Open Reduction and Internal Fixation of Lisfranc Injuries: An Operative Masterclass
Key Takeaway
This masterclass provides an exhaustive, real-time walkthrough of open reduction and internal fixation for Lisfranc injuries. Fellows will learn intricate midfoot anatomy, critical preoperative planning, and a granular, step-by-step intraoperative execution from incision to hardware application. We cover neurovascular protection, meticulous soft tissue handling, and strategies for achieving anatomical reduction and stable fixation, alongside comprehensive pearls, pitfalls, and postoperative care.
Comprehensive Introduction and Patho-Epidemiology
The tarsometatarsal (TMT) joint complex, eponymously named after the Napoleonic-era surgeon Jacques Lisfranc de St. Martin, represents the critical transition zone between the midfoot and the forefoot. Injuries to this region are notoriously complex, often subtle, and historically fraught with high rates of misdiagnosis. A Lisfranc injury is not a singular pathological entity but rather a broad, heterogeneous spectrum of midfoot trauma ranging from subtle, purely ligamentous sprains to grossly unstable, high-energy fracture-dislocations. As orthopedic surgeons, we must approach these injuries with an exceptionally high index of suspicion, as failure to recognize and anatomically restore the TMT complex inevitably leads to progressive midfoot collapse, post-traumatic osteoarthritis, and profound functional disability for the patient.
Epidemiologically, Lisfranc injuries account for approximately 0.2% of all fractures, translating to an incidence of roughly 1 in 100,000 individuals per year. However, this statistic likely underestimates the true burden of disease, as up to 20% of these injuries are missed during the initial emergency department evaluation. The subtle diastasis of the first and second metatarsal bases can easily be overlooked on non-weight-bearing radiographs, particularly in polytraumatized patients where distracting injuries command immediate attention. The clinical consequence of a missed Lisfranc injury is a rapid deterioration of the longitudinal and transverse arches of the foot, leading to a rigid, painful, and planovalgus deformity that is exceedingly difficult to salvage.

The patho-mechanisms driving Lisfranc injuries are broadly categorized into direct and indirect forces. Direct trauma involves a high-energy crush mechanism to the dorsum of the midfoot, typically seen in industrial accidents or motor vehicle collisions. These injuries are frequently associated with severe soft tissue compromise, open fractures, and highly comminuted bony architecture, culminating in a complex presentation that threatens the viability of the limb. Conversely, indirect trauma is far more common and often results from lower-energy mechanisms, such as athletic injuries or simple ground-level falls.
The classic indirect mechanism involves a longitudinal axial load applied to a plantarflexed foot. As the patient's body weight drives downward through the hindfoot, the metatarsal heads are fixed against the ground, creating a massive bending moment across the TMT joints. Depending on the precise vector of the force—whether coupled with abduction, adduction, or rotational torque—the capsuloligamentous structures will fail in a predictable sequence. Hyper-plantarflexion ruptures the dorsal ligaments first, followed by the intra-articular and plantar ligaments, ultimately leading to dorsal dislocation of the metatarsal bases. Recognizing this specific pathoanatomy is the foundation upon which our operative strategy is built.
Detailed Surgical Anatomy and Biomechanics
Before a single incision is planned, an exhaustive, three-dimensional understanding of midfoot osteology and ligamentous anatomy is paramount. The structural integrity of the Lisfranc complex relies on a synergistic relationship between inherent bony architecture and robust ligamentous restraints. In the coronal plane, the bases of the first three metatarsals and their corresponding cuneiforms form a highly stable, trapezoidal structure known as the "Roman Arch." The plantar aspect of these bones is narrower than the dorsal aspect, creating a natural concavity that forms the transverse arch of the foot.

The absolute keystone of this Roman Arch is the base of the second metatarsal. It is uniquely recessed proximally into a mortise formed by the medial and lateral cuneiforms, while articulating directly with the middle cuneiform. This "locking" mechanism severely restricts translation in the coronal and sagittal planes. Any disruption of this keystone—whether via a fracture of the second metatarsal base or a rupture of its ligamentous anchors—destabilizes the entire midfoot, allowing the remaining metatarsals to displace dorsally and laterally.

