Open Reduction and Internal Fixation of Pediatric Lateral Condyle Humerus Fractures: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for a masterclass on open reduction and internal fixation of pediatric lateral condyle humerus fractures. We'll meticulously cover surgical anatomy, preoperative planning, granular intraoperative execution, critical pearls and pitfalls, and comprehensive postoperative management, ensuring optimal outcomes for these challenging injuries.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a masterclass on a ubiquitous yet notoriously unforgiving pediatric injury: the displaced lateral condyle fracture of the humerus. This is a critical pathology for any practicing orthopedic surgeon to master, as these fractures represent approximately 10% to 15% of all pediatric elbow fractures, ranking second only in frequency to supracondylar humerus fractures. Our overarching surgical objective is immutable: to restore absolute articular congruity and meticulously maintain physeal integrity, thereby ensuring optimal long-term biomechanical function in these growing patients.
The pathogenesis of the lateral condyle fracture is a subject of classical orthopedic debate, primarily revolving around two distinct mechanistic theories. The "pull-off" theory, originally championed by Wadsworth, posits that an avulsion force is generated by the extensor musculature and the lateral collateral ligament complex. This typically occurs when a varus stress is applied to an extended, supinated forearm, causing the robust soft tissue attachments to avulse the lateral condylar fragment. Conversely, the "push-off" theory suggests that an axial load, combined with a valgus force transmitted through the radial head, directly shears the lateral condyle from the distal humerus. In clinical reality, a combination of these forces is often at play, dictating the ultimate fracture pattern and degree of displacement.
It is absolutely critical for the operating surgeon to recognize that even seemingly nondisplaced fractures can harbor profound occult instability. These fractures frequently hinge on a seemingly intact bridge of articular cartilage, offering a deceptive and highly precarious sense of stability. This cartilage hinge can swiftly unravel with minimal physiological stress, or degrade over time if the articular surface has been microscopically violated or if significant surrounding soft tissue injury is present. Consequently, what presents as a benign, nondisplaced fracture in the emergency department can rapidly evolve into a displaced, surgically demanding lesion within days.
The epidemiological peak for this injury occurs in children between the ages of four and ten years. This age distribution corresponds to a period of rapid ossification and high physical activity, making the distal humeral physis particularly vulnerable to shear and avulsion forces. Understanding the nuances of this epidemiology and the underlying biomechanical forces is the first step in approaching these fractures with the requisite respect and surgical precision. Failure to achieve anatomical reduction inevitably leads to a cascade of devastating long-term complications, underscoring the absolute necessity for mastery of this operative technique.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the distal humerus and its enveloping soft tissue envelope is paramount for successful surgical intervention. The lateral condyle is a complex, multi-tissue structure comprising the capitellum (the primary hemispherical articulation with the radial head) and a significant portion of the lateral metaphysis. Proximally, these fracture lines almost invariably originate in the posterolateral metaphysis. The fracture then propagates distally along the physis (the growth plate) before taking an abrupt turn to exit through the epiphysis.
Osteology and Physeal Architecture
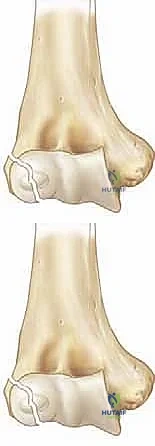
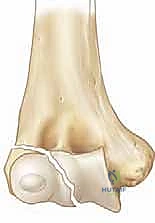
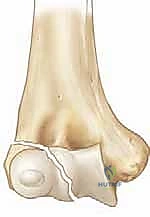
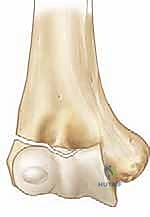
The precise location where the fracture line exits the epiphysis forms the basis of the classic Milch classification, which has profound biomechanical implications. In a Milch Type I fracture, the line traverses the metaphysis and physis, then extends directly across the ossific nucleus of the capitellum. This is functionally analogous to a Salter-Harris type IV fracture. While less common, it strictly involves the lateral aspect of the joint. In contrast, the much more common Milch Type II fracture extends from the metaphysis, travels along the physis, and exits medially through the unossified trochlear groove, medial to the capitellar ossification center.

