Mastering Distal Humerus ORIF: An Intraoperative Guide to Supracondylar and Intercondylar Fractures

Key Takeaway
This masterclass guides fellows through open reduction and internal fixation (ORIF) of complex supracondylar and intercondylar distal humerus fractures. We'll cover comprehensive surgical anatomy, meticulous preoperative planning, exact patient positioning, and a step-by-step intraoperative execution from the surgeon's perspective. Learn critical pearls, pitfalls, and strategies for achieving stable fixation and optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Open reduction and internal fixation (ORIF) of comminuted supracondylar and intercondylar fractures of the distal humerus represents one of the most formidable challenges in orthopedic trauma surgery. These fractures present a unique set of complexities driven by the intricate articular anatomy, the inherently thin cortical bone of the distal humerus, and the critical neurovascular structures running in close proximity to the surgical field. The paramount objective for the orthopedic surgeon is to restore a stable, anatomically reduced articular surface that permits immediate, unprotected active motion, thereby mitigating the profound stiffness that classically plagues the traumatized elbow. Achieving this requires not merely mechanical competence, but a profound understanding of elbow biomechanics, meticulous soft tissue handling, and absolute precision in osteosynthesis.
Distal humerus fractures exhibit a classic bimodal epidemiologic distribution, predominantly affecting two distinct patient populations with vastly different physiological profiles and injury mechanisms. The first peak occurs in younger individuals (typically males in their second to fourth decades) who sustain high-energy trauma, such as motor vehicle collisions, motorcycle accidents, or falls from significant heights. These injuries are frequently characterized by severe osseous comminution, profound soft tissue stripping, and a higher incidence of open fractures. The second demographic peak comprises older patients, predominantly postmenopausal females with underlying osteopenia or frank osteoporosis, who sustain these injuries from low-energy mechanisms, most commonly a simple fall from a standing height. In this latter cohort, the poor bone stock severely compromises hardware purchase, making stable internal fixation a biomechanical conundrum.


The classification of these fractures is primarily dictated by the AO/OTA alphanumeric system, which categorizes distal humerus fractures into type 13-A (extra-articular), 13-B (partial articular), and 13-C (complete articular). The 13-C fractures—specifically the C2 and C3 subtypes—are the focus of this text, characterized by complete dissociation of the articular block from the diaphyseal shaft, coupled with varying degrees of articular and metaphyseal comminution. The "spool" shape of the trochlea and the hemispherical capitellum must be anatomically reconstructed to restore the complex hinge-and-pivot kinematics of the ulnohumeral and radiocapitellar joints. Failure to recognize the extent of coronal shear components or profound metaphyseal bone loss during the initial evaluation will inevitably lead to catastrophic intraoperative difficulties and subsequent construct failure.
Furthermore, the initial evaluation must extend beyond the osseous injury to encompass a rigorous assessment of the soft tissue envelope and neurovascular status. The incidence of associated nerve injuries, particularly to the ulnar nerve due to its tethered position in the cubital tunnel, can be as high as 25% in high-energy trauma. Open fractures require emergent gross debridement, administration of broad-spectrum intravenous antibiotics, and meticulous temporization, often utilizing spanning external fixation if definitive ORIF must be delayed. The surgeon must synthesize the patient's chronological age, physiological demands, bone quality, and fracture morphology to formulate a definitive treatment strategy that balances the risks of extensive surgical exposure against the necessity of rigid biomechanical stability.
Detailed Surgical Anatomy and Biomechanics
A masterful execution of distal humerus ORIF demands an encyclopedic knowledge of the regional anatomy and its biomechanical implications. The distal humerus is best conceptualized biomechanically as a triangle or a "tie-arch," consisting of two robust cortical columns—the medial and lateral columns—that diverge distally from the humeral diaphysis to support the articular segment (the "tie"). The medial column terminates in the medial epicondyle and the medial aspect of the trochlea, while the lateral column ends at the lateral epicondyle and capitellum. The articular segment itself is angled approximately 30 degrees anteriorly relative to the humeral shaft, a critical anatomical parameter that must be restored to allow for full elbow flexion.

