Open Reduction & Internal Fixation of the Talus: An Operative Masterclass

Key Takeaway
This masterclass guides fellows through open reduction and internal fixation of talus fractures. We'll meticulously cover comprehensive surgical anatomy, critical preoperative planning, and granular intraoperative execution, emphasizing precise technique and rationale. Learn to navigate complex talar injuries, manage potential pitfalls, and optimize postoperative outcomes for these challenging fractures with significant avascular necrosis risk.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater and to this definitive masterclass. Today, we are undertaking an exhaustive review of a highly challenging, yet critically important injury in orthopedic traumatology: the displaced fracture of the talus. As practicing orthopedic surgeons, you are acutely aware that while these fractures are relatively uncommon—accounting for roughly 0.1% to 0.85% of all fractures and approximately 3% to 6% of all foot fractures—the consequences of mismanagement for ankle and hindfoot function are predictably devastating. Our objective here is not merely the mechanical fixation of a fractured bone; it is the absolute restoration of precise talar anatomy, the preservation of an intensely fragile vascular envelope, and the mitigation of catastrophic complications such as avascular necrosis (AVN) and post-traumatic arthrosis.
The patho-epidemiology of talar fractures is fundamentally linked to high-energy trauma. Historically termed "aviator's astragalus" due to its prevalence among early pilots crashing their biplanes, the modern equivalent is almost exclusively seen in severe motor vehicle collisions, motorcycle accidents, and falls from significant heights. The classic mechanism of injury for a talar neck fracture involves extreme hyperdorsiflexion of the foot combined with a massive axial load. In this scenario, the talar neck is driven violently against the sharp anterior lip of the tibial plafond, which acts as a fulcrum, causing the neck to fail in tension inferiorly and compression superiorly.
When this hyperdorsiflexion is coupled with a hindfoot supination force, the talar body is forced to subluxate or dislocate posteriorly and medially out of the mortise, frequently generating an associated medial malleolus fracture. The energy required to produce these fracture-dislocations is immense, meaning the talus fracture is rarely an isolated event. We must maintain a high index of suspicion for concomitant injuries, particularly fractures of the lumbar spine, tibial plateau, calcaneus, and the contralateral extremity. The soft tissue envelope surrounding the ankle is notoriously thin and unforgiving; thus, the initial trauma often results in severe contusions, fracture blisters, or open injuries that dictate our entire surgical timeline.
Understanding the gravity of this injury requires an appreciation of the talus's unique role in human bipedal locomotion. It is the mechanical keystone of the longitudinal arch, responsible for receiving the entire weight of the body from the tibial plafond and distributing it seamlessly to the calcaneus and the midfoot. Any incongruity in this complex load-bearing system alters contact stresses exponentially. Even a single millimeter of displacement or a few degrees of varus malunion in the talar neck can drastically reduce the contact area of the subtalar joint, leading inexorably to rapid, debilitating post-traumatic arthritis. Therefore, our surgical mandate is perfection.



Detailed Surgical Anatomy and Biomechanics
To successfully navigate the surgical management of the talus, one must possess an encyclopedic understanding of its unique osteology, its complex articular relationships, and, most importantly, its precarious extraosseous vascular supply. The talus is an anatomical anomaly; it is the second largest tarsal bone, yet it is completely devoid of any muscular or tendinous attachments. It functions entirely as an intercalated segment, a passive conduit for immense biomechanical forces transferring between the lower leg and the foot.
Osteology and Articular Surfaces
The talus boasts seven distinct articulations, and astonishingly, approximately 60% of its surface area is covered by hyaline articular cartilage. Superiorly, the talar dome (trochlea) articulates with the tibial plafond and the medial and lateral malleoli to form the highly constrained ankle (talocrural) joint. Inferiorly, the talus rests upon the calcaneus, forming the subtalar joint via three distinct facets: the large posterior facet, and the smaller middle and anterior facets. Anteriorly, the convex talar head articulates with the concave navicular, forming the talonavicular joint, which is the crucial ball-and-socket mechanism driving midfoot and hindfoot motion. The integrity of all these articular surfaces is paramount; any step-off or gap will act as a stress riser, destroying the joint over time.
Regional Anatomy of Talar Fractures
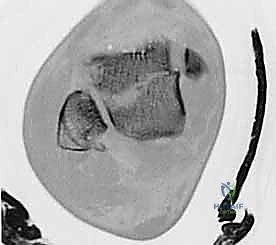
Fractures of the talus are broadly categorized by their anatomic location: the neck, the body, and the processes. The talar neck is the most frequent site of fracture. It is the anatomical waist of the bone, connecting the bulky body to the head. It deviates medially and plantarly, making it highly susceptible to bending and shear forces. Fractures here are typically in the coronal plane.
Talar body fractures involve the dome and extend into or posterior to the lateral process. These can present as sagittal, coronal, horizontal shear, or severe crush patterns. Because they directly involve the primary weight-bearing axis of the ankle and posterior subtalar joints, they carry an exceptionally high risk of articular incongruity and subsequent arthrosis.
Process fractures are often misdiagnosed as severe sprains. The lateral process fracture (snowboarder's fracture) is sustained by sudden inversion and dorsiflexion, often resulting in comminution or avulsion of the lateral talocalcaneal ligament. The posterior process features medial and lateral tubercles separated by the groove for the flexor hallucis longus (FHL) tendon. Fractures here (often the lateral tubercle, or Shepherd's fracture) result from forced plantarflexion and impingement against the posterior tibia.



