Femoral Head Fracture Fixation: An Intraoperative Masterclass

Key Takeaway
Welcome to this intraoperative masterclass on Open Reduction and Internal Fixation (ORIF) of femoral head fractures. We'll delve into comprehensive surgical anatomy, meticulous patient positioning, and step-by-step execution of the Smith-Peterson and Ganz surgical dislocation approaches. Expect detailed discussions on neurovascular risks, precise instrument use, and critical pearls to optimize outcomes and manage complications in these challenging high-energy injuries.
Comprehensive Introduction and Patho-Epidemiology
Femoral head fractures represent one of the most formidable and technically demanding injuries encountered in orthopaedic trauma surgery. Occurring almost exclusively in the setting of high-energy hip dislocations, these fractures are identified in approximately 5% to 15% of all traumatic hip dislocation events. The mechanism of injury typically involves a massive axial load transmitted through the femoral shaft to a flexed hip, classically seen in motor vehicle collisions as the "dashboard injury." When the hip is flexed and adducted, the femoral head is driven posteriorly against the firm rim of the acetabulum, resulting in a posterior dislocation with a shearing osteochondral fracture of the femoral head. Conversely, an abducted and externally rotated limb subjected to a similar force vector will typically yield an anterior dislocation with an associated impaction or shear fracture of the anterior femoral head.
The pathophysiology of these injuries extends far beyond the macroscopic osseous failure. The immense shear forces required to fracture the dense subchondral bone of the femoral head invariably inflict significant, often irreversible, damage to the delicate articular cartilage. This chondral injury, combined with the primary mechanical disruption of the osseous architecture, sets the stage for rapid, progressive post-traumatic osteoarthritis. Furthermore, the traumatic dislocation event violently stretches, tears, or avulses the capsuloligamentous structures, gravely threatening the tenuous extraosseous blood supply to the femoral head. Consequently, the orthopaedic surgeon is faced with a dual mandate: achieve absolute anatomic reduction of the articular surface to restore joint congruity, and meticulously preserve the residual vascularity to mitigate the devastating complication of osteonecrosis.
Epidemiologically, femoral head fractures disproportionately affect young, active individuals involved in high-velocity trauma. Because of the extreme energy required to produce this injury pattern, these patients frequently present as polytrauma victims with concomitant life-threatening head, thoracic, abdominal, or pelvic injuries. The orthopaedic management of the femoral head fracture must therefore be seamlessly integrated into the Advanced Trauma Life Support (ATLS) resuscitation protocols. The initial focus is invariably on emergent closed reduction of the hip joint to relieve tension on the neurovascular structures and capsular vessels, followed by a highly calculated, meticulously executed open reduction and internal fixation (ORIF) once the patient's physiologic status permits.
The overarching goal of surgical intervention is the precise restoration of the articular sphere, rigid stabilization of the fracture fragments to allow for early mobilization, and the exhaustive removal of any osteochondral debris from the joint space. Failure to achieve these objectives invariably leads to rapid joint destruction, necessitating complex reconstructive arthroplasty in a young patient demographic. Therefore, mastering the surgical anatomy, understanding the nuances of the various surgical approaches, and executing flawless intraoperative fixation techniques are paramount for any trauma surgeon undertaking the management of these complex injuries.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the hip joint's surgical anatomy is the cornerstone of successful femoral head fracture fixation. The proximal femur and acetabulum form a highly constrained, intrinsically stable ball-and-socket joint, deepened by the fibrocartilaginous acetabular labrum. The labrum not only enhances femoral head coverage but also creates a crucial "suction seal" that contributes to joint stability and the retention of synovial fluid for cartilage nourishment. During a traumatic dislocation, this labrum is frequently torn, avulsed, or incarcerated within the joint space, necessitating careful intraoperative inspection and, when indicated, primary repair or debridement to prevent ongoing mechanical symptoms and joint deterioration.
The vascular anatomy of the proximal femur is notoriously unforgiving and dictates our surgical approach. The primary arterial supply to the critical superior, weight-bearing dome of the femoral head is derived from the medial femoral circumflex artery (MFCX). The MFCX, a branch of the deep femoral artery, courses posteriorly and superiorly, running deep to the quadratus femoris muscle. It gives rise to the critical retinacular vessels that penetrate the joint capsule just inferior to the piriformis tendon and ascend along the posterosuperior femoral neck. Surgical Warning: The MFCX and its terminal retinacular branches are extraordinarily vulnerable during posterior surgical approaches and any aggressive dissection around the posterior femoral neck. Iatrogenic injury to these vessels during exposure or reduction maneuvers will almost certainly precipitate devastating avascular necrosis (AVN).
Supplementary vascular contributions arise from the lateral femoral circumflex artery (LFCX) anteriorly and the foveal artery running within the ligamentum teres. The foveal artery's contribution is highly variable and generally insufficient to sustain the femoral head in the absence of the MFCX, particularly in adults. Crucially, the anterior half of the femoral neck is largely devoid of critical intra-capsular vascular structures. This anatomic reality provides a significant strategic advantage, rendering anterior surgical approaches (such as the Smith-Peterson) inherently safer regarding the preservation of the femoral head's primary blood supply, provided the dissection remains meticulously within the established internervous planes.
