Mastering Distal Femur ORIF: An Intraoperative Guide to Complex Fractures

Key Takeaway
This masterclass provides an immersive, step-by-step guide to open reduction and internal fixation (ORIF) of distal femur fractures. Fellows will learn comprehensive surgical anatomy, meticulous preoperative planning, and granular intraoperative execution techniques. We cover neurovascular risks, muscle dynamics, precise hardware application, and strategies for managing potential complications, ensuring optimal patient outcomes for these challenging injuries.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we are confronting the distal femur fracture—a notoriously unforgiving injury that demands absolute precision, a mastery of 3D biomechanics, and flawless surgical execution. These are not merely fractured bones; they are complex disruptions of the lower extremity's load-bearing architecture. Handled poorly, the long-term outcomes are devastating, leading to post-traumatic arthritis, limb length discrepancy, and profound functional deficits. Handled with expertise, we restore not just anatomy, but the patient's biomechanical foundation and quality of life. Our ultimate objective is a perfect triad: anatomical articular congruity, exact mechanical axial alignment, and restoration of anatomical length.

Occurring within the terminal 9 to 15 cm of the femur, these fractures represent up to a third of all femoral fractures (excluding the hip) and frequently violate the articular surface. We operate on a bimodal demographic: high-energy polytrauma in the young, and low-energy osteoporotic insufficiency in the elderly. The epidemiology of these fractures is rapidly evolving. With the exponential rise in total knee arthroplasties (TKA), the incidence of periprosthetic distal femur fractures has surged, presenting a unique subset of challenges involving compromised bone stock, retained cement mantles, and the necessity of achieving fixation around existing hardware. Regardless of the patient profile, anatomic reduction of the joint surface remains our non-negotiable primary mandate.

The pathophysiology of distal femur fractures is dictated by the mechanism of energy transfer and the inherent structural vulnerabilities of the metaphyseal bone. In high-energy blunt trauma, axial loading combined with varus, valgus, or rotational moments results in severe comminution, often driving the diaphyseal shaft into the intercondylar notch, effectively splitting the condyles. This creates the classic AO/OTA type 33-C3 fracture pattern. Conversely, in the osteoporotic patient, a simple ground-level fall can result in a spiral metaphyseal fracture that propagates into the joint. The soft tissue envelope, while more robust than that of the distal tibia, is frequently subjected to massive stripping from the initial trauma, predisposing the patient to hematoma formation, delayed healing, and deep infection.

Historically, the management of these fractures was fraught with high rates of nonunion and hardware failure, largely due to a misunderstanding of the interplay between absolute and relative stability. The evolution from rigid, non-locking plates that compressed the periosteum to modern pre-contoured, locked plating systems has revolutionized our approach. We now understand that while the articular block demands absolute stability and primary bone healing via interfragmentary compression, the metaphyseal-diaphyseal segment requires relative stability. This modern paradigm promotes secondary bone healing through enchondral ossification, preserving the delicate periosteal blood supply and mitigating the risk of biologically barren nonunions.
Detailed Surgical Anatomy and Biomechanics
To execute a flawless reduction, you must think in three dimensions and anticipate the muscular forces actively fighting your hardware. The supracondylar zone is the crucial transition from diaphyseal cortical bone to the structurally weaker cancellous bone of the condyles. This thin-cortex, wide-canal architecture explains the severe comminution often encountered, particularly in osteoporotic bone. Crucially, the distal femur is trapezoidal in cross-section. The posterior aspect is vastly wider than the anterior face (decreasing in width by nearly 25% as you move anteriorly). When contouring and applying your lateral plate, this geometry dictates that the plate must sit flush against the anterior half of the condyles to prevent inadvertent malalignment. Furthermore, the medial femoral condyle is deeper (anterior-to-posterior) and extends further distally than the lateral condyle.
To achieve optimal outcomes, we must master the biomechanical battlefield. The mechanical femoral axis—the load-bearing line extending from the center of the femoral head through the center of the knee down to the ankle—typically rests 3 degrees off the vertical. Conversely, the anatomic femoral axis dictates approximately 9 degrees of valgus at the knee joint. Consequently, the lateral distal femur sits at an anatomic axis of roughly 81 degrees, while the medial distal femur rests at 99 degrees. Misjudging this angular relationship by even a few degrees guarantees malalignment, altered joint kinematics, and accelerated post-traumatic osteoarthritis. The surgeon must constantly reference these axes intraoperatively, utilizing fluoroscopy and alignment grids to ensure the mechanical axis passes precisely through the center of the knee joint.
Without complete paralytic anesthesia, fracture reduction is an uphill battle against massive deforming forces. The quadriceps and hamstrings exert profound longitudinal forces, driving severe fracture shortening and proximal migration. The gastrocnemius, originating on the posterior condyles, acts as a relentless flexor of the distal fragment, generating the classic apex-posterior (extension) deformity. In split intra-articular fractures, independent head traction causes insidious rotational malalignment of the individual condyles. Finally, the adductor magnus, anchored to the adductor tubercle, forces the distal segment into a stubborn varus deformity. Overcoming these forces requires strategic use of femoral distractors, Schanz pins as joysticks, and precise patient positioning.

