Masterclass: Unit Rod Instrumentation for Neuromuscular Scoliosis Correction

Key Takeaway
Join this masterclass on unit rod instrumentation for neuromuscular scoliosis. We'll meticulously cover patient selection, preoperative planning, and precise intraoperative execution from incision to closure. Learn critical anatomical considerations, advanced surgical techniques, and strategies for managing potential complications. This guide provides an exhaustive, real-time walkthrough for fellows, emphasizing optimal outcomes in complex spinal deformity correction.
Comprehensive Introduction and Patho-Epidemiology
Neuromuscular scoliosis represents one of the most formidable challenges in pediatric orthopedic surgery. Unlike idiopathic scoliosis, which often presents in otherwise healthy adolescents and primarily affects the coronal plane, neuromuscular spinal deformity is a complex, three-dimensional disease process inextricably linked to profound systemic comorbidities. The primary objective of surgical intervention in this population is rarely cosmetic; rather, it is a functional salvage operation designed to restore sitting balance, halt the relentless decline of pulmonary mechanics, alleviate pain, and significantly ease the burden of care for the patient's family and nursing staff. The unit rod instrumentation system, utilizing a pre-contoured, continuous U-shaped rod combined with segmental sublaminar wire fixation, has long stood as a highly reliable, biomechanically sound, and cost-effective workhorse for achieving these goals.
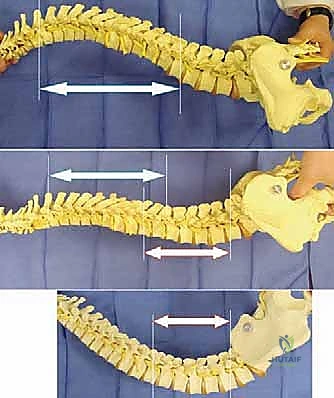
The pathogenesis of neuromuscular scoliosis is deeply rooted in the underlying neurologic or myopathic disorder, which invariably disrupts the delicate equilibrium of paraspinal musculature and postural reflexes. The prevalence of spinal deformity in non-ambulatory neuromuscular patients approaches an astonishing 100%. In conditions such as Cerebral Palsy (CP)—the most ubiquitous etiology of neuromuscular scoliosis—the deformity arises from a static encephalopathy that produces dynamic spasticity, asymmetric muscle tone, and truncal hypotonia. These curves are characteristically long, sweeping, C-shaped thoracolumbar deformities that invariably encompass the pelvis, leading to severe pelvic obliquity. This obliquity creates a "windswept" posture, rendering independent sitting impossible and predisposing the patient to intractable ischial decubitus ulcers.

Conversely, myopathic conditions such as Duchenne Muscular Dystrophy (DMD) and Spinal Muscular Atrophy (SMA) present a different pathophysiological cascade. In DMD, an X-linked recessive absence of dystrophin leads to relentless, progressive myofiber degeneration. Once these patients lose ambulatory capacity, typically in early adolescence, the spine rapidly collapses under the forces of gravity. The progression of the scoliotic curve in DMD exhibits a direct, deleterious correlation with the decline in Forced Vital Capacity (FVC). Without surgical stabilization, these patients succumb to cor pulmonale or restrictive pulmonary failure. Similarly, myelomeningocele presents unique patho-anatomical hurdles, including absent posterior elements (spina bifida), tethered cord syndrome, and hydrocephalus, all of which complicate both the natural history and the surgical approach to the scoliotic curve.
The natural history of untreated neuromuscular scoliosis is universally grim. Unlike idiopathic curves, which often stabilize upon skeletal maturity, neuromuscular curves continue to progress relentlessly throughout adulthood, often at rates exceeding 2 to 4 degrees per year. Conservative modalities, including custom-molded thoracolumbosacral orthoses (TLSO) and complex wheelchair seating modifications, are purely palliative. They may assist in temporary postural support for the growing child but possess absolutely no efficacy in halting curve progression. Therefore, definitive posterior spinal fusion and instrumentation remains the gold standard, ideally executed before the deformity becomes rigid and before the patient's cardiopulmonary reserves are irreversibly depleted.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the posterior spinal and pelvic anatomy is the absolute prerequisite for safe execution of unit rod instrumentation. The surgical corridor necessitates a massive, contiguous exposure from the upper thoracic spine (typically T2 or T3) down to the sacrum and bilateral ilia. The muscular envelope, comprising the trapezius, latissimus dorsi, and the deep erector spinae group (iliocostalis, longissimus, spinalis), must be meticulously elevated subperiosteally. In neuromuscular patients, this musculature is often heavily atrophied, fibrotic, or replaced by adipose tissue, altering normal surgical planes and increasing the risk of inadvertent penetration into the epidural space during dissection.
The osteology of the neuromuscular spine presents significant fixation challenges. Disuse osteopenia, combined with the effects of anti-epileptic medications and poor nutritional status, renders the vertebral bodies and posterior elements structurally compromised. The unit rod technique elegantly circumvents the limitations of poor cancellous bone density (which plagues pedicle screw fixation in this population) by utilizing the cortical bone of the laminae. The sublaminar space, bounded anteriorly by the dura mater and posteriorly by the ligamentum flavum and lamina, is the critical anatomic zone for this procedure. The surgeon must navigate this space with extreme precision, utilizing doubled 16-gauge or 18-gauge wires. The epidural venous plexus is often engorged, particularly in the prone position, and careless wire passage can result in catastrophic epidural hemorrhage or direct contusion to the spinal cord.

