Open Reduction and Internal Fixation of Phalangeal Condylar Fractures: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for a masterclass on phalangeal condylar fracture fixation. We'll meticulously cover hand anatomy, precise reduction techniques, K-wire and screw application, and crucial intraoperative decision-making. Learn to manage complex patterns and prevent complications for optimal patient outcomes, ensuring early mobilization and functional restoration.
📄 Show Short Video Transcript
Phalangeal condylar fractures demand high anatomical precision due to the minimal tolerance for joint displacement. This surgical video outlines the step-by-step management of these injuries, focusing on preserving the delicate soft-tissue envelope and achieving stable internal fixation.
Key Topics Covered:
Pathomechanics: How axial loading and shear forces cause instability.
Anatomical Pitfalls: Avoiding subperiosteal stripping to protect the fragment's vascularity.
Fixation Technique: Utilizing the dorsal-lateral approach, ligamentotaxis, and miniature lag screws (1.0 to 1.5-millimeter).
Rehabilitation: Balancing rigid fixation with early active motion to prevent stiffness.
Resources:
Find more hand surgery guides and orthopedic training materials at https://hutaif-ortho.com.
Timestamps:
0:00 – Intro
0:20 – Mechanism & Pathology
0:50 – Indications & Anatomy
1:15 – Avoiding Avascular Necrosis
1:35 – Surgical Approach and Screw Fixation
2:15 – Complications & Rehab
2:40 – Outro
Comprehensive Introduction and Patho-Epidemiology
Phalangeal condylar fractures represent a formidable challenge within the realm of hand traumatology, demanding an uncompromising degree of precision from the operating surgeon. These injuries, which predominantly afflict the proximal and middle phalanges, disrupt the intricate kinematics of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. Because the phalangeal condyles operate within a highly constrained, specialized articular environment, even minor residual incongruities can precipitate devastating long-term functional deficits. The overarching goal for the orthopaedic hand surgeon remains steadfastly aligned with foundational AO principles: achieving an absolute anatomic reduction of the articular surface, securing rigid internal fixation to neutralize deforming forces, and instituting immediate, protected mobilization to circumvent the ubiquitous complication of periarticular fibrosis.
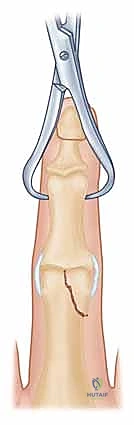
The epidemiology of these fractures reveals a bimodal distribution, frequently affecting young, active individuals engaged in competitive athletics, as well as industrial workers subjected to high-energy crush or shear mechanisms. The classic mechanism of injury involves a combination of axial loading coupled with sudden, forceful angular deviation—often varus or valgus stress—applied to the extended or partially flexed digit. This force vector shears the condyle from the phalangeal shaft, creating an unstable intra-articular fragment. While unicondylar fractures are the most common presentation, high-energy trauma can result in complex bicondylar or triplane fracture patterns that severely destabilize the entire joint construct.

The pathophysiology of untreated or inadequately reduced phalangeal condylar fractures follows a predictable and unforgiving cascade. The disruption of the articular cartilage, combined with the loss of the collateral ligament's anchoring point, leads to immediate joint subluxation and kinematic failure. The resulting abnormal contact stresses rapidly accelerate cartilage degradation, culminating in post-traumatic osteoarthritis. Furthermore, the inherent rotational instability of these fragments inevitably leads to digital scissoring during flexion, severely impairing the patient's grip strength and overall hand mechanics. Consequently, conservative management is rarely indicated for displaced fractures, making surgical intervention the definitive standard of care.
To master the operative management of these injuries, the surgeon must transcend basic fracture care and adopt a microscopic mindset. The fragments are often diminutive, osteoporotic, and tethered by critical, fragile soft-tissue hinges that provide their sole vascular supply. Stripping these fragments to achieve a "perfect" visual reduction can inadvertently induce iatrogenic avascular necrosis (AVN), transforming a reconstructable fracture into an unsalvageable nonunion. Therefore, the contemporary approach emphasizes biologically respectful dissection, strategic utilization of surgical windows, and the application of miniature implants that provide maximum stability with minimal footprint.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of digital anatomy is the absolute prerequisite for successful surgical intervention. The osteology of the PIP joint is characterized by the complex interaction between the bicondylar head of the proximal phalanx and the reciprocally contoured base of the middle phalanx. The proximal phalangeal head features two distinct condyles separated by a shallow intercondylar groove (the trochlea). These condyles are asymmetric, with the ulnar condyle typically projecting slightly further distally and volarly than the radial condyle, a morphological nuance that dictates the slight supination of the digits during composite flexion. The articular surface extends significantly onto the volar aspect, accommodating the massive arc of motion typical of the PIP joint (0 to 110 degrees).
