

Comprehensive Introduction and Patho-Epidemiology
Chronic Achilles tendinopathy represents one of the most pervasive and recalcitrant pathologies encountered in orthopedic foot and ankle surgery. Historically and erroneously termed "tendinitis," this condition is rarely an acute inflammatory event. Instead, it is a complex, progressive degenerative process—a failed healing response characterized fundamentally by angiofibroblastic hyperplasia, mucoid degeneration, and a profound disorganization of the collagen matrix. When this degenerative cascade becomes refractory to exhaustive conservative measures, surgical intervention transitions from an elective consideration to a mechanical necessity. We typically consider surgical debridement and repair only after a minimum of three to six months of a meticulously structured non-operative regimen has failed to yield symptomatic relief or functional restoration.
The epidemiology of Achilles tendinopathy is bimodal and diverse, affecting both high-demand elite athletes and sedentary middle-aged individuals. In the athletic population, particularly runners and jumping athletes, the pathology is driven by repetitive microtrauma that outpaces the tendon's intrinsic reparative capacity. Conversely, in the sedentary population, intrinsic factors such as advancing age, metabolic syndrome, obesity, and the use of certain pharmaceuticals (notably fluoroquinolone antibiotics and systemic corticosteroids) precipitate tenocyte apoptosis and matrix degradation. We have routinely observed that patients with long-standing, multi-year tendinopathy present with significantly poorer tissue quality, necessitating more extensive intraoperative debridement and inherently carrying a higher risk of postoperative complications and reoperation.
At the cellular and molecular level, the tendinopathic Achilles tendon is a hostile environment. Normal Achilles tendon tissue is composed predominantly of highly organized Type I collagen parallel bundles. In the tendinopathic state, we see a pathological shift toward Type III collagen, which is mechanically inferior and structurally disorganized. Furthermore, there is an upregulation of matrix metalloproteinases (MMPs) and an influx of haphazard, non-functional neovascularization accompanied by nociceptive nerve fibers—the primary drivers of the patient's chronic pain. For today's masterclass, we are focusing explicitly on non-insertional tendinopathy, localized to the main body of the tendon approximately 2 to 6 cm proximal to its calcaneal insertion. Open debridement, excision of the fibrotic paratenon, and restoration of a healthy biological milieu remain the gold standard for these recalcitrant cases.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, a profound, three-dimensional understanding of the posterior ankle anatomy is non-negotiable. This anatomical roadmap is your primary safeguard against devastating iatrogenic complications. The Achilles tendon is the thickest, strongest, and arguably the most mechanically stressed tendon in the human body, serving as the confluent aponeurosis of the triceps surae muscle group.
The Triceps Surae Complex and Tendon Architecture
The triceps surae comprises the two heads of the gastrocnemius and the underlying soleus muscle. The gastrocnemius, crossing both the knee and ankle joints, is primarily responsible for rapid, explosive plantarflexion. Its fibers transition into a broad aponeurosis at the mid-calf. The soleus, originating below the knee, is a postural muscle composed largely of slow-twitch fibers. Its tendon merges with the deep surface of the gastrocnemius aponeurosis to form the Achilles tendon proper. The soleus muscle fibers continue to insert into the anterior surface of the Achilles tendon throughout much of its proximal length, contributing significantly to its bulk and cross-sectional area.
The Achilles tendon itself measures approximately 15 cm in length. A critical biomechanical feature is the 90-degree spiral twist of its fibers as they descend from proximal to distal. The fibers originating from the medial gastrocnemius rotate to insert posteriorly on the calcaneus, while the lateral fibers rotate to insert anteriorly. This spiraling architecture enhances the tendon's ability to store and release elastic energy during locomotion; however, it also generates significant internal shear stresses, particularly in the mid-substance, predisposing this specific region to microtearing and subsequent degeneration.
Neurovascular Topography and the Watershed Zone
The neurovascular relationships dictate our surgical approach. The sural nerve, a purely sensory branch formed by contributions from the tibial and common fibular nerves, is the structure most at risk. It descends superficially along the posterolateral aspect of the calf, piercing the deep fascia approximately 10 cm proximal to the lateral malleolus. Crucially, in the operative zone of the mid-substance Achilles, the sural nerve and its accompanying short saphenous vein lie strictly posterolateral to the tendon. An incision placed directly posterior or posterolateral places these structures in the direct line of fire, risking painful neuroma formation, complex regional pain syndrome, and venous lymphatic disruption.