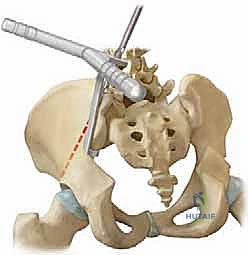
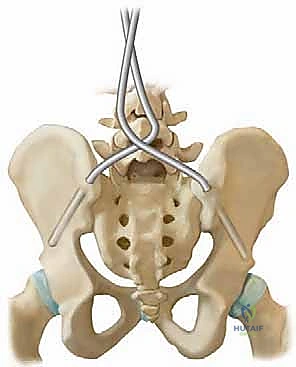
Distal fixation is arguably the most critical component of the construct, as failure to adequately control the pelvis will result in recurrent obliquity and sitting imbalance. The Galveston technique, or modern variations utilizing intra-iliac posts or screws, relies on the robust cortical bone between the inner and outer tables of the ilium. The optimal trajectory begins at the posterior superior iliac spine (PSIS) and advances anteriorly and distally, passing just superior to the greater sciatic notch. This trajectory maximizes bone purchase while avoiding the sciatic nerve and the superior gluteal neurovascular bundle. The surgeon must possess a pristine three-dimensional understanding of the pelvic anatomy, as the ilium in neuromuscular patients is often dysplastic, narrow, and severely rotated.
Biomechanically, the unit rod construct is a masterpiece of load-sharing and stress distribution. By utilizing a single, continuous, pre-contoured rigid rod (typically 1/4 inch or 3/16 inch stainless steel) and securing it at every available segmental level with sublaminar wires, the construct dissipates corrective forces across the entire length of the spine. This minimizes the stress concentrated at any single bone-implant interface, drastically reducing the risk of implant pullout in osteopenic bone. The primary corrective maneuver is a powerful cantilever force. The distal limbs of the unit rod are first docked into the ilium. The proximal U-shaped portion, which initially stands proud of the kyphoscoliotic thoracic spine, is then gradually leveraged down to the midline. This maneuver translates the spine to the rod, simultaneously correcting the coronal deformity, restoring sagittal contours, and forcefully leveling the pelvis.
Exhaustive Indications and Contraindications
The decision to proceed with major spinal reconstruction in a fragile neuromuscular patient requires a delicate calculus, balancing the inevitable progression of the deformity against the formidable physiological insult of the surgery. Patient selection must be rigorous, multi-disciplinary, and focused entirely on functional outcomes and quality of life.
| Parameter | Indications for Surgical Intervention | Absolute & Relative Contraindications |
|---|---|---|
| Curve Magnitude | Coronal Cobb angle > 50° in a growing child; > 40° with documented rapid progression. | Stable, non-progressive curves < 40° in a mature patient (Relative). |
| Pelvic Obliquity | > 15° leading to seating intolerance, loss of sitting balance, or impending ischial decubitus ulcers. | Absence of pelvic obliquity in a patient with a balanced spine (pelvic fixation may be omitted). |
| Pulmonary Function | FVC declining but still > 30-35% predicted (ideal window for intervention). | FVC < 20% predicted, severe pulmonary arterial hypertension, ventilator dependence without tracheostomy (Absolute). |
| Nutritional Status | Optimized albumin (>3.5 g/dL) and total lymphocyte count; gastrostomy tube functional if needed. | Severe, uncorrected malnutrition (Albumin < 3.0 g/dL); active systemic infection (Absolute). |
| Sagittal Profile | Severe hyperkyphosis causing skin breakdown over spinous processes; hyperlordosis preventing seating. | Medically unstable patient unable to tolerate prone positioning or prolonged anesthesia (Absolute). |
The timing of surgery is paramount. Intervening too early in a very young child risks the "crankshaft phenomenon" unless anterior fusion is also performed, while intervening too late invites insurmountable cardiopulmonary complications and rigid deformities that require highly morbid osteotomies. In DMD, the window of opportunity is notoriously narrow; surgery is universally recommended shortly after the cessation of ambulation, prior to the inevitable precipitous drop in vital capacity.
Contraindications are primarily medical rather than anatomical. A patient with profound, uncorrectable malnutrition will experience catastrophic wound dehiscence and deep surgical site infections. Similarly, patients with severe, irreversible cardiac dysfunction (e.g., advanced dystrophic cardiomyopathy) or pulmonary failure may not survive the hemodynamic shifts associated with blood loss and prone positioning. In such cases, the surgeon must have the wisdom to decline operative intervention, focusing instead on palliative seating and comfort care.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock upon which a successful neuromuscular spinal fusion is built. The preparation begins weeks, if not months, prior to the operative date, involving a coordinated effort between orthopedic surgery, pediatric pulmonology, cardiology, neurology, and anesthesiology.
Radiographic evaluation must be exhaustive. Standard full-length standing or sitting anteroposterior (AP) and lateral radiographs are obtained to measure the primary Cobb angles, regional kyphosis/lordosis, and the degree of pelvic obliquity. However, the most critical imaging for surgical decision-making is the supine traction or side-bending radiograph. These dynamic films dictate the flexibility of the curve. If the curve remains rigid (correcting less than 30-40%) or if the pelvic obliquity cannot be leveled passively, the surgeon must plan for extensive posterior column osteotomies (Ponte osteotomies) or, in severe cases, a staged anterior release.

