Ankle Mortise Restoration: An Intraoperative Masterclass in Bimalleolar ORIF

Key Takeaway
This masterclass details open reduction and internal fixation for bimalleolar ankle fractures. We cover essential anatomy, preoperative planning, and meticulous intraoperative execution from a surgeon's perspective. Learn precise techniques for fibular and medial malleolar fixation, including instrument use and hardware application. We emphasize neurovascular protection, fracture reduction pearls, and strategies for avoiding common pitfalls to ensure optimal patient outcomes and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
The Biomechanical Imperative of Mortise Restoration
Colleagues, the management of bimalleolar ankle fractures remains a cornerstone of orthopedic trauma surgery, yet it is a pathology that unforgivingly exposes technical inadequacies. The ankle is a highly constrained, modified hinge joint whose optimal function relies entirely on an anatomically congruent tibiotalar mortise. The biomechanical tolerance for error in this region is virtually nonexistent. Landmark biomechanical studies, notably the seminal work by Ramsey and Hamilton, demonstrated that a mere 1 millimeter of lateral talar shift results in a staggering 42% decrease in tibiotalar contact area. This exponential reduction in contact area dramatically increases peak articular contact stresses, inexorably driving the joint toward rapid, debilitating post-traumatic osteoarthritis if left uncorrected.
Our surgical mission extends far beyond the mere radiographic alignment of bone fragments; it is the meticulous restoration of the intricate biomechanical symphony of the ankle. The lateral malleolus acts as the primary buttress against lateral talar translation, while the medial malleolus and its robust deltoid ligament complex provide the essential medial restraint against valgus and external rotation forces. When both columns are disrupted, the talus becomes unmoored, leading to catastrophic joint instability. Restoration of fibular length, alignment, and rotation is the sine qua non of ankle mortise reconstruction, as the talus will faithfully follow the lateral malleolus.
Furthermore, the soft tissue envelope surrounding the ankle is notoriously thin and unforgiving. The interplay between osseous injury and the surrounding vascularity dictates not only our surgical timing but also our approach. A bimalleolar fracture is not merely a fracture of the tibia and fibula; it is a profound osteoligamentous disruption that demands a holistic understanding of joint kinematics. Failure to appreciate the nuanced interplay between the bony architecture and the syndesmotic and collateral ligaments will inevitably result in suboptimal functional outcomes, regardless of how aesthetically pleasing the postoperative radiographs may appear.
Pathoanatomy and the Lauge-Hansen Classification Framework
To truly master the surgical management of these injuries, one must thoroughly comprehend the mechanism of injury. The Lauge-Hansen classification remains an indispensable framework for understanding the sequential, predictable progression of osteoligamentous damage based on the position of the foot at the moment of impact and the deforming force applied. Unlike purely descriptive classifications, Lauge-Hansen provides a mechanistic roadmap that guides our intraoperative reduction maneuvers—essentially, we reverse the mechanism of injury to achieve anatomic reduction.

The most frequently encountered pattern in clinical practice is the Supination-External Rotation (SER) injury. In this mechanism, the foot is supinated, placing the lateral structures under tension, followed by an external rotation force. This predictably unfolds in four stages: Stage 1 involves the rupture of the anteroinferior tibiofibular ligament (AITFL). Stage 2 results in the classic short, oblique, or spiral fracture of the distal fibula, typically running from anteroinferior to posterosuperior. Stage 3 sees the force propagate posteriorly, causing a rupture of the posteroinferior tibiofibular ligament (PITFL) or, more commonly, an avulsion fracture of the posterior malleolus. Finally, Stage 4 culminates in the failure of the medial structures—either a transverse avulsion fracture of the medial malleolus or a rupture of the deep deltoid ligament. A bimalleolar SER fracture inherently represents a Stage 4 injury.
Conversely, the Pronation-External Rotation (PER) pattern initiates with the foot in pronation, tensioning the medial structures first. Stage 1 is a transverse medial malleolar fracture or deltoid rupture. Stage 2 involves rupture of the AITFL or an anterior syndesmotic avulsion (Chaput or Wagstaffe fragment). Stage 3 results in a high, short oblique or spiral fracture of the fibula above the level of the syndesmosis (suprasyndesmotic). Stage 4 is the posterior syndesmotic failure or posterior malleolar fracture. Recognizing these patterns is paramount; an SER fibula is reduced with internal rotation, whereas a PER fibula requires meticulous attention to restoring length and addressing the invariably disrupted syndesmosis.
Detailed Surgical Anatomy and Biomechanics
Osteology of the Distal Tibia, Fibula, and Talar Dome
Before making any incision, a profound, three-dimensional understanding of the regional osteology is mandatory. The distal tibia flares in the supramalleolar region, marking a critical transition from the dense, diaphyseal cortical bone to the structurally vulnerable metaphyseal cancellous bone. This transition zone dictates our fixation strategies, often necessitating the use of locking technology or specialized buttress plating when fracture lines extend proximally into the metadiaphysis.