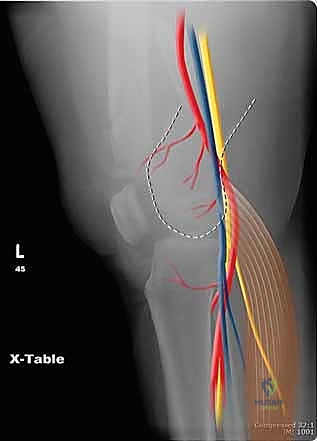
The neurovascular danger zones in this region are unforgiving. The posterior aspect of the distal femur is perilous territory. The popliteal artery and tibial nerve sit in frightening proximity to the posterior bone cortex, separated only by a thin layer of fat and the joint capsule. A posteriorly displaced metaphyseal spike, or careless placement of deep Hohmann retractors over the posterior condyles, can result in catastrophic iatrogenic injury. Proximally and medially, the surgeon must respect the superficial femoral artery (SFA) as it transitions through the adductor hiatus into the popliteal fossa. A meticulous preoperative neurovascular exam is mandatory; any Ankle-Brachial Index (ABI) less than 0.9, side-to-side pulse discrepancy, or expanding hematoma dictates an immediate CT angiogram.
Exhaustive Indications and Contraindications
The rationale for operative intervention in distal femur fractures is overwhelmingly supported by the literature. Non-operative management—typically involving skeletal traction followed by cast bracing—is fraught with complications, including profound knee stiffness, varus/valgus collapse, deep vein thrombosis, and unacceptable malunion. Consequently, conservative management is relegated strictly to non-ambulatory patients with severe baseline dementia, or those whose medical comorbidities render the administration of anesthesia an unacceptable mortality risk. For the vast majority of the population, surgical stabilization is the definitive standard of care, aimed at facilitating early mobilization, restoring joint congruity, and preventing the systemic sequelae of prolonged recumbency.

Absolute indications for Open Reduction and Internal Fixation (ORIF) encompass a broad spectrum of critical scenarios. Open fractures demand immediate operative debridement and stabilization to mitigate the risk of catastrophic osteomyelitis. Fractures associated with acute vascular compromise—such as a popliteal artery tear secondary to a displaced metaphyseal spike—require emergent skeletal stabilization, often preceding or occurring concurrently with vascular repair. Furthermore, any intra-articular fracture with displacement exceeding 2 millimeters necessitates anatomic reduction to prevent rapid-onset post-traumatic arthropathy. Ipsilateral lower extremity injuries, such as the "floating knee" (concomitant tibial shaft fracture), also represent absolute indications to restore the mechanical axis of the entire limb.

Relative indications involve nuanced, patient-specific decision-making. Severe osteopenia or osteoporosis presents a significant challenge; while surgery is indicated, the choice of implant (e.g., dual plating vs. locked lateral plating vs. distal femoral replacement) becomes highly subjective. Periprosthetic fractures above a well-fixed TKA component are generally treated with locked plating, but if the component is loose, revision arthroplasty with a distal femoral replacement may be the superior choice. Additionally, highly comminuted extra-articular fractures (OTA 33-A3) might be managed with minimally invasive plate osteosynthesis (MIPO) or retrograde intramedullary nailing, depending on the surgeon's expertise and the specific fracture morphology.