The blood supply to the Achilles tendon is another critical factor in the pathogenesis of tendinopathy. The tendon receives perfusion from three primary sources: the musculotendinous junction proximally, the osteotendinous junction distally, and the paratenon via the mesotenon anteriorly. Angiographic studies have definitively demonstrated a relative "watershed" or hypovascular zone located 2 to 6 cm proximal to the calcaneal insertion. This region relies heavily on the diffusion of nutrients from the paratenon. When the paratenon becomes thickened and fibrotic (paratendinopathy), this tenuous blood supply is further compromised, accelerating intratendinous degeneration and impairing the healing response.
The Paratenon Sheath
Unlike tendons of the hand or foot that are enclosed in true synovial sheaths, the Achilles tendon is enveloped by a paratenon. This is a delicate, highly vascularized, multi-layered connective tissue sheath that functions as an elastic sleeve, allowing the tendon to glide smoothly against surrounding tissues with up to 1.5 cm of excursion. In chronic tendinopathy, the paratenon undergoes severe inflammatory and fibrotic changes, becoming thickened, scarred, and densely adherent to the underlying epitenon. This paratendinopathy not only restricts tendon excursion, causing mechanical pain, but also strangles the vascular supply to the underlying tendon body. Meticulous excision of this pathological tissue is a mandatory step in the surgical reconstruction.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of successful outcomes in Achilles tendinopathy surgery. The decision to proceed with open debridement must be based on a rigorous evaluation of the patient's clinical history, physical examination, imaging findings, and response to non-operative modalities.
| Category | Specific Parameters | Clinical Rationale |
|---|---|---|
| Absolute Indications | Failure of >6 months of conservative care (eccentric loading, shockwave, orthotics). | Exhaustion of biological healing potential requires mechanical debridement. |
| Progressive, debilitating pain interfering with ADLs or sport. | Quality of life impairment justifies surgical morbidity risk. | |
| MRI/US confirmed high-grade intratendinous mucoid degeneration or partial tearing. | Structural failure cannot be reversed without sharp excision of necrotic tissue. | |
| Relative Indications | Concomitant severe paratendinopathy with palpable, painful nodularity. | Excision of fibrotic paratenon restores glide and vascularity. |
| Professional or high-level athletes failing a shorter (3-month) conservative window. | Time-sensitive career demands may accelerate the surgical timeline. | |
| Absolute Contraindications | Active local or systemic infection. | High risk of deep space infection and catastrophic tendon necrosis. |
| Severe peripheral vascular disease (PVD) or uncontrolled diabetes mellitus. | Unacceptable risk of wound dehiscence, flap necrosis, and amputation. | |
| Poor soft tissue envelope (e.g., prior radiation, extensive scarring). | Inability to achieve primary, tension-free skin closure over the tendon. | |
| Relative Contraindications | Active smoking or nicotine use. | Significantly impairs microvascular perfusion; mandates preoperative cessation. |
| Unrealistic patient expectations or inability to comply with prolonged NWB rehab. | Postoperative non-compliance frequently leads to repair rupture or joint stiffness. |
The clinical decision-making process requires a frank discussion with the patient regarding the anticipated timeline for recovery. Patients must understand that open debridement is not a "quick fix." The biological maturation of the newly remodeling tendon tissue takes months, and a return to unrestricted, high-impact activities typically requires a minimum of 6 to 9 months. Operating on a patient who expects to run a marathon six weeks post-operatively is a setup for clinical failure and patient dissatisfaction.
Furthermore, we must meticulously evaluate the patient's medical comorbidities. The posterior heel has notoriously poor vascularity, and the skin flaps elevated during this procedure are highly susceptible to ischemia. Patients with uncontrolled diabetes, small vessel disease, or active tobacco use are at an exponentially higher risk for catastrophic wound complications. In our practice, we mandate a minimum of four weeks of strict smoking cessation prior to any elective Achilles tendon reconstruction, confirmed via serum cotinine testing if necessary.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning mitigates intraoperative surprises and optimizes the surgical workflow. This begins with a highly specific physical examination.
