient-specific application.
The primary oncologic indication is a massive, infiltrative malignancy—such as a high-grade soft tissue sarcoma or a primary bone sarcoma (e.g., osteosarcoma, Ewing sarcoma)—where limb-salvage techniques would fail to achieve negative margins without sacrificing critical neurovascular structures, thereby rendering the limb functionally useless. Furthermore, local tumor recurrence, particularly within a previously irradiated field, is a strong indication for amputation due to the high risk of catastrophic wound complications and the unlikelihood of successful secondary salvage.
Contraindications are equally critical to recognize. The most absolute contraindication to a below-knee amputation is tumor extension into the proximal third of the leg or the popliteal fossa, which would compromise the oncologic margins of the posterior flap. In such cases, an above-knee amputation (AKA) or through-knee amputation is mandated. Additionally, severe peripheral vascular disease that precludes adequate perfusion of the long posterior flap is a relative contraindication, potentially necessitating a higher level of amputation to ensure primary wound healing.
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Primary Indications | Massive infiltrative sarcomas of the foot/ankle; Neurovascular bundle encasement; Failed limb salvage. | Limb salvage would result in a non-functional, insensate, or painful extremity. Amputation provides definitive local control. |
| Secondary Indications | Local recurrence in previously irradiated fields; Intractable infection in a tumorous limb; Palliation for fungating masses. | Tissue beds compromised by radiation have abysmal healing rates. Palliative amputation drastically improves quality of life. |
| Absolute Contraindications | Proximal tumor extension into the planned flap territory; Inadequate oncologic margins at the BKA level. | Proceeding would result in intralesional resection and inevitable massive local recurrence. Requires AKA. |
| Relative Contraindications | Severe, uncorrectable peripheral vascular disease; Extensive venous stasis disease or chronic ulceration at the flap site. | High risk of posterior flap necrosis and wound dehiscence. Requires vascular surgery consultation and possible higher amputation. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the blueprint that dictates the success of the extirpation and the viability of the reconstruction. We rely on a comprehensive suite of advanced imaging modalities to precisely map the tumor's three-dimensional volume, assess medullary involvement, and evaluate the patency of the vascular tree. This data directly informs our amputation level and flap geometric design.
Advanced Imaging and Vascular Assessment
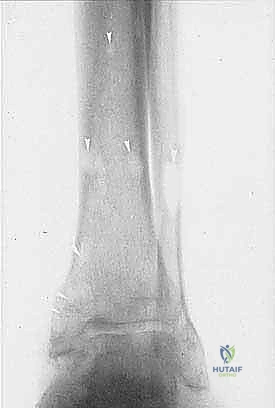
Plain radiography remains the initial step, identifying gross cortical destruction or subtle lytic changes, as seen in our index case of angiosarcomatosis. However, Magnetic Resonance Imaging (MRI) is the undisputed gold standard for soft tissue mapping. T1-weighted and fluid-sensitive MRI sequences allow us to delineate the tumor's relationship to the fascial compartments and, most importantly, the posterior tibial neurovascular bundle. Computed Tomography (CT) is utilized to assess subtle cortical breakthrough and intramedullary skip lesions. If the tumor approaches the mid-shaft, a bone scan or PET-CT is mandatory to rule out proximal osseous metastasis. Finally, CT angiography or conventional angiography is critical if vascular compromise is suspected; confirming robust flow in the posterior tibial artery is non-negotiable for a long posterior flap.
Flap Design and Mathematical Templating
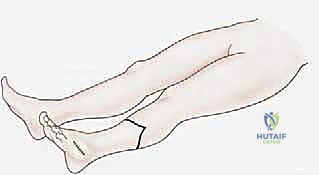
The ideal tibial bone length for a BKA is between 12.5 and 17.5 centimeters from the medial joint line. This length provides a sufficient lever arm for prosthetic control while maintaining adequate soft tissue clearance for modern prosthetic foot components. The geometry of the long posterior flap must be mathematically calculated. The length of the posterior flap must be at least 1.5 times the anteroposterior diameter of the leg at the level of the planned bone transection. This ensures a tension-free closure where the suture line rests anteriorly, away from the distal weight-bearing surface of the stump.
Patient Positioning and Operating Room Setup
The patient is positioned supine on a radiolucent operating table. The operative extremity is meticulously prepped and draped free to allow for full circumferential access and dynamic manipulation during the procedure. A pneumatic tourniquet is placed as proximally as possible on the thigh. Prior to inflation, the limb is elevated for 3 to 5 minutes to exsanguinate the venous system; we strictly avoid using an Esmarch bandage over the tumor to prevent theoretically catastrophic systemic embolization of tumor cells. The C-arm fluoroscopy unit is draped and positioned on standby to verify osteotomy levels if necessary.


