Mastering Type IV Fractures: Essential Periprosthetic Strategies
Key Takeaway
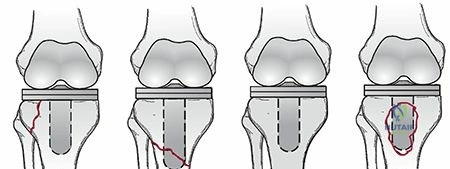
Looking for accurate information on Mastering Type IV Fractures: Essential Periprosthetic Strategies? Type IV fractures, as per the AAOS classification, are periprosthetic fractures located within Level III of the femur. These fractures traverse or lie within the area of the femoral stem. Specifically, type IVA denotes a spiral fracture around the stem tip, while type IVB refers to a simple transverse or short oblique fracture in that region.
Introduction and Epidemiology
Periprosthetic femoral fractures (PFFs) represent a significant and increasingly prevalent complication following total hip arthroplasty (THA), posing substantial challenges for orthopedic surgeons. These fractures are complex entities, often occurring in elderly, osteopenic patients with compromised bone stock and the presence of a foreign body (the prosthetic stem). The title "Mastering Type IV Fractures" refers to the most complex and often distal periprosthetic femoral fractures, frequently encompassing Vancouver Type B3 and Type C classifications, which demand sophisticated surgical strategies for successful outcomes.
Incidence and Mortality
The incidence of PFFs has historically varied based on prosthetic design, surgical technique, and patient demographics. Intraoperative fractures occur with an overall incidence ranging from 0.3% to 5%. Postoperative PFFs, typically defined as those occurring after initial hospital discharge, have an incidence reported around 0.1%.
However, specific risk factors significantly impact these rates:
* PFFs occur more frequently with uncemented components, exhibiting an incidence from 2.6% to 5% in primary THA.
* The incidence escalates dramatically in noncemented revisions, potentially reaching as high as 21%, underscoring the inherent challenges of revision surgery in a compromised bone environment.
Mortality associated with PFFs is a critical concern, particularly in vulnerable populations. Studies indicate a higher mortality rate in patients over 70 years of age, with male patients demonstrating a 2.1% mortality compared to 1.2% in women, highlighting the need for comprehensive medical optimization in these patients.
Risk Factors for Periprosthetic Femoral Fractures
A thorough understanding of predisposing factors is paramount for both prevention and effective management. These can be broadly categorized into patient-related and surgery-related risks.
Patient-Related Risk Factors:
* Osteopenia and Osteoporosis: Diminished bone mineral density, whether primary osteoporosis or secondary to osteolysis around the implant, substantially increases fracture susceptibility.
* Rheumatoid Arthritis: Patients with inflammatory arthropathies often present with poorer bone quality and may be on medications that further impair bone metabolism.
* Previous Failed Open Reduction and Internal Fixation (ORIF): Prior trauma or surgery to the femur can create areas of cortical weakening, stress risers, and altered bone morphology.
Surgery-Related Risk Factors:
* Stress Risers Secondary to Cortical Defects: Existing or iatrogenically created cortical defects (e.g., screw holes from previous hardware, cortical windows) can concentrate stress and initiate fracture propagation.
* Revision Surgery: The process of implant removal, reaming, and broaching in an already compromised femur significantly elevates the risk of fracture. This is the predominant setting for Type IV/Vancouver B3 fractures.
* Inadequate Implant Site Preparation: Using an inappropriately large implant or insufficient reaming or broaching can lead to excessive hoop stress and subsequent fracture during stem insertion.
* Pericapsular Pathology: A scarred or contracted capsule, if inadequately released, can impede surgical access and leverage, contributing to intraoperative fracture during component manipulation or dislocation.
* Loose Components: A loose femoral component can lead to altered load transfer and localized stress, contributing to cortical erosion and subsequent fracture, accounting for up to 33% of periprosthetic femur fractures in some series.
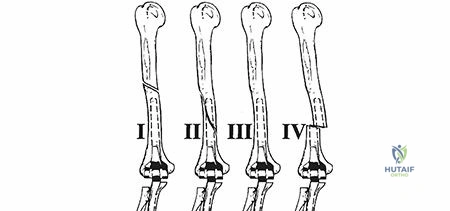
Figure 1: Radiograph illustrating a periprosthetic femoral fracture (Type IV equivalent) distal to a well-fixed femoral stem.
