Limited Open Achilles Tendon Repair: An Intraoperative Masterclass with the Achillon Instrument

Key Takeaway
This masterclass guides fellows through a limited open Achilles tendon repair using the Achillon instrument. We cover meticulous preoperative planning, precise patient positioning, and detailed intraoperative execution from incision to closure. Emphasis is placed on comprehensive anatomy, neurovascular considerations, and the exact application of the Achillon device for robust tendon approximation, ensuring excellent functional outcomes and minimizing complications.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows and colleagues, to the operating theater. Today, we are undertaking a definitive exploration of a prevalent yet biomechanically critical injury: the acute rupture of the Achilles tendon. The procedure we will detail is the limited open repair utilizing the specialized Achillon instrument. This technique represents a highly refined, modern surgical approach that elegantly marries the biomechanical benefits of direct anatomical visualization with the profound biological advantages of minimized soft tissue disruption. Historically, the management of acute Achilles tendon ruptures has been heavily debated, oscillating between traditional, extensile open repairs—which carry a notoriously high risk of wound necrosis and deep infection—and purely percutaneous techniques, which risk sural nerve entrapment and potentially higher re-rupture rates due to non-anatomic apposition of the tendon stumps.
This limited open, or "mini-open," technique is specifically indicated for acute ruptures, optimally addressed within three weeks of the initial injury. The prime anatomical target for this instrumentation is a rupture occurring between 2.0 and 7.0 cm proximal to the calcaneal tuberosity. Epidemiologically, this specific topographic zone accounts for over 90% of all Achilles tendon ruptures. For pathological disruptions higher than 8 cm, which often involve the musculotendinous junction, we generally favor nonoperative functional management. Conversely, distal avulsions occurring less than 2 cm from the calcaneal insertion typically necessitate direct bony fixation utilizing suture anchors or transosseous tunnels, rendering the Achillon device less applicable.
The patho-epidemiology of Achilles tendon ruptures reveals a bimodal distribution, though it is most frequently encountered in the third to fifth decades of life. These injuries are ubiquitous among high-level athletes, "weekend warriors," and occasionally sedentary individuals. The classic presentation involves a sudden, highly audible "pop" or "snap" during a forceful eccentric contraction of the gastrocnemius-soleus complex—typically during forced ankle dorsiflexion with a contracted calf muscle, such as pushing off during a tennis match or basketball game. While most acute presentations represent complete transverse or oblique disruptions, partial injuries and intratendinous delaminations do occur and require astute clinical differentiation.
On physical examination, the clinician must maintain a high index of suspicion. Expect to identify moderate to severe localized edema posteriorly, accompanied by ecchymosis that may track distally toward the heel. The pathognomonic finding is a palpable, tender defect or "soft spot" typically situated 2.5 to 5 cm proximal to the calcaneal insertion. The Thompson squeeze test is universally positive, demonstrating an absence of passive plantarflexion when the calf muscle belly is compressed. Furthermore, patients will report a profound inability to perform a single-leg heel raise, and when placed in a prone position with the knees flexed to 90 degrees (Matles test), the affected ankle will demonstrate spontaneous, excessive resting dorsiflexion compared to the contralateral uninjured limb.
Detailed Surgical Anatomy and Biomechanics
A rigorous comprehension of the surgical anatomy and regional biomechanics is non-negotiable before making an incision. The Achilles tendon is the largest and strongest tendon in the human body, measuring approximately 9 to 15 cm in length and roughly 0.9 cm in cross-sectional diameter. It represents the distal confluence of the gastrocnemius and soleus muscle bellies. As the tendon descends toward its insertion on the posterior aspect of the calcaneal tuberosity, its fibers undergo a complex 90-degree internal rotation. This spiral configuration is biomechanically significant, as it provides viscoelastic properties that allow the tendon to store and release kinetic energy efficiently, while also distributing tensile forces more evenly across its cross-section.
Crucially, unlike many other tendons that are housed within a true synovial sheath, the Achilles tendon is enveloped by the paratenon. This highly vascularized, delicate connective tissue sheath functions as a gliding surface and is the primary source of extrinsic vascularization for the tendon. The blood supply to the Achilles is derived from three distinct sources: the musculotendinous junction proximally, the osseous insertion distally, and the paratenon via the mesotenon anteriorly. A critical clinical pearl is the existence of an intrinsic "watershed" area of profound hypovascularity located approximately 2.5 to 6 cm proximal to the calcaneal tuberosity. This hypovascular zone precisely correlates with the most common site of spontaneous rupture, underlining the biological vulnerability of this region and dictating the necessity for meticulous, tissue-sparing surgical techniques that preserve the paratenon.