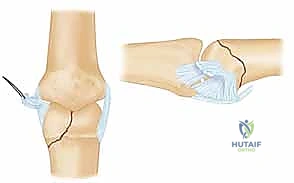
The ligamentous stabilizers of the PIP joint form a robust, box-like constraint system. The primary stabilizers are the proper and accessory collateral ligaments. The proper collateral ligament (PCL) originates from a distinct recess on the dorsal-lateral aspect of the condyle and inserts broadly onto the volar-lateral base of the middle phalanx. It is lax in extension but becomes maximally taut in flexion, resisting varus and valgus stress. The accessory collateral ligament (ACL) originates more volarly on the condyle and inserts directly into the lateral margins of the volar plate; it is taut in extension. Because these ligaments attach directly to the condylar fragments in a fracture scenario, they act as powerful deforming forces, yet they also serve as vital vascular conduits and reduction aids through the principle of ligamentotaxis.
Dorsally, the extensor mechanism envelops the joint, presenting a significant surgical obstacle. The extensor digitorum communis trifurcates over the proximal phalanx. The central slip inserts onto the dorsal base of the middle phalanx, while the lateral bands diverge, passing dorsal to the axis of rotation of the PIP joint to eventually form the terminal tendon. Between the central slip and the lateral bands lies a critical triangular interval—the retinacular window—which serves as our primary surgical corridor for dorsal-lateral approaches. Disruption of the central slip or excessive scarring of the lateral bands will inevitably lead to a boutonnière deformity or severe extension lag.
The neurovascular anatomy demands meticulous respect. The proper digital arteries and nerves course along the midaxial line of the digit, volar to the axis of the collateral ligaments. The vascular supply to the phalangeal condyles is precarious, derived from small, arborizing metaphyseal and epiphyseal vessels that branch from the proper digital artery and travel within the periosteal and ligamentous sleeves.
FATAL PITFALL: Aggressive subperiosteal stripping of the condylar fragment, particularly on its lateral and volar aspects, severs these tenuous vessels. This ischemic insult virtually guarantees avascular necrosis of the fragment, leading to structural collapse, nonunion, and catastrophic joint failure. Dissection must be strictly extra-periosteal whenever possible.
Exhaustive Indications and Contraindications
The decision to proceed with operative management in phalangeal condylar fractures is dictated by the absolute necessity to restore articular congruity and joint stability. The tolerance for displacement in the PIP or DIP joint is practically zero. Any articular step-off greater than 1.0 mm, or a gap exceeding 2.0 mm, represents an absolute indication for open reduction and internal fixation (ORIF). Even seemingly minuscule step-offs alter the contact mechanics of the joint, leading to exponential increases in peak cartilage stress and subsequent rapid-onset arthrosis.
Clinical findings often provide the most compelling indications for surgery. Joint subluxation, observable on true lateral radiographs, indicates that the collateral ligament complex has been functionally uncoupled from the phalangeal shaft, rendering the joint grossly unstable. Furthermore, any rotational deformity, clinically manifested as digit overlap or "scissoring" during active composite flexion, mandates surgical correction. Scissoring not only impairs the function of the injured digit but mechanically blocks the adjacent normal digits, drastically reducing overall grip efficiency.