Navigating the muscular intervals requires a precise understanding of the surrounding neurovascular relationships. In the anterior (Smith-Peterson) approach, the primary internervous plane lies between the tensor fascia lata (superior gluteal nerve) laterally and the sartorius (femoral nerve) medially. Deep to this, the rectus femoris is mobilized, and the iliocapsularis is elevated to expose the anterior capsule. The lateral femoral cutaneous nerve (LFCN) is highly variable and frequently encountered superficial to the sartorius or TFL; it must be identified and protected to prevent painful postoperative meralgia paresthetica. Conversely, posterior approaches place the sciatic nerve at direct risk. The sciatic nerve typically exits the greater sciatic foramen inferior to the piriformis and descends deep to the gluteus maximus, resting directly upon the short external rotators. Traumatic posterior dislocations frequently stretch or contuse the sciatic nerve, making meticulous preoperative documentation of its function and careful intraoperative protection absolutely essential.
Exhaustive Indications and Contraindications
The decision-making process for the surgical management of femoral head fractures relies heavily on the precise characterization of the fracture morphology, best categorized by the Pipkin classification system. Originally described in 1957, this system remains the gold standard for guiding treatment algorithms and predicting clinical outcomes. The classification divides these injuries into four distinct types based on the relationship of the fracture line to the fovea capitis and the presence of associated fractures of the femoral neck or acetabulum.
| Pipkin Classification | Fracture Description | Primary Treatment Indication | Surgical Approach Preference |
|---|---|---|---|
| Type I | Fracture of the femoral head inferior to the fovea capitis. The fragment does not involve the primary weight-bearing zone. | Excision of small fragments; ORIF for large, fixable fragments to restore joint congruity. | Anterior (Smith-Peterson) approach for direct visualization and excision/fixation. |
| Type II | Fracture of the femoral head superior to the fovea capitis. The fragment involves the critical weight-bearing dome. | Absolute indication for anatomic ORIF. Excision is contraindicated due to loss of weight-bearing surface. | Anterior (Smith-Peterson) or Ganz Surgical Dislocation depending on fragment size and posterior extension. |
| Type III | Type I or II fracture associated with a fracture of the femoral neck. | Emergent ORIF. High risk of AVN. Fixation of neck takes priority, followed by head fixation. | Ganz Surgical Dislocation or combined approaches. Arthroplasty considered in older patients. |
| Type IV | Type I or II fracture associated with a fracture of the acetabulum (usually posterior wall). | ORIF of both the femoral head and the acetabular fracture. | Posterior (Kocher-Langenbeck) if posterior wall requires fixation; Ganz approach for complex combined patterns. |
Operative intervention is definitively indicated for all Pipkin Type II, III, and IV fractures, as well as any Type I fracture with a fragment large enough to be internally fixed or any fracture associated with an irreducible hip joint, incarcerated intra-articular loose bodies, or persistent joint incongruity following closed reduction. The primary goal is the absolute anatomic restoration of the articular surface. Even minor step-offs or gaps in the weight-bearing dome will dramatically accelerate the onset of post-traumatic osteoarthritis due to altered contact mechanics and elevated peak focal stresses on the remaining cartilage.
Non-operative management is exceptionally rare and is strictly reserved for a very narrow subset of clinical scenarios. It may be considered only for highly selected Pipkin Type I fractures characterized by very small, non-displaced fragments located well outside the weight-bearing zone, provided the hip joint is concentrically reduced, perfectly stable through a full range of motion, and entirely free of any incarcerated osteochondral debris on fine-cut computed tomography. Furthermore, the patient must be highly compliant and capable of adhering to a strict, prolonged regimen of restricted weight-bearing.
Contraindications to acute internal fixation include profound hemodynamic instability precluding safe anesthesia, active systemic infection, or severe, pre-existing ipsilateral hip osteoarthritis where primary total hip arthroplasty (THA) would yield a more predictable and durable outcome. In the elderly, low-demand patient with osteopenic bone, primary THA is increasingly favored over complex ORIF for displaced Pipkin II or III fractures, given the exceptionally high rates of fixation failure, AVN, and the necessity for secondary salvage procedures in this demographic.
Pre-Operative Planning, Templating, and Patient Positioning
The preoperative phase begins the moment the patient arrives in the trauma bay. Given the high-energy nature of these injuries, the initial assessment must rigorously adhere to ATLS protocols. Life-threatening hemorrhagic, thoracic, and cranial injuries must be identified and stabilized before any definitive orthopaedic intervention is contemplated. Once the patient is physiologically stable, attention is directed to the injured extremity. The absolute paramount priority is the emergent closed reduction of the dislocated hip. A dislocated hip places the capsular vessels under extreme tension, and the duration of dislocation is directly correlated with the incidence of subsequent avascular necrosis. Reduction must be performed urgently under deep conscious sedation or general anesthesia with complete skeletal muscle relaxation to prevent further iatrogenic shearing of the articular cartilage against the acetabular rim during the reduction maneuver.