Neurovascular Considerations
The primary neurovascular structure at risk during any Achilles tendon intervention is the sural nerve. Formed by the union of the medial sural cutaneous nerve and the sural communicating branch of the common peroneal nerve, it provides sensory innervation to the lateral and posterior aspect of the distal third of the leg, as well as the lateral aspect of the foot and fifth toe. The sural nerve courses distally along the posterolateral aspect of the calf, piercing the deep fascia approximately midway down the leg. It then runs superficially, intimately associated with the small saphenous vein, progressively crossing the lateral border of the Achilles tendon from medial to lateral at an average distance of 9.8 cm proximal to the calcaneal insertion.
Distally, the nerve lies in close proximity to the lateral border of the tendon. It is imperative to identify and protect this structure throughout the surgical approach. Iatrogenic injury to the sural nerve—whether via direct laceration, traction neuropraxia, or entrapment within a percutaneous suture—can lead to distressing paresthesias, painful neuromas, and significant postoperative morbidity. Our deliberate choice of a medial paratendinous incision is strategically designed to maximize the distance from the nerve's anticipated trajectory, thereby minimizing the risk of iatrogenic injury. However, anatomical variants are common, and constant intraoperative vigilance remains paramount.
Relevant Osteology and Biomechanics
The calcaneal tuberosity serves as our definitive distal bony landmark. While the limited open technique specifically targets mid-substance tendinous disruptions, it is incumbent upon the surgeon to rule out calcaneal avulsion fractures preoperatively via standard radiography. Biomechanically, the Achilles tendon must withstand immense forces; during normal walking, it experiences loads up to 3 times body weight, which can escalate to 10 times body weight during sprinting or jumping. Consequently, our surgical repair must not only achieve anatomical apposition to facilitate biological healing but must also possess sufficient immediate mechanical strength to withstand early postoperative resting tension and the forces introduced during early functional rehabilitation.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of surgical success. The limited open repair utilizing the Achillon system is not a panacea for all posterior heel pathology; its application must be strictly governed by established clinical parameters.
| Parameter | Indications for Limited Open Repair | Contraindications for Limited Open Repair |
|---|---|---|
| Chronicity | Acute rupture (intervention < 3 weeks from injury). | Chronic rupture (> 3-4 weeks), neglected tears. |
| Location | Mid-substance rupture (2.0 to 7.0 cm proximal to insertion). | Musculotendinous junction tears (> 8 cm); Calcaneal avulsions (< 2 cm). |
| Tear Morphology | Complete or high-grade partial acute traumatic ruptures. | Intratendinous degenerative tendinosis without acute frank rupture. |
| Soft Tissue Envelope | Intact, healthy overlying skin without significant abrasions. | Open ruptures, severe cellulitis, compromised skin (e.g., severe venous stasis). |
| Patient Factors | Active individuals, athletes, compliant patients capable of rehab. | Severe peripheral vascular disease, uncontrolled diabetes, heavy smoking history, systemic steroid dependence, non-ambulatory status. |
| Previous Surgery | Primary, virgin surgical field in the posterior ankle. | Prior Achilles tendon surgery, existing local hardware or severe scarring. |
The rationale behind these strict contraindications is deeply rooted in the biology of tendon healing. Chronic ruptures typically exhibit significant tendon retraction and fatty infiltration of the muscle belly, necessitating extensile exposures, V-Y fascial advancements, or flexor hallucis longus (FHL) tendon transfers to bridge the gap. Similarly, patients with profound microvascular compromise (diabetics, heavy smokers, chronic steroid users) are at an exponentially higher risk for catastrophic wound complications, making nonoperative management or vastly different surgical approaches more prudent.
Pre-Operative Planning, Templating, and Patient Positioning
Before the patient is transported to the operating theater, meticulous preoperative planning is essential to ensure a seamless intraoperative workflow.
Imaging Review and Templating
While a thorough history and physical examination are often sufficient to establish the diagnosis of an acute Achilles tendon rupture, standard plain radiographs (weight-bearing AP, lateral, and mortise views of the ankle) are mandatory in the traumatic setting. These films are scrutinized to rule out associated osseous pathology, particularly calcaneal avulsion fractures, posterior malleolar fractures, or significant calcific tendinopathy that might complicate the passage of the Achillon instrument or alter our fixation strategy.