Between these two columns lie the olecranon fossa posteriorly and the coronoid and radial fossae anteriorly. The bone separating these fossae is extraordinarily thin—often translucent—and provides negligible structural support for internal fixation. Therefore, the biomechanical integrity of any osteosynthesis construct relies entirely on securing the articular fragments to the robust cortical bone of the medial and lateral columns. The articular geometry is equally complex; the trochlea is not a simple cylinder but a spool with a central groove that dictates the tracking of the ulna, while the capitellum is a purely anterior and inferior structure that does not extend posteriorly. Recognizing these spatial relationships is vital when placing interfragmentary screws to avoid joint penetration.
The neurovascular topography surrounding the distal humerus is dense and unforgiving. The ulnar nerve is the most vulnerable structure during the posterior approach to the elbow. It courses distally through the posterior compartment of the arm, piercing the medial intermuscular septum to enter the cubital tunnel, bounded by the medial epicondyle anteriorly, the olecranon laterally, and Osborne’s fascia superficially. The radial nerve, while located more proximally in the spiral groove, pierces the lateral intermuscular septum to enter the anterior compartment and lies in close proximity to the lateral column during proximal plate extension. The median nerve and brachial artery are situated anteriorly, generally protected by the brachialis muscle, but remain at risk during aggressive anterior retractor placement or penetrating drill bits.
Ligamentous stability of the elbow is intrinsically linked to the osseous anatomy. The medial collateral ligament (MCL) complex, specifically its anterior bundle, originates from the anteroinferior surface of the medial epicondyle and inserts on the sublime tubercle of the ulna, serving as the primary restraint to valgus stress. The lateral ulnar collateral ligament (LUCL) originates from the lateral epicondyle and inserts on the supinator crest of the ulna, acting as the primary restraint to varus and posterolateral rotatory instability. During the surgical approach and subsequent fracture mobilization, absolute care must be taken to preserve the origins of these ligaments. If epicondylar comminution involves the ligamentous origins, they must be meticulously repaired or reconstructed at the conclusion of the case to prevent devastating postoperative instability.
Exhaustive Indications and Contraindications
The decision-making paradigm for distal humerus fractures is nuanced, requiring the surgeon to weigh the benefits of anatomical restoration against the morbidity of extensive surgical exposure. Open reduction and internal fixation remains the gold standard for the vast majority of displaced supracondylar and intercondylar fractures in physiologically active patients. The primary indication is any displaced intra-articular fracture (AO/OTA Type 13-B and 13-C) where the articular congruity is disrupted, as even a 2-millimeter step-off can lead to rapid post-traumatic arthrosis. Furthermore, displaced extra-articular fractures (Type 13-A) that cannot be maintained in acceptable alignment with closed methods, or those associated with neurovascular compromise, mandate surgical intervention.
Conversely, absolute contraindications to ORIF are exceedingly rare but include active, uncontrolled infection at the surgical site, or a patient whose medical comorbidities render them unfit for general or regional anesthesia. Relative contraindications are more common and heavily influence the choice between ORIF and Total Elbow Arthroplasty (TEA). Severe osteopenia or frank osteoporosis in a low-demand, elderly patient presents a massive challenge for ORIF, as the screws will inevitably fail to achieve adequate purchase in the "eggshell" bone, leading to early construct failure. In these specific scenarios, primary TEA has emerged as a highly successful alternative, providing immediate stability, allowing for early mobilization, and demonstrating superior short-to-medium-term outcomes in appropriately selected geriatric populations.
Another critical consideration is the presence of pre-existing symptomatic elbow pathology, such as advanced rheumatoid arthritis or severe primary osteoarthritis. In a patient with a pre-existing destroyed joint who sustains a distal humerus fracture, attempting complex ORIF is often a fool's errand; the patient is better served by bypassing osteosynthesis and proceeding directly to TEA. Furthermore, severe soft tissue compromise, such as massive degloving injuries or highly contaminated open fractures (Gustilo-Anderson Grade III), may necessitate a staged approach. In these cases, the initial procedure is limited to meticulous debridement, temporary spanning external fixation, and delayed definitive ORIF once the soft tissue envelope has adequately declared itself and recovered.
| Clinical Parameter | Indications for ORIF | Indications for Primary TEA |
|---|---|---|
| Patient Age / Demand | Physiologically young, high functional demand, heavy laborers. | Elderly (>65 years), low functional demand, sedentary lifestyle. |
| Bone Quality | Normal to mild osteopenia; adequate cortical thickness for screw purchase. | Severe osteoporosis; "eggshell" bone, inability to achieve rigid fixation. |
| Fracture Morphology | Reconstructable articular fragments, even if highly comminuted. | Unreconstructable articular comminution, extreme distal shear fractures. |
| Pre-existing Joint Status | Normal, asymptomatic elbow joint prior to injury. | Pre-existing rheumatoid arthritis or advanced osteoarthritis. |
| Soft Tissue Envelope | Intact or manageable soft tissue injuries. | (TEA contraindicated in active infection or severe soft tissue loss). |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning is the bedrock upon which successful distal humerus osteosynthesis is built. It begins with an exhaustive radiographic evaluation. Standard anteroposterior (AP) and lateral radiographs are mandatory but frequently insufficient for fully characterizing the complex 3D geometry of a comminuted 13-C fracture. Due to the overlap of the radius and ulna, as well as the inherent rotational deformities of the fracture fragments, the true extent of articular comminution is often masked. Therefore, a high-resolution Computed Tomography (CT) scan with 3D reconstructions and multiplanar reformatting is considered the standard of care for all intra-articular distal humerus fractures. The CT scan allows the surgeon to map the fracture lines, identify coronal shear components (e.g., capitellar or trochlear shear fractures), and quantify the degree of metaphyseal bone loss.