The Milch Type II pattern is inherently and significantly more unstable. By exiting through the apex of the trochlea, the fracture effectively destabilizes the lateral trochlear ridge. This ridge is the primary osseous buttress preventing lateral translation of the radioulnar complex. When this buttress is compromised, the entire forearm is permitted to subluxate laterally, carrying the fractured condylar fragment with it. Radiographically, a Milch Type II may deceptively resemble a Salter-Harris type II injury, but its intra-articular extension makes it functionally akin to a Salter-Harris type III or IV, demanding meticulous anatomical reduction.
Surgical Warning: The distal humeral physis is an exquisitely delicate structure, and the vascularity to the lateral condylar epiphysis is tenuous. Any iatrogenic damage to the physis, particularly through aggressive retraction or ill-placed fixation, can initiate a premature growth arrest. A lateral physeal arrest predictably results in a progressive cubitus valgus deformity. Furthermore, if central physeal damage occurs, the patient is at high risk for developing a "fishtail" deformity of the distal humerus, leading to early-onset osteoarthritis and mechanical impingement.
Musculoligamentous Restraints and Vascularity
The distal fragment we are tasked with reducing typically retains robust and clinically significant soft tissue attachments. The origins of the Extensor Carpi Radialis Longus (ECRL), Extensor Carpi Radialis Brevis (ECRB), and the supinator muscle exert a continuous distal and rotational pull on the fragment. Furthermore, the Lateral Collateral Ligament (LCL) complex—comprising the radial collateral ligament, the annular ligament, and the lateral ulnar collateral ligament (LUCL)—remains firmly attached. This complex provides crucial posterolateral rotatory stability to the elbow.
These retained muscular and ligamentous attachments are a double-edged sword. Mechanically, they make the fragment highly resistant to closed reduction maneuvers and predispose it to severe rotational displacement, often flipping the articular surface out of the joint entirely. However, biologically, these attachments are the sole lifeline of the fragment. The blood supply to the lateral condyle enters predominantly through its posterior non-articular surface via vessels running within these soft tissue attachments.
Clinical Pearl: The absolute cardinal rule of lateral condyle fracture surgery is the preservation of the posterior soft tissue hinge. We must meticulously avoid any excessive stripping of the soft tissues on the posterior aspect of the lateral condyle. Aggressive posterior dissection will inevitably devascularize the fragment, leading to avascular necrosis (AVN), nonunion, and catastrophic failure of the procedure. All joint visualization and fracture clearing must be performed from an anterior perspective.
Neurovascular Topography
While isolated lateral condyle fractures rarely present with acute neurovascular compromise—a stark contrast to their supracondylar counterparts—the operating surgeon must maintain a hyper-vigilant awareness of the surrounding neurovascular topography. The radial nerve courses anterior to the lateral epicondyle, dividing into its superficial sensory branch and the deep motor branch (the posterior interosseous nerve, or PIN). The PIN wraps intimately around the radial neck within the supinator muscle.
Our standard lateral surgical approach typically remains proximal and superficial to the PIN, but extreme care is warranted during deep distal dissection or when placing retractors. The ulnar nerve, located in the cubital tunnel posterior to the medial epicondyle, is not directly in our surgical field during a lateral approach. However, its anatomical relevance becomes paramount in the setting of complications. A malunited lateral condyle fracture that progresses to a severe cubitus valgus deformity will chronically stretch the ulnar nerve, leading to tardy ulnar nerve palsy years or even decades after the initial injury.
Finally, the brachial artery and median nerve course anteriorly in the antecubital fossa. While far from the lateral column, overly aggressive medial retraction of the anterior soft tissue envelope can inadvertently compress or stretch these structures. Gentle, precise retractor placement, utilizing instruments like baby Hohmanns or Ragnell retractors placed carefully on bone, is essential to protect the anterior neurovascular bundle while achieving adequate visualization of the joint surface.
Exhaustive Indications and Contraindications
The decision-making algorithm for pediatric lateral condyle fractures is dictated almost entirely by the degree of displacement, the integrity of the articular surface, and the stability of the fracture pattern. Because the distal humerus is largely cartilaginous in young children, plain radiography often underestimates the true extent of displacement and articular incongruity. Therefore, a high index of suspicion and a low threshold for operative intervention are required to prevent the dismal natural history of a neglected displaced fracture.
The universally accepted threshold for surgical intervention is >2 mm of displacement on any radiographic view. Fractures displaced greater than 2 mm have a notoriously high rate of nonunion and subsequent deformity if treated nonoperatively. The synovial fluid within the joint bathes the fracture site, inhibiting the formation of a provisional fracture callus, making rigid mechanical stabilization an absolute biologic necessity for union. Furthermore, any evidence of rotational displacement, regardless of the absolute translation in millimeters, is an absolute indication for open reduction, as closed reduction of a rotated fragment is virtually impossible.
Defining Operative Thresholds
| Parameter | Indication for Operative Fixation (ORIF/CRPP) | Indication for Nonoperative Management (Casting) |
|---|---|---|
| Displacement | > 2 mm on AP, Lateral, or Internal Oblique view | < 2 mm on all radiographic views |
| Articular Surface | Incongruous, disrupted cartilage hinge | Congruous, intact cartilage hinge (verified) |
| Rotation | Any degree of rotational malalignment | No rotation |
| Stability | Unstable on stress examination under anesthesia | Stable on stress examination under anesthesia |
| Presentation | Acute or subacute (< 3 weeks) | Acute, strictly nondisplaced |
Contraindications to acute open reduction and internal fixation are relatively few but clinically significant. The most prominent contraindication is a late presentation (typically defined as greater than 3 to 4 weeks post-injury) of a displaced fracture. In these delayed scenarios, the fragment is often encased in dense, fibrotic callus, and the articular surface may have already undergone remodeling. Attempting a forceful open reduction in a late-presenting case requires extensive soft tissue stripping, which drastically increases the risk of avascular necrosis of the capitellum.