Contraindications, while relatively rare in the context of healthy, active patients, must be carefully considered. Absolute contraindications include active, untreated local infections or severe systemic comorbidities that preclude the safe administration of anesthesia. Relative contraindications revolve around the "reconstructability" of the fracture. In cases of extreme, high-energy comminution where the condyle is pulverized into osteochondral dust (often termed a "pilon-type" variant), attempting rigid internal fixation may be futile. In such scenarios, alternative salvage procedures, such as primary arthrodesis, dynamic distraction external fixation, or volar plate arthroplasty, may be more appropriate initial strategies.
| Category | Specific Criteria / Conditions | Clinical Rationale |
|---|---|---|
| Absolute Indications | Articular step-off > 1.0 mm | Prevents rapid post-traumatic osteoarthritis. |
| Joint subluxation on radiography | Restores kinematic stability and joint tracking. | |
| Clinical rotational deformity (scissoring) | Restores normal composite grip mechanics. | |
| Bicondylar or Triplane fracture patterns | Inherently unstable; non-operative management fails universally. | |
| Relative Indications | Displaced extra-articular condylar neck fractures | High risk of secondary displacement and angular deformity. |
| Open fractures | Requires immediate debridement and stabilization. | |
| Absolute Contraindications | Active local soft tissue infection | High risk of deep joint space infection (septic arthritis). |
| Medically unstable patient | Anesthetic risks outweigh orthopaedic benefits. | |
| Relative Contraindications | Extreme osteochondral comminution | Implants cannot achieve purchase; consider primary arthrodesis. |
| Severe pre-existing osteoarthritis | Fixing the fracture will not restore a functional, painless joint. | |
| Non-compliant patient | Inability to follow strict early mobilization protocols leads to profound stiffness. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the hallmark of the master surgeon; these fractures are won or lost before the skin is ever incised. The clinical assessment must aggressively seek out subtle signs of instability. While the finger may appear relatively well-aligned in extension, asking the patient to actively flex the digits will frequently unmask a rotational malalignment. The surgeon must evaluate the plane of the fingernail in maximum flexion; it should point directly toward the scaphoid tubercle. Any deviation indicates a rotational component to the condylar displacement that must be corrected intraoperatively.
Radiographic evaluation must be exhaustive. Standard posteroanterior (PA) and lateral views are often insufficient due to the superimposition of the condyles. True, perfectly lateral radiographs of the isolated digit are mandatory to assess dorsal or volar subluxation. Furthermore, oblique views (both pronated and supinated) are critical to profile the entire articular surface and identify the true extent of the fracture line. In contemporary practice, for any fracture pattern that appears complex, comminuted, or involves both condyles, a high-resolution, fine-cut Computed Tomography (CT) scan with 3-dimensional reconstructions is strongly recommended. Cartilage is radiolucent, and plain films consistently underestimate the size of the osteochondral fragment and the degree of articular impaction.

Templating involves selecting the appropriate implant system based on the fracture morphology. Unicondylar fractures with a large fragment may accommodate one or two 1.0 mm, 1.3 mm, or 1.5 mm lag screws. If the fragment is small or highly comminuted, smooth 0.028-inch or 0.035-inch Kirschner wires (K-wires) may be the only viable option, though they lack the compressive benefits of lag screws. For bicondylar fractures, the surgeon must plan for a geometric reconstruction, often requiring a combination of transverse intercondylar screws to reconstitute the phalangeal head, followed by a mini-condylar plate or dorsal-to-volar screws to secure the reconstructed head to the diaphysis.
The operating room setup must optimize visualization and efficiency. The patient is positioned supine with the operative extremity extended onto a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm and inflated to 250 mmHg following meticulous exsanguination with an Esmarch bandage; a bloodless field is non-negotiable when dealing with 1-2 millimeter articular fragments. A mini C-arm fluoroscopy unit is draped sterilely and brought in parallel to the hand table, allowing the surgeon to obtain dynamic AP, lateral, and oblique views without moving the patient's arm. The surgeon typically sits in the axilla, with the assistant positioned opposite, ensuring both have an unobstructed view of the monitor.
