Lateral Decubitus Hip Arthroscopy: Comprehensive Surgical Technique and Portal Anatomy
Key Takeaway
The lateral decubitus position for hip arthroscopy offers distinct advantages, particularly in obese patients and those with large anterolateral osteophytes. By utilizing gravity to retract adipose tissue and optimizing the traction vector, surgeons can achieve excellent joint distraction. This guide details the precise biomechanics, anatomical landmarks, and step-by-step portal placement required to safely execute lateral position hip arthroscopy while minimizing neurovascular complications and optimizing intra-articular visualization.
Comprehensive Introduction and Patho-Epidemiology
Hip arthroscopy has revolutionized the management of non-arthritic hip pain, evolving over the past three decades from a diagnostic novelty into a highly efficacious, minimally invasive intervention for complex intra-articular and extra-articular pathology. Historically, access to the central and peripheral compartments of the hip joint required a highly morbid surgical dislocation, as popularized by Ganz. While open surgical dislocation remains the gold standard for specific extensive deformities, arthroscopic techniques have largely supplanted open procedures for the management of femoroacetabular impingement (FAI), labral tears, chondral defects, and ligamentum teres pathology. The transition to arthroscopic management has significantly reduced postoperative morbidity, accelerated rehabilitation timelines, and minimized the risk of avascular necrosis of the femoral head by preserving the medial circumflex femoral artery and its retinacular branches.
The epidemiological landscape of hip pathology has become increasingly defined as diagnostic imaging modalities, particularly high-resolution magnetic resonance arthrography (MRA) and 3D computed tomography (CT), have advanced. Femoroacetabular impingement is now recognized as a primary etiological factor in the development of early-onset osteoarthritis in the young, active population. Cam morphology, characterized by an aspherical femoral head-neck junction and a reduced anterior offset, is highly prevalent in athletic populations, particularly those involved in high-impact, multidirectional sports during skeletal immaturity. Pincer morphology, defined by focal or global acetabular overcoverage (e.g., coxa profunda, acetabular retroversion), leads to linear contact between the acetabular rim and the femoral neck. Both pathomechanical entities ultimately result in shear forces at the chondrolabral junction, precipitating labral tears, chondral delamination, and progressive joint degeneration.
While the supine position for hip arthroscopy, popularized by Byrd, is widely utilized, the lateral decubitus position offers profound anatomical and biomechanical advantages that are increasingly recognized by high-volume joint preservation surgeons. Pioneered in the late 1980s and early 1990s by Dr. J.M. Glick, the lateral approach is particularly intuitive for reconstructive surgeons accustomed to performing total hip arthroplasty (THA) or trauma surgery in the lateral decubitus position. The spatial orientation of the acetabulum and proximal femur in the lateral position is highly familiar, reducing the cognitive load required to navigate the complex three-dimensional anatomy of the hip joint.
Furthermore, the lateral position leverages gravity to displace redundant adipose tissue and muscular bulk away from the surgical field. In the supine position, the pannus and anterior thigh soft tissues fall directly over the anterior portals, increasing the depth to the joint and exacerbating instrument friction. Conversely, in the lateral decubitus position, these tissues fall anteriorly and medially, significantly reducing the soft-tissue distance to the joint capsule. This gravitational advantage makes the lateral position exceptionally beneficial in obese and morbidly obese patients, facilitating easier portal establishment, superior instrument maneuverability, and a drastically reduced risk of fluid extravasation into the abdominal cavity.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the complex osseous, capsuloligamentous, and neurovascular anatomy of the hip is paramount for safe and effective lateral decubitus hip arthroscopy. The hip is a highly constrained, multiaxial ball-and-socket (enarthrodial) joint designed for both extreme stability and a wide functional range of motion. The osseous anatomy comprises the hemispherical acetabulum, which is oriented with approximately 15 to 20 degrees of anteversion and 40 to 45 degrees of inclination, and the femoral head, which typically exhibits 10 to 15 degrees of anteversion. The "safe zone" for arthroscopic portal placement is generally defined by the anterior and lateral aspects of the joint, bounded by the neurovascular bundle medially and the sciatic nerve posteriorly.