Advanced imaging, such as high-resolution musculoskeletal ultrasound or Magnetic Resonance Imaging (MRI), is not universally required for acute, clinically obvious ruptures. However, if the diagnosis is equivocal, if the patient presents subacutely, or if a partial tear is suspected, MRI is invaluable. When reviewing advanced imaging, the surgeon must specifically evaluate the exact level of the rupture, the degree of tendon retraction (gap size), the presence of interstitial tendinosis in the remaining stumps, and the integrity of the plantaris tendon, which can sometimes masquerade as an intact Achilles on clinical exam.
Instrumentation: The Achillon System
Our primary surgical armamentarium for this procedure centers on the Achillon device (Integra LifeSciences). This specialized instrumentation is engineered specifically to facilitate a reproducible, mini-invasive repair.
* The device is available in both rigid polymer (single-use) and stainless steel (reusable) iterations.
* Its core function is to act as a precise stereotactic guide for the passage of sutures through the tendon stumps, ensuring robust core purchase while minimizing the need for extensive soft tissue dissection.
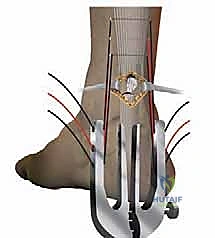
* The instrument features a pair of internal branches that are connected to external branches. Both sets of branches possess corresponding, aligned apertures. This geometry guarantees that a needle passed through an external aperture will perfectly traverse the tendon and exit the corresponding opposite aperture.
* The two internal branches are uniquely angled at 8 degrees relative to one another. This specific angulation anatomically mirrors the natural V-shape cross-section of the Achilles tendon, ensuring the device cups the tendon appropriately without causing iatrogenic crush injury.
* A micrometric screw mechanism at the base allows the surgeon to precisely adjust the opening width of the branches to accommodate varying tendon diameters and morphologies.
* The system utilizes specialized straight needles pre-loaded with high-tensile strength, non-absorbable polyblend sutures (e.g., #2 FiberWire or similar). A custom needle driver is employed, featuring a broadened support surface to facilitate pushing the needle through dense tendinous tissue while protecting the surgeon's gloves from accidental puncture.
Patient Positioning and Anesthesia
Optimal patient positioning is critical for surgical access, visualization, and the ability to assess intraoperative tendon tension accurately.
- Anesthesia: The procedure is typically performed under general anesthesia or a robust regional block (spinal or epidural) combined with a popliteal sciatic nerve block for postoperative analgesia. Prior to final positioning, an examination under anesthesia is performed to reconfirm the palpable defect and assess the degree of resting equinus.
- Prone Positioning: The patient is meticulously positioned prone on the operating table. All bony prominences—including the chest, iliac crests, patellae, and dorsal forefeet—must be heavily padded to prevent pressure necrosis and peripheral nerve palsies. The feet should extend just beyond the edge of the operating table to allow for unhindered, full-range manipulation of the ankle joint.
- Tourniquet Application: A well-padded pneumatic tourniquet is applied to the proximal thigh of the operative extremity. It is inflated strictly after exsanguination to provide a pristine, bloodless surgical field. This is vital for the delicate identification of the paratenon and the avoidance of the sural nerve.
- Preparation and Draping: Crucially, both lower extremities are prepped and draped into the sterile field. This bilateral exposure allows the surgical team to directly compare the resting Achilles tendon tension and the degree of spontaneous plantarflexion of the repaired limb against the contralateral, uninjured limb.
- Draping Caveat: We explicitly avoid the use of adhesive plastic draping (Ioban) directly over the posterior calf. Because this technique relies on percutaneous suture passes that exit the skin laterally and medially, plastic drapes can become entangled in the sutures or drawn into the subcutaneous tissues, creating a nidus for infection.
Step-by-Step Surgical Approach and Fixation Technique
We are now scrubbed, the tourniquet is inflated, and the bilateral field is secured. Our overarching objective is to achieve a biomechanically rigid, anatomically reduced repair while strictly adhering to the principles of soft tissue preservation.
Step 1: Incision Planning and Superficial Dissection
We begin by carefully palpating the posterior ankle to precisely localize the rupture gap. The incision is planned as a longitudinal, medial paratendinous approach, measuring approximately 2.0 to 3.0 cm in length, centered directly over the palpable defect. By placing the incision medially, we maximize our distance from the laterally coursing sural nerve.