Advanced imaging is frequently indicated. An MRI of the entire neuraxis is mandatory in patients with congenital deformities (e.g., myelomeningocele) or in those exhibiting atypical neurologic symptoms, to rule out tethered cord, syringomyelia, or Chiari malformations. A preoperative CT scan can be invaluable for mapping dysplastic pelvic anatomy, allowing the surgeon to measure the precise width and trajectory of the iliac teardrop for Galveston post insertion. Furthermore, a DEXA scan is highly recommended to quantify bone mineral density, which will directly influence the choice of fixation and the aggressiveness of the intraoperative correction maneuvers.

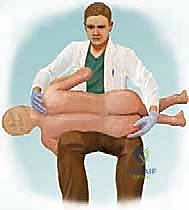
In the operating theater, patient positioning is a meticulous, time-consuming process that demands the surgeon's direct supervision. The patient is typically placed prone on a specialized four-poster frame or a Jackson spinal table. The primary goal is to allow the abdomen to hang completely free. Any abdominal compression will translate to increased intra-abdominal pressure, engorgement of the epidural venous plexus (Batson's plexus), and subsequent torrential intraoperative bleeding. Meticulous padding of all bony prominences, particularly the face, axillae, and peroneal nerves, is non-negotiable to prevent devastating positioning palsies.
Neuromonitoring, utilizing Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), is standard of care. However, the surgeon must recognize that baseline signals in severe CP or myelomeningocele patients are often degraded or entirely absent. A robust blood conservation strategy must be implemented prior to incision, including the prophylactic administration of Tranexamic Acid (TXA), utilization of intraoperative cell salvage, and ensuring the immediate availability of type-specific cross-matched packed red blood cells and fresh frozen plasma.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a unit rod instrumentation is a marathon requiring stamina, anatomical precision, and a methodical cadence. The procedure can be conceptually divided into exposure, preparation of fixation points, rod contouring, cantilever reduction, and arthrodesis.
1. Exposure and Soft Tissue Dissection
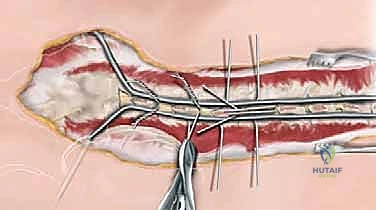
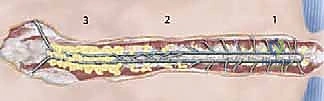
Following meticulous skin preparation and draping, a perfectly straight midline incision is made from the spinous process of T2 down to the sacrum, extending slightly laterally toward the posterior superior iliac spines (PSIS). Subperiosteal dissection is carried out utilizing Cobb elevators and electrocautery. The dissection must be strictly subperiosteal to minimize blood loss, sweeping the paraspinal musculature laterally to expose the tips of the transverse processes in the thoracic spine and the facet joints in the lumbar spine.