Ligamentous stability is provided by an intricate network of dorsal, interosseous, and plantar ligaments. The dorsal ligaments are relatively thin and weak, making them susceptible to initial rupture during hyper-plantarflexion injuries. The plantar ligaments, conversely, are thick, stout, and serve as the primary stabilizers of the arch. The most critical of these is the Lisfranc ligament, a massive interosseous structure originating from the lateral aspect of the medial cuneiform and inserting obliquely onto the medial aspect of the second metatarsal base. It is imperative to note that there is no direct intermetatarsal ligament between the first and second metatarsals. This anatomical void represents the primary vulnerability of the midfoot, rendering the first-second TMT interval entirely dependent on the Lisfranc ligament for stability.

Biomechanically, the midfoot is divided into three distinct functional columns. The medial column consists of the first metatarsal and the medial cuneiform; it exhibits minimal inherent motion and is primarily designed for rigid load transmission during the toe-off phase of gait. The middle column comprises the second and third metatarsals and their respective cuneiforms; this is the most rigid segment of the foot, acting as the central axis of stability. Because the medial and middle columns are non-essential for accommodative motion, they are highly amenable to rigid internal fixation or primary arthrodesis.

In stark contrast, the lateral column—consisting of the fourth and fifth metatarsals articulating with the cuboid—is highly mobile. It must retain its flexibility to allow the foot to adapt to uneven terrain. Therefore, rigid fixation of the lateral column is strictly contraindicated; if stabilization is required, it must be achieved with flexible, temporary implants such as Kirschner wires (K-wires) to preserve essential joint kinematics. Neurovascularly, the dorsalis pedis artery and the deep peroneal nerve descend over the dorsum of the foot, typically coursing directly over the first-second intermetatarsal space. These structures are at high risk during dorsal approaches and must be meticulously protected via full-thickness subperiosteal dissection.
Exhaustive Indications and Contraindications
The decision-making process for operative intervention in Lisfranc injuries hinges on the degree of instability, the specific anatomical structures involved, and the physiological status of the patient. The overarching goal of surgery is the precise, anatomical restoration of the TMT joint complex to re-establish the functional columns of the foot. Any displacement greater than 2 millimeters at any of the TMT joints, or any evidence of gross instability on stress radiographs, constitutes an absolute indication for operative management.
Historically, open reduction and internal fixation (ORIF) was the universal gold standard for all Lisfranc injuries. However, contemporary orthopedic literature has driven a paradigm shift, particularly regarding purely ligamentous injuries. Purely ligamentous disruptions have a notoriously poor healing capacity and a high propensity for late collapse and post-traumatic arthritis, even with anatomical ORIF. Consequently, primary arthrodesis of the medial and middle columns is increasingly indicated for purely ligamentous injuries, whereas ORIF remains the treatment of choice for bony fracture-dislocations where the articular cartilage remains largely intact.

Contraindications to operative intervention must be carefully weighed to prevent catastrophic surgical complications. Severe soft tissue compromise, such as massive fracture blisters, deep abrasions, or impending compartment syndrome, is an absolute contraindication to immediate definitive internal fixation. In these scenarios, the surgeon must employ damage control orthopedics, utilizing joint-spanning external fixation or temporary K-wire stabilization until the soft tissue envelope has recovered.

Patient-specific factors also play a critical role in surgical planning. Severe peripheral vascular disease (PVD) or uncontrolled diabetes mellitus with dense peripheral neuropathy (Charcot arthropathy) represent significant relative, if not absolute, contraindications to standard ORIF. In neuropathic patients, the risk of hardware failure, nonunion, and catastrophic midfoot collapse is exponentially higher; these patients often require extended periods of non-weight bearing, ultra-rigid fixation constructs (such as beaming techniques), or primary arthrodesis supplemented with robust orthotic management.
Indications and Contraindications Matrix
| Parameter | Indications for Operative Intervention (ORIF / Arthrodesis) | Contraindications (Absolute and Relative) |
|---|---|---|
| Anatomical | >2mm displacement at any TMT joint; Loss of arch height; "Fleck sign" present; Gross instability on stress views. | Non-displaced, stable injuries on weight-bearing radiographs. |
| Pathological | Bony fracture-dislocations (ORIF); Purely ligamentous injuries (Primary Arthrodesis preferred). | Active soft tissue infection; Severe crush injury with unresuscitable skin envelope. |
| Patient Factors | High-demand athletes; Healthy adults requiring restoration of normal foot biomechanics. | Severe peripheral neuropathy (Charcot); Critical limb ischemia; Non-ambulatory status. |
| Timing | Acute injuries (within 2-3 weeks) once soft tissue swelling has subsided (wrinkle sign present). | Delayed presentation (>6 weeks) may require salvage arthrodesis rather than acute ORIF. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the bedrock of a successful Lisfranc reconstruction. The clinical examination is the first critical step. Patients typically present with an inability to bear weight, diffuse midfoot edema, and exquisite tenderness over the TMT joints. The presence of plantar ecchymosis—the classic "bruise on the bottom of the foot"—is highly pathognomonic for a Lisfranc injury, representing bleeding from the disrupted plantar ligaments tracking along the fascial planes. The "piano key" test, involving passive dorsal and plantar flexion of the individual metatarsal heads, will elicit sharp pain at the involved TMT articulations.

