Pediatric Ankle Fractures: An Intraoperative Masterclass on Surgical Management

Key Takeaway
This masterclass offers an immersive, step-by-step guide to surgically managing pediatric ankle fractures. We delve into intricate physeal anatomy, detailed preoperative planning, and precise intraoperative execution from incision to fixation. Emphasis is placed on meticulous reduction, preserving growth plates, and avoiding neurovascular complications. Fellows will gain critical insights into preventing premature physeal closure and optimizing long-term functional outcomes for our young patients.
Comprehensive Introduction and Patho-Epidemiology
Pediatric ankle fractures represent a formidable intersection of complex biomechanics, dynamic skeletal development, and high-energy trauma. Comprising approximately 5% of all pediatric fractures, they stand as the second most common long-bone physeal injury, superseded only by fractures of the distal radius. However, unlike the distal radius, which possesses a robust capacity for spontaneous remodeling in the sagittal and coronal planes, the distal tibia is remarkably unforgiving. The ankle is a highly constrained, weight-bearing hinge joint; even minor articular incongruity or subtle physeal disruption can precipitate catastrophic long-term sequelae, including profound angular deformity, leg length discrepancy, and early-onset post-traumatic osteoarthritis.
The fundamental distinction between pediatric and adult ankle trauma lies in the presence of the physis, or growth plate. In the skeletally immature patient, the ligamentous structures—specifically the deltoid ligament medially and the tibiofibular syndesmotic complex laterally—frequently exhibit greater tensile strength than the adjacent chondro-osseous junction of the physis. Consequently, forces that would typically yield a ligamentous sprain or syndesmotic rupture in an adult are preferentially translated through the zone of provisional calcification within the growth plate, resulting in Salter-Harris fracture patterns. This anatomic reality mandates a paradigm shift in our diagnostic and therapeutic approach; we must assume a physeal injury is present in any pediatric patient presenting with ankle trauma until definitively proven otherwise.
Our overarching surgical objective in managing these injuries is unequivocal: the restoration of near-anatomic alignment. The contemporary orthopedic literature universally supports a stringent tolerance of no more than 2 millimeters of residual displacement at the articular surface or the physeal line. While nonoperative management via closed reduction and cast immobilization remains the gold standard for undisplaced or minimally displaced fractures, surgical intervention is absolutely mandated when this 2-millimeter threshold is breached. The failure to achieve and maintain this degree of reduction exponentially increases the risk of the most dreaded complication in pediatric orthopedics: premature physeal closure (PPC) and subsequent asymmetric growth arrest.
As we navigate this intraoperative masterclass, we will meticulously deconstruct the surgical management of pediatric ankle fractures. From the nuanced interpretation of three-dimensional advanced imaging to the execution of precise, tissue-sparing surgical approaches, our focus will remain on the preservation of physeal vitality and the restoration of articular congruity. This chapter is designed to equip the orthopedic surgeon with the advanced cognitive and technical armamentarium required to master these delicate, high-stakes injuries.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, a profound, three-dimensional understanding of the distal tibial and fibular anatomy is paramount. The pediatric ankle is not a static structure; it is a dynamic, evolving biomechanical entity whose morphology dictates both the fracture pattern and our surgical strategy.
The Distal Tibial Physis and Kump's Bump
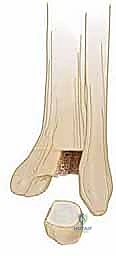
The distal tibial physis is a predominantly transverse structure responsible for approximately 45% of the longitudinal growth of the tibia (averaging 3 to 4 millimeters per year). However, its topography is not perfectly flat. It possesses a highly consistent, anterior-medial undulation, eponymously termed Kump’s bump. This structure typically becomes radiographically apparent within the first two years of life and serves as the critical epicenter for the physiological closure of the growth plate.

Physiological physeal closure is an asymmetric, predictable process. It invariably initiates at Kump’s bump—the central-medial aspect of the physis—typically around 15 years of age in females and 17 years of age in males. From this central-medial nexus, the closure process progresses medially, then posteriorly, and finally laterally over a period of approximately 18 months. This asymmetric closure pattern is the fundamental biomechanical prerequisite for the development of transitional fractures, such as Tillaux and triplane injuries, which occur exclusively during this 18-month window of vulnerability.
Damage to Kump's bump, whether from the initial traumatic impact (particularly shearing forces inherent in abduction-type injuries) or iatrogenic injury during aggressive reduction maneuvers, is strongly implicated in the pathogenesis of premature physeal closure. The surgeon must exercise extreme caution when manipulating fragments in this central-medial zone. Furthermore, transphyseal fixation, if deemed absolutely necessary, must be executed with smooth, unthreaded Kirschner wires, meticulously avoiding the central-medial physis whenever possible to minimize the risk of inducing an iatrogenic physeal bar.
Ligamentous Attachments and the Perichondral Ring
The ligamentous anatomy of the pediatric ankle is inextricably linked to the epiphyseal ossification centers. The anteroinferior tibiofibular ligament (AITFL), a robust structure critical for syndesmotic stability, originates from the anterolateral tubercle of the distal tibia (Chaput's tubercle) and inserts onto the anterior tubercle of the distal fibula (Wagstaffe's tubercle). In the adolescent ankle undergoing asymmetric physeal closure, the lateral aspect of the physis remains open and mechanically vulnerable while the medial aspect is fused. An external rotation force applied to the foot will tension the AITFL; because the ligament is stronger than the open lateral physis, it avulses the anterolateral epiphyseal fragment, creating the classic juvenile Tillaux fracture.