Armed with advanced imaging, the surgeon must engage in meticulous preoperative templating. This involves selecting the appropriate surgical approach, anticipating the sequence of reduction, and choosing the optimal implant configuration. The current biomechanical consensus strongly favors dual-plate osteosynthesis for complete articular fractures. The surgeon must decide between an orthogonal plating configuration (one plate medial, one plate posterolateral) or a parallel plating configuration (one plate medial, one plate lateral). While both constructs provide adequate stability when applied correctly, parallel plating, as championed by O'Driscoll, often provides superior biomechanical resistance to rotational and varus/valgus forces, particularly in the setting of extreme metaphyseal comminution. The templating phase ensures that the selected plates will not impinge on the olecranon or coronoid fossae and that screws can be interdigitated to maximize fixation in the distal articular block.
Patient positioning is a critical logistical step that dictates the ease of surgical exposure and intraoperative fluoroscopic assessment. The two most common positions are the lateral decubitus position and the prone position. The prone position is frequently preferred by trauma surgeons as it provides unparalleled, unhindered access to the posterior aspect of the elbow. The patient is placed prone with the operative arm draped free over a well-padded bolster or a specialized arm holder, allowing the elbow to flex to 120 degrees and the forearm to hang freely. This gravity-assisted positioning naturally aids in reducing the fracture and allows for full dynamic assessment of elbow range of motion throughout the procedure.
Alternatively, the lateral decubitus position with the arm resting over a radiolucent post is an excellent option, particularly for patients with severe pulmonary or airway comorbidities that preclude prone positioning. Regardless of the chosen position, the setup must allow for unimpeded, orthogonal fluoroscopic imaging. The C-arm should be brought in from the contralateral side or from the head of the table. A sterile tourniquet is typically applied high on the brachium to provide a bloodless surgical field, though it should be deflated prior to final closure to achieve meticulous hemostasis and assess the vascularity of the ulnar nerve.
Step-by-Step Surgical Approach and Fixation Technique
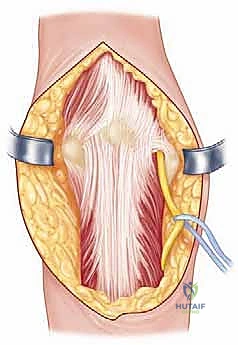
The surgical approach dictates the quality of the reduction; inadequate exposure is the most common cause of malreduction in distal humerus fractures. For complex C-type fractures, the extensile posterior approach utilizing an olecranon osteotomy is the unequivocal gold standard. A longitudinal midline incision is made over the posterior arm, curving slightly laterally around the tip of the olecranon to prevent a painful scar directly over the bony prominence, and extending distally along the subcutaneous border of the ulna. Full-thickness fasciocutaneous flaps are elevated medially and laterally to protect the cutaneous nerves and preserve the vascularity of the skin.