In cases of late presentation with established nonunion but minimal symptoms, many academic surgeons advocate for benign neglect or a delayed in situ stabilization rather than a heroic, devascularizing anatomical reduction. Another relative contraindication is the presence of severe, active local soft tissue infection or massive fracture blistering that precludes a safe surgical incision. In such cases, a period of temporizing immobilization and intravenous antibiotics may be required until the soft tissue envelope is optimized for surgical intervention.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful surgical outcome. The operative strategy begins long before the patient enters the theater. It requires a meticulous synthesis of the patient's history, a detailed physical examination, and a comprehensive review of all available imaging modalities. The surgeon must anticipate the fracture pattern, the required trajectory of fixation, and the potential pitfalls specific to the patient's anatomy.
Clinical Evaluation and Diagnostic Imaging
The clinical evaluation must be gentle yet exhaustive. Most patients present with localized swelling, ecchymosis, and exquisite tenderness over the lateral aspect of the elbow following a fall. A palpable gap or distinct crepitus over the lateral condyle is pathognomonic for a displaced, unstable fracture. A rigorous neurovascular examination is mandatory, documenting the status of the radial, median, and ulnar nerves, as well as distal perfusion, prior to any intervention.

Standard radiographic evaluation must include true anteroposterior (AP), lateral, and internal oblique views of the elbow. The internal oblique view is particularly critical, as it profiles the lateral condyle and often reveals the maximum extent of displacement that may be obscured on standard AP and lateral projections. If the degree of displacement is equivocal (hovering around the 2 mm mark), advanced imaging or dynamic assessment is required.
While Magnetic Resonance Imaging (MRI) can definitively assess the integrity of the cartilaginous hinge, it is cumbersome, expensive, and often requires general anesthesia in pediatric patients. Therefore, the gold standard for equivocal cases is an intraoperative arthrogram combined with a dynamic stress examination under fluoroscopy. By injecting radiopaque dye into the joint, the surgeon can directly visualize whether the articular cartilage is breached. If the dye leaks through the fracture site, or if the fragment displaces under gentle varus stress, the fracture is deemed unstable and mandates fixation.
Patient Positioning and Operative Setup
Optimal patient positioning is crucial for unhindered access and seamless fluoroscopic imaging. The patient is placed supine on the operating table. The operative extremity is typically positioned on a radiolucent hand table. Some surgeons prefer to place the patient flush with the edge of the main operating table, utilizing an arm board, which allows the C-arm to come in parallel to the table for effortless AP and lateral imaging without repositioning the arm.

A sterile, well-padded non-sterile tourniquet is applied high on the brachium. Exsanguination with an Esmarch bandage is performed, and the tourniquet is inflated to the appropriate pediatric pressure (typically 100 mmHg above systolic blood pressure, or roughly 200-250 mmHg). The entire upper extremity is prepped and draped free, allowing for full, unrestricted range of motion of the elbow during the procedure.
The C-arm fluoroscopy unit should be positioned either parallel to the table or coming in from the head of the bed, depending on surgeon preference and room layout. The monitor must be placed directly in the surgeon's line of sight. Before making the incision, a "time out" is performed, and baseline fluoroscopic images are obtained to confirm the fracture pattern and plan the precise location of the incision.
Step-by-Step Surgical Approach and Fixation Technique
The operative execution requires a blend of delicate soft tissue handling and rigid mechanical stabilization. The goal is to achieve absolute anatomical reduction of the articular surface while preserving the precarious blood supply to the lateral condylar fragment.
The Direct Lateral Approach
We utilize a direct lateral approach to the elbow. An incision, approximately 3 to 5 centimeters in length, is made centered over the lateral epicondyle, extending proximally along the lateral supracondylar ridge and distally towards the radial head. The subcutaneous tissues are sharply divided, and hemostasis is achieved. The deep fascia is incised in line with the skin incision.

