Pilon Fracture ORIF: An Intraoperative Masterclass in Distal Tibial Reconstruction
Key Takeaway
Welcome, fellows, to an immersive intraoperative masterclass on open reduction and internal fixation of pilon fractures. We'll delve into comprehensive surgical anatomy, meticulous preoperative planning, and a granular, real-time breakdown of the surgical execution. Expect extensive pearls, pitfalls, and post-operative strategies to optimize outcomes for these complex distal tibial injuries. This guide ensures you grasp every critical detail for successful pilon fracture management.
Comprehensive Introduction and Patho-Epidemiology
The Pilon Concept and Mechanism of Injury
Welcome to the operating theater, colleagues. Today, we delve into one of the most formidable challenges in orthopaedic trauma: the pilon fracture. For the uninitiated, the terms "pilon" and "plafond" are frequently used interchangeably in the literature. They refer to the critical, weight-bearing articular surface of the distal tibia—the very ceiling of the ankle mortise. A fracture here is not merely a disruption of cortical bone; it is a devastating insult to the foundation of the ankle joint. The implications for patient mobility, long-term joint kinematics, and overall quality of life are profound. The mechanism of injury is predominantly high-energy axial loading. The dense, unyielding dome of the talus is driven with immense force into the distal tibial articular surface, acting much like a pestle in a mortar.

This catastrophic impact invariably results in significant metaphyseal comminution just proximal to the articular plafond. The force vector often dictates the fracture pattern; for instance, a foot in dorsiflexion during impact will frequently drive the anterior plafond into the adjacent metaphysis, creating severe anterior comminution. Conversely, lower-energy injuries—often rotational in nature—might present with a more spiral fracture pattern extending into the metaphysis or diaphysis. These lower-energy variants sometimes feature a distinct cortical spike that can serve as a valuable read for our anatomical reduction. Regardless of the energy level, our overarching goals, originally codified by Ruëdi and Allgöwer, remain absolute: precise articular reconstruction, restoration of extremity length and alignment, stable fracture fixation, and the facilitation of early joint motion to preserve cartilage viability.
Epidemiological Profile and Polytrauma Considerations
Before we even consider making an incision, we must contextualize the pilon fracture within the broader scope of the patient's trauma. These injuries are rarely isolated events. As orthopaedic surgeons, we must maintain a high index of suspicion and investigate thoroughly for associated injuries. Epidemiological data indicates that a significant 5% to 10% of these plafond fractures are bilateral, a scenario that drastically complicates post-operative rehabilitation and weight-bearing protocols. Furthermore, approximately 30% of our patients will present with ipsilateral lower extremity injuries. We must actively rule out concurrent tibial shaft fractures, calcaneal fractures, and ligamentous knee injuries that could be masked by the severe ankle trauma.

The axial skeleton is not immune to these high-energy forces; up to 15% of patients will have concomitant injuries to the spine, pelvis, or upper extremities. Therefore, a comprehensive trauma workup adhering strictly to Advanced Trauma Life Support (ATLS) protocols is absolutely non-negotiable. While pilon fractures are relatively uncommon—accounting for roughly 1% of all lower extremity fractures and 5% to 10% of all tibial fractures—their complexity demands mastery. Every orthopaedic surgeon exposed to trauma will inevitably encounter them, making a deep, nuanced understanding of their characteristics, classification, and management principles vital to your armamentarium.
Pathogenesis of Cartilage and Soft Tissue Injury
The true insidious nature of the pilon fracture lies not just in the shattered bone, but in the devastating trauma to the surrounding soft tissue envelope and the articular cartilage itself. The distal tibia is notorious for its precarious vascularity and minimal soft tissue coverage. In high-energy axial loading, the thin cutaneous and subcutaneous layers are crushed between the unyielding bone fragments and the external environment. This results in significant soft tissue contusion, fracture blisters, and a high risk of full-thickness necrosis. Recognizing that 20% to 40% of plafond fractures present as open injuries underscores the severe nature of the trauma and the critical need for aggressive, yet meticulous, soft tissue management.