The Vascular Achilles' Heel
The true peril of treating talus fractures lies in its vascular anatomy. Because there are no muscle attachments to provide collateral intraosseous perfusion, the talus relies entirely on an extraosseous anastomotic ring. The primary blood supply to the talar body comes from the artery of the tarsal canal, a major branch of the posterior tibial artery. This vessel courses laterally through the tarsal canal and enters the talar body through its inferior neck. Consequently, any displaced fracture of the talar neck threatens to shear this critical vessel, setting the stage for AVN.
The secondary blood supply is derived from the deltoid branch of the posterior tibial artery, which supplies the medial aspect of the body. The dorsalis pedis artery and its branches (the artery of the tarsal sinus) supply the head, neck, and lateral body. An anastomosis between the peroneal artery and the dorsalis pedis forms the lateral tarsal sinus artery, contributing to the lateral supply. During our surgical approaches, we must act as meticulous stewards of this remaining vascularity. The anteromedial approach places the deltoid branch at risk, while the anterolateral approach endangers the branches of the dorsalis pedis. Stripping the soft tissues blindly is a guaranteed path to iatrogenic avascular necrosis.
Exhaustive Indications and Contraindications
The surgical decision-making process for talus fractures is governed by a strict adherence to the principles of articular congruity and biomechanical alignment. The threshold for operative intervention is exceptionally low. In the modern era of orthopedic traumatology, almost all displaced fractures of the talar neck, body, or processes warrant Open Reduction and Internal Fixation (ORIF).
Non-operative management is strictly reserved for truly non-displaced fractures. However, plain radiographs are notoriously unreliable for confirming a lack of displacement. A fracture that appears non-displaced on an AP and lateral X-ray may demonstrate 2-3 millimeters of translation or varus angulation on a high-resolution CT scan. Therefore, the diagnosis of a "Hawkins Type I" (non-displaced talar neck fracture) can only be definitively made after a comprehensive CT evaluation. If any displacement is identified, the injury is immediately reclassified as a Hawkins Type II, and surgical fixation is indicated.
The timing of surgery has undergone a significant paradigm shift. Historically, displaced talus fractures were considered absolute surgical emergencies, driven by the belief that immediate reduction was necessary to "un-kink" the remaining blood supply and prevent AVN. However, landmark literature by Vallier et al. has demonstrated that delayed fixation (waiting for optimal soft tissue conditions) does not increase the rate of AVN, provided that any gross dislocation of the joints is urgently reduced in the emergency department. Therefore, we now operate on a "urgently optimized" schedule, allowing severe swelling to subside to minimize wound complications.
| Indications for ORIF | Contraindications to ORIF |
|---|---|
| Displaced Talar Neck Fractures (Hawkins II, III, IV) | Truly non-displaced fractures (Hawkins I) confirmed by CT |
| Displaced Talar Body Fractures (>1-2mm step-off) | Severe, prohibitive soft tissue compromise (e.g., active fracture blisters over planned incisions) |
| Displaced Lateral or Posterior Process Fractures | Active, untreated local soft tissue infection |
| Open Fractures (Requires urgent debridement and stabilization) | Non-ambulatory patient or severe medical comorbidities precluding anesthesia |
| Talar dislocations with skin tenting or neurovascular compromise (Emergent) | Severe osteopenia where hardware purchase is impossible (Relative) |
Pre-Operative Planning, Templating, and Patient Positioning
Before we ever approach the scrub sink, meticulous preoperative planning must be executed. This is not a fracture that can be "figured out" intraoperatively. The surgeon must possess a precise, three-dimensional understanding of the fracture morphology, a clear strategy for the surgical approach, and a backup plan for severe comminution.
Clinical Evaluation and Soft Tissue Assessment
The initial evaluation begins with a rigorous assessment of the soft tissue envelope. We utilize the Tscherne classification for closed injuries to document the degree of swelling, ecchymosis, and the presence of fracture blisters. Severe swelling, particularly common in high-energy Hawkins Type III and IV fractures, often precludes immediate definitive surgery. In these cases, the extremity is temporarily splinted or placed in a spanning external fixator until the "wrinkle sign" appears, indicating that the soft tissues can safely tolerate an incision. A comprehensive neurovascular examination is non-negotiable. Tibial nerve dysfunction or vascular compromise can occur, particularly with posterior dislocations of the talar body, and must be documented immediately.
Advanced Imaging and 3D Templating
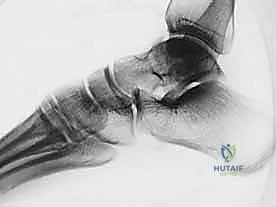
Plain radiographs remain our initial diagnostic workhorse. A standard ankle series (AP, mortise, and lateral) and foot series (AP, oblique, and lateral) are mandatory. The lateral view is critical for assessing the sagittal alignment of the talar neck and body. We also utilize the specialized Canale view to assess for varus or valgus malalignment of the talar neck. To obtain this view, the knee is flexed, the foot is placed in equinus and everted, and the X-ray tube is directed 15 degrees caudad. This view is indispensable both preoperatively and intraoperatively to confirm anatomic reduction.
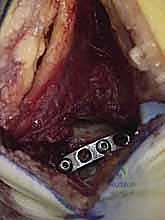
However, Computed Tomography (CT) is the absolute gold standard and is non-negotiable for any suspected talus fracture. Fine-cut (1mm) axial, sagittal, and coronal reconstructions provide invaluable data regarding the fracture pattern (coronal vs. sagittal split), the degree of comminution (especially medial neck comminution, which predictably leads to varus malunion), and the presence of intra-articular step-offs. We utilize these CT images for digital templating, determining the optimal trajectory for our lag screws and deciding whether supplemental mini-fragment plate fixation will be necessary to buttress areas of severe comminution.