Initial imaging consists of an anteroposterior (AP) radiograph of the pelvis, which will confirm the dislocation and often reveal the gross presence of a femoral head fracture (as seen in the image above). However, plain radiographs drastically underestimate the complexity of the injury. Crucially, definitive surgical planning must never delay the emergent reduction. Once the hip is concentrically reduced, a comprehensive imaging protocol is mandatory.
Following reduction, a fine-cut computed tomography (CT) scan of the pelvis with sagittal, coronal, and 3D reconstructions is the definitive diagnostic modality. The CT scan is essential for precisely defining the fracture morphology, mapping the size and location of the fragments, identifying subtle associated acetabular fractures, and, most importantly, detecting incarcerated osteochondral loose bodies within the joint space that would preclude non-operative management. Preoperative templating based on these CT reconstructions allows the surgeon to select the optimal surgical approach, anticipate the required fixation implants (e.g., headless compression screws, bioabsorbable pins), and formulate a step-by-step intraoperative strategy.
Following a successful closed reduction, the patient is typically placed in longitudinal skeletal traction utilizing a distal femoral or proximal tibial pin with approximately 20 to 30 pounds of weight. Traction serves multiple critical functions: it unloads the injured articular cartilage, maintains joint distraction to prevent third-body wear from retained intra-articular debris, and provides patient comfort by stabilizing the limb and reducing muscle spasms. Definitive surgical intervention is ideally performed within 24 to 48 hours, allowing time for adequate physiologic resuscitation and the assembly of a specialized orthopaedic trauma team, while minimizing the risks associated with prolonged bed rest.
Patient positioning is entirely dictated by the chosen surgical approach. For the anterior Smith-Peterson approach—our primary focus for isolated anterior femoral head fractures—the patient is positioned supine on a radiolucent operating table. A small bump is placed beneath the ipsilateral hemipelvis to slightly elevate the operative side and allow for unrestricted access to the lateral aspect of the hip. The entire affected lower extremity must be draped free into the sterile field. This free draping is absolutely critical, as it allows the surgeon to manipulate the limb through a full range of motion intraoperatively, facilitating complex reduction maneuvers, optimizing visualization of the femoral head through different windows of exposure, and allowing for dynamic assessment of joint stability following fixation.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the surgical approach and subsequent fracture fixation demands meticulous soft tissue handling, precise anatomic knowledge, and advanced osteosynthesis skills. Today, we detail the intraoperative masterclass for the Smith-Peterson Anterior Approach, the workhorse technique for the direct visualization and fixation of Pipkin I and II fractures located on the anterior or anteromedial aspect of the femoral head.
Incision and Superficial Dissection
With the patient properly positioned and the limb draped free, the anatomic landmarks are palpated and marked. The incision begins at the anterosuperior iliac spine (ASIS) and extends distally and slightly laterally for approximately 10 to 15 centimeters, aiming toward the lateral border of the patella. This curvilinear incision follows the natural Langer lines of the skin, promoting optimal wound healing.