Step-by-Step Surgical Approach and Fixation Technique
The execution of the below-knee amputation demands a seamless transition between aggressive oncologic extirpation and delicate plastic reconstruction. We begin with the anterior approach, systematically dissecting through the compartments, managing neurovascular structures, performing the osteotomies, and finally sculpting the posterior myofasciocutaneous flap.
Incision and Anterior Dissection
Using a #10 blade, the skin incision is made exactly as templated, proceeding boldly through the epidermis, dermis, and subcutaneous fat directly to the deep fascia. It is imperative that the scalpel remains strictly perpendicular to the skin to avoid beveling the dermal edges, which can compromise marginal vascularity and lead to delayed wound healing. The anterior transverse incision connects the medial and lateral apices of the planned posterior flap.
We incise the deep fascia of the anterior compartment and use electrocautery to transect the tibialis anterior, extensor digitorum longus, and extensor hallucis longus muscles down to the interosseous membrane. As we retract these muscle bellies, we isolate the anterior tibial artery and vein. These vessels are meticulously skeletonized, clamped, and doubly ligated with heavy silk sutures (e.g., 0 or 2-0 silk). The deep peroneal nerve is identified, gently distracted distally, sharply transected with a fresh blade, and allowed to retract deep into the proximal muscle bed, safely away from the distal stump interface.

Lateral Compartment and Osteotomies
Attention is then turned to the lateral compartment. The peroneus longus and brevis muscles are transected. The superficial peroneal nerve is identified, subjected to traction neurectomy, and allowed to retract. We then prepare for the osteotomies. The periosteum of the tibia is incised circumferentially at the planned resection level (12.5 to 17.5 cm from the joint line). We use an oscillating saw to create a transverse cut through the tibia. Crucially, before completing the transverse cut, we create a 45-degree anterior bevel starting 1.5 to 2 cm proximal to the transverse cut. This eliminates the sharp anterior tibial crest. A rasp is then used to aggressively smooth all cortical edges. The fibula is exposed and transected 4 to 5 cm proximal to the tibial cut using a reciprocating saw or Gigli saw, ensuring it is well-recessed to prevent lateral stump pain.
Posterior Flap Creation and Neurovascular Management
With the bones transected, we place a bone hook in the distal tibial segment and apply anterior traction. This exposes the deep posterior compartment from a proximal-to-distal perspective. We identify and doubly ligate the posterior tibial artery and vein, as well as the peroneal artery and vein. The tibial nerve is a massive structure that requires special attention; it is dissected proximally, ligated to prevent bleeding from the vasa nervorum, sharply transected, and allowed to retract deep into the popliteal fossa.
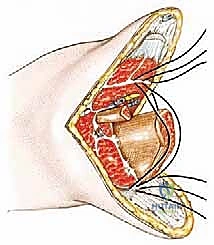
We then complete the creation of the long posterior flap. Using a large amputation knife or heavy electrocautery, we bevel the gastrocnemius and soleus muscles from proximal-deep to distal-superficial, aiming for the musculocutaneous junction at the distal extent of the skin flap. This creates a beautifully tapered, highly vascularized cushion of muscle and skin. The specimen is then passed off the field for formal pathologic and margin analysis.
Myodesis and Layered Closure
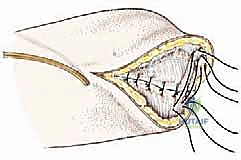
The final stage is the reconstruction of the stump via myodesis. Unlike a simple myoplasty (sewing muscle to muscle), a myodesis anchors the posterior muscle complex directly to the bone, preventing distal soft tissue redundancy and providing a stable, dynamic envelope for the prosthesis. We drill several small holes into the anterior and lateral cortices of the distal tibia. Heavy non-absorbable sutures (e.g., #1 or #2 FiberWire or Ethibond) are passed through the robust fascia of the gastrocnemius flap and securely tied through the tibial drill holes, bringing the posterior flap anteriorly over the bone end.

Once the myodesis is secure, we place a closed-suction drain deep to the muscle layer, exiting laterally. The deep fascial layers are meticulously reapproximated with interrupted absorbable sutures to eliminate dead space. The subcutaneous tissue is closed with 2-0 or 3-0 absorbable sutures, and the skin is expertly approximated using either non-absorbable nylon sutures or surgical staples, ensuring absolutely no tension on the anterior suture line.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, below-knee amputations, particularly in the oncologic setting where patients may have undergone neoadjuvant chemotherapy or radiation, carry a significant risk of complications. Recognizing these early and intervening aggressively is paramount to salvaging the residual limb and maintaining the patient's functional trajectory.
Wound dehiscence and flap necrosis are the most dreaded early complications. These typically result from unrecognized vascular insufficiency, excessive tension on the anterior suture line, or traumatic handling of the skin edges. If superficial epidermolysis occurs, conservative management with advanced wound care may suffice. However, full-thickness necrosis requires urgent return to the operating room for surgical debridement and potentially a wedge resection or revision to a higher amputation level.