Simultaneously, the articular cartilage undergoes a massive mechanical insult. The initial impact causes immediate chondrocyte death at the fracture margins, while the surrounding cartilage suffers from sub-lethal mechanical stress that can initiate a cascade of apoptosis and matrix degradation. Even with a perfectly executed, anatomically congruent surgical reduction, the initial cartilage impact energy is a primary determinant of long-term post-traumatic arthrosis. Our surgical intervention must therefore balance the mechanical necessity of rigid internal fixation against the biological imperative of preserving the tenuous blood supply to the metaphyseal fragments and the overlying integument.
Detailed Surgical Anatomy and Biomechanics
Osteology of the Distal Tibial Plafond and Ankle Mortise
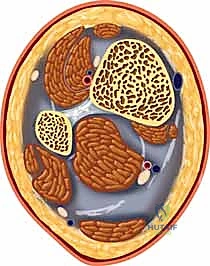
To successfully reconstruct a pilon fracture, one must possess an intimate, three-dimensional understanding of the distal tibial anatomy. The pilon is the concave, weight-bearing articular surface of the distal tibia, articulating with the convex dome of the talus. The talus itself is predominantly covered in articular cartilage and acts as a highly constrained ball bearing within the ankle mortise, restrained medially by the medial malleolus and laterally by the distal fibula. The tibial plafond is not a simple flat surface; it features a subtle sagittal ridge that corresponds to the central groove of the talar dome, providing intrinsic osseous stability to the joint.

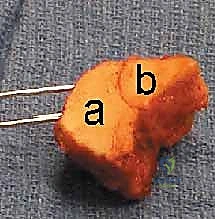
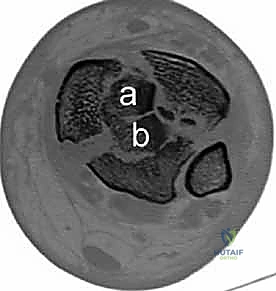
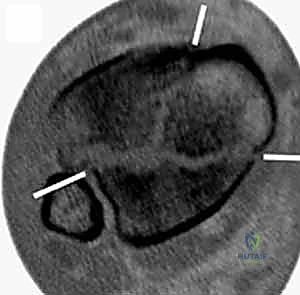
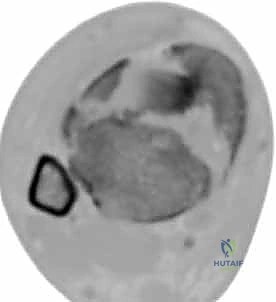
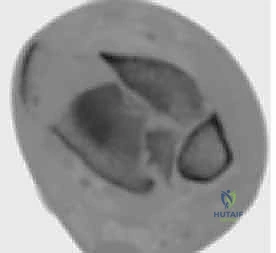
Research by Cole and colleagues, mapping complex articular (AO/OTA 43-C3) plafond fractures via high-resolution CT scans, revealed a remarkably consistent fracture pattern. They demonstrated that all complex fractures exited the tibiofibular joint laterally and at two separate locations medially. This forms a characteristic coronally oriented Y-pattern, typically creating three major articular fragments. Understanding this Y-pattern is the cornerstone of our reduction strategy. The three major fragments consist of a posterior plafond fragment (often remaining attached to the posterior syndesmotic ligaments), an anterolateral fragment (the tubercle of Chaput), and a medial malleolar fragment.

The Syndesmotic Complex and Fibular Interaction
In approximately 90% of pilon fractures, we will encounter an associated distal fibula fracture. This is not merely a bystander injury; it is a critical indicator of the energy imparted to the limb and plays a pivotal role in our reconstructive algorithm. The syndesmosis, the robust fibrous joint connecting the distal tibia and fibula, is functionally disrupted in the vast majority of pilon fractures due to the combination of the fibular fracture and the separation of the anterolateral tibial plafond. The anterolateral fragment contains the critical anteroinferior tibiofibular ligament (AITFL) attachment.

The biomechanical interplay here is crucial. The fibula acts as a lateral buttress and a template for tibial length and rotation. Often, the fibula must be addressed first to restore the lateral column, which indirectly aids in the reduction of the anterolateral tibial fragment via the intact AITFL (ligamentotaxis). By meticulously fixing both the fibula and the anterolateral plafond (Chaput's tubercle), we frequently restore the syndesmotic anatomy and function without the need for trans-syndesmotic screws. However, routine intraoperative stress testing of the syndesmosis remains mandatory after definitive fixation of the fibula and pilon to ensure absolute stability of the mortise.
Critical Neurovascular Anatomy and Muscular Intervals
Navigating the surgical approaches to the distal tibia requires strict adherence to internervous and intermuscular planes to avoid catastrophic iatrogenic injury. When utilizing the standard anteromedial approach, the saphenous vein and nerve are superficial structures that cross the operative field and must be meticulously mobilized and protected. The deep dissection typically exploits the interval between the tibialis anterior tendon (retracted laterally) and the medial crest of the tibia.