Contraindications to immediate definitive ORIF must be strictly respected to avoid disastrous outcomes. Active, untreated local infection at the surgical site is an absolute contraindication to internal hardware placement; these cases require aggressive debridement and temporary external fixation. In the setting of a critically unstable polytrauma patient exhibiting the lethal triad of coagulopathy, hypothermia, and acidosis, definitive plating is contraindicated. Instead, Damage Control Orthopedics (DCO) principles must be employed, utilizing rapid external fixation to stabilize the bone and control hemorrhage until the patient's physiologic status is optimized.
| Variable | Indications for Operative Intervention (ORIF/Nailing) | Contraindications to Immediate Definitive Fixation |
|---|---|---|
| Fracture Pattern | Intra-articular displacement > 2mm, coronal plane (Hoffa) fractures, floating knee. | Highly contaminated open fractures (requires staged DCO). |
| Soft Tissue/Vascular | Associated popliteal artery injury, impending compartment syndrome. | Active soft tissue infection, severe burn eschar over the approach site. |
| Patient Physiology | Hemodynamically stable, optimized comorbidities, ambulatory demand. | Unstable polytrauma (lethal triad), medically unfit for anesthesia. |
| Bone Quality | Adequate stock for screw purchase (even in osteoporotic bone with locking plates). | Unreconstructible comminution in the elderly (consider Distal Femoral Replacement). |
Pre-Operative Planning, Templating, and Patient Positioning
Surgical victories are forged in the planning room. Approaching a complex C3 fracture without a 3D mental model and templated hardware is an invitation to failure. Advanced imaging protocols are the cornerstone of this preparation. Plain radiographs, while fundamental, are insufficient on their own. You must obtain full-length femur views to rule out ipsilateral neck or shaft injuries and to assess the uninjured contralateral mechanical axis for templating. Traction radiographs are an invaluable, yet often underutilized, tool; by applying longitudinal traction, the surgeon can pull out metaphyseal comminution, unmasking the true articular fracture profile and providing a clearer picture of the necessary plate length.

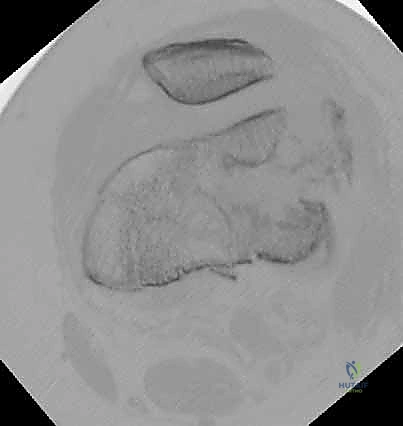
Computed Tomography (CT) is the gold standard and is absolutely mandatory for all intra-articular distal femur fractures. 2D coronal and sagittal cuts, combined with 3D surface-rendered reconstructions, allow the surgeon to map the comminution puzzle meticulously. CT imaging is particularly critical for identifying occult coronal plane fractures (Hoffa fractures), which occur in up to 38% of intra-articular distal femur fractures and are frequently missed on plain films. Failure to identify and independently fix a Hoffa fragment will result in catastrophic articular collapse once the patient begins weight-bearing.
Digital templating transforms the CT data into a definitive surgical blueprint. The surgeon must pre-select the appropriate plate length, ensuring adequate working length and a minimum of three to four bicortical locking screws in the intact diaphyseal bone proximal to the fracture zone. Templating also allows the surgeon to anticipate the trajectory of independent interfragmentary lag screws. These screws must be strategically placed outside the footprint of the lateral locking plate to avoid hardware collision. Meticulous planning of screw trajectories ensures that the anterior-to-posterior screws for a Hoffa fragment do not intersect with the medial-to-lateral screws compressing the intercondylar split.