The skin and subcutaneous adipose tissues are incised sharply down to the level of the deep investing fascia of the thigh. Hemostasis of the superficial dermal vessels is meticulously achieved with electrocautery. The deep fascia is then identified, appearing as a thick, glistening white layer overlying the anterior compartment musculature.

The initial fascial incision is made directly over the medial muscular belly of the tensor fascia lata (TFL). It is critical to incise the fascia slightly lateral to the actual internervous interval to avoid inadvertently entering the sheath of the sartorius muscle or injuring the lateral femoral cutaneous nerve, which frequently arborizes in this immediate vicinity.
Developing the Internervous Interval
The core of the superficial dissection relies on developing the true internervous plane between the TFL (innervated by the superior gluteal nerve) and the sartorius (innervated by the femoral nerve).
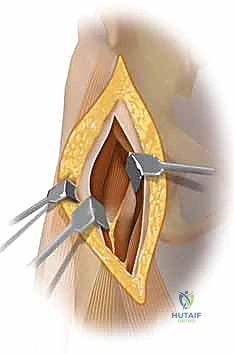
Using blunt finger dissection and careful sharp dissection with Metzenbaum scissors, the medial border of the TFL is separated from the lateral border of the sartorius. The TFL is retracted laterally using a Hibbs or Richardson retractor, while the sartorius is gently retracted medially. As this interval is opened, the surgeon must remain vigilant for the lateral femoral cutaneous nerve, gently mobilizing it and retracting it medially with the sartorius to prevent traction neuropraxia.
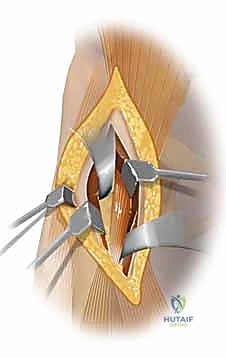
Deepening the dissection within this interval reveals the direct and indirect heads of the rectus femoris muscle. An overlying layer of deep investing fascia must be longitudinally divided to clearly expose the rectus. The rectus femoris is then mobilized and retracted medially. At the inferior aspect of this deep exposure, the ascending branches of the lateral femoral circumflex artery and vein will be encountered transversely crossing the operative field. These vessels must be meticulously isolated, ligated with heavy silk sutures, and divided to allow for adequate distal exposure and to prevent catastrophic postoperative hematoma formation.
Capsulotomy and Fracture Exposure
Deep to the rectus femoris lies the iliocapsularis muscle and the dense, fibrous anterior capsule of the hip joint. The iliocapsularis is bluntly elevated off the anterior capsule and swept medially.

A robust, T-shaped or H-shaped capsulotomy is then performed. The vertical limb of the capsulotomy is made parallel to the axis of the femoral neck, while the transverse limbs are made adjacent to the acetabular rim and the intertrochanteric line. Heavy tagging sutures (e.g., #1 Vicryl or Ethibond) are placed in the capsular flaps to facilitate retraction and subsequent watertight closure.

Upon opening the capsule, the fracture site is immediately visualized. The joint is thoroughly irrigated to clear hematoma and small osteochondral debris. The main fracture fragment is carefully identified. It is imperative to avoid stripping any residual soft tissue attachments from the fragment, as these may provide a tenuous but critical blood supply. The fracture bed on the femoral head is meticulously debrided of any interposed clot or loose cancellous bone that would impede a perfect anatomic reduction.
Reduction and Provisional Fixation
Achieving an anatomic reduction is the most critical step of the procedure. The hip is gently externally rotated and extended to optimize the presentation of the anterior femoral head.

Using a dental pick or a small bone hook, the fracture fragment is gently manipulated into its anatomic position. The reduction must be absolutely perfect; even a 1-millimeter step-off is unacceptable in the weight-bearing dome. Once reduced, the fragment is provisionally stabilized using multiple smooth 1.5mm or 2.0mm Kirschner wires (K-wires). These wires should be placed peripherally to avoid interfering with the planned trajectory of the definitive fixation screws.
Definitive Internal Fixation
Definitive fixation is typically achieved using multiple small-fragment (2.0mm to 3.0mm) headless compression screws or, in specific cases, bioabsorbable pins. Headless screws are preferred as they provide superior interfragmentary compression and rotational stability while allowing the implant to be buried entirely beneath the articular cartilage, thereby preventing catastrophic third-body wear against the acetabulum.
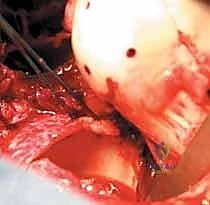
The guide wires for the headless compression screws are drilled perpendicular to the fracture plane to maximize compression.
The depth is measured meticulously. It is critical to select a screw length that provides adequate thread purchase in the dense subchondral bone of the intact femoral head without penetrating the posterior cortex or the posterior articular surface.