The tibial articular surface, the tibial plafond, is a concave structure with distinct anterior and posterior lips that provide crucial sagittal plane stability. The posterior lip, or posterior malleolus, extends further distally than the anterior lip, acting as a primary restraint against posterior talar translation. The talar dome itself is uniquely wedge-shaped—approximately 2 to 3 millimeters wider anteriorly than posteriorly. This anatomical quirk is biomechanically vital; during ankle dorsiflexion, the wider anterior portion of the talus engages the mortise, tensioning the syndesmosis and conferring maximum osseous stability. Consequently, syndesmotic fixation must ideally be performed with the ankle in neutral or slight dorsiflexion to prevent over-compression and subsequent loss of motion.

The lateral malleolus, representing the distal extent of the fibula, is not merely a straight bone but possesses a distinct lateral bow and external rotation relative to the tibial shaft. It extends approximately 1 to 1.5 centimeters distal and slightly posterior to the medial malleolus. The medial articular facet of the lateral malleolus articulates with the lateral facet of the talus, forming a critical interface for load transfer and rotational stability. Anatomic restoration of the fibular bow and length is essential; shortening or malrotation of the fibula will invariably lead to a widened mortise and lateral talar shift.
The Syndesmotic Complex and Medial Osteoligamentous Structures
The structural integrity of the ankle mortise relies heavily on the syndesmotic ligament complex, the robust fibrous articulation uniting the distal tibia and fibula. This complex is composed of four distinct components: the anteroinferior tibiofibular ligament (AITFL), the posteroinferior tibiofibular ligament (PITFL), the inferior transverse ligament (a specialized deep component of the PITFL), and the interosseous ligament, which is the distal continuation of the interosseous membrane. The PITFL is the strongest of these ligaments, contributing the majority of the syndesmotic resistance to lateral fibular displacement.

Medially, the anatomy is equally complex. The medial malleolus consists of the anterior and posterior colliculi, separated by the intercollicular groove. The anterior colliculus extends further distally and serves as the origin for the superficial deltoid ligaments (tibionavicular, tibiocalcaneal, and superficial tibiotalar ligaments). The posterior colliculus, which is broader and more robust, along with the intercollicular groove, provides the origin for the deep deltoid ligament (deep anterior and posterior tibiotalar ligaments).