The anterolateral approach presents a higher density of at-risk structures. The superficial peroneal nerve courses subcutaneously over the distal fibula and the anterolateral aspect of the ankle. It is highly variable in its branching pattern and exquisitely susceptible to injury during the initial incision and superficial dissection. Deep to the extensor retinaculum, we must identify and protect the anterior tibial artery and the deep peroneal nerve, which lie between the extensor hallucis longus and the extensor digitorum longus. When working near the syndesmosis or applying anterolateral plates, extreme caution must be exercised to prevent retraction injuries to this neurovascular bundle. If a posteromedial or posterolateral approach is required for posterior malleolar or complex posterior pilon fragments, the posterior tibial artery, tibial nerve, and the flexor tendons within the tarsal tunnel are the critical structures commanding our respect.
Exhaustive Indications and Contraindications
Defining the Parameters for Operative Intervention
The decision to operate on a pilon fracture is rarely binary; it requires a nuanced assessment of the fracture morphology, the patient's physiological reserve, and, most importantly, the integrity of the soft tissue envelope. Operative intervention is generally indicated for all displaced, intra-articular fractures of the distal tibia to restore joint congruity and axial alignment. The goal is to prevent the rapid onset of post-traumatic arthrosis and to provide a stable construct that allows for early, active range of motion.
| Indication for Operative Fixation | Rationale and Clinical Objective |
|---|---|
| Articular Step-off > 2mm | Restores joint congruity to minimize abnormal contact stresses and delay post-traumatic osteoarthritis. |
| Axial Malalignment (Varus/Valgus > 5°) | Corrects mechanical axis to prevent eccentric loading of the ankle and knee joints. |
| Open Fractures | Requires immediate surgical debridement, irrigation, and stabilization to prevent deep sepsis and osteomyelitis. |
| Polytrauma / Damage Control | Early external fixation provides skeletal stability, aids in resuscitation, and facilitates nursing care in the ICU. |
| Syndesmotic Instability | Restores the anatomical mortise to prevent chronic talar shift and debilitating instability. |

While open reduction with internal fixation (ORIF) remains the gold standard for achieving anatomical articular reconstruction, the timing of this intervention is the most critical variable. We no longer rush these high-energy injuries to the operating room for immediate definitive plating. The modern standard of care mandates a staged approach. Initial management involves spanning external fixation to restore length and alignment, allowing the traumatized soft tissues to rest and recover. Definitive ORIF is delayed until the soft tissue envelope demonstrates readiness—typically indicated by the resolution of edema, the re-epithelialization of fracture blisters, and the return of skin wrinkling (the "wrinkle test"), which usually occurs 10 to 21 days post-injury.
Recognizing Absolute and Relative Contraindications
Recognizing when not to perform immediate or extensive internal fixation is a hallmark of a mature trauma surgeon. Absolute contraindications to immediate definitive ORIF include severe, unresuscitated polytrauma where the patient cannot tolerate a prolonged surgical procedure, and active, gross contamination or established infection at the surgical site. In these scenarios, damage control orthopedics with external fixation is the only acceptable immediate intervention.

Relative contraindications are heavily dependent on the host's physiological status and local tissue health. Severe peripheral vascular disease, uncontrolled diabetes mellitus with profound neuropathy (Charcot arthropathy risk), and active smoking significantly elevate the risk of wound dehiscence, deep infection, and nonunion. In patients with exceptionally poor bone stock (severe osteoporosis) or those who are non-ambulatory at baseline, the risks of complex articular reconstruction may outweigh the benefits. In such highly compromised hosts, alternative strategies such as definitive circular external fixation (Ilizarov technique) or even primary tibiotalar arthrodesis should be strongly considered as the primary definitive procedure.
The Role of Damage Control Orthopedics
The concept of Damage Control Orthopedics (DCO) is paramount in the management of high-energy pilon fractures. When a patient presents with a swollen, blistered, and ecchymotic ankle, making an incision through that compromised tissue is a recipe for catastrophic wound slough and deep bone infection. DCO dictates immediate skeletal stabilization via a spanning external fixator, typically a delta frame configuration utilizing calcaneal and tibial shaft Schanz pins.
This temporary construct serves multiple vital functions: it restores gross limb length, corrects severe angular deformities, and utilizes ligamentotaxis to partially reduce the articular fragments. Most importantly, it immobilizes the soft tissue envelope, drastically reducing ongoing mechanical trauma to the microvasculature and facilitating the resolution of edema. During this period, the limb is elevated, and meticulous wound care is provided. This staged protocol has revolutionized pilon fracture management, reducing historical deep infection rates from over 30% to less than 10% in modern trauma centers.
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities and Fracture Mapping
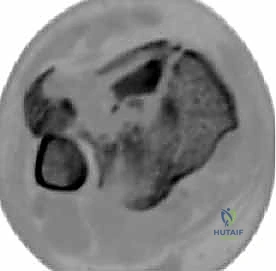
The complexity of pilon fractures renders standard orthogonal radiographs grossly inadequate for definitive surgical planning. While initial AP, lateral, and mortise views are necessary for the trauma bay assessment and external fixator application, a high-resolution, fine-cut Computed Tomography (CT) scan is absolutely mandatory prior to definitive ORIF. The CT scan must be obtained after the application of the spanning external fixator, as the ligamentotaxis will have partially reduced the fragments, providing a much clearer picture of the true articular comminution and the specific fracture lines.