Figure 2: Lateral view of a periprosthetic femoral fracture, demonstrating complex comminution in the distal segment.
Surgical Anatomy and Biomechanics
Effective management of Type IV PFFs necessitates a robust understanding of femoral anatomy, periprosthetic bone characteristics, and the biomechanical interplay between the implant and bone.
Femoral Anatomy and Periprosthetic Morphology
The femur is a long bone with specific curvatures (anterior bow and varying angles of anteversion/retrovulsion) that influence implant selection and fracture patterns. The cortical thickness varies along its length, being densest in the mid-diaphysis and thinner proximally and distally. The presence of a femoral stem alters the natural stress distribution within the bone, creating areas of stress shielding (reduced stress in areas protected by the implant) and stress concentration (at the tip of the stem, around screw holes, or at transitions in cortical thickness).
For Type IV fractures, which typically involve the distal femur (Vancouver Type C) or significant portions of the diaphyseal bone with severe bone loss and an unstable implant (Vancouver Type B3), specific anatomical considerations are critical:
* Distal Femoral Metaphysis: This region is characterized by thinner cortices, cancellous bone dominance, and proximity to the knee joint. Fixation in this area requires implants designed for metaphyseal engagement.
* Medial and Lateral Columns: Understanding the structural integrity of these columns is essential for planning plate application.
* Vascularity: The rich vascular supply to the femur can be compromised by extensive dissection, prior surgery, or fracture displacement, potentially impacting bone healing.
Biomechanical Principles of Periprosthetic Fractures
The biomechanics of a periprosthetic femur differ significantly from an intact femur. The stem acts as a load-bearing structure, which can either protect the bone or create stress risers.
* Stress Shielding: The stiff metallic stem unloads the surrounding bone, particularly proximally, potentially leading to bone atrophy and increased porosity, predisposing to fracture.
* Stem-Bone Interface: The quality of the interface (cemented vs. uncemented, porous coating) influences load transfer. A loose stem or a short stem can create a significant stress riser at its distal tip.
* Working Length of Fixation: For plate fixation, the concept of working length (the unsupported length of the plate between the innermost screws proximal and distal to the fracture) is critical. Longer working lengths generally allow for more elastic fixation, promoting secondary bone healing, while shorter working lengths provide rigid fixation, suitable for absolute stability in certain fracture patterns.
* Neutral Bending Axis: Understanding the neutral bending axis of the femur (approximately anterolateral) is important for placing cortical windows or strut grafts to minimize their impact as stress risers.
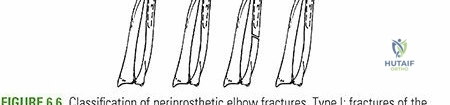
Figure 3: Illustration of various femoral stem designs and their interaction with femoral bowing, critical for understanding stress distribution.
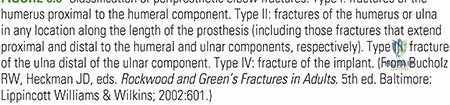
Figure 4: Diagram showing stress shielding effects around a femoral stem, leading to bone resorption in proximal areas.
Indications and Contraindications
The decision-making process for managing Type IV PFFs is complex, weighing fracture characteristics, implant stability, bone quality, and patient-specific factors.
Operative Indications
The vast majority of Type IV PFFs, including Vancouver B3 and C fractures, necessitate surgical intervention due to their inherent instability and the presence of compromised bone and/or implant.
* Displaced or Unstable Fractures: Any fracture with significant displacement (e.g., >2mm or >10 degrees angulation), rotational deformity, or inherent instability that precludes non-operative healing.
* Unstable Femoral Component (Vancouver B2/B3): If the femoral stem is loose, significantly subsided, or clearly failed, revision of the stem is indicated, often combined with fracture fixation. This is a hallmark of many "Type IV" scenarios.
* Fractures Distal to a Stable Stem (Vancouver C): Although the stem is stable, the fracture requires internal fixation to restore mechanical integrity and allow weight-bearing.
* Fracture Nonunion or Malunion: Failed previous treatment or malalignment requiring corrective osteotomy.
* Functional Impairment: Inability to mobilize or bear weight, leading to significant disability and loss of independence.
