Open Reduction of Supracondylar Fractures of the Humerus
Comprehensive Introduction and Patho-Epidemiology
Supracondylar fractures of the distal humerus represent the most common type of elbow fracture in the pediatric population, accounting for nearly sixty percent of all fractures around the elbow in children under the age of ten. The vast majority of these injuries are extension-type fractures, resulting from a fall onto an outstretched hand with the elbow in full extension. This mechanism generates severe bending moments across the structurally vulnerable distal humerus, leading to failure of the anterior cortex and subsequent displacement of the distal fragment posteriorly. While historically managed with olecranon skeletal traction or closed reduction and casting—methods fraught with high rates of malunion and Volkmann ischemic contracture—the modern gold standard for displaced supracondylar fractures is closed reduction and percutaneous pinning (CRPP).
Despite the high success rate of CRPP, a critical subset of supracondylar fractures defies closed reduction techniques, necessitating open reduction. During preoperative planning, the orthopedic surgeon must carefully analyze the pathoanatomy of the injury to anticipate the reasons why an open procedure may become necessary. The primary driver for an open reduction is the inability to achieve an acceptable, stable anatomic reduction via closed means. This irreducibility is most frequently caused by soft tissue interposition, typically involving the brachialis muscle, the anterior periosteum, or, critically, the neurovascular bundle. When the proximal metaphyseal spike buttonholes through these anterior structures, closed manipulation often tightens the soft tissue noose around the bone, rendering percutaneous pinning impossible without preceding open release.
The decision to transition from a closed to an open procedure must be made judiciously but without hesitation when indicated. Prolonged, repeated attempts at closed reduction not only traumatize the delicate pediatric physis and surrounding soft tissues but also significantly increase the risk of iatrogenic neurovascular injury and subsequent compartment syndrome. An open reduction allows for direct visualization of the fracture fragments, meticulous extrication of entrapped neurovascular structures, and precise anatomic alignment of the medial and lateral columns.
While the overall incidence of open reduction for supracondylar fractures has decreased over the last two decades due to improved closed reduction techniques and enhanced fluoroscopic imaging, mastery of the open approach remains an indispensable skill for the pediatric orthopedic surgeon. The literature demonstrates that when an open reduction is performed promptly and executed with meticulous surgical technique, the long-term functional and radiographic outcomes are highly comparable to those achieved with successful closed reduction, albeit with a slightly protracted course of postoperative rehabilitation regarding terminal range of motion.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the complex osseous and neurovascular anatomy of the pediatric elbow is paramount for safely navigating an open reduction. The distal humerus is uniquely designed to accommodate the complex hinge and rotational movements of the elbow joint. It is characterized by two robust pillars of bone—the medial and lateral columns—that diverge distally to support the articular segment. Between these columns lies a remarkably thin, diaphanous wafer of bone that separates the anterior coronoid fossa from the posterior olecranon fossa. This thin central region creates a significant stress riser, making the supracondylar region inherently prone to fracture under high-energy axial and bending loads.
The muscular anatomy surrounding the distal humerus plays a critical role in both the displacement of the fracture and the challenges of reduction. The brachialis muscle drapes directly over the anterior aspect of the distal humerus capsule. In severe extension-type injuries, the sharp anterior spike of the proximal humeral shaft frequently lacerates and buttonholes through the brachialis muscle and the overlying anterior periosteum. The triceps muscle, attaching to the olecranon, acts as a deforming force, pulling the distal fragment proximally and posteriorly, resulting in the classic shortening and apex-anterior angulation seen on lateral radiographs.
The neurovascular anatomy is the most critical consideration during both closed and open management of these fractures. The brachial artery and the median nerve course together through the anterior compartment of the arm, crossing the elbow joint centrally within the antecubital fossa. In extension-type fractures with posterolateral displacement of the distal fragment, the proximal metaphyseal spike is driven anteromedially, placing the brachial artery and median nerve at extreme risk of tethering, contusion, or outright laceration. The bicipital aponeurosis (lacertus fibrosus) acts as a rigid fascial band that can further compress these structures against the displaced bone, exacerbating vascular compromise.
The radial and ulnar nerves also possess distinct vulnerabilities based on the fracture pattern. The radial nerve courses from posterior to anterior, piercing the lateral intermuscular septum just above the radiocapitellar joint. It is particularly susceptible to tethering in extension-type fractures with posteromedial displacement, where the proximal spike is driven anterolaterally. Conversely, the ulnar nerve passes posterior to the medial epicondyle within the cubital tunnel. While less commonly injured by the initial trauma in extension fractures, the ulnar nerve is highly vulnerable in flexion-type fractures and is at significant iatrogenic risk during the placement of medial entry pins. Understanding these anatomic relationships dictates not only the surgical approach but also the systematic identification and protection of these structures during open reduction.
