Achilles Tendon Lengthening: An Open Sliding Masterclass

Key Takeaway
Join us in the OR for an immersive masterclass on open sliding Achilles tendon lengthening. We'll meticulously cover patient selection, detailed anatomy, precise surgical steps for equinus correction, and crucial intraoperative pearls. Learn to navigate neurovascular structures, achieve optimal dorsiflexion, and manage potential complications for successful patient outcomes. This guide ensures comprehensive understanding from incision to postoperative care.
Comprehensive Introduction and Patho-Epidemiology
Equinus deformity represents one of the most pervasive and biomechanically devastating conditions encountered in both pediatric and adult reconstructive orthopedic surgery. Defined strictly as a condition in which the ankle is restricted from dorsiflexing beyond a neutral (zero-degree) position with the hindfoot in a neutral alignment, equinus forces the patient to bear weight predominantly on the metatarsal heads. This seemingly isolated sagittal plane deformity triggers a cascade of compensatory kinematic deviations throughout the entire lower extremity kinetic chain. Uncorrected equinus invariably leads to midfoot breaching, hindfoot valgus or varus, knee hyperextension (genu recurvatum), and profound alterations in pelvic tilt and lumbar lordosis, fundamentally destroying the efficiency of the human gait cycle.
The patho-epidemiology of equinus is broadly categorized into congenital, developmental, and acquired etiologies, each dictating a nuanced approach to surgical management. Congenital equinus is a hallmark of complex foot deformities such as idiopathic clubfoot (talipes equinovarus) and congenital vertical talus. In these scenarios, the contracture is often rigid and associated with profound dysplasia of the talocrural and subtalar articulations. Acquired equinus, conversely, is frequently the sequela of upper motor neuron lesions, most notably cerebral palsy (CP), traumatic brain injury, or cerebrovascular accidents. In the spastic patient, the initial deformity is dynamic—driven by velocity-dependent overactivity of the triceps surae—but inevitably transitions into a rigid, myostatic contracture characterized by a reduction in serial sarcomeres and an increase in fibrotic, non-compliant connective tissue within the muscle belly and tendon.
Beyond neurologic etiologies, orthopedic surgeons must be acutely aware of post-traumatic and iatrogenic causes of equinus. Severe lower extremity burns often result in dense, unyielding posterior scar contractures that tether the calcaneus in plantarflexion. Similarly, prolonged immobilization in a plantarflexed position following tibial or foot trauma can induce rapid shortening of the gastrocsoleus complex. Idiopathic toe walking, while often resolving spontaneously in early childhood, can persist and result in a structural equinus requiring operative intervention in adolescence. Recognizing the underlying etiology is not merely an academic exercise; it fundamentally alters the surgical algorithm, dictating whether an isolated gastrocnemius recession, a sliding Achilles lengthening, or a more radical Z-lengthening is warranted.
A critical distinction must be made preoperatively between a dynamic deformity and a rigid, fixed myostatic contracture. Dynamic equinus, which corrects under anesthesia or with the administration of paralytic agents, is often amenable to conservative measures such as botulinum toxin injections, serial casting, or targeted orthotic management. However, once the deformity becomes fixed—meaning passive dorsiflexion is impossible even when spasticity is eliminated—surgical lengthening becomes the mandatory standard of care. The open sliding Achilles tendon lengthening, the focus of this masterclass, is a powerful, reliable technique designed specifically to address fixed equinus that significantly impairs ambulation, skin integrity, and overall quality of life.
Detailed Surgical Anatomy and Biomechanics
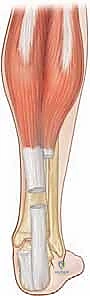
A profound, three-dimensional understanding of the triceps surae and its tendinous insertion is the absolute foundation of a successful open sliding Achilles lengthening. The triceps surae is a composite structure comprising the gastrocnemius and the soleus muscles, which, despite sharing a common distal insertion, possess vastly different origins, fiber types, and biomechanical functions. The gastrocnemius is a biarticular muscle, originating from the posterior aspects of the medial and lateral femoral condyles. Composed predominantly of Type II fast-twitch muscle fibers, it functions primarily as a powerful plantarflexor during the propulsive phase of gait and assists in knee flexion. Because it crosses both the knee and the ankle, the tension within the gastrocnemius is highly dependent on knee position—a physiological reality that forms the basis of the Silfverskiöld test.