📄 ( Show Short Video Transcript
Welcome to this intraoperative master class on fangial condular fractures. These injuries present a formidable challenge in hand traumatology where the tolerance for articular displacement is practically zero. Today we will cover the pathoepidemiology, surgical anatomy and the precise operative techniques required to restore perfect joint kinematics. Typically affecting young athletes or industrial workers, these fractures result from axial loading combined with sudden varys or vgus shear. If left untreated, the disruption of the articular cartilage and loss of collateral ligament anchoring leads to a predictable cascade, immediate joint subluxation, accelerated cartilage degradation, and rapid post-traumatic osteoarthritis. Clinically, rotational instability manifests as digital scissoring, severely impairing grip mechanics. Because of this, conservative management is rarely indicated for displaced fractures. Any articular step off greater than 1.0 mm or clinical scissoring is an absolute indication for open reduction and internal fixation. However, the surgical approach requires a microscopic mindset. The vascular supply to these tiny condular fragments is highly precarious. Here is the fatal pitfall. Aggressive subparostial stripping particularly on the lateral and aspects will sever the fragments only vascular tether. This iatrogenic eskeemic insult virtually guarantees avascular necrosis and catastrophic joint failure. Dissection must be strictly extrapostial. For most unicondular fractures, the dorsal lateral approach is the workhorse. We utilize the retinacular window between the central slip and lateral bands. Reduction is achieved carefully using ligamenttotaxis. For definitive fixation, we rely on interfragmentary compression using miniature 1.0 to 1.5 mm lag screws. Crucially, the near cortex must be counterunk. Because the cortical bone here is incredibly thin, a prominent screw head will impinge on the collateral ligament, restricting motion. Postoperatively, you are in a biological race between fracture consolidation and restrictive scar tissue. Postoperative stiffness is the most ubiquitous complication affecting up to 50% of cases. internalization the political general organization protect your function.
Step-by-Step Surgical Approach and Fixation Technique
Anesthesia and Dynamic Assessment
The procedure commences with the administration of anesthesia—typically a regional brachial plexus block supplemented with sedation, or general anesthesia, depending on patient factors and anticipated surgical duration. Complete muscle relaxation is highly beneficial. Prior to incision, a rigorous fluoroscopic examination under anesthesia (EUA) is performed. The surgeon applies gentle varus, valgus, and rotational stress to the joint while visualizing it under live fluoroscopy. This dynamic assessment confirms the fracture pattern, elucidates hidden instability, and solidifies the planned surgical approach and fixation vector.
Surgical Approaches: Precision and Soft Tissue Respect
The choice of surgical approach is dictated by the fracture geometry. The paramount objective is to gain adequate visualization of the articular surface while inflicting minimal collateral damage to the extensor mechanism and the fragment's vascular tether.
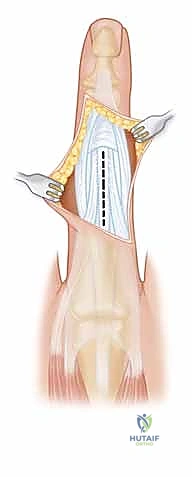
The Dorsal-Lateral Approach (For Unicondylar Fractures):
This is the workhorse approach for the vast majority of Type I, II, and III unicondylar fractures. A slightly curvilinear incision is made centered over the PIP joint, positioned between the dorsal midline and the midaxial line on the side of the fracture.


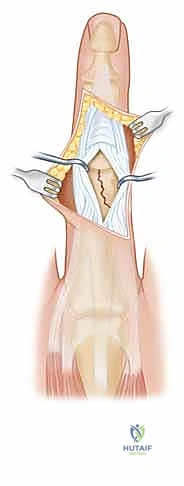
Subcutaneous tissues are bluntly dissected to expose the extensor mechanism. The critical step is identifying the interval between the lateral band and the central slip. Using a 15-blade scalpel or fine tenotomy scissors, this retinacular interval is longitudinally incised. The lateral band is retracted volarly, and the central slip is retracted dorsally, exposing the underlying joint capsule.

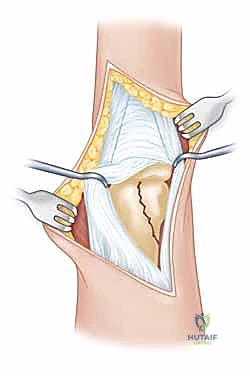
The capsule is then incised longitudinally, revealing the fracture hematoma and the displaced condyle. It is imperative to avoid stripping the collateral ligament attachment from the fragment.