Symptomatic neuromas and phantom limb pain are complex, interrelated neuro-centric complications. While phantom sensation is nearly universal, debilitating phantom limb pain occurs in a smaller subset of patients and requires a multidisciplinary pain management approach, including gabapentinoids, tricyclic antidepressants, and targeted nerve blocks. A symptomatic neuroma typically presents as a localized, exquisitely tender nodule with a positive Tinel's sign at the stump surface. This is usually the result of inadequate proximal traction neurectomy during the index procedure. Management begins with targeted steroid injections, but refractory cases necessitate surgical excision of the neuroma and deeper proximal burying of the nerve stump into a healthy muscle belly or bone.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Wound Dehiscence / Flap Necrosis | 10% - 15% | Vascular insufficiency, excessive tension, smoking, poor nutrition, prior radiation. | Aggressive debridement, negative pressure wound therapy (NPWT), potential revision to AKA if extensive. |
| Symptomatic Neuroma | 5% - 10% | Inadequate proximal retraction of transected nerves (especially tibial or deep peroneal). | Ultrasound-guided injections; surgical excision and targeted muscle reinnervation (TMR) or deep burying. |
| Deep Infection | 3% - 8% | Hematoma formation, immunocompromise (chemotherapy), prolonged operative time. | Emergent I&D, deep tissue cultures, prolonged targeted intravenous antibiotic therapy. |
| Joint Contracture (Knee Flexion) | 15% - 20% | Inadequate postoperative splinting, prolonged wheelchair use, poor physical therapy compliance. | Aggressive physical therapy, serial casting, dynamic splinting; rarely requires surgical release. |
Phased Post-Operative Rehabilitation Protocols
The surgical closure of the skin marks only the beginning of the patient's rehabilitative journey. A highly structured, phased postoperative protocol is essential for shaping the residual limb, preventing contractures, and ensuring a successful transition to independent prosthetic ambulation.
Phase 1: Immediate Post-Operative Management and Healing (Weeks 0-3)
Immediately following wound closure, a rigid or semi-rigid dressing is applied in the operating room. An Immediate Post-Operative Rigid Dressing (IPORD) is highly favored as it controls edema, protects the vulnerable surgical site from trauma, and crucially, maintains the knee in full extension to prevent flexion contractures. The primary goals during this phase are pain control, wound healing, and early mobilization out of bed. The closed-suction drain is typically removed within 48 to 72 hours when output significantly diminishes.
Phase 2: Pre-Prosthetic Training and Stump Shaping (Weeks 3-8)
Once the surgical wound demonstrates robust healing and the sutures or staples are removed (usually around 21 days), the focus shifts to aggressive stump shaping and desensitization. The patient is transitioned to a compressive shrinker sock, which must be worn continuously to promote a conical stump shape and reduce interstitial edema. Physical therapy intensifies, focusing on strengthening the quadriceps, hip extensors, and core musculature. Maintaining full knee extension remains a critical priority, as even a mild flexion contracture exponentially increases the energy expenditure required for prosthetic ambulation.
Phase 3: Prosthetic Fitting and Gait Training (Weeks 8+)
When the residual limb volume stabilizes and the soft tissue envelope is mature, the patient is referred to the prosthetist for casting and fabrication of a preparatory (temporary) prosthesis. This phase involves intensive gait training within parallel bars, progressing to a walker, and eventually to independent ambulation with a cane or no assistive device. The socket fit will require frequent adjustments as the stump continues to atrophy and remodel over the first year. The ultimate goal is the delivery of a definitive, custom-designed prosthesis tailored to the patient's specific activity level and functional demands.
Summary of Landmark Literature and Clinical Guidelines
The modern approach to oncologic lower extremity amputation is heavily informed by landmark clinical trials and established oncologic guidelines. The National Comprehensive Cancer Network (NCCN) guidelines for Soft Tissue Sarcoma dictate that surgical resection must achieve negative margins (R0 resection). In cases where amputation is required to achieve this, the guidelines emphasize that the functional outcome of a well-planned amputation often supersedes the morbidity of a compromised limb salvage.
Furthermore, while originally designed for severe lower extremity trauma, the findings of the Lower Extremity Assessment Project (LEAP) study are highly relevant to our oncologic population. The LEAP study definitively demonstrated that when comparing successful limb salvage to major amputation in severe lower extremity trauma, there was no significant difference in functional outcomes or quality of life at two and seven years post-injury. This data provides robust evidence to support our clinical decision-making when counseling patients with massive extremity tumors: a meticulously executed below-knee amputation, paired with advanced prosthetic rehabilitation, is not a failure of treatment, but rather a highly effective, definitive reconstructive procedure that restores mobility and preserves life.