In the lumbar region, the dissection is carried over the sacral ala and the PSIS to prepare for pelvic fixation. Meticulous hemostasis is maintained throughout; packing the gutters with laparotomy sponges soaked in warm saline helps control venous oozing. Once the spine is fully exposed, complete facetectomies are performed at every level to be fused. This not only provides a massive surface area for bone grafting but also significantly increases the flexibility of the spine, facilitating the subsequent correction.
2. Preparation of the Pelvic Foundation (Galveston Technique)
The foundation of the unit rod construct lies in the pelvis. The PSIS is identified, and a starting hole is created using a burr or awl. The trajectory is critical: the drill must pass between the inner and outer tables of the ilium, directed roughly 15 degrees laterally and 15 degrees caudally, aiming just superior to the sciatic notch.

A blunt probe is utilized to palpate the trajectory, ensuring there is no cortical breach into the sciatic notch or the true pelvis. Once the trajectory is confirmed, the pathway is sequentially enlarged to accommodate the distal limbs of the unit rod.
3. Sublaminar Wire Passage
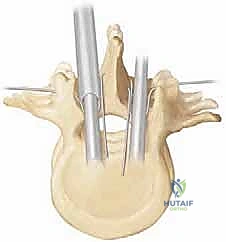
This is the most perilous phase of the procedure. The ligamentum flavum is meticulously excised at the midline using Kerrison rongeurs to expose the epidural space. Doubled 16-gauge or 18-gauge stainless steel wires, pre-bent into a smooth, semi-circular loop, are carefully passed under each lamina.
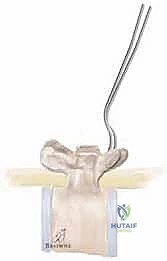
The technique requires a delicate "flossing" motion. The tip of the wire must be kept in direct contact with the undersurface of the lamina at all times to avoid plunging into the spinal cord.

Once the loop emerges from the cephalad edge of the lamina, it is grasped with a nerve hook and pulled through. The wires are then sharply bent over the posterior elements to prevent them from slipping back into the canal and compressing the cord.

4. Unit Rod Contouring and Insertion
The unit rod must be custom-contoured to match the patient's ideal sagittal profile, incorporating appropriate thoracic kyphosis and lumbar lordosis. The distal limbs are bent to perfectly match the trajectory of the intra-iliac pathways prepared earlier.