The Extensor-Splitting or Flap Approach (For Bicondylar Fractures):
For complex Type IV and V fractures, a wider exposure is mandated. A dorsal longitudinal incision is utilized. The surgeon may opt to split the central slip longitudinally in the midline, though this carries a higher risk of postoperative extensor lag. Alternatively, a Chamay approach (creating a distally based V-shaped flap of the central slip) or mobilizing the entire extensor mechanism by incising both lateral retinacular borders allows for complete visualization of both condyles and the articular surface.
Articular Reduction and Provisional Fixation
Once the fracture site is exposed, the hematoma is meticulously irrigated and cleared using a fine dental pick or a small curette. The joint surface is inspected to identify any impacted osteochondral fragments, which must be gently elevated. Reduction is achieved using a combination of direct manipulation with a dental pick and indirect reduction via ligamentotaxis (applying traction and stressing the collateral ligament).

Once anatomic reduction of the articular surface is visually confirmed, it is provisionally stabilized. A specialized, pointed reduction forceps (e.g., a Weber clamp) can be applied, placing one tine on the intact condyle and the other on the fractured condyle. Alternatively, a 0.028-inch K-wire is driven percutaneously to hold the reduction. This provisional wire must be placed strategically so as not to interfere with the planned trajectory of the definitive lag screws. Fluoroscopy is utilized at this stage to confirm absolute articular congruity in multiple planes.

Definitive Internal Fixation: The Art of Lag Mechanics
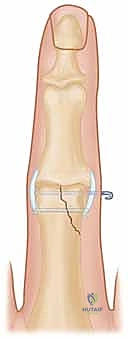
The gold standard for fixation is interfragmentary compression utilizing miniature lag screws (1.0 mm, 1.3 mm, or 1.5 mm). The technique must be flawless. A glide hole (matching the external diameter of the screw thread) is drilled through the near cortex of the fractured condyle. A drill sleeve is inserted into the glide hole, and a thread hole (matching the core diameter of the screw) is drilled into the far, intact cortex.
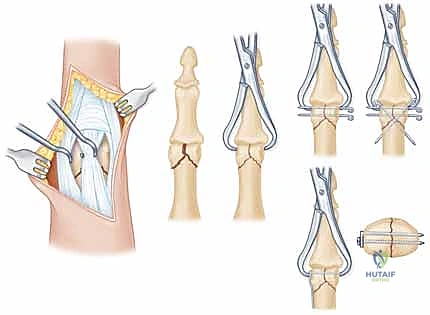


Crucially, the near cortex must be countersunk. The cortical bone of the phalangeal condyle is incredibly thin; without countersinking, the screw head will remain prominent, causing severe impingement of the collateral ligament or lateral band, leading to pain and restricted motion. The screw is measured and inserted, achieving robust interfragmentary compression. Whenever possible, two screws should be utilized to control rotational forces, though fragment size often limits the surgeon to a single screw supplemented by an anti-rotation K-wire.



For bicondylar fractures, the two condyles are first lagged together to reconstruct the articular block. This reconstructed block is then secured to the phalangeal shaft using either crossed K-wires, dorsal-to-volar lag screws, or a laterally applied low-profile titanium mini-plate, depending on the fracture morphology and available bone stock.



Following fixation, the tourniquet is deflated to ensure adequate perfusion to the digit and the fracture fragment. The joint is put through a full, passive range of motion to ensure there is no mechanical block, no crepitus, and that the fixation construct remains absolutely rigid under stress. The capsule and extensor mechanism are meticulously repaired with fine absorbable sutures (e.g., 4-0 or 5-0 Monocryl or Vicryl), and the skin is closed.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following phalangeal condylar fractures remain distressingly common, primarily due to the unforgiving nature of the digital anatomy. The surgeon must be acutely aware of these potential pitfalls, counsel the patient appropriately preoperatively, and possess the technical armamentarium to manage them when they arise.
The most ubiquitous complication is postoperative stiffness, characterized by a loss of both flexion and extension at the PIP joint. This results from a combination of intra-articular fibrosis, capsular contracture, and adhesions tethering the extensor mechanism or flexor tendons to the fracture callus. The incidence of clinically significant stiffness can exceed 30%, even with rigid fixation and early motion. Management begins with aggressive, prolonged hand therapy utilizing dynamic and static progressive orthoses. If conservative measures fail after 4 to 6 months, a surgical tenolysis and PIP joint capsulotomy may be indicated to restore functional glide.