Advanced Clinical Evaluation
Our patient typically presents with localized pain 2 to 6 cm proximal to the insertion. On examination, we look for the classic "painful arc" sign. We ask the patient to actively dorsiflex and plantarflex the ankle while we palpate the nodule. In isolated paratendinopathy, the area of maximum thickening remains fixed relative to the malleoli. In true intratendinous tendinopathy, the nodule moves proximally and distally with tendon excursion. We also perform the Royal London Hospital test: tenderness to palpation of the Achilles tendon is elicited with the ankle in neutral, but this tenderness significantly decreases or disappears when the ankle is maximally dorsiflexed, as the tendon is placed under tension, blanching the neovessels.
Imaging Modalities
While the diagnosis is primarily clinical, imaging is critical for surgical mapping. Soft tissue radiographs are obtained to rule out insertional calcifications or a Haglund's deformity, which would necessitate a different surgical approach. High-resolution Ultrasound (US) is our first-line dynamic modality. It clearly delineates hypoechoic zones of degeneration, measures tendon thickness, and, crucially, utilizes color Doppler to identify the degree of pathological neovascularization.
Magnetic Resonance Imaging (MRI) is the definitive study for preoperative templating in complex cases. We scrutinize the axial and sagittal T1 and T2-weighted sequences. Tendinosis appears as fusiform thickening with intermediate signal intensity on T1 and high signal intensity on T2, representing mucoid degeneration and interstitial tearing. The MRI allows us to quantify the percentage of cross-sectional area involved. If the MRI indicates that more than 50% of the tendon is severely degenerated, we must preoperatively consent the patient for, and prepare for, a tendon augmentation procedure, such as a Flexor Hallucis Longus (FHL) transfer or a V-Y fascial advancement.

Operating Room Setup and Positioning
Optimization of the surgical field is paramount. The patient is placed in the prone position. We utilize general anesthesia or a robust regional neuraxial block (spinal/epidural) combined with deep sedation. The prone position allows for simultaneous, bilateral comparison of tendon tension and provides unobstructed, direct access to the posterior compartment of the leg.
The ankles must be positioned completely clear of the operating table edge, allowing for unrestricted, full intraoperative range of motion. This is critical for assessing tendon tension after repair and for the application of the postoperative splint. Soft gel bolsters are placed under the shins and the anterior chest to prevent pressure necrosis and facilitate ventilation. A pneumatic tourniquet is applied high on the proximal thigh. Following strict sterile prep and drape, the limb is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250-300 mmHg. A bloodless field is absolutely essential; attempting to identify subtle pathological tissue changes in a bloody field is an exercise in futility and compromises the surgical outcome.
Step-by-Step Surgical Approach and Fixation Technique
We are now scrubbed, the patient is prepped, and the tourniquet is inflated. The execution of this procedure demands meticulous tissue handling and a deep respect for the fragile soft tissue envelope of the posterior ankle.
Incision and Flap Elevation
The surgical approach dictates the safety of the soft tissue envelope. We utilize a longitudinal incision, approximately 8 to 12 cm in length, placed strictly medial to the palpable medial border of the Achilles tendon. This medial placement is a deliberate, calculated maneuver to maximize the distance from the sural nerve and short saphenous vein, which reside posterolaterally. A direct posterior incision is strongly discouraged, as it places the resulting scar directly over the tendon, leading to severe shoe-wear irritation and adherence.

Using a #10 scalpel, the skin is incised. The most critical technical pearl of this exposure is the creation of full-thickness fasciocutaneous flaps. We do not dissect in the subcutaneous plane. Instead, we carry the dissection sharply down to the superficial fascia of the paratenon. The skin and subcutaneous fat must be elevated as a single, robust unit. Thinning the skin flaps by dissecting superficially will invariably lead to marginal skin necrosis, wound dehiscence, and potentially devastating deep infection. Retraction should be gentle, utilizing blunt retractors (e.g., Senn or Army-Navy) rather than self-retaining retractors that can cause ischemic crush injury to the skin edges.
Paratenon Management
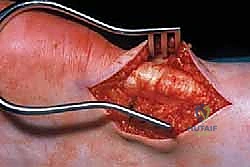
As the full-thickness flaps are retracted, the paratenon comes into view. In the healthy state, it is a thin, translucent, gliding layer. In our chronic tendinopathy patient, it will appear as a thickened, opaque, hypervascular, and densely fibrotic rind encasing the tendon.
Using fine Metzenbaum scissors or a #15 blade, a longitudinal incision is made through the paratenon, directly in the midline of the underlying tendon. We then carefully dissect the paratenon away from the epitenon. In areas of severe paratendinopathy, the tissue will be firmly adherent. We perform a thorough, sharp excision of all thickened, pathological paratenon tissue, particularly anteriorly where it tethers the tendon to the deep fascia (Kager's fat pad). This release is vital to restore normal tendon excursion and remove the source of constrictive ischemia.