The interval for deep dissection is typically between the brachioradialis and extensor carpi radialis longus (ECRL) anteriorly, and the triceps posteriorly. Alternatively, some surgeons prefer the Kocher interval between the anconeus and the extensor carpi ulnaris (ECU) for more distal access, though the standard lateral approach is usually sufficient. The common extensor origin is identified. In displaced fractures, the fascia is often already torn, and the hematoma points the way to the fracture site.
The anterior aspect of the fracture is meticulously exposed. A periosteal elevator or a Freer elevator is used to gently sweep the anterior capsule and brachialis muscle off the distal humerus to visualize the metaphyseal fracture line and the joint surface. Crucially, no dissection is performed on the posterior aspect of the lateral condyle. The posterior soft tissue attachments must remain completely inviolate to preserve the vascularity of the fragment.
Articular Reduction and Provisional Fixation
Once the anterior aspect of the fracture is exposed, the joint must be thoroughly irrigated to evacuate the fracture hematoma. Small curettes or a dental pick are utilized to meticulously remove any interposed periosteum, organized clot, or small osteochondral debris that would block an anatomical reduction. Visualization of the articular surface is paramount; the surgeon must see the cartilage of the capitellum and the trochlea to ensure perfect congruity.
Reduction is achieved by manipulating the fragment using a combination of direct pressure and positioning of the arm. Often, supinating the forearm and applying a gentle varus stress can help unlock the fragment. A sharp dental pick or a small bone tenaculum can be used to carefully manipulate the metaphyseal portion of the fragment. The reduction is judged visually by assessing the articular cartilage anteriorly and the metaphyseal fracture line laterally.
Once anatomical reduction is visually confirmed, it is provisionally held in place. This can be done with a smooth K-wire used as a "joystick," or by having an assistant maintain pressure with a dental pick. The reduction is then rigorously verified under multi-planar fluoroscopy. The surgeon must scrutinize the AP, lateral, and oblique views to ensure there is no residual step-off, gap, or rotational malalignment.
Definitive Internal Fixation Constructs
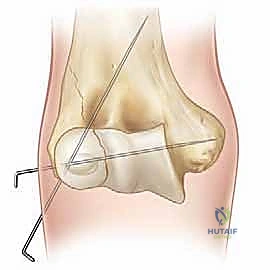
Definitive fixation is standardly achieved utilizing two or three smooth Kirschner wires (K-wires), typically 1.6 mm or 2.0 mm in diameter, depending on the size of the child. The trajectory of these wires is critical for biomechanical stability. The first wire is usually driven from the lateral epicondyle, directing it proximally and medially, aiming to engage the intact medial cortex of the distal humeral metaphysis.

The second wire should be placed divergently from the first to maximize rotational stability. A common and highly effective configuration is to place the second wire slightly more anteriorly and direct it more transversely across the distal humerus, aiming for the medial column above the olecranon fossa. It is imperative to avoid penetrating the olecranon fossa with the K-wires, as this will mechanically block elbow extension.

In older children or adolescents with a large metaphyseal fragment, a cannulated screw (typically 3.5 mm or 4.0 mm) can be utilized for compression across the metaphyseal fracture line, supplemented by a K-wire for rotational control. However, screws must never cross the physis. Once fixation is secure, the K-wires are bent, cut, and typically left protruding through the skin to facilitate easy removal in the clinic, although some surgeons prefer to bury them beneath the skin to reduce infection risk. The wound is then copiously irrigated and closed in layers.
Complications, Incidence Rates, and Salvage Management
The lateral condyle fracture is infamous for its complication profile, which is significantly higher than that of supracondylar fractures. These complications stem from the intra-articular nature of the injury, the tenuous blood supply, and the constant pull of the extensor musculature. A deep understanding of these pitfalls is essential for both prevention and salvage management.