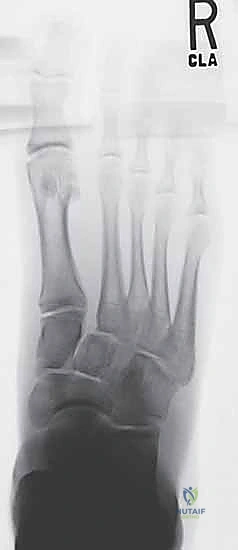
Imaging must be comprehensive. Standard non-weight-bearing anteroposterior (AP), oblique, and lateral radiographs are the initial screening tools. On the AP view, the medial border of the second metatarsal must align perfectly with the medial border of the middle cuneiform. On the oblique view, the medial border of the fourth metatarsal must align with the medial border of the cuboid. The lateral view is scrutinized for any dorsal displacement of the metatarsal bases or flattening of the longitudinal arch. Look specifically for the "fleck sign" in the first intermetatarsal space, which represents a bony avulsion of the Lisfranc ligament from the base of the second metatarsal.

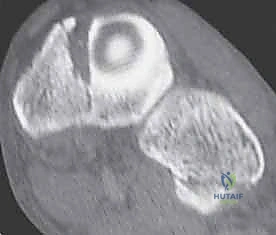
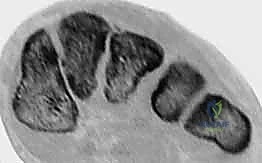
If non-weight-bearing radiographs are equivocal, weight-bearing films are absolutely mandatory to unmask subtle, dynamic instability. However, in the modern era, a fine-cut Computed Tomography (CT) scan is considered the gold standard for pre-operative templating. A CT scan provides unparalleled visualization of occult intra-articular comminution, impaction of the cuneiforms, and the precise trajectory of fracture lines. This three-dimensional understanding allows the surgeon to anticipate the need for bone grafting, select the optimal fixation constructs (e.g., dorsal bridge plates vs. trans-articular screws), and plan the sequence of reduction.

Patient positioning and operating room setup must be optimized for efficiency and fluoroscopic access. The patient is placed supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral, upward-facing position. A thigh or calf tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying the delicate neurovascular structures on the dorsum of the foot. The fluoroscopy (C-arm) unit is positioned on the contralateral side, entering perpendicular to the table, allowing for rapid and effortless transitions between AP, oblique, and lateral views without compromising the sterile field.

Step-by-Step Surgical Approach and Fixation Technique
Incision Placement and Deep Dissection
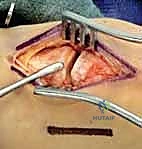
The surgical approach to the Lisfranc complex typically utilizes a dual-incision technique to access all functional columns while minimizing soft tissue complications. The primary dorsomedial incision is centered over the first intermetatarsal space, extending from the naviculocuneiform joint proximally to the mid-shaft of the first and second metatarsals distally. This incision provides excellent access to the medial and middle columns (1st and 2nd TMT joints). During superficial dissection, the extensor hallucis brevis (EHB) muscle belly is identified and retracted laterally.

Deep dissection in the first web space must be exceedingly meticulous to identify and protect the dorsalis pedis artery and the deep peroneal nerve. These structures are typically mobilized together and retracted laterally. A full-thickness subperiosteal flap is elevated off the joint capsules to preserve the delicate vascular supply to the skin edges. If the lateral column is involved, a secondary dorsolateral incision is made centered over the 3rd and 4th TMT joints. It is an absolute surgical imperative to maintain a minimum "skin bridge" of 5 to 7 centimeters between these two incisions to prevent catastrophic skin necrosis and wound breakdown.