The stability of the hip joint is heavily reliant on its robust capsuloligamentous complex, which must be systematically managed during arthroscopy. The capsule is reinforced by three primary extracapsular ligaments: the iliofemoral, pubofemoral, and ischiofemoral ligaments. The iliofemoral ligament, or the Y ligament of Bigelow, is the strongest ligament in the human body, originating from the anterior inferior iliac spine (AIIS) and inserting along the intertrochanteric line. It forms the thick anterior capsule and is the primary restraint to hip extension and external rotation. The pubofemoral ligament reinforces the inferior capsule, while the ischiofemoral ligament reinforces the posterior capsule. Deep to these structures lies the zona orbicularis, a circumferential collar of capsular fibers that encircles the femoral neck and acts as a crucial secondary stabilizer against joint distraction.
Neurovascular considerations dictate the precise placement of all arthroscopic portals. The lateral femoral cutaneous nerve (LFCN), a sensory branch from the lumbar plexus (L2-L3), is at the highest risk of iatrogenic injury during the establishment of the direct anterior portal. The LFCN exhibits significant anatomical variability, frequently branching into multiple fascicles as it courses distal to the inguinal ligament over the sartorius muscle. The femoral artery, vein, and nerve lie in the anterior groin, well medial to the standard arthroscopic safe zone, but their proximity mandates strict adherence to anatomical landmarks. Posteriorly, the sciatic nerve exits the greater sciatic foramen and courses deep to the gluteus maximus; it is at risk during the establishment of the posterior peritrochanteric portal, particularly if the portal trajectory is directed too far posteriorly or if the hip is externally rotated.
The biomechanics of joint distraction are central to the success of the procedure. The hip joint is stabilized not only by its osseous architecture and ligamentous restraints but also by a highly effective negative intra-articular pressure, commonly referred to as the "vacuum seal." Successful central compartment arthroscopy requires overcoming these formidable forces to achieve a minimum of 8 to 10 millimeters of joint distraction. This space is mandatory to allow the safe introduction of a 5-millimeter arthroscope and working instruments without causing iatrogenic scuffing of the delicate articular cartilage or avulsion of the acetabular labrum. If excessive traction force is applied without neutralizing the vacuum seal, the surgeon risks catastrophic neuropraxia to the pudendal or sciatic nerves. Therefore, the physiological vacuum must be broken via the intra-articular introduction of air or fluid before definitive traction is applied.
Exhaustive Indications and Contraindications
The decision to proceed with lateral decubitus hip arthroscopy involves a meticulous evaluation of the patient's clinical presentation, advanced imaging findings, and individual morphotype. The primary indication for hip arthroscopy is symptomatic femoroacetabular impingement (cam, pincer, or mixed morphology) that has failed exhaustive conservative management, including targeted physical therapy, activity modification, and intra-articular corticosteroid injections. Associated intra-articular pathologies, such as symptomatic acetabular labral tears, focal full-thickness chondral defects, and ligamentum teres avulsions or hypertrophy, are also prime indications for arthroscopic intervention.
The lateral decubitus position is particularly favored over the supine position in specific clinical scenarios based on patient morphology and the location of the primary pathology. Patients with a high Body Mass Index (BMI > 30) represent a distinct indication for the lateral approach. In these individuals, the gravitational displacement of the pannus and subcutaneous adipose tissue away from the lateral trochanteric region drastically reduces the soft-tissue depth. This minimizes the "fulcrum effect" on arthroscopic instruments, allowing for greater angular maneuverability and reducing the requisite length of the cannulas. Furthermore, patients presenting with massive anterolateral osseous deformities, such as giant cam lesions or prominent anterior inferior iliac spine (AIIS) subspine impingement, benefit from the lateral position, which allows the surgeon to establish primary access via the posterior peritrochanteric portal, effectively bypassing the anterior osseous obstruction.