Intratendinous Debridement
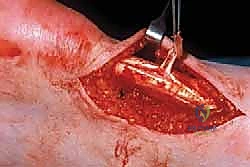
With the paratenon excised, the main body of the Achilles tendon is fully exposed. We visually and palpably inspect the tendon. Healthy tendon is firm, pearly white, and exhibits tightly packed longitudinal striations. Pathological tissue is visually distinct: it is dull, gray or yellowish, lacks normal striations, and feels soft, boggy, and nodular.

We make one or more longitudinal tenotomies directly into the areas of maximal nodularity and thickening. As we open the tendon, the degenerated tissue often extrudes. It has a characteristic granular, disorganized, and friable appearance, universally described in the literature as "crabmeat." Using a fresh #15 blade, a scalpel, or a sharp curette, we aggressively but precisely excise all macroscopic "crabmeat" tissue.

The debridement must be carried down to healthy, bleeding, firm tendon margins. Do not leave necrotic tissue behind, as it will act as a nidus for continued pain and failed healing. Once the macroscopic disease is removed, we perform multiple longitudinal fenestrations (micro-tenotomies) in the remaining healthy tendon. These parallel cuts, spaced a few millimeters apart, decompress the tendon, disrupt any microscopic zones of degeneration, and crucially, stimulate a profound neovascularization and cellular healing response from the viable tenocytes.

Defect Management and Reconstruction
Following exhaustive debridement, we must assess the structural integrity of the remaining tendon. The management strategy is dictated by the volume of tissue resected.
If less than 50% of the cross-sectional area of the tendon has been resected, the tendon can usually be reconstructed primarily. We perform a side-to-side tubularization repair. Using a heavy, absorbable monofilament or braided suture (e.g., 0-Vicryl or 2-0 FiberWire), we approximate the medial and lateral edges of the healthy tendon over the defect. This buries the raw, debrided surfaces, reduces the bulk of the tendon, and restores a smooth, cylindrical contour that facilitates gliding.

If the debridement was massive, resulting in the loss of greater than 50% of the tendon's cross-sectional area, primary tubularization is insufficient and places the patient at high risk for postoperative rupture. In these scenarios, we must augment the repair. The gold standard for augmentation in this setting is the transfer of the Flexor Hallucis Longus (FHL) tendon. The FHL is harvested, passed through a transverse drill hole in the calcaneus or secured with an interference screw, and interwoven into the remaining Achilles tendon. This provides robust, in-phase vascularized tissue to bridge the defect and offload the compromised Achilles.
Closure is performed meticulously. If any healthy paratenon remains, it is loosely approximated over the tendon to provide a gliding layer. The subcutaneous tissue is closed with buried interrupted 2-0 or 3-0 absorbable sutures to take all tension off the skin edges. The skin is closed with a non-absorbable monofilament (e.g., 3-0 nylon or Prolene) using a vertical mattress technique to ensure edge eversion and optimize vascularity.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, surgery on the Achilles tendon carries a distinct and unforgiving complication profile. The posterior heel is a high-tension, poorly vascularized environment, and complications here can rapidly cascade into limb-threatening scenarios.
| Complication | Estimated Incidence | Etiology & Pathogenesis | Salvage / Management Strategy |
|---|---|---|---|
| Superficial Wound Dehiscence | 5% - 10% | Thin skin flaps, excessive retraction, premature suture removal, smoking. | Local wound care, strict immobilization, oral antibiotics if cellulitis is present. Secondary intention healing. |
| Deep Infection / Necrosis | 1% - 3% | Progression of superficial dehiscence, hematoma formation, diabetic microangiopathy. | Aggressive operative I&D, vacuum-assisted closure (VAC), possible free tissue transfer (e.g., ALT flap) for coverage. |
| Sural Nerve Injury/Neuroma | 2% - 5% | Iatrogenic transection or traction injury during lateral/posterior approaches. | Gabapentinoids, diagnostic blocks. If refractory, surgical excision of neuroma and burying the stump into muscle. |
| Post-operative Tendon Rupture | 1% - 4% | Over-aggressive debridement without augmentation, patient non-compliance with NWB protocol. | Revision surgery with robust augmentation (FHL transfer, V-Y turn-down flap, or allograft reconstruction). |
| Deep Vein Thrombosis (DVT) | 1% - 2% | Prolonged prone positioning, tourniquet use, postoperative cast immobilization. | Chemical prophylaxis (LMWH or DOACs) in high-risk patients. Therapeutic anticoagulation upon diagnosis. |
The most feared complication is profound wound breakdown leading to exposed tendon or deep infection. This is precisely why we emphasize thick, full-thickness flaps and strict medial incision placement. If a deep infection occurs, the necrotic tendon must be aggressively debrided, often leaving a massive gap. Salvage in these catastrophic cases requires a multidisciplinary approach, frequently involving plastic surgery for free tissue transfer (such as an anterolateral thigh flap) to provide a vascularized soft tissue envelope, followed by staged tendon reconstruction using allograft or autograft options once the infection is eradicated.