Equally critical to our surgical understanding is the perichondral ring of La Croix. This structure is a dense, fibrous transitional zone located at the periphery of the physis, bridging the articular cartilage of the epiphysis to the periosteum of the metaphysis. It provides crucial mechanical stability to the growth plate and retains immense chondrogenic and osteogenic potential.
However, during a displacement injury (most notably Salter-Harris Type I and II fractures), the periosteum on the tension side of the fracture is frequently torn and stripped from the metaphysis, while remaining rigidly attached to the perichondral ring. As the fracture recoils or during attempts at closed reduction, this robust periosteal sleeve can become invaginated and interposed directly within the physeal fracture gap. This entrapped periosteum acts as an impenetrable mechanical barrier to anatomic reduction. When a closed reduction feels "rubbery" or springs back to a displaced position, periosteal entrapment must be the primary diagnostic suspicion, mandating an open surgical approach to meticulously extricate the tissue and achieve cortical apposition.
Neurovascular Topography and Surgical Approaches
The distal tibia and fibula are enveloped by a complex network of neurovascular structures that dictate our surgical windows. Meticulous dissection and proactive protection of these structures are non-negotiable tenets of pediatric ankle trauma surgery.
The anterior approach, frequently utilized for Tillaux fractures and the anterior component of triplane fractures, places the superficial peroneal nerve (SPN) at significant risk. The SPN transitions from deep to superficial in the middle third of the leg and its terminal branches cascade across the anterolateral ankle. Retraction must be gentle, as the nerve is highly susceptible to traction neuropraxia. More medially, the deep peroneal nerve and the anterior tibial artery and veins descend in the interval between the tibialis anterior and the extensor hallucis longus. While this interval is generally safe for deeper dissection, the neurovascular bundle must be identified and protected, particularly when placing anterior-to-posterior epiphyseal screws.
The posteromedial approach, often necessary for displaced medial malleolar fractures or Salter-Harris Type IV injuries, navigates treacherous anatomical terrain. The posterior tibial neurovascular bundle—comprising the posterior tibial artery, posterior tibial nerve, and accompanying venae comitantes—runs directly deep to the flexor retinaculum, nestled between the tendons of the tibialis posterior and the flexor digitorum longus. This bundle is extremely vulnerable during the surgical approach and during the placement of medial-to-lateral fixation. Dissection must be precise, utilizing the tendon sheaths as anatomical landmarks to safely mobilize and retract the bundle.