A #15 blade is used to incise the skin and subcutaneous fat. Gentle retraction is applied using fine skin hooks or a small Weitlaner retractor. Meticulous hemostasis is achieved with bipolar electrocautery. The underlying paratenon, a glistening, thin fascial layer, is now visualized.
Step 2: Paratenon Management
The preservation of the paratenon is perhaps the most critical biological step of this operation. Using fine tenotomy scissors, the paratenon is carefully incised longitudinally, matching the length of the skin incision.

Immediately upon opening the paratenon, we place fine absorbable stay sutures (e.g., 3-0 Vicryl) on the medial and lateral edges of the sheath. These stay sutures allow us to elevate and retract the paratenon gently, creating a working corridor while protecting the tissue from crush injury caused by standard retractors. This ensures the sheath remains viable for a watertight closure at the conclusion of the case.
Step 3: Proximal Stump Capture and Suture Passage
With the paratenon open, the hematoma is evacuated, and the disorganized, "mop-end" fibers of the ruptured tendon are exposed. We identify the proximal and distal stumps.

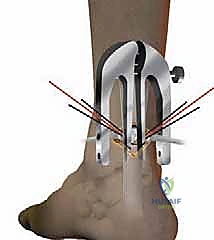
We begin with the proximal stump. The Achillon instrument, in its fully closed position, is introduced deep to the paratenon but superficial to the deep posterior compartment fascia, sliding proximally along the tendon.

Using an Allis or Babcock clamp, the proximal tendon stump is grasped and pulled distally, ensuring it is seated securely between the internal branches of the Achillon device.

The micrometric screw is then engaged, progressively widening the instrument's branches until they comfortably but snugly accommodate the tendon's girth.
The surgeon must verify the correct positioning by palpating the skin externally; the internal branches should be distinctly palpable on either side of the tendon, confirming that the tendon is captured and the sural nerve is safely excluded outside the device's footprint.

We now proceed with suture passage. Three specialized straight needles, armed with high-strength non-absorbable suture, are passed sequentially through the designated apertures of the external branches. The needle pierces the skin, traverses the external branch, passes through the tendon substance guided by the internal branch, and exits the contralateral side.

This creates a robust, multi-level core suture configuration within the proximal stump. Once all three sutures are passed, the needles are cut, and the Achillon instrument is carefully withdrawn, leaving the sutures traversing the proximal tendon and exiting the skin laterally and medially.
Step 4: Distal Stump Capture and Suture Passage
Attention is now turned to the distal stump. The process is repeated with meticulous care.

The Achillon instrument is inverted and directed distally toward the calcaneal insertion, again remaining deep to the paratenon. The distal stump is grasped and drawn proximally into the jaws of the device.
After confirming placement and ensuring the sural nerve is clear laterally, the distal sutures are passed through the corresponding apertures.

It is critical during the distal passage to angle the needles slightly to avoid striking the calcaneal tuberosity, particularly if the rupture is closer to the 2.0 cm distal limit of our indication. The instrument is then withdrawn.
Step 5: Suture Retrieval and Knot Tying
At this juncture, we have three sets of sutures exiting the skin proximally and three sets exiting distally.
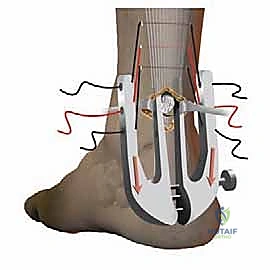
Using a small hemostat or a specialized suture retriever, the free ends of the sutures are systematically pulled from the percutaneous puncture sites back into the primary medial paratendinous incision. This step effectively transitions the percutaneous suture passes into a centralized location for tying, burying the knots deep to the paratenon.
The ankle is now placed into resting equinus (plantarflexion). The degree of plantarflexion is meticulously matched to the contralateral, uninjured limb to restore precise anatomical resting tension. The corresponding proximal and distal sutures are paired and tied securely using a surgeon's knot followed by multiple alternating half-hitches. The tension must be sufficient to appose the tendon ends without causing ischemic necrosis of the stumps.
Step 6: Paratenon and Skin Closure
With the tendon securely repaired, we focus on the biological closure.