* Prophylactic Fixation: Rarely, for impending fractures with severe cortical thinning or large stress risers, although this is less common for established Type IV fractures.
Non-Operative Indications
Non-operative management of Type IV PFFs is rarely appropriate due to the complexity and instability typically associated with these fracture patterns. It may be considered under highly specific circumstances.
* Non-Displaced, Stable Fractures with Stable Implant (Vancouver B1 or stable A): While Type IV usually refers to B3 or C, if a truly minimally displaced fracture occurs in a low-demand patient with a stable component and excellent bone stock (e.g., a hairline crack not compromising stability), non-operative treatment with protected weight-bearing could be contemplated, though this is exceedingly rare for what would be classified as "Type IV".
* Prohibitive Medical Comorbidities: Patients with severe, uncorrectable medical conditions that render them unfit for major surgery, where the risks of anesthesia and intervention outweigh the potential benefits.
* Non-Ambulatory Status: For patients who are pre-morbidly non-ambulatory and experiencing minimal pain, the goal may shift from functional recovery to comfort, with operative intervention deemed unnecessary.
Contraindications
Absolute contraindications to operative management of Type IV PFFs are limited and primarily revolve around patient fitness and active infection.
* Active Periprosthetic Joint Infection: Surgery in the presence of active infection carries a high risk of propagation and treatment failure. Definitive fracture management should typically be delayed until the infection is controlled, often through a two-stage approach.
* Extremely Poor Medical Prognosis/Life Expectancy: If a patient's life expectancy is very short or their medical status is extremely fragile, rendering recovery from major surgery improbable.
Table: Operative vs. Non-Operative Indications for Periprosthetic Femur Fractures
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Displacement | Displaced (>2mm, >10° angulation) | Non-displaced, stable (rare for Type IV) |
| Implant Stability | Unstable femoral component (Vancouver B2/B3) | Stable femoral component (Vancouver B1/C – if fracture stable) |
| Fracture Location | Distal to stem (Vancouver C) | Proximal or diaphyseal, minimal displacement, stable implant (rare) |
| Bone Stock Quality | Poor bone stock requiring reconstruction (Vancouver B3) | Adequate bone stock, minimal comminution (rare) |
| Patient Function | Ambulatory patient with significant functional impairment | Non-ambulatory, minimal pain, no functional demand |
| Comorbidities | Medically optimized for surgery | Prohibitive medical comorbidities, high surgical risk |
| Specific Scenarios | Nonunion/Malunion, impending fracture in selected cases | Active infection (defer definitive fixation) |
Figure 5: Preoperative radiograph demonstrating a Vancouver Type C fracture, distal to a well-fixed stem, requiring ORIF.
Pre Operative Planning and Patient Positioning
Comprehensive preoperative planning is the cornerstone of successful management for Type IV PFFs. These are often complex cases that benefit from a systematic approach to imaging, implant selection, and surgical strategy.
Comprehensive Patient Evaluation
Beyond the immediate fracture, a thorough assessment of the patient's overall health is essential. This includes:
* Medical Comorbidities: Identification and optimization of cardiac, pulmonary, renal, and metabolic conditions. Geriatric consultation may be beneficial.
* Nutritional Status: Malnutrition can impair wound healing and bone consolidation.
* Functional Status and Activity Level: Pre-injury mobility and expected post-operative demands influence implant choices and rehabilitation goals.
* Bone Quality Assessment: Clinical history (osteoporosis, steroid use, previous fractures), DEXA scans if available, and radiographic evidence of osteopenia or osteolysis.
Advanced Imaging
Standard radiographs (AP and lateral views of the entire femur, including hip and knee joints) are the initial step. However, Type IV fractures often benefit from more advanced imaging:
* Oblique Views: Can better delineate fracture lines, comminution, and implant-bone interface.
* Computed Tomography (CT) Scan: Indispensable for assessing fracture morphology, comminution, implant loosening (especially with metal artifact reduction sequences), and bone stock. This aids in surgical approach planning and implant templating.
* Bone Scan or Aspiration: In cases where infection is suspected, these are crucial for differential diagnosis, as infection significantly alters management.
Implant Analysis and Templating
Detailed analysis of the existing femoral stem is vital.
* Stem Type: Cemented vs. uncemented, material, geometry (tapered, cylindrical), modularity. This dictates removal strategy and potential compatibility with revision systems.