The lateral approach to the distal fibula requires vigilance regarding the sural nerve, which courses posteriorly to the lateral malleolus alongside the short saphenous vein. When extending incisions proximally or dissecting posterior to the fibula for syndesmotic evaluation, the sural nerve must be visually identified and protected. Additionally, the terminal branches of the SPN crossing the anterior aspect of the lateral malleolus must be respected during subcutaneous dissection.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in pediatric ankle fractures hinges on a delicate balance between the inherent remodeling potential of the child and the absolute requirement for articular and physeal congruity. The threshold for operative management is significantly lower in the ankle compared to other pediatric long bones due to the joint's weight-bearing demands and constrained kinematics.
| Parameter | Absolute Indications for Surgery | Relative Indications for Surgery | Contraindications |
|---|---|---|---|
| Displacement | Intra-articular step-off > 2mm | Physeal gap 1-2mm with instability | Undisplaced fractures (<2mm) |
| Soft Tissue | Open fractures (Gustilo-Anderson I-III) | Severe soft tissue swelling (delay surgery) | Active local skin infection |
| Reduction | Inability to achieve/maintain closed reduction | "Rubbery" reduction (suspected trapped periosteum) | Acceptable closed reduction maintained in cast |
| Neurovascular | Associated neurovascular compromise | Impending compartment syndrome | Severe, life-threatening polytrauma (damage control first) |
| Fracture Pattern | Displaced Tillaux or Triplane fractures | Salter-Harris III/IV with any displacement | Asymptomatic non-unions of accessory ossicles |
The "2-millimeter rule" is the cornerstone of our decision-making matrix. Any intra-articular step-off or physeal gap exceeding 2 millimeters after a concerted attempt at closed reduction is an absolute indication for surgical intervention. Residual intra-articular displacement alters the contact mechanics of the tibiotalar joint, exponentially increasing focal peak pressures and paving the way for early-onset osteoarthritis. Similarly, a physeal gap greater than 2 millimeters provides a conduit for the formation of a fibrovascular bridge, which rapidly ossifies into a physeal bar, tethering growth and resulting in angular deformity.
Open fractures represent an orthopedic emergency requiring immediate surgical debridement, copious irrigation, and stabilization. The presence of neurovascular compromise that does not resolve with closed reduction similarly demands urgent operative exploration. Furthermore, the clinical presentation of a "rubbery" or springy reduction—where the fracture perfectly aligns under tension but immediately displaces upon release—is highly diagnostic of periosteal interposition. This cannot be overcome with cast molding and necessitates an open approach to clear the fracture site.
Contraindications to definitive internal fixation are primarily limited to undisplaced fractures that can be reliably managed with rigid cast immobilization. In cases of severe soft tissue compromise, such as massive fracture blisters or impending compartment syndrome, definitive open reduction may be temporarily contraindicated. In these scenarios, the application of a bridging external fixator or a meticulously molded splint is required until the soft tissue envelope recovers sufficiently to permit safe surgical incisions.
Pre-Operative Planning, Templating, and Patient Positioning
The success of any surgical intervention is largely determined before the patient enters the operating theater. In the context of pediatric ankle fractures, meticulous pre-operative planning, reliant on high-quality imaging and a thorough understanding of the injury mechanism, is absolutely critical.
Diagnostic Imaging Modalities
The initial evaluation mandates a dedicated, high-quality radiographic series of the ankle, comprising three specific projections: a true anteroposterior (AP), a lateral, and a 20-degree internally rotated mortise view. The mortise view is arguably the most critical radiograph in our arsenal. By internally rotating the leg to align the medial and lateral malleoli parallel to the imaging cassette, the mortise view eliminates the bony overlap of the distal tibiofibular syndesmosis. This provides an unobstructed assessment of talar symmetry within the ankle mortise and allows for the precise visualization of epiphyseal fragments that are frequently obscured on standard AP views, particularly the anterolateral fragment pathognomonic of Tillaux fractures.


While plain radiographs are sufficient for diagnosing many Salter-Harris Type I and II injuries, they frequently underestimate the complexity and degree of displacement in intra-articular and transitional fractures. Therefore, we maintain a very low threshold for obtaining computed tomography (CT) scans. For any intra-articular fracture demonstrating displacement on plain films, and routinely for all suspected Tillaux and triplane fractures, a fine-cut CT scan with multi-planar reconstruction (sagittal and coronal) and three-dimensional (3D) surface rendering is considered the standard of care.


3D CT reconstructions are invaluable for pre-operative templating. They allow the surgeon to virtually rotate the fracture fragments, precisely delineate the size and spatial orientation of the metaphyseal spike in triplane injuries, and map the exact trajectory required for screw placement to achieve perpendicular compression across the fracture plane without violating the open physis. Furthermore, we routinely obtain an AP radiograph of the contralateral, uninjured ankle to accurately assess the patient's baseline physeal maturity and skeletal age, which directly influences our choice of fixation hardware (e.g., smooth pins vs. threaded screws).

Operating Room Setup and Patient Positioning
Optimal patient positioning and operating room ergonomics are essential for facilitating efficient and safe surgery. The patient is positioned supine on a fully radiolucent operating table. A crucial, yet often overlooked, step is the placement of a well-padded bump beneath the ipsilateral hip. This internally rotates the lower extremity, neutralizing the natural external rotation of the hip and presenting the ankle mortise in a true AP orientation relative to the ceiling. This significantly simplifies intraoperative fluoroscopy and hardware trajectory planning.

A pneumatic tourniquet is applied to the proximal thigh, but it is only inflated if visualization is compromised by excessive hemorrhage, as we prefer to maintain perfusion to the delicate physeal and periosteal tissues whenever possible. The C-arm fluoroscopy unit must be positioned on the contralateral side of the table, entering perpendicular to the operative field. The surgeon and assistant should be able to effortlessly rotate the C-arm through a full 180-degree arc to obtain perfect AP, mortise, and lateral views without compromising the sterile field. Prior to incision, the limb is exsanguinated, and the surgical site is prepped and draped to allow access from the proximal third of the tibia down to the toes, ensuring the ability to assess rotational alignment dynamically.