The deep deltoid ligament is the primary medial stabilizer of the ankle, resisting lateral talar excursion and external rotation. In bimalleolar equivalent fractures (isolated lateral malleolus fracture with a deep deltoid rupture), the deep deltoid is torn, rendering the joint highly unstable. When a medial malleolar fracture occurs, it often propagates through the supracollicular region or directly between the colliculi. Understanding the specific origins of these ligaments is crucial when placing lag screws into the medial malleolus; one must ensure the hardware adequately captures the specific colliculus associated with the primary stabilizing ligamentous structures.
Critical Neurovascular Topography
Surgical approaches to the ankle are fraught with potential neurovascular pitfalls that demand meticulous dissection techniques. Medially, the great saphenous vein and the accompanying saphenous nerve course superficially, passing anterior to the medial malleolus. These structures are highly vulnerable during the standard medial approach. Injury to the saphenous nerve can result in painful neuromas or troublesome paresthesias along the medial border of the foot, significantly impacting patient satisfaction.
Laterally, the superficial peroneal nerve is the primary structure at risk. It pierces the deep fascia of the lateral compartment to become superficial approximately 7 to 10 centimeters proximal to the distal tip of the fibula. As it descends, it crosses the surgical field anteriorly. When extending the lateral incision proximally for high fibular fractures or when utilizing minimally invasive plate osteosynthesis (MIPO) techniques, the superficial peroneal nerve must be explicitly identified and protected.
Proximally and anteriorly, the deep peroneal nerve and anterior tibial artery traverse the anterior compartment, coursing over the anterior capsule of the ankle joint. While less commonly encountered in standard bimalleolar approaches, they are at risk during anterior approaches or when placing anterior-to-posterior syndesmotic or posterior malleolar screws. Posteriorly, the tibial nerve and posterior tibial artery reside within the tarsal tunnel, protected by the flexor retinaculum. Aggressive posterior retraction during medial malleolar fixation or errant drill bit penetration through the posterior cortex of the tibia can jeopardize these critical structures.
Exhaustive Indications and Contraindications
Decision Making in Bimalleolar Fractures
The overarching goal in the management of bimalleolar ankle fractures is the restoration of a stable, anatomically congruent joint to permit early mobilization and prevent post-traumatic arthrosis. Operative intervention is unequivocally indicated for any bimalleolar fracture exhibiting displacement, talar shift, or mortise widening on initial or stress radiographs. Even in cases where the fracture appears minimally displaced in a cast, the inherent instability of a two-column injury makes secondary displacement highly probable once swelling subsides.
Nonoperative management of true bimalleolar fractures is exceedingly rare and generally reserved for patients who are non-ambulatory at baseline or possess profound medical comorbidities that preclude safe administration of anesthesia. In these highly selected cases, strict immobilization in a well-molded, long-leg or short-leg cast with weekly radiographic surveillance is mandatory to monitor for insidious loss of reduction. However, the surgeon must clearly document the acceptance of a likely malunion and subsequent functional deficit.
The decision to operate must also carefully weigh the state of the soft tissue envelope. Severe fracture blisters, massive edema, or skin abrasions dictate a delay in definitive internal fixation. In such scenarios, the ankle should be temporarily stabilized in a well-padded splint or, if grossly unstable or dislocated, a spanning external fixator. Definitive ORIF should be delayed until the soft tissues have recovered, typically indicated by the return of skin wrinkles (the "wrinkle sign") and the resolution of fracture blisters, which may take 7 to 14 days.
Indications and Contraindications Table
| Category | Specific Condition | Rationale / Surgical Implications |
|---|---|---|
| Absolute Indications | Displaced bimalleolar fractures | Inherent instability; high risk of post-traumatic OA if left unreduced. |
| Talar subluxation / Dislocation | Requires immediate closed reduction; definitive ORIF necessary to restore mortise congruity. | |
| Open fractures | Requires emergent irrigation, debridement, and stabilization to prevent deep joint space infection. | |
| Syndesmotic widening | Indicates disruption of the tibiofibular articulation; requires reduction and stabilization. | |
| Relative Indications | Minimally displaced fractures in active patients | Operative fixation allows for early mobilization, preventing stiffness and muscle atrophy. |
| Bimalleolar equivalent fractures | Fibula fracture with deep deltoid rupture; requires fibular fixation to restore lateral buttress. | |
| Absolute Contraindications | Active infection at the surgical site | High risk of deep hardware infection and subsequent osteomyelitis. |
| Non-ambulatory patient | Risks of surgery (anesthesia, infection) outweigh the functional benefits of anatomic reduction. | |
| Uncorrectable severe peripheral arterial disease | High likelihood of catastrophic wound failure and potential need for amputation. | |
| Relative Contraindications | Severe, uncontrolled diabetes mellitus | Increased risk of infection, delayed wound healing, and Charcot neuroarthropathy. |
| Poor soft tissue envelope (blisters, severe edema) | Delay surgery until soft tissues recover (wrinkle sign) to minimize wound dehiscence. | |
| Severe osteoporosis | Hardware failure is common; requires specialized techniques (locking plates, augmentation). |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Radiographic Assessment
A rigorous preoperative protocol is the bedrock of a successful surgical outcome. The clinical evaluation must begin with a comprehensive assessment of the patient's physiologic reserve and local soft tissue integrity. The Tscherne classification of closed soft tissue injuries should be utilized to document the degree of contusion, blistering, and compartment tension. A meticulous neurovascular exam, documenting baseline sensory and motor function of the superficial peroneal, deep peroneal, sural, saphenous, and tibial nerves, is critical from both a clinical and medicolegal standpoint.

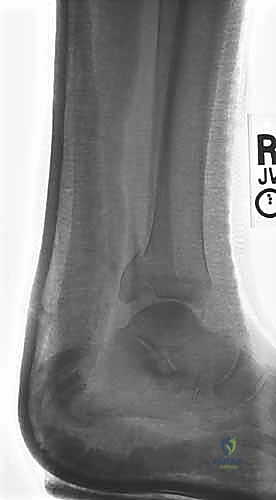
Standard radiographic evaluation consists of three dedicated views: the anteroposterior (AP), lateral, and mortise views. The mortise view, obtained with the leg internally rotated 15 to 20 degrees, profiles the entire tibiotalar articulation. We critically assess the medial clear space (normal ≤ 4mm), the superior clear space, and the tibiofibular overlap (normal > 1mm on mortise, > 6mm on AP). The lateral radiograph is scrutinized for posterior malleolar involvement, talar subluxation, and the specific fracture pattern of the fibula, which hints at the Lauge-Hansen mechanism.