* Stem Length and Position: Assess if the stem is appropriately sized and centered. A short stem may have contributed to distal stress risers.
* Signs of Loosening: Subsidence, cement mantle fracture, peri-prosthetic lucencies, cement debonding.
Extensive templating is mandatory. This involves using full-length radiographs and ideally CT data to:
* Determine Fracture Reduction Strategy: Identify key fragments and plan their reduction.
* Select Revision Stem (if needed): For Vancouver B2/B3, plan for a longer, often extensively coated or modular stem that bypasses the fracture by at least two cortical diameters or 4-6 cm, whichever is greater, and achieves distal fixation in healthy bone.
* Select Fixation Plate: For Vancouver C fractures, plan for a long locking compression plate (LCP) or a specific distal femoral plate. The plate should span the fracture adequately, with sufficient screw fixation both proximal (to the existing stem or healthy bone) and distal.
* Anticipate Bone Grafting/Allograft Needs: Plan for structural or particulate allografting, especially in cases of significant bone loss or comminution (seed content point 15, 16).
* Consider Strut Allograft or Plate Support: For substantial diaphyseal defects or to augment fixation, particularly in B3 scenarios (seed content point 16).
Surgical Strategy Refinement
Based on imaging and templating:
* Approach Planning: Determine the optimal surgical approach (e.g., standard lateral, direct anterior, extended trochanteric osteotomy, transfemoral).
* Instrumentation: Ensure availability of revision instrument sets, stem removal tools, various plate lengths, screws, cables, and bone graft materials.
* Anticipate Challenges: Plan for potential difficulties such as retained cement, broken implants, or severe bone loss.
* Cortical Windows: If utilized for stem removal or inspection, plan their anterolateral location in line with the neutral bending axis of the femur, ensuring they are <30% of the bone diameter (seed content points 17, 18). These are strategic for minimizing future stress risers.
* Correct Starting Point for Reaming/Broaching: Crucial for preventing iatrogenic fracture during stem insertion, especially in revision settings (seed content point 19).
Patient Positioning
The choice of patient positioning depends on the planned surgical approach and surgeon preference.
* Lateral Decubitus Position: Most common for posterolateral or direct lateral approaches. Allows excellent access to the entire femoral shaft. Requires careful padding and securing the patient.
* Supine Position: Often preferred for direct anterior approaches. Can also be used for some lateral approaches with a bump under the hip.
* Prepping and Draping: Ensure wide sterile field, extending from the iliac crest to below the knee, allowing for intraoperative fluoroscopy and potential longer incisions.
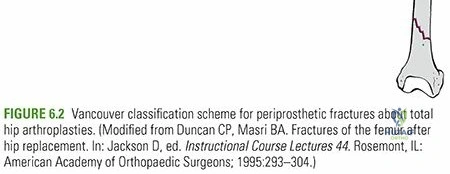
Figure 6: Preoperative templating example, illustrating selection of a revision stem to bypass the fracture and achieve stable fixation.
Figure 7: Anteroposterior and lateral radiographs showing an extensively porous-coated revision stem used for a complex periprosthetic fracture.
Detailed Surgical Approach and Technique
The surgical management of Type IV PFFs, encompassing Vancouver B3 and C fractures, is highly individualized and demands meticulous technique. The primary goals are fracture reduction, stable fixation, and restoration of mechanical alignment and length, often coupled with revision of the femoral component.
Surgical Exposures
The choice of surgical approach is dictated by the fracture location, implant characteristics, and the need for stem removal.
* Standard Lateral Approach (Modified Hardinge): A versatile approach offering excellent exposure of the entire femoral shaft. It involves splitting the vastus lateralis, preserving abductor musculature.
* Posterolateral Approach: Provides good posterior exposure, useful if posterior comminution or displacement is significant.
* Direct Anterior Approach: Less commonly used for extensive PFFs due to limited exposure of the distal femur and challenges with stem removal.
* Extended Trochanteric Osteotomy (ETO): A critical approach for Vancouver B2/B3 fractures requiring the removal of well-fixed or extensively ingrown femoral stems. It involves osteotomizing a segment of the greater trochanter with attached abductors, reflecting it proximally, providing wide exposure to the proximal femur and enabling controlled stem removal. The osteotomy is then reattached with cables or wires.