Step-by-Step Surgical Approach and Fixation Technique
The surgical management of pediatric ankle fractures demands a highly tailored approach, dictated by the specific fracture morphology, the patient's remaining growth potential, and the presence of soft tissue interposition. Our techniques range from minimally invasive percutaneous pinning to complex, multi-planar open reductions.
Closed Reduction and Percutaneous Pinning (CRPP)
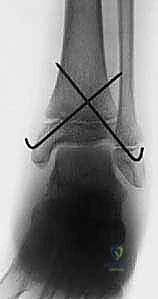
For displaced Salter-Harris Type I and II fractures where a concentric, anatomic reduction can be achieved via closed manipulation, percutaneous pinning is the preferred modality. The reduction maneuver must be deliberate and mechanistically sound, essentially reversing the forces of the initial injury as described by the Lauge-Hansen classification. For example, a supination-external rotation injury requires a reduction maneuver of internal rotation and pronation while applying longitudinal traction.

Once reduction is confirmed fluoroscopically in all three planes, fixation is achieved using smooth, unthreaded Kirschner wires (typically 1.6mm or 2.0mm, depending on the child's size). The pins are introduced percutaneously, taking care to avoid major neurovascular structures. For distal tibial fractures, crossed pins are frequently utilized, starting from the medial and lateral malleoli and directed proximally across the physis into the metaphysis. It is imperative that these pins are smooth to minimize physeal damage; threaded pins or screws must never cross an open physis with significant remaining growth potential. The pins are typically bent and left protruding through the skin to facilitate easy removal in the clinic at 3 to 4 weeks post-operatively.

Open Reduction and Internal Fixation (ORIF) of Tillaux Fractures
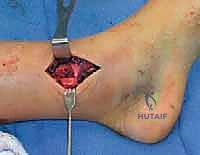
When a Tillaux fracture exhibits greater than 2 millimeters of displacement, ORIF is indicated. We utilize a targeted anterolateral approach, making a longitudinal incision centered over the anterolateral aspect of the distal tibia, directly over Chaput's tubercle. Careful subcutaneous dissection is performed to identify and mobilize the terminal branches of the superficial peroneal nerve.

The extensor retinaculum is incised, and the interval between the peroneus tertius and the extensor digitorum longus is developed. The joint capsule is opened to allow direct visualization of the articular surface. The fracture site is meticulously debrided of hematoma and any interposed periosteum using a dental pick or small curette. Reduction is achieved by internally rotating the foot while applying direct, posterior-to-anterior pressure on the avulsed anterolateral epiphyseal fragment using a dental pick or a small bone hook.

Once anatomic articular congruity is visually and fluoroscopically confirmed, provisional fixation is achieved with a smooth K-wire. Definitive fixation is then performed using a single, partially threaded cannulated screw (typically 3.5mm or 4.0mm). The crucial technical point here is the screw trajectory: it must be placed entirely within the epiphysis, running parallel to the articular surface from lateral to medial, strictly avoiding penetration of the open, medial aspect of the physis.
Open Reduction and Internal Fixation (ORIF) of Triplane Fractures
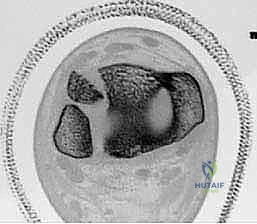
Triplane fractures are inherently complex, presenting as a Salter-Harris Type IV injury with distinct sagittal (epiphyseal), transverse (physeal), and coronal (metaphyseal) fracture lines. The surgical strategy must address both the intra-articular epiphyseal component and the structural metaphyseal component.

The approach is dictated by the location of the metaphyseal spike, which is most commonly posterior or posterolateral. An anterolateral approach is frequently utilized to address the epiphyseal (Tillaux-like) fragment. Reduction of the epiphyseal fragment often spontaneously reduces the metaphyseal component, as the fragments are intimately linked by the intact posterior hinge of periosteum. However, if the metaphyseal fragment remains displaced, a separate posterolateral or limited anteromedial approach may be required to clear interposed tissue and achieve reduction.

Fixation of a triplane fracture typically requires a two-screw construct. First, the epiphyseal fragment is secured with a partially threaded screw directed from lateral to medial, parallel to the joint space, identical to the Tillaux technique. Second, the metaphyseal spike is stabilized with an anterior-to-posterior (or posterior-to-anterior, depending on the approach) partially threaded screw placed entirely within the metaphysis, parallel to the physis. This "epiphyseal-metaphyseal" screw configuration provides rigid, orthogonal stability without violating the growth plate.

Medial Malleolar Fractures and Periosteal Entrapment
Displaced medial malleolar fractures (Salter-Harris Type III or IV) are notorious for periosteal entrapment. A posteromedial approach is utilized, curving the incision gently behind the medial malleolus. The saphenous vein and nerve are retracted anteriorly. The flexor retinaculum is identified, and deep dissection must meticulously protect the posterior tibial neurovascular bundle.

Upon exposing the fracture site, the surgeon will frequently encounter a dense, white, fibrous band of periosteum interposed within the phy
Clinical & Radiographic Imaging Archive