Joint Preparation and the Sequence of Reduction
Once the joints are exposed, all hematoma, soft tissue interposition, and small, non-structural osteochondral fragments must be rigorously debrided to allow for anatomical reduction. If a primary arthrodesis is planned, the articular cartilage of the medial and middle columns is systematically denuded down to bleeding subchondral bone using a combination of osteotomes, curettes, and high-speed burrs.

The sequence of reduction is critical and must proceed in a logical, stepwise fashion, typically moving from medial to lateral. The absolute priority is the anatomical restoration of the keystone—the second metatarsal base into the cuneiform mortise. A point-to-point reduction clamp is placed with one tine on the medial aspect of the medial cuneiform and the other on the lateral aspect of the second metatarsal base. Compression across this interval recreates the vector of the intact Lisfranc ligament. Once the second metatarsal is perfectly reduced and provisionally pinned, the first TMT joint is reduced, followed by the third TMT joint. The lateral column (4th and 5th TMTs) will often spontaneously reduce once the medial and middle columns are stabilized; if not, they are reduced and pinned.

Definitive Fixation Strategies
The philosophy of fixation has evolved significantly. For the rigid medial and middle columns, solid, trans-articular cortical screws (typically 3.5mm or 4.0mm) have historically been the workhorse. The "home run screw" is placed from the medial cuneiform, directed distally and laterally into the base of the second metatarsal, directly mimicking the anatomical path of the Lisfranc ligament. Additional trans-articular screws are placed across the 1st and 3rd TMT joints.

However, trans-articular screws inherently damage the articular cartilage and are prone to breakage when the patient begins weight-bearing. Therefore, the use of dorsal bridge plating has gained immense popularity for ORIF. Low-profile, anatomically contoured dorsal plates stabilize the joints without violating the articular surfaces, preserving the cartilage and reducing the risk of iatrogenic arthritis.
For the mobile lateral column, rigid fixation (screws or plates) is strictly prohibited, as it will inevitably lead to hardware failure and a stiff, painful foot. The lateral column must be stabilized with smooth K-wires (typically 1.6mm or 2.0mm) driven from the base of the 4th and 5th metatarsals into the cuboid. These wires provide temporary stability while the soft tissues heal and are routinely removed in the clinic at 6 to 8 weeks post-operatively to restore essential lateral column kinematics.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following Lisfranc injuries remain a formidable clinical challenge. The severity of the initial trauma, combined with the complex biomechanics of the midfoot, predisposes patients to a variety of early and late sequelae. The most pervasive and debilitating long-term complication is post-traumatic osteoarthritis (PTOA). Even with perfectly anatomical ORIF, the incidence of PTOA in the TMT joints can exceed 50%, particularly in purely ligamentous injuries or cases with severe intra-articular comminution. The initial impact drives osteochondral shear forces that cause irreversible chondrocyte death, leading to joint space narrowing, osteophyte formation, and chronic midfoot pain.

Hardware-related complications are also exceedingly common. Trans-articular screws are subjected to immense bending moments during the toe-off phase of gait. If these screws are not removed prior to the initiation of full weight-bearing, fatigue failure and screw breakage are highly predictable events. While a broken screw within the substance of the bone may be asymptomatic, it severely complicates future salvage operations. Dorsal bridge plates, while sparing the joint, can cause significant soft tissue irritation, extensor tendon tendinopathy, and necessitate a secondary surgery for hardware removal in up to 30% of patients.

Early post-operative complications center around the soft tissue envelope. Wound dehiscence, marginal skin necrosis, and superficial surgical site infections occur in approximately 5-10% of cases, heavily influenced by the timing of surgery and the width of the skin bridge. Deep infections are rare but catastrophic, requiring immediate operative debridement and potential hardware explantation. Furthermore, due to the high-energy nature of these injuries, the surgeon must remain hyper-vigilant for the development of compartment syndrome of the foot. Excessive post-operative pain out of proportion to the procedure, particularly pain with passive stretch of the toes, demands immediate evaluation and potential fasciotomy.

When primary ORIF fails—manifesting as painful nonunion, malunion with planovalgus collapse, or severe PTOA—salvage management is required. The definitive salvage procedure is a midfoot arthrodesis. This involves taking down the failed hardware, aggressively resecting the sclerotic or deformed joint surfaces, restoring the anatomical arch height with structural bone graft (autograft or allograft), and utilizing ultra-rigid fixation (multi-hole plates or beaming screws) to achieve a solid fusion. While an arthrodesis sacrifices midfoot motion, it is highly effective at alleviating pain and providing a stable, plantigrade foot for ambulation.