In scenarios where a lateral malleolar fracture exists with medial tenderness but no obvious medial fracture (suspected bimalleolar equivalent), dynamic stress testing is essential. A manual external rotation stress radiograph or a gravity stress view will unmask deep deltoid incompetence, evidenced by a medial clear space widening of greater than 4 to 5 millimeters.


Advanced Imaging and Preoperative Templating
While plain radiography is sufficient for standard bimalleolar fractures, the threshold for obtaining a computed tomography (CT) scan should be low, particularly when posterior malleolar involvement is suspected or when the fracture configuration is highly comminuted. CT imaging provides unparalleled detail regarding articular impaction, the size and precise location of posterior malleolar fragments, and the presence of intra-articular loose bodies. This three-dimensional understanding fundamentally alters the surgical approach, often dictating the need for a posterolateral or posteromedial approach to address the posterior column directly.


Preoperative templating is an often-overlooked but vital step. Using digital templating software, the surgeon should anticipate the required plate length, screw trajectories, and potential areas of hardware conflict. For the fibula, determining whether a standard one-third tubular plate, a pre-contoured locking plate, or an antiglide construct will be utilized ensures that the appropriate inventory is available in the operating theater. Anticipating the trajectory of medial malleolar screws helps prevent joint penetration or intersection with planned syndesmotic screws.
Operating Room Setup and Patient Positioning
The patient is positioned supine on a radiolucent operating table to facilitate unimpeded fluoroscopic imaging. A well-padded bump is placed beneath the ipsilateral hip to internally rotate the lower extremity, bringing the lateral malleolus into a neutral, easily accessible position. This seemingly minor adjustment prevents the surgeon from constantly fighting the natural external rotation of the leg during fibular fixation.
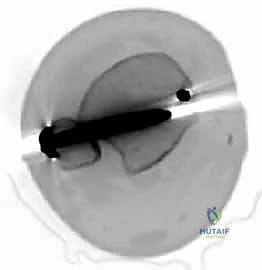
A pneumatic tourniquet is applied to the proximal thigh, well-padded with cast padding. The entire lower extremity, from the toes to the tourniquet, is meticulously prepped and draped free. This allows for full manipulation of the knee and ankle joints, enabling the surgeon to apply necessary traction, rotation, and stress maneuvers during the procedure. The fluoroscopy unit (C-arm) is typically positioned on the contralateral side of the table, entering perpendicular to the limb, allowing for rapid transition between AP, mortise, and lateral views without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The Lateral Approach and Fibular Osteosynthesis
The surgical sequence typically begins with the lateral malleolus, as restoring fibular length and rotation provides a template for reducing the talus and the medial side. A longitudinal incision is made centered over the fibula, curving slightly anteriorly at its distal extent to follow the contour of the bone. The dissection proceeds through the subcutaneous tissues, taking immense care to identify and protect the superficial peroneal nerve proximally and the sural nerve distally. The fracture hematoma is evacuated, and the fracture ends are meticulously debrided of interposed periosteum or soft tissue.


Anatomic reduction of the fibula is achieved using pointed reduction forceps. In typical short oblique or spiral fractures (SER patterns), an interfragmentary lag screw is placed perpendicular to the fracture plane to achieve absolute stability and interfragmentary compression. This is followed by the application of a neutralization plate, typically a one-third tubular plate or a pre-contoured locking plate, positioned laterally.
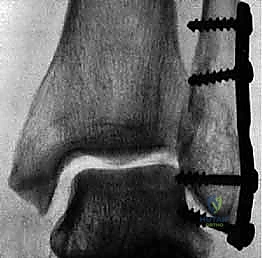

Alternatively, for specific oblique patterns, a posterior antiglide plate can be utilized. This biomechanically superior construct resists the proximal and posterior displacement forces acting on the distal fragment and often precludes the need for an independent lag screw, as the plate itself compresses the fracture as it is tensioned to the bone.



The Medial Approach and Malleolar Fixation
Once the lateral column is stabilized, attention is directed to the medial malleolus. A longitudinal or slightly curvilinear incision is made centered over the medial malleolus. The great saphenous vein and nerve are retracted anteriorly. The fracture site is exposed, and the periosteum is elevated minimally—
Clinical & Radiographic Imaging Archive