* Transfemoral Approach: A more extensive osteotomy of the femoral shaft (often spiral or oblique) allowing for direct visualization and removal of a very difficult stem, particularly in severely malaligned or compromised femurs. This approach is reserved for the most challenging B3 scenarios.
Fracture Classification and Treatment Principles
As stated in the introduction, "Type IV fractures" will be addressed in the context of the widely accepted Vancouver Classification system for PFFs, specifically focusing on complex B3 and C types.
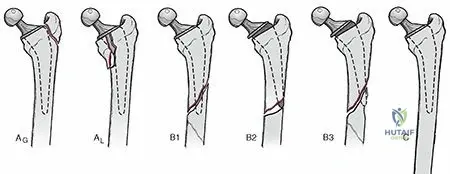
- Vancouver Type A Fractures: Proximal to the stem, stable implant. Treated with ORIF or non-operatively if stable.
- Vancouver Type B Fractures: Occur around or at the level of the stem.
- Type B1: Stable stem, adequate bone stock. Treated with ORIF (plate and cables).
- Type B2: Unstable stem, adequate bone stock. Requires stem revision (often with a longer, uncemented, extensively coated stem) and fracture fixation.
- Type B3: Unstable stem, poor bone stock (comminution, osteolysis). The most challenging, requiring stem revision with significant bone reconstruction (allografts, impaction grafting) and fracture fixation. This often aligns with the complexity implied by "Type IV".
- Vancouver Type C Fractures: Distal to a stable stem. Treated with ORIF (long plate fixation). This also aligns with "Type IV" when involving significant distal comminution or bone loss.
Stem Revision for Unstable Implants (Vancouver B2/B3)
- Exposure and Fragment Mobilization: After appropriate exposure (often ETO for B2/B3), carefully dissect soft tissues to identify fracture fragments. Use cerclage wires or clamps to provisionally stabilize major fragments and aid in reduction.
- Stem Removal: This is a critical and potentially destructive step.
- Cemented Stems: Removal involves identifying and removing the cement mantle using osteotomes, burs, and ultrasonic devices. Careful attention is needed to avoid perforation.
- Uncemented Stems: May require extensive burring, osteotome work along the stem-bone interface, and specialized extractors. The use of cortical windows (seed point 17) can facilitate stem removal by allowing direct visualization and controlled osteotome access. These windows should be placed anterolaterally in line with the neutral bending axis and be limited to less than 30% of the bone diameter (seed point 18) to minimize creating new stress risers.
- Bone Stock Management and Reconstruction:
- For significant diaphyseal defects or comminution, impaction bone grafting with morselized allograft is a viable option to reconstruct the femoral canal and provide biological support.
- Structural allografts or strut allografts can be used to bridge large defects or augment the host bone, often secured with cerclage wires or screws (seed point 16).
- Revision Stem Insertion: Select a revision stem (e.g., modular, extensively coated, tapered fluted) that is long enough to bypass the most distal fracture line by at least two cortical diameters (seed point 14). Achieve stable distal fixation in healthy bone. Ensure correct starting point for reaming/broaching (seed point 19) to avoid iatrogenic fracture.
- Fracture Fixation: Once the revision stem is implanted, the fracture fragments are reduced and secured to the stem or host bone using cerclage wires, cables, or plates. Plates are often applied to the lateral aspect of the femur, bridging the defect and securing fragments. Bone grafting the defect (seed point 15) is critical to promote healing.
Open Reduction and Internal Fixation for Distal Fractures (Vancouver C)
- Exposure and Reduction: A standard lateral approach provides excellent access. Distal femoral fractures are often highly comminuted. Indirect reduction techniques are preferred to preserve soft tissue attachments. Traction on the leg and manipulation with bone clamps or external fixator pins can aid reduction. Cerclage wires may be used provisionally to hold comminuted fragments or to create a stable tube for plate application.
- Plate Selection and Application:
- Locking Compression Plates (LCPs): Distal femoral LCPs are the workhorse for Vancouver C fractures. These precontoured plates are designed to match the distal femoral anatomy and provide angular stable fixation, which is crucial in osteopenic bone.
- The plate should be long enough to span the fracture, extending well into healthy bone both proximally (around the existing stable stem) and distally (into the metaphyseal/epiphyseal bone).