Lying deep to the gastrocnemius is the soleus muscle, a uniarticular powerhouse originating from the posterior tibia, the fibular head, and the interosseous membrane. The soleus is composed predominantly of Type I slow-twitch, fatigue-resistant muscle fibers, reflecting its critical role as a postural stabilizer. It acts continuously during the stance phase of gait to decelerate the forward progression of the tibia over the fixed foot, a mechanism known as the plantarflexion-knee extension couple. Because the soleus does not cross the knee joint, its tension is independent of knee flexion or extension. The aponeuroses of these two distinct muscles coalesce in the mid-to-distal calf to form the Achilles tendon, the thickest and strongest tendon in the human body, capable of withstanding loads up to ten times body weight during vigorous activity.
The most critical anatomical feature of the Achilles tendon, and the precise reason the sliding lengthening technique is possible, is its complex internal rotation as it descends toward the calcaneus. The tendon undergoes a 90-degree internal (lateral) rotation. Consequently, the fibers originating from the medial gastrocnemius, which begin medially, rotate to insert on the posterior and lateral aspect of the calcaneal tuberosity. Conversely, the fibers originating from the soleus, which begin deep and anterior, rotate to insert on the medial aspect of the calcaneus.

This spiraling architecture can be easily conceptualized by crossing your index and middle fingers. When performing an open sliding lengthening, we exploit this rotation by making a proximal cut in the medial aspect of the tendon (predominantly releasing soleus fibers) and a distal cut in the anterior or lateral aspect (predominantly releasing gastrocnemius fibers). When the ankle is forcibly dorsiflexed, the intact fibers slide past one another, elongating the tendon while maintaining structural continuity.
Neurovascular considerations in this region are paramount to avoiding catastrophic iatrogenic injury. The sural nerve, a purely sensory branch formed by contributions from the tibial and common peroneal nerves, courses subcutaneously down the posterior calf. It typically runs lateral to the Achilles tendon in the distal third of the leg, supplying sensation to the lateral hindfoot and midfoot. While an anteromedial surgical incision minimizes the risk to the sural nerve, aberrant anatomy or overly aggressive lateral dissection can lead to nerve transection or painful neuroma formation. Furthermore, the blood supply to the Achilles tendon is notoriously tenuous. The tendon receives vascular contributions proximally from the muscle bellies and distally from the osteotendinous junction. However, the critical mid-substance "watershed zone," located 2 to 6 centimeters proximal to the insertion, relies almost entirely on the extrinsic vascularity provided by the paratenon. The paratenon is a highly vascularized, loose connective tissue sheath supplied primarily by branches of the posterior tibial artery. Meticulous preservation of this paratenon during surgical dissection is non-negotiable, as devascularization will inevitably lead to delayed healing, wound breakdown, or frank tendon rupture.
Exhaustive Indications and Contraindications
The decision to proceed with an open sliding Achilles tendon lengthening must be based on a rigorous evaluation of the patient's functional status, the chronicity of the deformity, and the presence of concurrent musculoskeletal pathology. The primary indication is a rigid, fixed equinus contracture that fails to respond to a comprehensive regimen of conservative management, including physical therapy, serial casting, orthotic bracing (Ankle-Foot Orthoses), and targeted chemodenervation (Botulinum toxin A). In the ambulatory patient, surgical intervention is indicated when the equinus deformity causes significant kinematic deviations, such as a persistent toe-walking gait, early heel rise during the stance phase, or the development of a compensatory genu recurvatum (knee hyperextension) to achieve plantigrade foot contact.