Sural nerve injuries, while less limb-threatening, are highly morbid for the patient, resulting in chronic, debilitating neuropathic pain along the lateral border of the foot. Prevention via anatomical knowledge and medial incision placement is the only reliable cure. If a neuroma forms, conservative management with targeted nerve blocks and desensitization is attempted, but surgical excision and proximal burying of the nerve stump into the deep muscle belly is often required.
Phased Post-Operative Rehabilitation Protocols
The surgical procedure is only fifty percent of the cure; a rigid, phased, and biologically respectful rehabilitation protocol constitutes the remaining fifty percent. The goal is to protect the healing tissue during the vulnerable inflammatory and early proliferative phases, while gradually introducing controlled mechanical stress to stimulate parallel collagen alignment and maturation.
Phase 1: Maximum Protection (Weeks 0 to 2)
Immediately postoperatively, the patient is placed in a well-padded, short-leg plaster or fiberglass splint with the ankle immobilized in 15 to 20 degrees of equinus (plantarflexion). This position maximally offloads the repaired tendon and the posterior skin incision, preventing tension-induced ischemia. The patient is strictly Non-Weight Bearing (NWB) on crutches or a knee scooter. Elevation of the limb above the level of the heart is mandated to minimize edema and hematoma formation. Sutures are typically removed at 14 to 21 days, only when the incision is completely sealed and dry.
Phase 2: Controlled Mobilization (Weeks 2 to 6)
Once the wound is healed, the patient is transitioned to a rigid Controlled Ankle Motion (CAM) walker boot fitted with a multi-layered heel lift (usually 2 to 3 cm). The patient remains NWB for an additional week, then gradually initiates Touch-Down Weight Bearing (TDWB), progressing to Partial Weight Bearing (PWB) as tolerated. During this phase, the patient is instructed to remove the boot multiple times daily to perform active, non-resistance range of motion (ROM) exercises, strictly limiting dorsiflexion to neutral (0 degrees) to protect the repair.
Phase 3: Early Strengthening (Weeks 6 to 12)
By week six, biological healing has progressed to the remodeling phase. The heel wedges in the CAM boot are sequentially removed (one layer every 1-2 weeks) until the foot is flat in the boot. The patient transitions to Full Weight Bearing (FWB). Physical therapy aggressively targets triceps surae strengthening, initially with isometric exercises, progressing to concentric loading. Proprioceptive training (e.g., BAPS board, single-leg stance) is initiated. Toward the end of this phase, the patient is transitioned out of the boot into a supportive athletic shoe with a small silicone heel cup.
Phase 4: Advanced Function and Return to Sport (Months 3 to 6+)
This final phase focuses on the restoration of explosive power, endurance, and sport-specific mechanics. We re-introduce the cornerstone of non-operative care: eccentric loading protocols (e.g., the Alfredson protocol), which are now safe to perform and critical for final collagen maturation. Plyometric exercises, agility drills, and a graduated return-to-run program are implemented. Clearance for full, unrestricted athletic competition is granted only when the patient demonstrates symmetrical ankle ROM, no pain with single-leg heel raises, and isokinetic strength testing reveals at least 90% strength compared to the contralateral uninjured limb. This milestone is rarely achieved before 6 months post-operatively.
Summary of Landmark Literature and Clinical Guidelines
The evolution of our understanding and management of Achilles tendinopathy is heavily rooted in landmark clinical literature. The paradigm shift from viewing this condition as an inflammatory "tendinitis" to a degenerative "tendinosis" was championed by the histological studies of Puddu et al
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding open-management-of-achilles-tendinopathy