Despite its versatility, hip arthroscopy is not universally applicable, and strict adherence to contraindications is necessary to prevent disastrous clinical outcomes. Absolute contraindications include active local or systemic infection, severe advanced osteoarthritis (Tönnis grade 3 or joint space less than 2 mm), and bony ankylosis of the joint. Attempting arthroscopy in the setting of advanced degenerative joint disease is universally associated with poor outcomes and rapid progression to total hip arthroplasty. Relative contraindications require careful preoperative deliberation and include severe developmental dysplasia of the hip (DDH) with a lateral center-edge angle (LCEA) of less than 20 degrees. In dysplastic patients, the labrum is often hypertrophic and serves as a primary structural stabilizer; resecting or altering this labrum without addressing the underlying osseous undercoverage can precipitate catastrophic iatrogenic macroinstability.
Other relative contraindications include profound protrusio acetabuli, which restricts joint distraction and limits instrument maneuverability due to the deep seating of the femoral head. Morbid obesity (BMI > 40) can also be considered a relative contraindication if the patient's body habitus exceeds the mechanical limits of the distraction table or the physical length of available arthroscopic instrumentation, although the lateral position mitigates this risk significantly compared to the supine approach.
| Category | Indications | Contraindications (Absolute & Relative) |
|---|---|---|
| Primary Pathology | Symptomatic FAI (Cam, Pincer, Mixed) | Active intra-articular or peri-articular infection |
| Soft Tissue Lesions | Acetabular labral tears, Ligamentum teres tears | Advanced Osteoarthritis (Tönnis Grade 3, < 2mm joint space) |
| Chondral/Synovial | Focal chondral defects, Synovial chondromatosis | Bony ankylosis or severe arthrofibrosis |
| Morphotype Advantage | High BMI / Obesity (Gravitational tissue displacement) | Severe Dysplasia (LCEA < 20°) without concomitant PAO |
| Osseous Deformities | Massive anterolateral cam lesions, AIIS impingement | Profound Coxa Profunda / Protrusio Acetabuli |
| Extra-articular | Greater trochanteric pain syndrome, Gluteus medius tears | Morbid obesity exceeding table mechanical limits |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive preoperative planning is the cornerstone of successful hip arthroscopy. This begins with a rigorous radiographic evaluation, including a standardized weight-bearing anteroposterior (AP) radiograph of the pelvis, a Dunn 45-degree lateral view, and a false profile view. These plain films are utilized to assess global acetabular version, measure the lateral center-edge angle (LCEA) and Tönnis angle, and identify the crossover sign indicative of cranial acetabular retroversion. The Dunn view is particularly critical for evaluating the sphericity of the femoral head-neck junction and calculating the alpha angle. Advanced cross-sectional imaging, specifically high-resolution Magnetic Resonance Arthrography (MRA) or a non-contrast 3-Tesla MRI, is mandatory for evaluating the integrity of the labrum, the articular cartilage, and the ligamentum teres. Three-dimensional CT reconstructions are increasingly utilized for precise preoperative templating of osseous resections in complex FAI cases.
Anesthetic management is a critical component of the preoperative setup. General anesthesia with profound neuromuscular blockade is universally recommended. Complete muscle relaxation is imperative to paralyze the robust pelvic and thigh musculature, thereby minimizing the mechanical traction forces required to distract the joint. This directly reduces the risk of traction-related neuropraxia. Additionally, hypotensive anesthesia (maintaining mean arterial pressure between 60 and 70 mmHg) is frequently employed to minimize intra-articular bleeding, which can severely compromise arthroscopic visualization due to the limited volume of the hip joint.