In the non-ambulatory patient, particularly those with severe, total-body involvement cerebral palsy (GMFCS Level IV or V), the indications shift from optimizing gait kinematics to facilitating nursing care, improving seating posture in a wheelchair, and preventing painful skin breakdown over the metatarsal heads or the anterior talus. A fixed equinus in a non-ambulatory patient often forces the foot off the wheelchair footplates, leading to progressive midfoot breakdown and severe pressure ulcerations. In these scenarios, achieving a plantigrade foot through an Achilles lengthening is a crucial quality-of-life intervention, even if independent ambulation is not the ultimate goal.
However, the contraindications to Achilles lengthening are equally, if not more, important to recognize, as inappropriate surgical intervention can lead to devastating, irreversible complications. The most absolute contraindication is a purely dynamic equinus deformity. If the ankle can be passively dorsiflexed to neutral when the patient is relaxed or under anesthesia, lengthening the tendon will inevitably result in a catastrophic over-lengthening. Over-lengthening destroys the plantarflexion-knee extension couple, rendering the soleus incapable of decelerating the tibia during stance. This forces the patient into a debilitating "crouch gait," characterized by excessive ankle dorsiflexion, knee flexion, and hip flexion, which is exponentially more energy-demanding and functionally limiting than the original equinus deformity.
Furthermore, an isolated Achilles lengthening is contraindicated if the equinus is primarily driven by a fixed bony block rather than soft tissue contracture. Anterior talar neck osteophytes, a flattened talar dome, or a malunited tibial fracture can mechanically restrict dorsiflexion. In such cases, soft tissue lengthening will fail to correct the deformity and may simply destabilize the hindfoot. Finally, profound weakness of the triceps surae, often seen in conditions like poliomyelitis or certain muscular dystrophies, is a relative contraindication. Lengthening an already weak muscle-tendon unit will further compromise plantarflexion power, severely impairing the patient's ability to achieve push-off during the terminal stance phase of gait.
| Parameter | Indications for Open Sliding Achilles Lengthening | Contraindications / Relative Contraindications |
|---|---|---|
| Deformity Type | Rigid, fixed myostatic contracture | Purely dynamic deformity (corrects with relaxation/anesthesia) |
| Clinical Presentation | Persistent toe-walking, early heel rise, genu recurvatum | Crouch gait, calcaneal gait, profound triceps surae weakness |
| Conservative Tx | Failure of serial casting, AFOs, Botox injections | Responsive to conservative measures or chemodenervation |
| Anatomic Factors | Soft tissue contracture confirmed by Silfverskiöld test | Fixed bony block (e.g., anterior ankle impingement, osteophytes) |
| Non-Ambulatory | Difficulty with shoe wear, wheelchair positioning, skin breakdown | Severe vascular compromise or active posterior ankle infection |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the absolute cornerstone of a successful Achilles tendon lengthening. The evaluation begins with a meticulous history, focusing on perinatal events, developmental milestones, and the progression of the deformity. In acquired cases, detailing previous trauma, periods of immobilization, or the presence of progressive neuromuscular disorders is critical. The physical examination must encompass the entire lower extremity kinetic chain, as equinus is rarely an isolated phenomenon. The surgeon must evaluate for concomitant hip flexion contractures, hamstring tightness, and torsional deformities of the femur and tibia, as addressing the ankle in isolation while ignoring proximal pathology will inevitably lead to suboptimal functional outcomes.