- Fixation Principles:
- Bicortical Screw Fixation: Aim for bicortical screws whenever possible, particularly distally, for maximal purchase.
- Working Length: Utilize the locking plate principles of relative stability. Ensure adequate working length between the most proximal and distal screw clusters to allow for micro-motion and callus formation.
- Screw Density: Adequate number of screws proximally and distally, typically 3-4 bicortical screws in each main fragment.
- Bypassing the Stem: If the fracture is close to the stem, ensure screws proximal to the fracture engage sound bone around or through the existing stem, or if possible, avoid direct contact with the stem to prevent stress shielding at the plate-stem interface.
- Bone Grafting: Autograft or allograft material can be packed into comminuted areas or bone defects to promote healing.
- Wound Closure: Meticulous layered closure with attention to muscle repair and skin approximation.
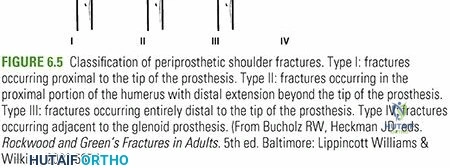
Figure 8: Intraoperative image demonstrating fracture reduction and temporary fixation with cerclage wires in preparation for definitive plating.
Figure 9: Radiograph showing a distal femoral locking plate used to stabilize a Vancouver Type C fracture.
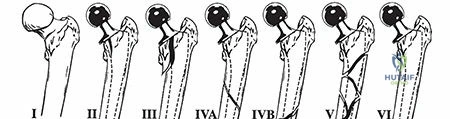
Figure 10: Surgical view of a long stem revision, highlighting the challenge of achieving stable fixation in compromised bone.
Figure 11: Postoperative radiograph demonstrating a successfully fixed Vancouver Type C fracture with a long locking plate spanning the fracture zone.
Complications and Management
Despite meticulous surgical planning and execution, complications following Type IV PFFs can be significant and require prompt recognition and appropriate management strategies.
Nonunion and Malunion
- Etiology: Nonunion (failure of bone healing) or malunion (healing in an unacceptable alignment) can result from inadequate reduction, unstable fixation, poor bone quality, infection, soft tissue interposition, or biological factors (e.g., poor vascularity, systemic illness).
- Incidence: Varies widely, reported between 5% and 20%, particularly in complex Type B3 and C fractures.
- Salvage Strategies:
- Nonunion: Requires revision surgery, often with more stable fixation (e.g., longer plate, larger stem), removal of nonunion tissue, aggressive debridement of fibrous tissue, bone grafting (autograft or allograft), and potentially biological augmentation (e.g., bone morphogenetic proteins). Correction of any underlying mechanical instability is paramount.
- Malunion: If symptomatic (e.g., leg length discrepancy, gait disturbance, pain, patellofemoral issues), corrective osteotomy and refixation may be indicated. Asymptomatic malunions may be observed.
Infection
- Etiology: Can be acute (perioperative contamination) or chronic (hematogenous spread or low-grade infection). The presence of a prosthesis increases the risk and complexity of treatment.
- Incidence: Ranges from 1% to 5%, but can be higher in revision cases.
- Salvage Strategies:
- Acute Infection (<4-6 weeks): Aggressive surgical debridement, irrigation, retention of stable implants (if feasible), and targeted intravenous antibiotics.
- Chronic Infection (>6 weeks) or Unstable Implants: Typically requires a staged approach:
- Explant of all prosthetic components, thorough debridement, placement of an antibiotic-loaded cement spacer, and targeted intravenous antibiotics.
- After infection markers normalize and symptoms resolve, reimplantation of new components. This is a very challenging scenario in Type IV fractures.
Implant Failure
- Etiology: Can manifest as screw breakage, plate fracture, stem loosening, or stem fracture. This is often a consequence of nonunion, excessive loading before healing, inadequate initial fixation strength, or progressive osteolysis.
- Incidence: Varies with fracture type and fixation method. Plate breakage in nonunion can be as high as 10-15%.
- Salvage Strategies: Revision fixation with a stronger construct, addressing the underlying cause of failure (e.g., nonunion management). This may involve converting to a longer revision stem and supplemental plating.
Neurovascular Injury
- Etiology: Potential for injury to the femoral nerve, sciatic nerve, superficial femoral artery, or profunda femoris vessels during exposure, dissection, implant insertion, or reduction maneuvers.