Patient positioning and operating room setup are critical for intraoperative efficiency. The patient is typically positioned supine on a radiolucent flat table. A sterile bump is placed under the ipsilateral knee to maintain approximately 30 to 45 degrees of flexion; this crucially relaxes the deforming pull of the gastrocnemius muscle, neutralizing the apex-posterior deformity. The fluoroscopy C-arm must be positioned to allow for effortless, orthogonal AP and lateral views of the entire distal femur without moving the patient's leg. A sterile tourniquet is applied high on the thigh, though its inflation is often reserved for specific moments of critical articular visualization to minimize ischemic time to the soft tissues.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Approaches and Soft Tissue Management
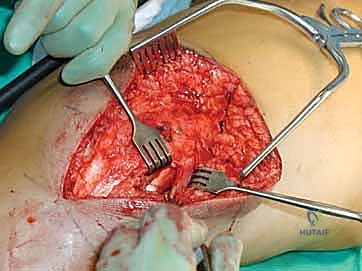
The choice of surgical approach dictates the quality of your articular exposure. For complex intra-articular fractures (Type C), the lateral parapatellar approach is the workhorse. The incision begins laterally over the diaphysis and extends distally, curving gently anterior to the lateral epicondyle and terminating at Gerdy’s tubercle. The iliotibial band is incised in line with its fibers. For extensive articular comminution, the standard approach can be extended into a "Swashbuckler" approach, elevating the vastus lateralis from the lateral intermuscular septum and reflecting it anteriorly to expose the entire anterior and lateral distal femur. Meticulous handling of the soft tissues is paramount; the periosteum must not be stripped from the metaphyseal fragments, as preserving this biological envelope is critical for secondary bone healing.

Anatomical Articular Reduction: The Foundation
The articular block must be reconstructed first, converting a complex Type C fracture into a simpler Type A pattern. The joint capsule is opened, and fracture hematoma is meticulously evacuated to allow direct visualization of the chondral surfaces. Provisional fixation is achieved using multiple smooth K-wires, deployed strategically to avoid the planned paths of definitive lag screws. If a coronal plane Hoffa fragment is present, it is reduced and compressed using anterior-to-posterior headless compression screws, countersunk beneath the articular cartilage. The intercondylar split is then reduced using a large pointed reduction forceps and secured with independent 3.5mm or 4.5mm cortical lag screws, placed anterior or posterior to the intended footprint of the lateral plate.
Metaphyseal and Diaphyseal Reduction Strategies
Once the articular block is solidly reconstructed, the focus shifts to restoring limb length, axial alignment, and rotation. This is the most technically demanding phase of the operation. The surgeon must resist the urge to anatomically reduce the comminuted metaphyseal fragments, as doing so requires devascularizing soft tissue stripping. Instead, indirect reduction techniques are employed. A femoral distractor or an articulated tension device can be applied between the intact diaphysis and the reconstructed condylar block to restore length. Schanz pins, placed percutaneously into the proximal and distal segments, serve as powerful joysticks to correct varus/valgus and rotational deformities under fluoroscopic guidance.

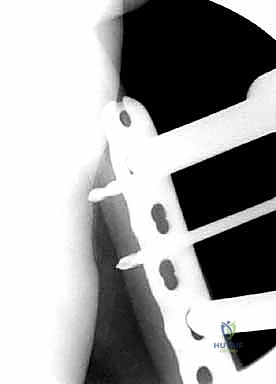
Plate Application and Biomechanical Fixation
With alignment restored, a pre-contoured distal femur locking plate is introduced. Using a MIPO technique, the plate is slid submuscularly along the lateral cortex, deep to the vastus lateralis. The trapezoidal geometry of the distal femur dictates that the plate must sit on the anterior half of the lateral condyle; placing it too posteriorly will drive the distal segment into internal rotation and valgus. The plate is provisionally secured with K-wires. Distally, a dense cluster of locking screws is placed to secure the articular block. Proximally, the fixation strategy shifts to relative stability. The surgeon must optimize the "working length" of the plate—leaving several screw holes empty over the fracture site to allow for micromotion and stimulate callus formation. A combination of locking and non-locking screws is used in the diaphysis to achieve a construct that is strong enough to bear loads but flexible enough to promote enchondral healing.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, distal femur fractures are plagued by high complication rates, necessitating vigilant post-operative monitoring and a readiness to employ salvage procedures. Nonunion and implant failure remain significant challenges, occurring in up to 15-20% of cases, particularly in the elderly and diabetic populations. Biomechanically, nonunions often result from a construct that is either too rigid (suppressing callus formation) or too flexible (leading to fatigue failure of the plate). Asymmetric callus formation, driven by the inherent stiffness of lateral locked plates, frequently leads to medial cortex failure. Management of aseptic nonunion typically requires hardware removal, debridement of the nonunion site, application of bone graft (autograft or orthobiologics), and revision fixation, often utilizing dual plating (medial and lateral) to increase construct stability.
Malunion is another critical complication, most commonly manifesting as varus collapse or apex-posterior bowing. Varus collapse is driven by the unopposed pull of the adductor magnus and is exacerbated if medial column comminution is not adequately supported. Rotational malunions, often subtle on plain radiographs, can dramatically alter patellofemoral tracking and knee kinematics. Salvage of a symptomatic malunion requires a corrective osteotomy, precise realignment using 3D-printed patient-specific guides, and rigid internal fixation. The consequences of untreated malunion include accelerated, asymmetric joint wear and early-onset osteoarthritis.