Patient positioning in the lateral decubitus orientation is arguably the most critical and unforgiving step of the entire procedure. Improper setup not only compromises surgical access but drastically increases the risk of devastating neurovascular complications. Following induction, the patient is carefully rolled into the lateral decubitus position on a specialized fracture table or a dedicated hip distraction apparatus. The operative hip faces superiorly. A well-padded, oversized perineal post is installed between the patient's legs. It is an absolute critical requirement that this post is positioned as far laterally as possible against the medial thigh of the operative leg, rather than resting directly in the perineal crease. This strategic lateralization directs the immense counter-traction vector against the robust musculature of the medial thigh, effectively protecting the delicate pudendal nerve and perineal soft tissues from ischemic crush injury.
The kinematics of the leg positioning dictate the ease of joint distraction. The foot of the operative extremity is secured firmly in a well-padded traction boot. Initially, the hip is abducted between 20 and 45 degrees to clear the perineal post. To optimize capsular relaxation and maximize the potential joint volume, the hip is placed in approximately 10 to 20 degrees of flexion, mild abduction, and slight internal or external rotation depending on the patient's specific capsular tension. This specific orientation relaxes the dense iliofemoral ligament, which is the primary barrier to femoral head distraction. An image intensifier (C-arm fluoroscopy) is then brought into the sterile field, positioned to provide an unobstructed AP view of the hip joint to continuously evaluate the traction vector and guide subsequent needle and instrument placement.
Step-by-Step Surgical Approach and Fixation Technique
The surgical technique begins with the precise identification and marking of surface anatomy. The anterior, posterior, and superior borders of the greater trochanter (GT) are outlined, serving as the primary reference point for the peritrochanteric portals. The Anterior Superior Iliac Spine (ASIS) is palpated and marked. The femoral pulse is identified anteriorly, and its course is delineated to ensure all portals remain safely lateral to this critical neurovascular bundle. The lateral approach typically utilizes three primary portals: the Anterior Peritrochanteric (AP), Posterior Peritrochanteric (PP), and Direct Anterior (DA) portals.
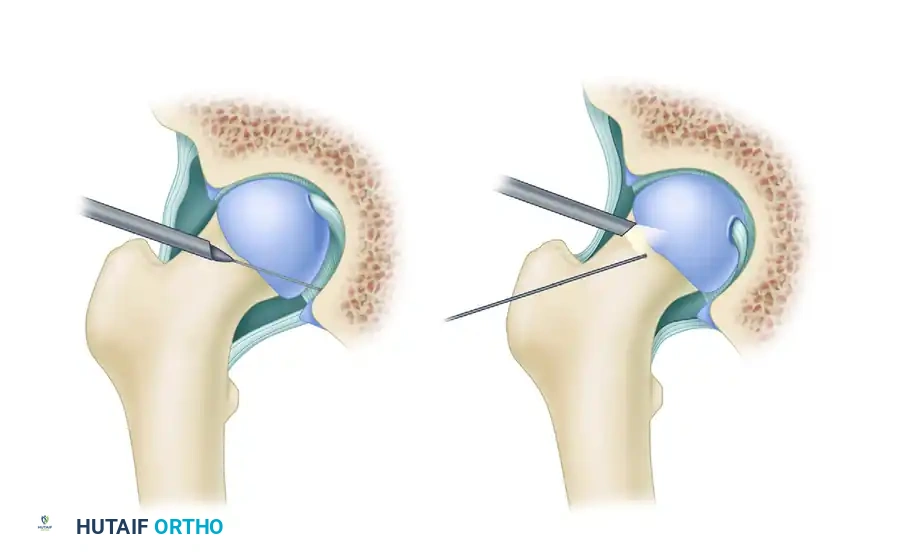
The initial access is most frequently achieved via the Anterior Peritrochanteric portal. Under continuous C-arm fluoroscopic guidance, a 6-inch, 18-gauge spinal needle is inserted slightly anterior and superior to the anterior tip of the greater trochanter. The trajectory is directed toward the central compartment, aiming for the "safe zone" between the femoral head and the lateral acetabular rim. The surgeon must rely on tactile feedback to feel the needle puncture the dense capsule while taking extreme care to avoid skewering the acetabular labrum or scuffing the femoral head cartilage. Once intra-articular placement is confirmed radiographically, the vacuum seal is broken by injecting 20 to 30 cc of sterile saline or ambient air. This immediately allows the joint to distract the requisite 8 to 10 millimeters. A flexible Nitinol guidewire is introduced through the needle, followed by a small skin incision, and a cannulated obturator and arthroscope cannula are passed over the wire using a firm twisting motion to breach the capsule.