Exhaustive Indications and Contraindications
The indications for open reduction of a pediatric supracondylar humerus fracture must be clearly defined to avoid unnecessary surgical morbidity while ensuring limb salvage and optimal functional outcomes. The absolute indication for immediate open reduction is an open fracture, which necessitates emergent surgical debridement, irrigation, and stabilization to mitigate the risk of deep infection and osteomyelitis. Similarly, a fracture presenting with a dysvascular hand that does not reconstitute perfusion following a gentle, anatomic closed reduction mandates emergent open exploration. In these scenarios, the brachial artery is often found to be entrapped within the fracture site, compressed by the lacertus fibrosus, or suffering from severe intimal damage and vasospasm requiring potential vascular reconstruction.
Irreducibility represents the most common relative indication that converts to an absolute indication intraoperatively. A supracondylar fracture that cannot be anatomically aligned via closed reduction and percutaneous pinning must be opened. Irreducibility is frequently heralded by clinical signs such as severe puckering or dimpling of the anterior skin (the "pucker sign"), which pathognomonically indicates that the proximal fragment has buttonholed through the brachialis muscle and is tethered to the deep dermis. Repeated, forceful attempts to reduce a buttonholed fracture blindly will only cause further soft tissue destruction and increase the risk of compartment syndrome.
Contraindications to open reduction are relatively few but must be respected. A primary contraindication is a fracture that can be adequately and stably reduced using closed methods. Unnecessary open reduction introduces risks of infection, increased scar formation, and prolonged postoperative stiffness. Furthermore, severe soft tissue compromise, such as extensive blistering or active superficial infection over the planned incision site, may necessitate a delay in surgery or an alteration of the surgical approach to avoid operating through compromised skin.
A highly debated topic within the realm of indications is the timing of surgical intervention. Historically, all displaced supracondylar fractures were treated as orthopedic emergencies. However, contemporary literature supports that in the absence of neurovascular compromise, open fractures, or severe soft tissue tenting, delayed treatment (typically within 12 to 24 hours) does not significantly increase the rate of complications or the necessity for open reduction. This paradigm shift allows for surgeries to be performed during daylight hours by specialized pediatric orthopedic teams, optimizing patient safety and surgical outcomes.
| Clinical Scenario | Indication Type | Rationale / Surgical Consideration |
|---|---|---|
| Open Fracture | Absolute | Requires emergent irrigation, debridement, and rigid internal fixation to prevent osteomyelitis. |
| Dysvascular Hand (Post-Reduction) | Absolute | Indicates brachial artery entrapment, laceration, or severe spasm. Requires anterior open exploration. |
| Irreducible Fracture (Buttonholing) | Absolute | Soft tissue interposition (brachialis/periosteum) prevents anatomic alignment. Open release is required. |
| Pucker Sign (Skin Tenting) | Relative to Absolute | High likelihood of brachialis buttonholing. Often fails closed reduction, necessitating an anterior approach. |
| Adequate Closed Reduction Achievable | Contraindication | Unnecessary open reduction increases risks of stiffness, infection, and iatrogenic injury. |
| Active Overlying Skin Infection | Relative Contraindication | Risk of seeding the fracture site. May require delayed treatment or alternative surgical approach. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful open reduction. The surgeon must meticulously review the mechanism of injury, the patient's medical history, and the physical examination findings. A comprehensive neurovascular examination is paramount and must be documented precisely. The examiner must assess the radial, median (including the anterior interosseous nerve branch, which is the most commonly injured nerve in extension-type fractures), and ulnar nerves. Vascular assessment includes palpation of the radial and ulnar pulses and evaluation of capillary refill. If the hand is pale, pulseless, and cold, the situation is an absolute emergency.
Radiographic evaluation requires high-quality, true anteroposterior (AP) and lateral views of the elbow. The surgeon must assess the direction of displacement of the distal fragment, as this dictates the location of the neurovascular structures at risk and guides the choice of surgical approach. Measurement of Baumann's angle and the anterior humeral line provides a template for the required anatomic reduction. Furthermore, the surgeon must plan the fixation strategy. For the vast majority of pediatric patients, 0.062-inch (1.6 mm) smooth Kirschner wires provide optimal biomechanical stability without causing excessive physeal damage. In very young children, 0.045-inch wires may be utilized, while older adolescents may require 2.0 mm pins. The surgical plan should default to at least three widely divergent lateral-entry pins for unstable Type III fractures, with a contingency for medial cross-pinning if lateral column fixation proves biomechanically insufficient.