- Incidence: Relatively low but devastating, <1%.
- Salvage Strategies: Immediate recognition is key. Vascular injuries require surgical repair by a vascular surgeon. Nerve injuries require close observation, electrodiagnostic studies, and often exploration if there is no sign of recovery.
Leg Length Discrepancy
- Etiology: Can result from improper fracture reduction, inappropriate stem length selection, or subsidence of the implant.
- Incidence: Varies with surgical technique and fracture complexity.
- Salvage Strategies: Significant symptomatic discrepancies may require shoe lifts, but severe discrepancies impacting gait or spine can necessitate revision arthroplasty to correct length.
Persistent Pain
- Etiology: Can be multifactorial: nonunion, implant loosening, nerve irritation, soft tissue impingement, chronic regional pain syndrome, or referred pain.
- Salvage Strategies: Thorough diagnostic workup including advanced imaging, nerve blocks, and ruling out infection. Treatment focuses on addressing the underlying cause.
Table: Common Complications of Periprosthetic Femur Fractures
| Complication | Incidence (%) | Salvage Strategies |
|---|---|---|
| Nonunion/Malunion | 5-20 | Revision fixation, bone grafting, debridement, corrective osteotomy, biological augmentation |
| Infection | 1-5 | Debridement, antibiotics, implant retention (acute) or staged explant/reimplant (chronic) |
| Implant Failure | Variable | Revision fixation with stronger construct, addressing underlying nonunion |
| Neurovascular Injury | <1 | Immediate surgical repair (vascular), observation/exploration (nerve) |
| Leg Length Discrepancy | Variable | Shoe lift, revision arthroplasty for severe symptomatic cases |
| Persistent Pain | Variable | Diagnostic workup, address underlying cause, pain management |
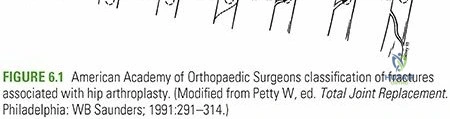
Figure 12: Radiograph showing a nonunion of a periprosthetic fracture, leading to implant loosening and requiring revision surgery.
Figure 13: Example of hardware failure (plate breakage) in a nonunion setting, necessitating further intervention.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation for Type IV PFFs is crucial for achieving optimal functional outcomes and preventing further complications. Protocols must be individualized based on fracture stability, fixation achieved, bone quality, and patient comorbidities. A multidisciplinary approach involving surgeons, physical therapists, and occupational therapists is essential.
Early Postoperative Phase (Weeks 0-6)
The initial phase focuses on pain control, wound healing, prevention of complications, and protecting the surgical repair.
* Pain Management: Aggressive multimodal pain control to facilitate early mobilization.
* Wound Care: Meticulous monitoring for signs of infection or wound dehiscence.
* Deep Vein Thrombosis (DVT) Prophylaxis: Pharmacological and mechanical prophylaxis initiated immediately postoperatively.
* Weight-Bearing Status: This is the most critical variable.
* Vancouver C (Stable Fixation): Often allowed protected weight-bearing (toe-touch or partial weight-bearing 25-50%) with crutches or a walker. Full weight-bearing is progressed based on radiographic healing.
* Vancouver B3 (Stem Revision with Bone Reconstruction): Typically requires strict non-weight-bearing or minimal toe-touch weight-bearing for 6-12 weeks, sometimes longer, to allow for bone graft incorporation and stem osseointegration.
* Range of Motion (ROM):
* Gentle, active-assisted and passive ROM exercises for the hip and knee, often within pain limits, to prevent stiffness.
* Continuous Passive Motion (CPM) machine may be used for knee ROM after distal femoral fractures.
* Muscle Activation: Isometric exercises for hip abductors, quadriceps, and gluteal muscles. Ankle pumps.
* Mobilization: Out-of-bed transfers and pivot transfers initiated early, adhering to weight-bearing restrictions.
Intermediate Phase (Weeks 6-12)
This phase focuses on progressive loading, strengthening, and gait retraining, contingent on radiographic evidence of healing.
* Radiographic Assessment: Repeat radiographs at 6 and 12 weeks to assess fracture healing. Progression of weight-bearing is based on signs of callus formation and stability.