Infection and severe wound complications are catastrophic events in distal femur ORIF. Risk factors include obesity, diabetes, smoking, and the presence of an open fracture. Deep infections presenting acutely require urgent irrigation and debridement, retention of stable hardware, and targeted intravenous antibiotics. Chronic or late-onset infections often necessitate complete hardware explantation, placement of antibiotic-impregnated cement spacers, and a staged reconstruction once the infection is eradicated. In cases of severe articular destruction combined with infection or profound bone loss, salvage may ultimately require a distal femoral replacement (megaprosthesis) or, in extreme cases, above-knee amputation.
| Complication | Incidence Rate | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Aseptic Nonunion | 10% - 20% | Construct too rigid (inadequate working length), smoking, devascularization. | Hardware exchange, autologous bone grafting, addition of medial plate. |
| Varus Malunion | 5% - 15% | Failure to support medial column, adductor pull, improper plate contouring. | Corrective closing/opening wedge osteotomy, revision ORIF. |
| Deep Infection | 3% - 8% | Open fractures, prolonged operative time, severe soft tissue stripping, diabetes. | Aggressive I&D, suppressive antibiotics, potential hardware removal/spacer. |
| Post-Traumatic OA | 20% - 40% | Inadequate articular reduction, cartilage necrosis from initial impact. | Delayed Total Knee Arthroplasty (TKA) or Distal Femoral Replacement. |
Phased Post-Operative Rehabilitation Protocols
The surgical procedure is only the first half of the battle; rigorous, phased rehabilitation is mandatory to optimize clinical outcomes and prevent debilitating arthrofibrosis. Phase I (0-2 weeks post-operatively) focuses on immediate edema control, pain management, and the initiation of early, protected motion. The knee is highly susceptible to stiffness due to quadriceps tethering and capsular scarring. We advocate for the immediate use of a Continuous Passive Motion (CPM) machine or active-assisted Range of Motion (ROM) exercises, aiming for 0 to 90 degrees of flexion. Weight-bearing is strictly restricted during this phase, typically limited to Non-Weight Bearing (NWB) or Toe-Touch Weight Bearing (TTWB) to protect the articular reduction and the metaphyseal hardware construct.

Phase II (2-6 weeks) emphasizes the progression of ROM and the prevention of patellar contracture. Aggressive patellar mobilization techniques are instituted to prevent the patellar tendon from scarring down to the anterior tibia and femur. The goal by the end of week six is to achieve full terminal extension (0 degrees) and at least 110 degrees of flexion. Quadriceps activation is critical; isometric quadriceps sets and straight leg raises are performed daily. Weight-bearing status remains restricted, as the biological healing of the metaphyseal segment is still in its infancy, and premature loading can lead to catastrophic hardware failure.

Phase III (6-12 weeks) is dictated by radiographic evidence of clinical healing. At the 6-week mark, orthogonal radiographs are scrutinized for the presence of bridging callus in the metaphysis and maintenance of the articular reduction. If callus is evident, the patient is transitioned to a progressive weight-bearing protocol, increasing load by 25% increments weekly. Closed kinetic chain exercises, such as partial wall squats and leg presses, are introduced to stimulate further bone healing through controlled axial compression (Wolff's Law). Proprioceptive training and stationary cycling are also incorporated to restore neuromuscular control.