The most critical component of the physical examination is the Silfverskiöld test, which differentiates an isolated gastrocnemius contracture from a combined gastrocsoleus contracture. With the patient supine and the subtalar joint locked in neutral to prevent spurious dorsiflexion through the transverse tarsal joint (a midfoot break), the surgeon passively dorsiflexes the ankle with the knee fully extended. The degree of dorsiflexion is recorded. The knee is then flexed to 90 degrees, relaxing the biarticular gastrocnemius, and ankle dorsiflexion is reassessed. If ankle dorsiflexion improves significantly (typically >10 degrees) with knee flexion, the contracture is isolated to the gastrocnemius, and a gastrocnemius recession (e.g., Strayer or Baumann procedure) is indicated. If severe equinus persists regardless of knee position, the contracture involves the entire triceps surae complex, necessitating an Achilles tendon lengthening.
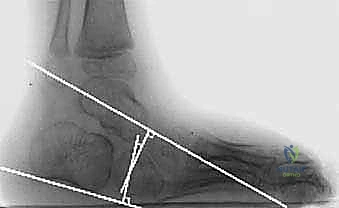
Instrumented three-dimensional gait analysis, when available, is the gold standard for preoperative planning, particularly in complex neuromuscular patients. Kinematic data will objectively quantify the degree of equinus throughout the gait cycle, while kinetic data will evaluate the power generated during push-off. Electromyography (EMG) can identify inappropriate, out-of-phase firing of the triceps surae or co-contraction of the anterior tibialis. Radiographic evaluation must include weight-bearing anteroposterior and lateral views of the foot and ankle. The surgeon must meticulously assess the lateral tibiocalcaneal angle, the lateral talocalcaneal angle, and Meary's angle to rule out midfoot breaching (rocker-bottom deformity) and to identify any osseous impingement at the anterior ankle joint that would preclude successful soft tissue lengthening.
Positioning in the operating room is dictated by the need for concomitant procedures. For an isolated Achilles lengthening, the patient is typically positioned supine. A pneumatic thigh tourniquet is applied to ensure a pristine, bloodless surgical field, which is essential for identifying the paratenon and avoiding iatrogenic injury to the sural nerve. The leg is prepped and draped freely to allow unrestricted manipulation of the knee and ankle. A sterile bump may be placed under the ipsilateral hip to internally rotate the leg, bringing the posteromedial aspect of the ankle into better view. If the patient requires simultaneous posterior procedures, such as hamstring lengthenings or posterior capsulotomies, the prone position is utilized. In the prone position, meticulous attention must be paid to padding all bony prominences, freeing the abdomen to prevent epidural venous engorgement, and ensuring the airway is secure and easily accessible by the anesthesia team.
Step-by-Step Surgical Approach and Fixation Technique
The open sliding Achilles tendon lengthening, heavily influenced by the principles described by White, is an elegant technique that achieves controlled elongation while preserving the continuity of the tendon. Following exsanguination and tourniquet inflation, a longitudinal incision is made over the posteromedial aspect of the distal leg. The incision typically begins 2 to 3 centimeters proximal to the calcaneal insertion and extends proximally for 5 to 7 centimeters, depending on the anticipated length of the slide. A posteromedial approach is strictly preferred over a direct posterior or posterolateral approach to minimize the risk of injury to the sural nerve and the short saphenous vein, and to avoid placing the surgical scar directly over the posterior shoe counter, which can lead to chronic irritation.
Sharp dissection is carried through the skin and subcutaneous tissue. Meticulous hemostasis is maintained. The surgeon will encounter the paratenon, a distinct, glistening, highly vascularized fascial layer investing the Achilles tendon. The paratenon must be incised longitudinally and carefully reflected off the underlying tendon. It is imperative to preserve the paratenon as a continuous sleeve, as it provides the primary extrinsic blood supply to the healing tendon. Excessive stripping or thermal necrosis from electrocautery in this region will inevitably lead to tendon desiccation, delayed healing, or catastrophic postoperative rupture.