Patient Positioning and Operating Room Setup
The patient is typically positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral, straight-up position, which greatly facilitates the anterolateral approach. A sterile thigh tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying small articular fragments and protecting delicate neurovascular structures. The C-arm fluoroscopy unit is positioned on the contralateral side of the table, ensuring unimpeded access for AP, lateral, and Canale views throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of a displaced talar neck or body fracture demands exceptional technical precision. The contemporary standard of care strongly favors a dual-incision technique—utilizing both anteromedial and anterolateral approaches. Historically, single incisions were used, which frequently resulted in a failure to recognize contralateral comminution, leading inevitably to varus or valgus malunion. By opening both sides, we achieve a panoramic view of the fracture, allowing for direct, anatomic reduction of the articular surfaces.
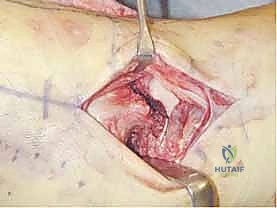
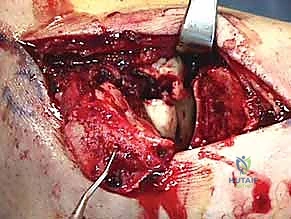
The Anteromedial and Anterolateral Approaches
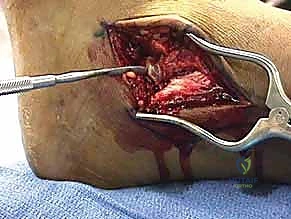
The anteromedial approach is initiated with an incision centered between the tibialis anterior tendon and the anterior border of the medial malleolus. Dissection is carried down carefully to avoid the saphenous nerve and vein. The capsule of the talonavicular joint is incised, exposing the medial aspect of the talar neck and head. It is absolutely critical during this approach to preserve the deep deltoid ligament inferiorly, as this structure protects the delicate deltoid branch of the posterior tibial artery—often the only remaining blood supply to the talar body. If the fracture extends deep into the talar body, a medial malleolar osteotomy (typically a chevron type) may be required to achieve adequate visualization of the talar dome.
The anterolateral approach is performed via an incision in line with the fourth ray, positioned lateral to the extensor digitorum longus tendon and medial to the fibula. We must be acutely aware of the superficial peroneal nerve branches (intermediate and medial dorsal cutaneous nerves) crossing this field. Deep dissection exposes the lateral aspect of the talar neck, the anterior process of the calcaneus, and the crucial subtalar joint.




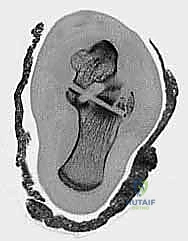
Fracture Reduction Techniques
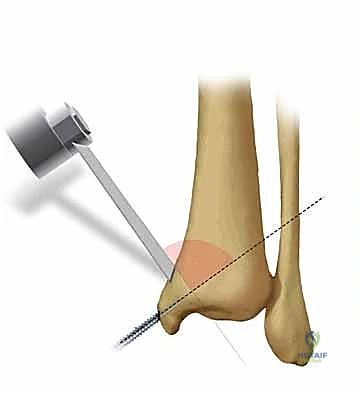
Once exposed, the fracture site is meticulously debrided of hematoma and interposed soft tissue or periosteum. Reduction of the talus is often exceedingly difficult due to its geometry and lack of levers. We frequently utilize 2.0mm or 2.5mm Schanz pins or threaded Kirschner wires placed strategically into the talar head and the talar body. These act as "joysticks," allowing the surgeon to manipulate the fragments in three dimensions.
Reduction must be assessed at three distinct cortical read points: the medial neck, the
Clinical & Radiographic Imaging Archive