With the arthroscope in the central compartment, the Direct Anterior portal is established under direct visualization. The landmark for this portal is the intersection of a sagittal line drawn distally from the ASIS and a horizontal line drawn medially from the proximal tip of the greater trochanter. A spinal needle is inserted at a 45-degree cephalad and 20-degree medial angle. Direct arthroscopic visualization ensures the needle enters safely anterior to the labrum. To protect the highly variable branches of the Lateral Femoral Cutaneous Nerve (LFCN), the skin incision must be limited strictly to the epidermis and dermis. A hemostat is then used to bluntly dissect through the subcutaneous adipose tissue down to the capsular level, pushing the nerve branches safely aside before introducing the cannula. The Posterior Peritrochanteric portal is subsequently established using similar fluoroscopic and direct visual guidance, aiming slightly anterior to avoid the posterior-lying sciatic nerve.
Once portals are established, an interportal capsulotomy is performed to connect the portal entry sites, utilizing a radiofrequency ablation wand or an arthroscopic scalpel. This controlled release of the thick iliofemoral ligament is essential to achieve the maneuverability required for complex instrument triangulation. The central compartment is systematically evaluated, and pathology is addressed. For acetabular labral tears, the "Fixation Technique" involves meticulous preparation of the acetabular rim. A motorized burr is used to decorticate the rim, creating a bleeding cancellous bone bed to promote biological healing, while simultaneously correcting any pincer morphology.
Drill guides are introduced, and anchor trajectories are carefully planned to avoid penetration into the articular cartilage. Suture anchors (typically 1.8mm to 2.9mm in diameter, composed of biocomposite materials or all-suture constructs) are impacted into the rim. Suture passing devices are utilized to shuttle high-strength sutures around or through the labral tissue. The labrum is then anatomically reduced and secured using either knotted or knotless sliding locking configurations, ensuring the restoration of the crucial suction seal against the femoral head. Following central compartment work, traction is released, and the peripheral compartment is accessed to perform a comprehensive osteochondroplasty of the femoral head-neck junction, resecting the cam lesion until normal anterior offset is restored.
Complications, Incidence Rates, and Salvage Management
While lateral decubitus hip arthroscopy is generally safe, the learning curve is notoriously steep, and complications can be devastating if meticulous technique is not adhered to. The overall complication rate ranges from 1.5% to 5%, with the vast majority being minor and transient. However, major complications, particularly those related to positioning, traction, and fluid management, require immediate recognition and aggressive salvage management.
Neurologic complications are the most frequently reported adverse events. Pudendal neuropraxia, characterized by perineal numbness, pain, and potentially sexual dysfunction, is directly correlated with excessive traction time and improper perineal post placement. The incidence ranges from 1% to 2% but is highly preventable by ensuring strict lateralization of the post against the medial thigh and limiting continuous traction to less than 120 minutes. If traction time exceeds this limit, a mandatory 10 to 15-minute release is required to restore perineal perfusion. Sciatic nerve neuropraxia can occur from excessive traction or direct trauma during posterior portal placement, while Lateral Femoral Cutaneous Nerve (LFCN) injury (meralgia paresthetica) occurs in up to 2% of cases due to sharp dissection during anterior portal establishment. Most neuropraxias are transient and resolve within 3 to 6 weeks with supportive care and gabapentinoids, but permanent nerve damage represents a catastrophic failure of technique.