Patient positioning and operating room setup are critical for seamless execution. The patient is placed supine on the operating table with the affected extremity extended onto a radiolucent hand table attachment. The patient should be positioned close to the edge of the main table to allow the surgeon unimpeded access. A sterile tourniquet is applied high on the proximal arm after meticulous skin preparation and sterile draping. The use of a sterile tourniquet allows for maximal exposure of the surgical field while providing the ability to achieve a bloodless field during critical dissection, though it must be deflated periodically to assess vascular perfusion if arterial injury is suspected.
The fluoroscopy unit (C-arm) must be positioned to allow effortless transition between AP and lateral imaging without compromising the sterile field. Typically, the C-arm is brought in parallel to the operating table, or perpendicular to it, depending on the surgeon's preference and the room's constraints. The surgeon must confirm that the C-arm can easily roll into the field to visualize the elbow in both planes before the incision is made. The monitor should be placed directly across from the surgeon for ergonomic viewing during the reduction and pinning phases of the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The selection of the surgical approach is dictated by the direction of fracture displacement and the presence of specific complications. While medial, lateral, and posterior approaches have been described, the transverse anterior approach through the antecubital fossa is widely considered the gold standard for extension-type supracondylar fractures requiring open reduction. The anterior approach provides direct, unparalleled visualization of the most commonly interposed structures—the brachialis muscle and the anterior periosteum—and allows for immediate identification and protection of the brachial artery and median nerve. Conversely, posterior approaches risk severe compromise to the delicate posterior blood supply of the distal fragment and are generally discouraged in the pediatric population.
Incision and Superficial Dissection
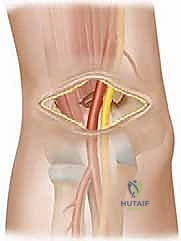
Once the patient is prepped, draped, and the sterile tourniquet is inflated, the surgical approach commences. A transverse incision is made directly across the antecubital fossa, following the natural skin creases to ensure an optimal cosmetic outcome.
TECH FIG 1 • A. Placement of a transverse incision for treatment of supracondylar fracture.
The incision is deepened through the subcutaneous tissue and fat using blunt dissection to avoid inadvertent injury to superficial structures. The surgeon must remain hyper-vigilant during this stage, as the severe trauma of the fracture can distort normal anatomic planes. The neurovascular bundle may be displaced from its anatomic bed and lie immediately beneath the subcutaneous tissue, putting it at extreme risk during careless initial dissection.

TECH FIG 1 • B. Incision through subcutaneous tissue and fat.
Deep Dissection and Neurovascular Management
As the dissection proceeds deeper, the surgeon will typically encounter the proximal metaphyseal spike of the humerus. This spike is often covered by a thin layer of torn brachialis muscle fibers and hemorrhagic periosteum.
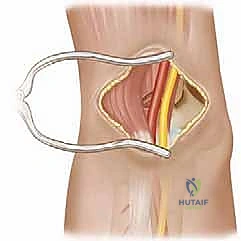
TECH FIG 1 • C. Deepening of incision with fracture site exposed.
Before any reduction maneuvers are attempted, the neurovascular bundle must be definitively located and protected. This step is absolute and must never be omitted, even in the absence of preoperative vascular compromise. The median nerve and brachial artery are typically found stretched over the anterior aspect of the proximal metaphyseal fragment. The lacertus fibrosus may need to be divided to relieve tension on these structures. Once identified, the neurovascular bundle is gently mobilized and retracted medially or laterally out of the surgical field using vessel loops or blunt retractors.
Fracture Reduction Maneuvers
Defining the outline of the distal fragment is frequently the most challenging aspect of the open reduction. Due to the extension-type mechanism, the distal fragment is displaced posteriorly and laterally, and the anterior periosteum is often folded over its articular surface, obscuring it from direct view.
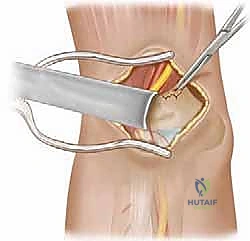
TECH FIG 2 • A. Proximal fragment retracted to try to expose distal fragment.
The classic impediment to reduction is the buttonholing of the proximal fragment through the anterior periosteum and brachialis muscle.

TECH FIG 2 • B. Sagittal view of fracture with proximal fragment shown buttonholing though muscle and periosteum.