The near cortex (articular surface of the fragment) is overdrilled or countersunk to ensure the trailing head of the screw will sit flush or slightly recessed beneath the cartilage.

The headless compression screws are then carefully inserted over the guide wires.

As the screws are advanced, the surgeon must visually confirm that the trailing threads fully engage the fragment and draw it tightly against the main body of the femoral head, achieving robust interfragmentary compression.

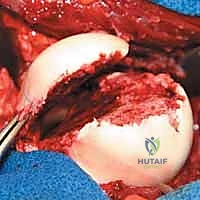
Once all screws are fully seated, the provisional K-wires are removed. The articular surface is meticulously palpated with a Freer elevator to guarantee that no screw heads are proud. A proud screw will act like a milling cutter, rapidly destroying the acetabular cartilage.

The joint is then irrigated copiously one final time. The hip is taken through a full range of motion under direct visualization to confirm the stability of the fixation and to ensure there is no impingement of the hardware against the acetabular rim.

Intraoperative fluoroscopy is utilized to obtain orthogonal views (AP and lateral) of the proximal femur. This final imaging confirms the anatomic reduction, verifies the appropriate length and trajectory of the screws, and ensures that no hardware has penetrated the joint space posteriorly. Following radiographic confirmation, the capsule is closed loosely to prevent hematoma accumulation, and the wound is closed in layers over a closed suction drain.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical execution, femoral head fractures are fraught with a high incidence of severe, life-altering complications. The immense energy of the initial trauma, combined with the tenuous vascularity of the proximal femur, creates an environment ripe for adverse outcomes. Patients must be extensively counseled preoperatively regarding these risks and the potential necessity for future reconstructive surgeries.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Management & Salvage Strategy |
|---|---|---|---|
| Avascular Necrosis (AVN) | 10% - 30% | Disruption of MFCX or retinacular vessels during dislocation or surgical exposure. Delayed reduction (>6 hours) exponentially increases risk. | Early stages: Core decompression (controversial in trauma). Late stages with collapse: Total Hip Arthroplasty (THA). |
| Post-Traumatic Osteoarthritis (PTOA) | 20% - 50% | Primary chondral damage at time of impact; non-anatomic reduction; retained intra-articular debris; proud hardware. | Conservative management initially (NSAIDs, injections). Definitive salvage is THA or, rarely in very young laborers, arthrodesis. |
| Heterotopic Ossification (HO) | 15% - 40% | Extensive soft tissue trauma, muscle stripping, and hematoma formation. Higher risk with posterior or extensile approaches. | Prophylaxis with Indomethacin or single-dose radiation. Surgical excision only if mature and mechanically restricting ROM. |
| Sciatic Nerve Palsy | 10% - 20% | Stretch or contusion during initial posterior dislocation; iatrogenic injury during posterior surgical approaches. | Observation and AFO for foot drop. Most recover partially or fully within 1-2 years. Nerve exploration rarely indicated acutely. |
Avascular necrosis remains the most feared complication, often presenting insidiously months to years after the index procedure. The pathophysiology is driven by the ischemia induced by the initial capsular tearing and vessel stretch, compounded by any iatrogenic damage during surgical exposure. If AVN progresses to subchondral collapse and joint incongruity, the only reliable salvage procedure is a Total Hip Arthroplasty. While THA provides excellent pain relief and functional restoration, performing it in a young, active patient introduces the long-term risks of implant wear, aseptic loosening, and the eventual need for complex revision arthroplasty.
Post-traumatic osteoarthritis is arguably the most common long-term sequela. Even with a perfectly executed anatomic reduction, the initial traumatic insult to the chondrocytes (the "dashboard" impact) often triggers a cascade of apoptosis and cartilage degradation. The presence of any residual step-off or gap at the fracture site will dramatically accelerate this process. Management of PTOA follows a standard escalating algorithm, beginning with activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid injections, ultimately culminating in THA when conservative measures fail.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following femoral head fracture fixation is a delicate balancing act. The surgeon must facilitate early mobilization to prevent joint stiffness and