Fluid extravasation is a significant risk due to the high-pressure fluid management systems required to maintain visualization and distention in the hip joint. Extravasation into the surrounding thigh musculature can lead to symptomatic swelling, and in rare cases, true compartment syndrome of the thigh requiring emergent fasciotomy. More insidiously, fluid can track superiorly through the iliopsoas bursa or retroperitoneal space, leading to massive intra-abdominal fluid accumulation. This can precipitate life-threatening abdominal compartment syndrome, hypothermia, and hemodynamic instability. The lateral decubitus position inherently reduces this risk compared to the supine position due to gravitational fluid drainage, but vigilant monitoring of fluid inflow versus outflow is mandatory. If unexplained hypotension or a tense abdomen is noted by the anesthesia team, the procedure must be immediately aborted, and general surgery consultation obtained.
Iatrogenic microinstability is an increasingly recognized complication resulting from aggressive capsulotomies that are left unrepaired. The anterior capsule is a critical restraint to extension and external rotation. Failure to close a large T-capsulotomy or interportal capsulotomy, particularly in patients with baseline ligamentous laxity or borderline dysplasia, can lead to persistent anterior hip pain, subluxation, and rapid joint degeneration. Salvage management for iatrogenic instability requires revision arthroscopy for capsular plication, or in severe cases of capsular deficiency, open or arthroscopic capsular reconstruction utilizing dermal allograft or iliotibial band autograft.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Pudendal Neuropraxia | 1.0% - 2.0% | Prevention: Lateralize perineal post, limit traction < 120 mins. Management: Supportive care, gabapentinoids, usually transient. |
| LFCN Neuropraxia | 1.5% - 2.5% | Prevention: Blunt dissection only for Direct Anterior portal. Management: Observation, local corticosteroid injection for neuroma. |
| Iatrogenic Cartilage Scuffing | 2.0% - 4.0% | Prevention: Break vacuum seal, ensure 8-10mm distraction prior to entry. Management: Debridement of loose flaps; avoid aggressive chondroplasty. |
| Fluid Extravasation (Abdominal) | < 0.5% | Prevention: Monitor fluid deficit, minimize pump pressure, lateral position. Management: Abort procedure, emergent general surgery consult if tense. |
| Iatrogenic Microinstability | 1.0% - 3.0% | Prevention: Routine capsular closure with high-strength sutures. Management: Revision arthroscopy for capsular plication or reconstruction. |
| Heterotopic Ossification (HO) | 1.0% - 5.0% | Prevention: Copious lavage of bone debris, post-op NSAIDs (Naproxen). Management: Observation; surgical excision if mature and symptomatic. |
Phased Post-Operative Rehabilitation Protocols
The success of lateral decubitus hip arthroscopy is inextricably linked to a rigorous, phased postoperative rehabilitation protocol. Rehabilitation must be highly individualized, dictated by the specific intra-articular procedures performed. A simple chondral debridement or isolated osteochondroplasty allows for an accelerated protocol, whereas a complex labral repair, microfracture, or capsular plication necessitates a highly protective and protracted recovery timeline to ensure biological healing.
Phase I: Maximum Protection Phase (Weeks 0 to 4)
The primary goals of the immediate postoperative phase are the protection of the surgical repair, reduction of acute inflammation, and the prevention of intra-articular adhesions. Weight-bearing is typically restricted to 20 pounds flat-foot weight-bearing using crutches for 2 to 4 weeks to protect labral repairs and prevent mechanical overload on osteochondroplasty sites (which are at a theoretical risk for femoral neck fracture). Immediate passive range of motion is initiated, often utilizing a Continuous Passive Motion (CPM) machine for 4 to 6 hours daily, or via a stationary bicycle with zero resistance. An abduction brace may be prescribed to limit hip extension past neutral and external rotation past 20 degrees, critically protecting the healing anterior capsule and iliofemoral ligament repair. Active hip flexion is strictly prohibited to prevent iliopsoas tendinitis, a common and frustrating postoperative complication.