Phase IV (12+ weeks) represents the transition to advanced strengthening and return to functional activities. Full weight-bearing is expected, and the focus shifts to resolving residual muscle atrophy and maximizing dynamic stability. Advanced plyometrics, agility drills, and sport-specific training are customized to the patient's baseline functional demand. It is imperative during this phase to manage patient expectations; maximum medical improvement following a complex distal femur fracture may take up to 18 to 24 months, and a permanent, mild deficit in terminal flexion is a common, acceptable outcome.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of distal femur fractures is deeply rooted in evolving biomechanical research and landmark clinical trials. The evolution from conventional plating to locked plating systems (e.g., the Less Invasive Stabilization System - LISS) represented a paradigm shift, drastically reducing the rates of primary fixation failure in osteoporotic bone. However, subsequent literature highlighted a new complication: the "too stiff" construct. Landmark biomechanical studies by Bottlang et al. demonstrated that standard locked plates often suppress interfragmentary motion on the near cortex, leading to asymmetric, deficient callus formation. This led to the development of "Far Cortical Locking" (FCL) screws and dynamic locking plates, which allow for controlled, parallel micromotion at the fracture site, significantly enhancing secondary bone healing.

The debate regarding the management of medial column comminution has also generated substantial literature. Single lateral locked plates, while standard, exhibit a high failure rate in the presence of severe medial cortical defects (OTA 33-A3 and C3). Recent multi-center retrospective reviews have strongly advocated for the addition of a medial supplemental plate (dual plating) in these high-risk scenarios. Biomechanical studies confirm that dual plating significantly increases the load to failure and torsional rigidity of the construct, effectively neutralizing the varus deforming forces of the adductor complex and mitigating the risk of lateral plate fatigue failure.

For extra-articular (Type A) distal femur fractures, the literature continues to compare retrograde intramedullary nailing against lateral locked plating. Several meta-analyses have demonstrated that retrograde nailing offers biomechanical advantages as a load-sharing
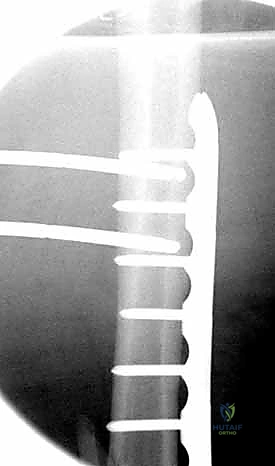
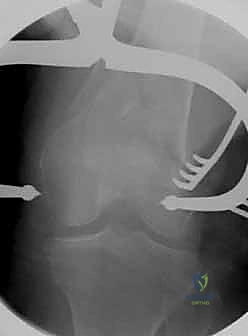
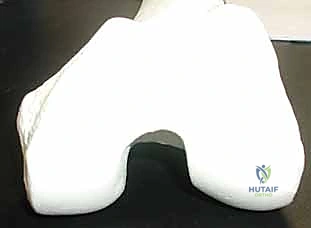
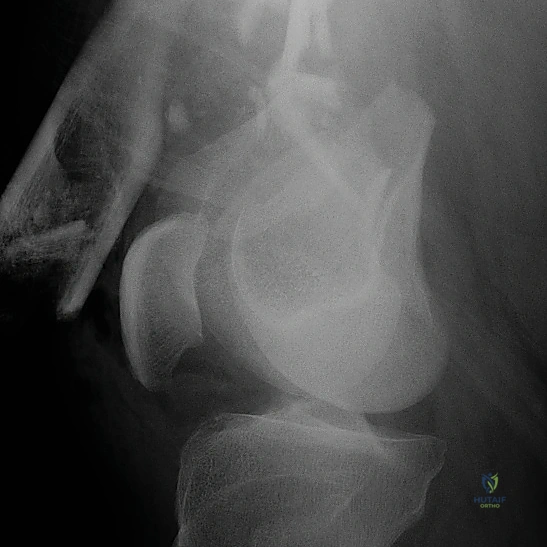
Clinical & Radiographic Imaging Archive