The previously tagged paratenon is re-approximated using a fine, absorbable running suture (e.g., 4-0 Monocryl or Vicryl). This watertight closure is imperative; it restores the gliding surface, prevents adhesions to the overlying skin, and re-establishes the crucial vascular envelope around the healing tendon.

The subcutaneous tissues are closed in a standard fashion, followed by skin closure using either a running subcuticular stitch or interrupted nylon sutures, depending on surgeon preference and skin quality.

A sterile, non-adherent dressing is applied, and the limb is immobilized in a well-padded short-leg splint or a rigid cast in approximately 15 to 20 degrees of plantarflexion to protect the repair during the initial inflammatory phase of healing.
Complications, Incidence Rates, and Salvage Management
Despite the refined nature of the limited open Achillon technique, complications can and do occur. A thorough understanding of these risks is essential for informed consent and prompt postoperative management.
| Complication | Estimated Incidence (Limited Open) | Etiology & Clinical Presentation | Salvage / Management Strategy |
|---|---|---|---|
| Sural Nerve Injury | 1.5% - 3.0% | Iatrogenic percutaneous puncture, traction neuropraxia. Presents as lateral foot numbness, burning, or neuroma formation. | Observation for neuropraxia. Gabapentinoids. If severe neuroma develops, surgical excision and burying of the nerve stump into local muscle. |
| Re-Rupture | 2.0% - 4.5% | Early non-compliant weight-bearing, aggressive forced dorsiflexion, intrinsic biological failure. | Revision surgery often requires V-Y advancement, FHL transfer, or allograft reconstruction due to retracted, scarred stumps. |
| Superficial Infection | 1.0% - 2.5% | Minor wound dehiscence, suture abscess at percutaneous sites. | Local wound care, oral antibiotics targeting skin flora (Staph/Strep). Usually resolves without deep space involvement. |
| Deep Infection | < 1.0% | Contamination of the deep tendon space. Presents with severe pain, erythema, purulent drainage. | Aggressive surgical debridement, hardware/suture removal if necessary, targeted IV antibiotics. High risk of subsequent construct failure. |
| Tendon Elongation | 5.0% - 10.0% | Viscoelastic creep of the repair, tying knots in insufficient equinus. Presents as decreased push-off strength and increased resting dorsiflexion. | Prolonged physical therapy focusing on aggressive eccentric strengthening. Rarely requires surgical shortening unless functionally debilitating. |
| DVT / PE | 1.0% - 5.0% | Venous stasis from immobilization, prone positioning, tourniquet use. | Prophylactic anticoagulation (LMWH or Aspirin) based on patient risk profile. Therapeutic anticoagulation if DVT/PE is confirmed via Doppler US or CTPA. |
The incidence of sural nerve injury is significantly lower in limited open techniques compared to purely percutaneous methods (which can approach 10-15% in some series) because the medial incision allows for direct palpation and avoidance of the lateral structures. Similarly, the risk of catastrophic deep wound infection is drastically reduced compared to traditional extensile open repairs, highlighting the immense value of this hybrid approach.
Phased Post-Operative Rehabilitation Protocols
The evolution of Achilles tendon repair has seen a paradigm shift from prolonged rigid immobilization to early functional rehabilitation. While protocols vary by institution, the underlying principle is that controlled, early mechanical loading stimulates tenocyte proliferation, improves collagen fiber alignment, and reduces the incidence of debilitating adhesions.
Phase I: Maximum Protection (Weeks 0 - 2)
Immediately postoperatively, the patient is strictly non-weight-bearing. The limb is immobilized in a bulky Jones dressing with a posterior splint, or a rigid cast, locked in 15 to 20 degrees of equinus (plantarflexion). The primary goals during this phase are wound healing, edema control (elevation), and pain management. Deep vein thrombosis (DVT) prophylaxis is initiated per institutional guidelines.
Phase II: Early Mobilization and Progressive Weight-Bearing (Weeks 2 - 6)
At the two-week mark, the surgical incision is inspected, and sutures are removed. The patient is transitioned into a controlled ankle motion (CAM) boot fitted with multiple heel wedges (typically three wedges, elevating the heel by approximately 3 cm). Weight-bearing is progressively advanced from partial to full weight-bearing as tolerated, strictly utilizing the wed