Phase II: Controlled Mobility and Early Strengthening (Weeks 4 to 8)
As biological healing progresses, the patient is gradually weaned off crutches to full weight-bearing with a normalized gait pattern. The focus shifts to restoring full, pain-free range of motion. Early isometric and isotonic strengthening of the gluteus medius, gluteus maximus, and core musculature is initiated. Aquatic therapy is highly beneficial during this phase, providing buoyancy to assist with gait mechanics while offering gentle resistance. The stationary bike resistance is gradually increased. Stretching of the anterior capsule and hip flexors is introduced cautiously, ensuring no stress is placed on the repaired labrum.
Phase III: Advanced Strengthening and Proprioception (Weeks 8 to 16)
This phase emphasizes closed kinetic chain exercises to restore functional strength and neuromuscular control. Exercises such as single-leg mini-squats, lunges, and lateral band walks are incorporated to maximize abductor and external rotator strength. Core stabilization remains a central component, as pelvic control is essential for optimal hip kinematics. Plyometric training and light jogging may be introduced toward the end of this phase, provided the patient demonstrates symmetric strength, no reactive effusion, and a pain-free normalized gait.
Phase IV: Return to Sport and High-Level Function (Weeks 16+)
The final phase bridges the gap between clinical rehabilitation and athletic performance. Progression to high-impact, multidirectional, and sport-specific drills is initiated. Return to play criteria are stringent and include: full, symmetric range of motion; isokinetic strength testing demonstrating >90% symmetry compared to the contralateral limb; successful completion of functional hop testing; and psychological readiness. For elite athletes, full return to high-level competition following labral repair and FAI correction typically requires 6 to 9 months of dedicated rehabilitation.
Summary of Landmark Literature and Clinical Guidelines
The evolution and validation of lateral decubitus hip arthroscopy are deeply rooted in landmark orthopedic literature. Dr. J.M. Glick’s seminal publications in the late 1980s and 1990s were the first to comprehensively describe the lateral approach, detailing the use of the fracture table and the precise anatomical landmarks for the peritrochanteric portals. His early work established the foundational safety profile of the technique, demonstrating that with meticulous positioning and fluoroscopic guidance, the central compartment could be accessed without the catastrophic morbidity associated with open dislocation.
Subsequent comparative literature has extensively evaluated the supine versus lateral decubitus positions. Studies by high-volume surgeons such as Dienst and Sampson have demonstrated that both positions yield equivalent long-term functional outcomes in the management of FAI and labral pathology. However, these studies consistently highlight the lateral position's superiority in managing obese patients and providing enhanced access to the posterior and lateral compartments. The literature confirms that the lateral position significantly reduces the incidence of fluid extravasation into the abdomen, a critical safety advantage in prolonged, complex reconstructions.
Long-term outcome studies, particularly those with 10-to-15-year follow-ups, have validated the efficacy of arthroscopic FAI correction and labral preservation. Literature from Philippon and Kelly has unequivocally shown that anatomical labral repair, combined with comprehensive restoration of the femoral head-neck offset, halts the progression of chondral damage and significantly improves patient-reported outcome measures (PROMs), such as the modified Harris Hip Score (mHHS) and the Non-Arthritic Hip Score (NAHS). Furthermore, recent biomechanical studies have underscored the critical importance of routine capsular closure, demonstrating that failure to repair the iliofemoral ligament alters hip kinematics and increases contact pressures at the chondrolabral junction.
Current clinical guidelines, including consensus statements from the International Society for Hip Arthroscopy (ISHA), strongly support the use of hip arthroscopy for symptomatic FAI and labral tears in patients without advanced osteoarthritis. The guidelines emphasize that the choice between the supine and lateral decubitus positions should be dictated by surgeon experience, patient morphotype, and specific pathological anatomy. Mastery of the lateral decubitus technique remains an essential skill for the comprehensive joint preservation surgeon, offering unparalleled biomechanical advantages for complex reconstructive challenges.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics ---