Nonunion is perhaps the most dreaded complication, historically occurring in up to 15% of inadequately treated cases. It is almost exclusively the result of failing to stabilize a displaced fracture, allowing synovial fluid to continuously wash away the fracture hematoma. Established nonunions present a massive reconstructive challenge. Surgical salvage typically involves rigid internal fixation with bone grafting, but this carries a severe risk of precipitating avascular necrosis due to the necessary surgical dissection.
Biologic and Mechanical Failures
| Complication | Estimated Incidence | Pathophysiology & Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Lateral Spurring / Overgrowth | 40% - 70% | Hyperemia stimulating periosteal overgrowth laterally; often cosmetic rather than functional. | Reassurance; rarely requires excision unless symptomatic or causing mechanical block. |
| Nonunion | 1% - 15% (if missed) | Lack of mechanical stability; synovial fluid inhibiting callus formation. | In situ fixation vs. bone grafting and rigid ORIF (high risk of AVN). |
| Cubitus Valgus / Malunion | 5% - 10% | Premature lateral physeal arrest or initial malreduction. | Corrective supracondylar closing wedge osteotomy if deformity is severe. |
| Tardy Ulnar Nerve Palsy | Variable (Late) | Chronic stretching of the ulnar nerve due to progressive cubitus valgus deformity. | Ulnar nerve transposition; often combined with corrective osteotomy. |
| Avascular Necrosis (AVN) | < 2% (Acute) | Iatrogenic stripping of posterior soft tissue attachments during surgery. | Difficult salvage; joint leveling procedures or arthroplasty in adulthood. |
Malunion, typically presenting as a cubitus valgus deformity, occurs either due to a failure to achieve anatomical reduction at the time of surgery or secondary to a premature arrest of the lateral aspect of the physis. While a mild valgus deformity may be purely cosmetic, a severe deformity alters the biomechanics of the elbow and places chronic traction on the ulnar nerve.

Tardy ulnar nerve palsy is a classic, late-stage complication directly linked to cubitus valgus. As the carrying angle of the elbow increases over years of growth, the ulnar nerve is stretched taut across the medial epicondyle. Patients present years or decades later with intrinsic muscle weakness, clawing, and sensory deficits in the ulnar distribution. Management requires anterior transposition of the ulnar nerve, frequently combined with a corrective dome or closing-wedge osteotomy of the distal humerus to restore mechanical alignment.
Lateral condylar overgrowth, or spurring, is the most common complication, seen in the majority of operatively treated cases. It is believed to be a hyperemic response to the trauma and surgery, leading to excess periosteal bone formation laterally. While it can cause a noticeable cosmetic bump, it rarely restricts range of motion and typically remodels over time. Parents should be counseled preoperatively about this highly probable, yet generally benign, outcome.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation phase is designed to protect the delicate osteosynthesis while mitigating the inevitable stiffness associated with pediatric elbow trauma. Unlike adults, children are remarkably resilient to permanent joint stiffness, provided the intra-articular anatomy has been perfectly restored. Therefore, our initial focus is heavily weighted towards protection rather than aggressive mobilization.
Immobilization and Pin Management
Immediately following wound closure, the arm is placed in a well-padded, long-arm posterior splint or a bivalved cast, with the elbow immobilized at approximately 90 degrees of flexion and the forearm in neutral rotation. This position relaxes the extensor musculature, minimizing the distracting forces on the lateral condyle fragment. The patient is typically discharged on the same day or following a 23-hour observation period, depending on institutional protocols and the child's comfort level.

The patient is seen in the clinic at 7 to 10 days postoperatively for a wound check and radiographic evaluation to ensure maintenance of reduction. If the K-wires were left exposed, pin site care is reviewed with the family. The elbow remains strictly immobilized in the long-arm cast for a total of 3 to 4 weeks. At the 3-to-4-week mark, clinical healing is assessed. If radiographs demonstrate early bridging callus and the fracture site is non-tender, the K-wires are removed in the outpatient clinic setting.

Restoration of Range of Motion
Following pin removal, the cast is discontinued, and the child is transitioned to a removable splint or sling for comfort, to be weaned over the next 1 to 2 weeks. The cornerstone of the rehabilitation protocol is active, child-directed range of motion. We strongly advise against aggressive, passive physical therapy or forceful manipulation by parents or therapists, as this can induce heterotopic ossification, exacerbate stiffness, and cause unnecessary pain.

Children will naturally regain their range of motion through play and daily activities. We encourage activities like swimming or reaching for toys to facilitate extension and flexion. It is vital to counsel parents that full restoration of elbow extension can take several months—often up to 6 months—and that patience is required. Serial radiographs are obtained at 6 weeks, 3 months, and 6 months postoperatively to monitor for complete union, physeal health, and the potential development of lateral spurring or fishtail deformity.

Summary of Landmark Literature and Clinical Guidelines
The contemporary management of pediatric lateral condyle fractures is heavily informed by decades of rigorous orthopedic research and evolving clinical classifications. A thorough understanding of this landmark literature is essential for any academic surgeon defending their treatment rationale
Clinical & Radiographic Imaging Archive