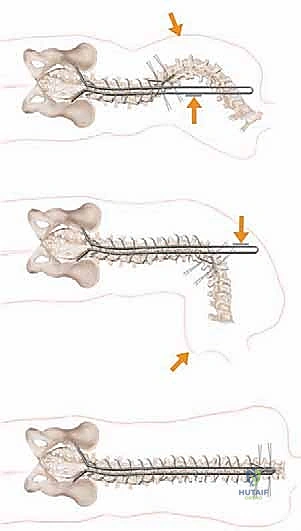
The correct width of the U-rod is selected to sit comfortably across the laminae. The rod is then introduced to the sterile field. The distal limbs are simultaneously impacted into the bilateral iliac holes. At this stage, the proximal U-portion of the rod will be standing high above the thoracic spine due to the uncorrected deformity.
5. The Cantilever Reduction Maneuver
With the pelvis securely docked, the cantilever reduction begins. The surgeon forcefully pushes the proximal U-portion of the rod down toward the thoracic spine. This maneuver requires significant physical force and utilizes the rod as a massive lever arm.
As the rod is brought down to the spine, it translates the apical vertebrae toward the midline, correcting the scoliosis, while simultaneously forcing the elevated hemi-pelvis down, correcting the pelvic obliquity.
Once the rod is approximated to the spine, the sublaminar wires are sequentially tightened around the rod.
Tightening begins at the apex of the curve to draw the spine to the rod, and then proceeds proximally and distally. The wires must be tensioned symmetrically to avoid asymmetric pull-out.
The wire ends are cut short and meticulously bent over the rod to prevent soft tissue irritation.

6. Decortication, Bone Grafting, and Closure
A robust arthrodesis is the ultimate goal; the hardware is merely an internal splint until biological fusion occurs. The remaining exposed posterior elements (laminae, transverse processes) are aggressively decorticated using a high-speed burr or gouges until bleeding cancellous bone is exposed.

Copious amounts of bone graft—typically a mixture of local autograft harvested from the spinous processes and facet joints, combined with massive volumes of allograft (cancellous chips and demineralized bone matrix)—are packed meticulously into the decorticated gutters.

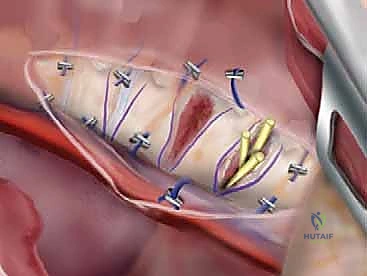
Closure is performed over deep subfascial drains. The paraspinal musculature and lumbodorsal fascia are closed in multiple watertight layers using heavy, absorbable sutures.

Given the poor soft tissue envelope in many neuromuscular patients, a meticulous, tension-free closure is vital to prevent postoperative wound dehiscence and deep infection.

Complications, Incidence Rates, and Salvage Management
Surgical intervention for neuromuscular scoliosis carries one of the highest complication profiles in all of orthopedic surgery. The systemic fragility of these patients amplifies the risks associated with major blood loss, prolonged anesthesia, and massive implantation of foreign material. The surgeon must be intimately familiar with potential pitfalls and possess clear algorithms for salvage management.
| Complication | Estimated Incidence | Etiology & Salvage Management Strategy |
|---|---|---|
| Massive Hemorrhage | 20 - 40% | Etiology: Extensive muscle dissection, epidural venous bleeding, poor vascular tone. Salvage: Pre-op TXA, cell saver, rapid transfusion protocols, meticulous bipolar cautery, packing gutters. |
| Surgical Site Infection (SSI) | 5 - 15% | Etiology: Poor nutrition, incontinence, thin soft tissue envelope, prolonged OR time. Salvage: Aggressive I&D, vacuum-assisted closure (VAC), targeted IV antibiotics, hardware retention if stable, nutritional optimization (TPN/Enteral). |
| Neurologic Deficit | 1 - 3% | Etiology: Direct cord trauma during wire passage, epidural hematoma, ischemic injury from over-correction. Salvage: Immediate release of correction, removal of offending wires, high-dose steroids (controversial), emergent MRI if post-op deficit noted. |
| Hardware Failure / Pullout | 5 - 10% | Etiology: Osteopenic bone, inadequate fixation points, pseudoarthrosis, uncontrolled spasticity. Salvage: Revision surgery, extension of fusion, addition of pedicle screws or pelvic screws, massive structural allografting. |
| Pseudoarthrosis | 5 - 15% | Etiology: Inadequate decortication, insufficient bone graft, malnutrition, infection. Salvage: Revision posterior fusion, exploration of the fusion mass, re-grafting with BMP (Bone Morphogenetic Protein), optimization of host biology. |
Pulmonary complications, including pneumonia, atelectasis, and prolonged ventilator dependence, are ubiquitous in the immediate postoperative period. The incidence of deep SSI is notably higher than in idiopathic scoliosis, largely driven by fecal and urinary incontinence contaminating the distal aspect of the incision, combined