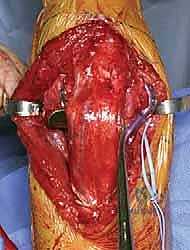
The immediate next step, prior to any deep dissection, is the identification, neurolysis, and protection of the ulnar nerve. The nerve is located proximally along the medial border of the triceps and traced distally into the cubital tunnel. The roof of the cubital tunnel (Osborne’s ligament) and the fascia of the flexor carpi ulnaris (FCU) are released to thoroughly decompress the nerve. Whether to perform a routine anterior subcutaneous transposition or leave the nerve in situ remains a topic of debate; however, if the hardware will impinge upon the nerve's native bed, or if extensive medial dissection is required, a tension-free anterior transposition using a fascial sling is highly recommended to prevent postoperative ulnar neuritis.

With the nerve protected, attention turns to the olecranon osteotomy. A chevron-shaped osteotomy, with the apex pointing distally, is preferred over a transverse cut as it provides inherent rotational stability and a larger surface area for healing. The osteotomy site is targeted at the bare area of the greater sigmoid notch, typically 2-3 centimeters distal to the olecranon tip. Crucially, before initiating the cut, the proximal ulna is pre-drilled and tapped for a 6.5mm or 7.3mm cannulated lag screw to ensure perfect alignment during subsequent repair. The osteotomy is initiated with a fine oscillating saw and completed with a thin osteotome to crack the subchondral bone, preserving the articular cartilage interdigitation. The olecranon fragment, with the triceps mechanism attached, is then reflected proximally, granting a breathtaking, 360-degree view of the distal humeral articular surface.

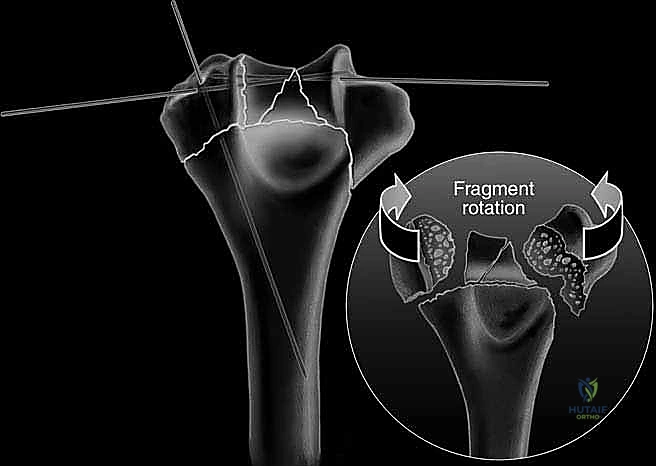

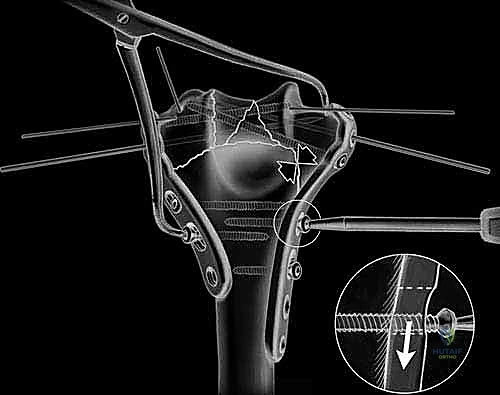
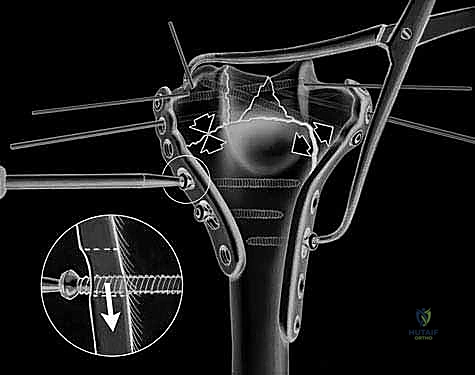
The fracture reduction sequence follows a strict "inside-out" and "bottom-up" philosophy. The primary objective is the anatomical restoration of the articular block (the "tie"). The trochlear and capitellar fragments are meticulously debrided of hematoma, reduced using pointed reduction forceps, and provisionally stabilized with smooth Kirschner wires. This articular assembly is then definitively fixed using headless compression screws or countersunk cortical lag screws, ensuring no hardware violates the joint surface. Once the articular block is reconstituted into a single, solid unit, it is reduced to the medial and lateral columns of the humeral diaphysis. Provisional fixation to the shaft is achieved with K-wires, and orthogonal fluoroscopy is utilized to confirm anatomical alignment, particularly the crucial 30-degree anterior tilt of the articular surface.