Complications and Salvage Strategies Matrix
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Post-Traumatic Arthritis | 30% - 60% | Chondral damage at impact; Purely ligamentous injuries; Inadequate reduction. | NSAIDs, custom orthotics (stiff Morton's extension); Definitive: Midfoot Arthrodesis. |
| Hardware Failure (Screw Breakage) | 15% - 25% | Weight-bearing prior to screw removal; Trans-articular screw placement. | Observation if asymptomatic. Removal if symptomatic. Use dorsal plates to prevent. |
| Wound Dehiscence / Necrosis | 5% - 10% | Operating through swollen tissues; Skin bridge < 5cm; Smoking; Diabetes. | Local wound care; Vacuum-assisted closure (VAC); Rarely requires flap coverage. |
| Iatrogenic Nerve Injury | 3% - 8% | Retraction injury to Deep Peroneal or Superficial Peroneal nerves. | Often transient neurapraxia. Gabapentinoids. Surgical exploration if complete transection suspected. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following Lisfranc reconstruction is a protracted and meticulously phased process. The primary objective is to protect the delicate capsuloligamentous repairs and bony fixation while allowing the soft tissue envelope to heal. Premature weight-bearing is the most common cause of early fixation failure and loss of reduction.

Phase I (Weeks 0-2): Strict Protection. Immediately post-operatively, the patient is placed in a well-padded, bulky posterior splint. They are strictly non-weight-bearing (NWB) on the operative extremity. Strict elevation above the level of the heart is mandatory to mitigate edema and prevent wound compromise. At the two-week mark, the patient returns to the clinic for suture removal and a thorough wound inspection.

Phase II (Weeks 2-6): Immobilization and Early Motion. Once the wounds are sealed, the patient is transitioned into a rigid, removable controlled ankle motion (CAM) boot or a short-leg cast. They remain strictly NWB. If a CAM boot is utilized, the patient may be permitted to perform gentle, active range of motion (ROM) exercises of the ankle and metatarsophalangeal (MTP) joints out of the boot, provided the lateral column was not pinned. If K-wires are present in the lateral column, they are typically pulled in the clinic at the 6-week mark.

Phase III (Weeks 6-12): Progressive Weight-Bearing. At 6 weeks, new weight-bearing radiographs are obtained to assess for maintenance of reduction and early bony healing. If satisfactory, the patient begins a progressive, graduated weight-bearing protocol in the CAM boot. This usually starts at 25% body weight, increasing by 25% weekly until full weight-bearing is achieved. Physical therapy is initiated, focusing on intrinsic foot muscle strengthening, proprioceptive training, and Achilles tendon stretching to counteract the equinus contracture that often develops during immobilization.
Phase IV (Months 3-6+): Hardware Management and Return to Activity. By 10 to 12 weeks, the patient is transitioned out of the CAM boot into a stiff-soled supportive shoe, often augmented with a custom orthotic featuring a rigid carbon fiber footplate to support the midfoot arch. If trans-articular screws were used for the medial and middle columns, a critical decision must be made regarding hardware removal. To prevent screw breakage, these screws are routinely removed in the operating room at 4 to 6 months post-operatively, before the patient is cleared for high-impact activities or running. If dorsal bridge plates or primary arthrodesis were utilized, routine hardware removal is not required unless the implants become symptomatic. Return to high-level sports typically takes 6 to 12 months and requires passing rigorous functional testing.

Summary of Landmark Literature and Clinical Guidelines
The evolution of Lisfranc injury management has been heavily guided by several landmark orthopedic studies. Historically, the classification system proposed by Myerson et al. (1986) provided the foundational language for describing these injuries. Myerson categorized Lisfranc fracture-dislocations into Type A (total incongruity), Type B (partial incongruity), and Type C (divergent). While this classification is highly descriptive of the radiographic appearance, it has largely been recognized as having limited prognostic value and does not strictly dictate the surgical approach, which is more heavily influenced by column theory and the specific tissues injured.

A pivotal shift in surgical philosophy was catalyzed by the randomized controlled trial conducted by **Ly
Clinical & Radiographic Imaging Archive