To achieve reduction, the surgeon inserts a hemostat or a curved periosteal elevator into the fracture site to grasp the cut edge of the entrapping periosteum. Using heavy scissors, the surgeon extends the cut edge of the periosteum to widen the buttonhole. This critical release frees the tethered distal fragment. The surgeon then applies longitudinal traction to the forearm with the elbow flexed at 90 degrees while simultaneously applying direct downward pressure on the proximal fragment. The distal fragment is translated anteriorly and levered onto the proximal shaft, restoring the anatomic alignment of the medial and lateral columns.
Pinning and Fixation Strategy
Once anatomic reduction is achieved and visually confirmed, the fracture must be rigidly stabilized. The fixation strategy mirrors that of closed reduction, utilizing smooth Kirschner wires (typically 0.062-inch). The surgeon must ensure that the pins engage both the medial and lateral columns of the distal fragment to provide adequate rotational and bending stability.
The preferred configuration is the placement of three widely divergent, lateral-entry pins. The pins are introduced through the lateral epicondyle, traversing the fracture site, and engaging the dense cortical bone of the medial proximal fragment. The surgeon must maximize the separation of the pins at the fracture site; convergent or closely clustered pins provide inferior biomechanical stability and risk loss of reduction. If lateral-only pinning is deemed unstable, a medial entry pin can be added to create a cross-pinning construct. However, medial pinning carries a documented risk of iatrogenic ulnar nerve injury. If a medial pin is utilized, the ulnar nerve must be definitively palpated or visualized, and the pin should be placed with the elbow in relative extension to allow the nerve to fall posteriorly away from the medial epicondyle. Following satisfactory fluoroscopic confirmation of pin placement and fracture alignment, the pins are bent, cut outside the skin, and the incision is closed in layers.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, open reduction of supracondylar fractures carries a risk profile that surgeons must be prepared to manage. Complications can arise from the initial traumatic insult or as iatrogenic consequences of the surgical intervention itself. Understanding the pathophysiology of these complications is essential for early recognition and effective salvage management.
Neurovascular injury is the most feared complication. Traumatic neuropraxias, particularly of the anterior interosseous nerve, are common but typically resolve spontaneously over 3 to 6 months. Iatrogenic nerve injuries, however, are devastating. The ulnar nerve is highly susceptible to injury during medial pin placement if blind percutaneous techniques are used or if the elbow is pinned in hyperflexion, which subluxates the nerve anteriorly. If an iatrogenic nerve injury is recognized postoperatively, early exploration and pin revision are mandated. Vascular compromise, if not adequately addressed during the open reduction, can lead to compartment syndrome.
Compartment syndrome of the forearm, leading to Volkmann ischemic contracture, is a catastrophic complication. The most reliable early clinical sign in a pediatric patient is increasing pain that is out of proportion to the injury, coupled with an escalating requirement for narcotic pain medication. Crucially, children who have sustained a concomitant median nerve injury may not complain of ischemic pain due to the profound sensory deficit in the hand. Therefore, serial, meticulous physical examinations, assessing for pain with passive extension of the fingers, are mandatory. If compartment syndrome is suspected, emergent fasciotomies of the forearm and arm must be performed without delay.
Malunion, specifically cubitus varus (the "gunstock deformity"), is the most common late complication of supracondylar fractures. Cubitus varus results from a failure to correct coronal plane medial impaction or from a loss of fixation leading to internal rotation of the distal fragment. While primarily a cosmetic deformity that does not severely limit elbow range of motion, severe cases can lead to late-onset posterolateral rotatory instability or tardy ulnar nerve palsy. Salvage management for symptomatic or cosmetically unacceptable cubitus varus involves a corrective lateral closing-wedge or dome osteotomy of the distal humerus, performed after skeletal maturity or when the child is older.
| Complication | Incidence Rate | Pathophysiology & Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Iatrogenic Ulnar Nerve Injury | 2 - 4% (with medial pins) | Direct penetration or tethering by medial entry Kirschner wire. | Immediate pin removal/revision. Open exploration if deficit persists. |
| Compartment Syndrome | < 1% | Severe swelling, arterial spasm, or undiagnosed vascular injury leading to elevated fascial pressures. | Emergent volar and dorsal forearm fasciotomies. Epimysiotomy if needed. |
| Cubitus Varus (Malunion) | 3 - 5% | Failure to correct medial column collapse or internal rotation. Loss of pin fixation. | Observation if asymptomatic. Corrective valgus-producing osteotomy if severe. |
| Pin Track Infection | 1 - 2% | Superficial bacterial colonization of exposed Kirschner wires. | Oral antibiotics. Early pin removal if fracture is clinically healed. |
| Loss of Motion / Stiffness | 5 - 10% | Prolonged immobilization, severe soft tissue trauma, or intra-articular scarring. | Aggressive postoperative ROM protocols. Rarely requires surgical capsular release. |
Phased Post-Operative Rehabilitation Protocols
The postoperative care of a child following an open reduction of a supracondylar fracture requires a delicate balance between protecting the surgical fixation and preventing long-term elbow stiffness. Immediately following wound closure, sterile dressings are applied. A strip of Xeroform or similar non-adherent dressing is wrapped meticulously around the exposed pin sites to prevent skin tethering and reduce the risk of superficial pin track infections. This is followed by bulky, sterile fluff dressings to accommodate anticipated postoperative swelling.