* Progressive Weight-Bearing: Gradually increase weight-bearing as tolerated and as radiographic healing progresses. Transition from walker to crutches, then to a single cane.
* Strengthening: Progressive resisted exercises for hip and knee musculature. Focus on hip abductors, extensors, and knee extensors/flexors.
* Gait Training: Emphasis on proper gait mechanics, balance, and endurance.
* Proprioception and Balance: Exercises to improve neuromuscular control.
* Activities of Daily Living (ADLs): Training for independence in daily tasks.
Advanced Phase (Weeks 12+)
This phase targets restoration of full strength, endurance, and return to pre-injury activities.
* Full Weight-Bearing: Achieved once complete radiographic union is confirmed and pain-free.
* Advanced Strengthening: Incorporate functional exercises, stairs, and uneven surfaces. Resistance training with increased loads.
* Sport-Specific Training: For active individuals, gradual reintroduction to low-impact recreational activities, guided by the physical therapist and surgeon. High-impact activities are generally discouraged.
* Long-Term Monitoring: Regular follow-up appointments (e.g., annually) with radiographs to monitor implant stability, bone remodeling, and identify late complications like osteolysis or heterotopic ossification.
Summary of Key Literature and Guidelines
The management of periprosthetic femoral fractures, particularly complex Type IV variants, has evolved significantly with advancements in implant design, surgical techniques, and a deeper understanding of fracture biomechanics. Key literature and guidelines consistently emphasize a few core principles.
Classification Systems
The Vancouver Classification System remains the international gold standard for categorizing PFFs. Its utility lies in guiding treatment decisions based on fracture location (A, B, C), implant stability (1, 2, 3), and bone stock quality (1, 2, 3).
* As elaborated, "Type IV fractures" in the context of this review largely refer to Vancouver Type B3 and Type C fractures, representing scenarios of unstable stems with poor bone stock or fractures distal to a stable stem, respectively. These categories demand the most intensive surgical planning and execution. While other regional classifications exist (e.g., the incomplete AAOS classification mentioned in the seed content), the Vancouver system is preferred for its comprehensive, prognostic, and treatment-guiding utility.
Core Treatment Principles
- Achieve Stable Fixation: Whether through plate osteosynthesis (for Type C) or revision arthroplasty with an extensively coated or modular stem (for Type B3), mechanical stability is paramount for bone healing. Locking plates have revolutionized the management of distal femoral fractures, providing angular stability crucial in osteopenic bone.
- Restore Bone Stock: Especially for Vancouver B3 fractures, reconstruction of the femoral canal and diaphyseal defects using impaction grafting or strut allografts is critical to ensure long-term stability of the revision stem and promote healing. The use of longer stems to bypass fracture lines and achieve fixation in healthy bone is a well-established principle (seed point 14).
- Optimal Implant Selection: The choice between cable plates, conventional plates, locking plates, and various revision stems (e.g., cemented vs. uncemented, porous-coated, modular, tapered fluted) depends on the specific fracture pattern, bone quality, and surgeon experience.
- Meticulous Surgical Technique: Precise reduction, careful handling of soft tissues, diligent stem removal, and accurate implant placement are crucial to minimize complications. Prophylactic measures such as appropriate reaming/broaching (seed point 19) and judicious use of cortical windows (seed points 17, 18) should be adhered to.
- Multidisciplinary Approach: Successful outcomes are often facilitated by close collaboration among orthopedic surgeons, geriatricians, anesthesiologists, and rehabilitation specialists, particularly for the elderly population with multiple comorbidities.
Evolving Strategies
Recent literature has explored the role of newer generation modular revision stems for B3 fractures, offering intraoperative flexibility. The debate continues regarding the optimal length of fixation, screw density, and the ideal biological augmentation strategies. Furthermore, advancements in 3D templating and patient-specific guides are promising for improving the precision of complex PFF revisions.
In conclusion, mastering Type IV periprosthetic femoral fractures necessitates a comprehensive approach, integrating thorough preoperative assessment, adherence to established biomechanical principles, meticulous surgical technique guided by the Vancouver classification, and a structured, individualized rehabilitation protocol. Continued vigilance against complications and a commitment to evolving best practices are essential for improving patient outcomes in this challenging clinical scenario.
Clinical & Radiographic Imaging