Avascular necrosis (AVN) of the condylar fragment is a catastrophic complication stemming from overzealous surgical dissection and the stripping of the collateral ligament attachments. The incidence is variable but directly correlates with the aggressiveness of the exposure. AVN presents radiographically as sclerosis and subsequent collapse of the condyle, leading to profound joint incongruity and severe pain. Salvage options for AVN are limited and generally involve joint-sacrificing procedures. In younger patients, a vascularized joint transfer from the toe may be considered, while older or lower-demand patients are typically managed with PIP joint arthrodesis (fusion) in a functional position (typically 30-40 degrees of flexion).
Malunion and nonunion occur when reduction is inadequate or fixation fails. Rotational malunion is particularly debilitating, causing the affected digit to cross over adjacent digits during grip (scissoring). Corrective intra-articular osteotomies are technically demanding and carry a high risk of subsequent stiffness. Post-traumatic osteoarthritis is an almost inevitable long-term consequence if an articular step-off greater than 1 mm is left unreduced. Depending on the patient's age and functional demands, symptomatic arthrosis is managed with either silicone or pyrocarbon arthroplasty (for low-demand patients seeking motion) or arthrodesis (for high-demand patients requiring stability and pain relief).
| Complication | Estimated Incidence | Primary Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Joint Stiffness | 30% - 50% | Capsular contracture, tendon adhesions, prolonged immobilization. | Aggressive hand therapy, dynamic splinting; surgical tenolysis/capsulotomy at 6 months. |
| Avascular Necrosis (AVN) | 5% - 15% | Iatrogenic stripping of soft tissue/vascular supply from the fragment. | Hemi-hamate arthroplasty, toe-to-hand joint transfer, or primary arthrodesis. |
| Rotational Malunion | 10% - 20% | Failure to recognize or correct rotation during intraoperative reduction. | Corrective derotational osteotomy (phalangeal or metacarpal base). |
| Post-Traumatic Arthrosis | 20% - 40% | Residual articular step-off > 1mm; initial cartilage impact damage. | NSAIDs, injections; eventual PIP joint arthroplasty or arthrodesis. |
| Infection (Deep) | < 2% | Contamination, compromised soft tissue envelope. | Prompt surgical debridement, hardware removal (if unstable), IV antibiotics. |
Phased Post-Operative Rehabilitation Protocols
The success of the operative intervention is inextricably linked to the quality and compliance of the postoperative rehabilitation. The biological race is between fracture consolidation and the formation of restrictive scar tissue. Rigid internal fixation buys the surgeon the privilege of early mobilization, which is the cornerstone of modern hand therapy protocols.
Phase I: Immediate Post-Operative (Days 1 to 7)
Immediately following surgery, the hand is placed in a bulky, non-compressive dressing and supported by a volar intrinsic-plus orthosis (wrist extended 20 degrees, metacarpophalangeal joints flexed 70-80 degrees, and interphalangeal joints in full extension). The primary goals during this phase are strict edema control, pain management, and protection of the surgical wound. Elevation is mandatory. Active motion of the uninvolved digits, wrist, and shoulder is encouraged immediately to prevent dependent edema and proximal stiffness.
Phase II: Early Active Motion (Weeks 1 to 4)
At the first postoperative visit (typically days 5-7), the bulky dressing is removed. Provided the fixation is deemed absolutely rigid by the operating surgeon, the patient transitions to a custom-fabricated thermoplastic orthosis. Supervised hand therapy commences. The cornerstone of this phase is protected, early active range of motion (AROM). The patient performs active composite flexion and extension exercises within a safe, pain-free arc. Buddy taping to an adjacent normal digit provides dynamic support and encourages normal kinematic tracking during exercise. Passive range of motion (PROM) is strictly avoided during this phase to prevent stretching the repaired capsule or displacing the fracture.
Phase III: Advanced Mobilization and Strengthening (Weeks 4 to 8)
By week 4, clinical and radiographic evidence of early callus formation should be present. The protective orthosis is gradually discontinued during the day but may be worn at night. If the patient is exhibiting significant stiffness or an extension lag, dynamic or static-progressive splinting (e.g., a Capener splint or a joint jack) is initiated to gently stretch the contracted