The limb is then immobilized in a well-padded posterior splint. Crucially, the elbow must be splinted in 60 to 90 degrees of flexion with the forearm in neutral rotation. Hyperflexion of the elbow (greater than 90 degrees) is strictly contraindicated in the immediate postoperative period, as it significantly increases the pressure within the antecubital fossa and can precipitate vascular compromise or compartment syndrome. The patient is routinely admitted to the pediatric ward overnight for rigorous, serial neurovascular observations. Nursing staff must be instructed to monitor for signs of excessive pain, changes in capillary refill, or alterations in digital sensation.
If the overnight observation period is uneventful, the bulky splint can be transitioned to a more rigid long-arm cast the following day, maintaining the elbow at approximately 80 degrees of flexion. The patient is discharged with strict instructions for cast care and elevation of the extremity. The cast and the Kirschner wires are typically maintained for 3 to 4 weeks, depending on the patient's age and radiographic evidence of early callus formation. At the 3-to-4-week mark, the cast is bivalved, and the pins are removed in the outpatient clinic setting. Because the pins are left protruding through the skin, removal is generally well-tolerated without the need for additional anesthesia.
Following pin removal, the patient is transitioned into a soft sling for comfort and initiated on a phased rehabilitation program. For the first two weeks post-pin removal, the patient is encouraged to perform active, gentle range-of-motion exercises out of the sling multiple times a day. Passive stretching or forceful manipulation by physical therapists or parents is strictly contraindicated, as it can induce heterotopic ossification (myositis ossificans) and paradoxically worsen stiffness. It is vital to counsel the family that children treated with open reduction generally experience a longer duration of postoperative stiffness compared to those treated with closed pinning. However, formal physical therapy is rarely necessary, as the vast majority of children will spontaneously regain functional, and eventually full, range of motion through normal daily play and activities over the subsequent 3 to 6 months.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of supracondylar humerus fractures is heavily guided by a robust body of orthopedic literature. The debate surrounding the optimal timing of surgical intervention has been a focal point of recent research. Historically, prompt, emergent reduction was considered mandatory to prevent neurovascular sequelae. However, landmark studies by Leet et al. and Mehlman et al. have fundamentally shifted this paradigm. Their retrospective analyses demonstrated that delaying surgical treatment of Type III supracondylar fractures for up to 24 hours does not result in a statistically significant increase in the rates of open reduction, compartment syndrome, or iatrogenic nerve injury, provided the patient presents without acute neurovascular compromise. This has allowed institutions to optimize resource allocation and perform these complex procedures during standard operating hours.
The choice of surgical approach for open reduction has also been extensively evaluated. Ay et al. published critical findings supporting the transverse anterior cubital approach as the most effective and safe method for addressing displaced supracondylar fractures. Their work highlighted that the anterior approach provides superior visualization of the neurovascular bundle and the interposed brachialis muscle, facilitating a safer and more anatomic reduction compared to lateral or medial approaches. Reitman et al. further corroborated these findings, reporting excellent long-term functional outcomes in a large cohort of children treated with open reduction and internal fixation via the anterior approach, noting a 79% combined excellent and good outcome rate at mid-term follow-up.
Biomechanical literature heavily influences the current guidelines on pin configuration. Sankar et al. investigated the causes of loss of pin fixation and emphasized the critical importance of pin spread at the fracture site. Their biomechanical models and clinical reviews definitively showed that three widely divergent lateral pins offer comparable torsional and bending stability to crossed medial-lateral pins, while completely eliminating the risk of iatrogenic ulnar nerve injury. Consequently, clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) now strongly recommend the use of divergent lateral entry pins as the first-line fixation strategy, reserving medial cross-pinning strictly for fracture patterns that remain rotationally unstable after optimal lateral column fixation.