Once the tendon is adequately exposed, the sliding lengthening is performed. The classic White technique involves two partial hemisections of the tendon. Understanding the 90-degree internal rotation of the tendon fibers is crucial here. The distal cut is made approximately 1 to 2 centimeters proximal to the calcaneal insertion. A scalpel is used to transversely divide the anterior two-thirds (or anterior half) of the tendon. Because of the internal rotation, these anterior fibers distally correspond to the gastrocnemius muscle.

The proximal cut is made 3 to 5 centimeters proximal to the distal cut. Here, the scalpel is used to transversely divide the medial two-thirds (or medial half) of the tendon. Proximally, these medial fibers correspond to the soleus muscle.

With the cuts completed, the surgeon firmly grasps the foot and forcefully dorsiflexes the ankle with the knee in full extension. The intact fibers of the tendon will slide past one another, allowing the tendon to elongate. The surgeon must carefully titrate the dorsiflexion force to achieve the desired correction—typically neutral or 5 degrees of dorsiflexion—without tearing the remaining intact fibers.

An alternative to the sliding technique is the open Z-lengthening, which is typically reserved for severe, rigid contractures where a slide will not yield sufficient length, or for revision cases. In a Z-lengthening, a complete longitudinal split is made down the center of the tendon, followed by a medial hemisection proximally and a lateral hemisection distally.

The tendon is allowed to elongate, and the overlapping ends are sutured together using a heavy, non-absorbable suture (e.g., #1 or #2 Ethibond) in a modified Kessler or Krackow configuration. While Z-lengthening offers precise control over the exact amount of lengthening, it completely disrupts the structural continuity of the tendon, requires robust suture fixation, and carries a higher risk of over-lengthening and postoperative rupture compared to the sliding technique.

Following the lengthening, regardless of the specific technique, the tourniquet is deflated, and meticulous hemostasis is achieved. Hematoma formation in this region is a primary driver of postoperative wound breakdown and infection. The paratenon is carefully reapproximated over the lengthened tendon using a fine, absorbable suture (e.g., 3-0 Vicryl). This step is critical for restoring the gliding layer and optimizing the vascular environment for tendon healing. The subcutaneous tissue is closed in layers, and the skin is reapproximated using a running subcuticular suture or interrupted nylon sutures, depending on the surgeon's preference and the quality of the surrounding soft tissue.
Complications, Incidence Rates, and Salvage Management
While the open sliding Achilles tendon lengthening is a highly effective procedure, it is fraught with potential complications that can severely compromise patient outcomes. The most devastating and feared complication is over-lengthening of the triceps surae. Over-lengthening fundamentally destroys the plantarflexion-knee extension couple, rendering the soleus incapable of stabilizing the tibia during the stance phase of gait. This results in a catastrophic "calcaneal gait" or "crouch gait," characterized by excessive ankle dorsiflexion, uncontrolled forward progression of the tibia, and compensatory knee and hip flexion. The patient loses all push-off power, and the energy expenditure of walking increases exponentially. Over-lengthening is notoriously difficult to salvage; it often requires complex tendon transfers (e.g., transferring the peroneus brevis or flexor hallucis longus to the calcaneus) or rigid bony stabilization (e.g., subtalar or triple arthrodesis), and the functional results of these salvage procedures are frequently disappointing.

Conversely, under-correction or recurrence of the equinus deformity is a common complication, particularly in the growing pediatric patient with spastic cerebral palsy. Recurrence rates in spastic populations can range from 15% to 30% over a five-year period. Recurrence is often driven by the underlying neurologic drive, failure to adhere to postoperative bracing protocols, or performing the surgery at too young an age (typically before age 6). Management of recurrent equinus requires a thorough re-evaluation; if the recurrence is rigid, a repeat lengthening, often necessitating a formal Z-lengthening due to altered anatomy and scarring, may be required.

Wound complications are a significant concern due to the tenuous vascularity of the posterior ankle skin and the high tension placed on the closure once the ankle is brought out of equinus. Superficial wound dehiscence or delayed healing occurs in approximately 5% to 10% of cases. Deep infection is less common (<2%) but is a surgical emergency that threatens the viability of the tendon. Meticulous surgical technique, preservation of the paratenon, absolute hemostasis, and avoiding excessive tension on the skin closure are paramount. If deep infection occurs, aggressive surgical debridement, targeted intravenous antibiotic therapy, and potentially negative pressure wound therapy are mandatory.
Iatrogenic injury to the sural nerve is a preventable but highly morbid complication. Entrapment, partial transection, or excessive traction on the nerve can lead to painful neuroma formation or debilitating
Clinical & Radiographic Imaging Archive