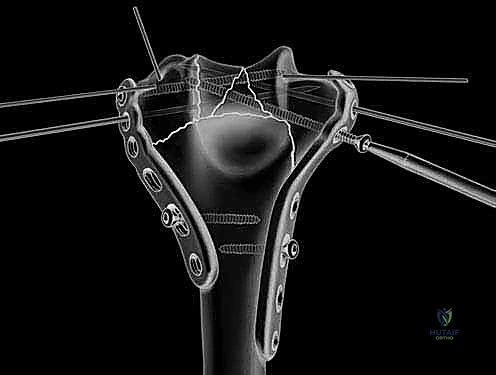
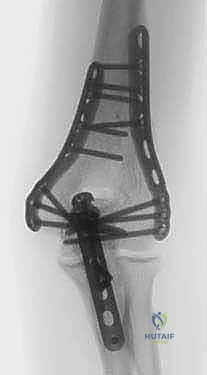
Definitive osteosynthesis is achieved through the application of dual pre-contoured anatomical plates. Following the principles of parallel plating, a plate is applied to the medial ridge and another to the lateral ridge of the distal humerus. The plates are positioned to maximize screw purchase in the distal articular block; ideally, multiple screws should interdigitate through the articular fragments, creating a "rebar" effect. The plates must be compressed to the bone using standard lag techniques or articulated tension devices before deploying locking screws. The stability of the construct is then rigorously tested by taking the elbow through a full, unhindered range of motion. Finally, the olecranon osteotomy is meticulously repaired using the previously drilled lag screw supplemented with a figure-of-eight tension band wire, or via a dedicated proximal ulna locking plate, ensuring rigid fixation to allow for immediate postoperative rehabilitation.



Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, ORIF of distal humerus fractures carries a formidable complication profile. The surgeon must be acutely aware of these risks, actively employ mitigation strategies intraoperatively, and possess the armamentarium to manage them when they arise. The most frequent and often most debilitating complication is postoperative elbow stiffness. The elbow joint capsule is highly reactive to trauma and surgical dissection, rapidly forming thick, fibrotic scar tissue. Loss of terminal extension is nearly universal, but functionally limiting stiffness (arc of motion less than 100 degrees) occurs in up to 15-20% of cases. Prevention relies entirely on achieving rigid internal fixation that permits immediate, aggressive postoperative mobilization.
Ulnar neuropathy is the most common neurological complication, with a reported incidence ranging from 10% to 25%. This can manifest as transient paresthesias, motor weakness, or profound, permanent neuropathic pain. The etiology is multifactorial, including initial trauma, intraoperative traction, hardware impingement, or postoperative perineural fibrosis. If a patient develops progressive ulnar neuropathy postoperatively, aggressive medical management (gabapentinoids, NSAIDs) is initiated. However, refractory cases or those with profound motor deficits necessitate early surgical re-exploration, hardware removal if impinging, and formal submuscular or subcutaneous transposition of the nerve.
Heterotopic ossification (HO) is another significant complication, particularly prevalent in high-energy trauma, delayed surgical interventions, or associated central nervous system injuries. HO can bridge the joint space, leading to complete ankylosis. Prophylaxis with non-steroidal anti-inflammatory drugs (e.g., Indomethacin) or single-dose perioperative radiation therapy should be strongly considered in high-risk patients. If clinically significant HO develops, surgical excision is delayed until the ossification is radiographically mature and the inflammatory phase has subsided, typically 6 to 12 months post-injury, often combined with an extensive capsular release.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Elbow Stiffness | 15% - 30% | Prolonged immobilization, capsular fibrosis, inadequate fixation. | Aggressive PT, dynamic splinting; late open or arthroscopic capsular release. |
| Ulnar Neuropathy | 10% - 25% | Traction injury, hardware impingement, perineural scarring. | Observation for transient neurapraxia; surgical neurolysis and transposition for refractory cases. |
| Nonunion / Hardware Failure | 2% - 10% | Poor bone stock, inadequate mechanical construct, infection. | Revision ORIF with bone grafting; Total Elbow Arthroplasty in elderly/osteoporotic patients. |
| Heterotopic Ossification | 5% - 15% | High-energy trauma, delayed surgery, head injury |