We rely heavily on 2D axial, coronal, and sagittal reformats, alongside 3D surface-rendered reconstructions. The surgeon must mentally dissect the fracture, mapping out the trajectory of every primary fracture line. We look specifically for the Y-pattern described by Cole, identifying the posterior malleolar fragment, the anterolateral Chaput fragment, and the medial malleolar fragment. Furthermore, we must identify areas of central articular impaction—these "die-punch" fragments are entirely devoid of soft tissue attachments and must be elevated and bone-grafted to restore the articular contour. Failure to recognize and plan for these impacted fragments will result in a non-congruent joint and rapid arthrosis.
AO/OTA Classification and Pre-Operative Templating
Utilizing the Orthopaedic Trauma Association (OTA) alphanumeric system, derived from the AO/ASIF classification, is essential for standardized communication and academic rigor. Distal tibial fractures are designated as Type 43. We must accurately classify the injury: 43-A (Extra-articular), 43-B (Partial Articular), or 43-C (Complete Articular). The 43-C3 (Complete Articular, Multifragmentary) represents the zenith of complexity, requiring the most meticulous planning.

Once the fracture is mapped and classified, formal pre-operative templating is performed. This involves selecting the appropriate surgical approaches based on the location of the major fracture lines and the condition of the soft tissue. We select our implants—typically pre-contoured, anatomically specific locking plates for the distal tibia, and standard one-third tubular or locking plates for the fibula. We anticipate the need for bone graft or orthobiologics to fill metaphyseal voids created after the elevation of impacted articular segments. We also plan the sequence of reduction: will we fix the fibula first to restore length, or is the medial column more amenable to initial stabilization? This mental rehearsal is critical for a smooth intraoperative flow.
Operating Room Setup and Patient Positioning
Proper operating room setup and patient positioning are foundational to a successful pilon reconstruction. The patient is typically positioned supine on a radiolucent flat Jackson table or a standard operating table with a radiolucent extension. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the ankle mortise into a neutral, upward-facing position, which is particularly helpful for anterolateral and anteromedial approaches.
If a direct posterior or posterolateral approach is mandated by a large, displaced posterior articular fragment that cannot be reduced indirectly, the patient may need to be positioned prone or lateral decubitus. A sterile tourniquet is applied to the proximal thigh to ensure a bloodless field, though its inflation time must be strictly monitored to prevent ischemic complications. Fluoroscopy must be positioned to allow effortless AP, lateral, and mortise views without compromising the sterile field or the surgeon's working space. The external fixator, if present, is prepped into the field, as it may be utilized intraoperatively for continued distraction or provisionally removed to facilitate plate placement.
Step-by-Step Surgical Approach and Fixation Technique
Strategic Incision Planning and Soft Tissue Handling
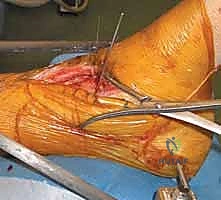
The surgical approach to the pilon fracture is dictated by the fracture morphology mapped on the pre-operative CT and the status of the soft tissue envelope. The cardinal rule of pilon surgery is absolute respect for the soft tissues. Incisions must be planned to allow direct access to the major fracture lines while maintaining adequate skin bridges (minimum of 7 cm) if multiple incisions are required. The anterolateral approach, utilizing the interval between the fibula and the extensor digitorum longus, provides excellent access to the Chaput fragment and the lateral articular surface.

Alternatively, the anteromedial approach provides superior visualization of the medial malleolus and the medial articular surface. Regardless of the approach, the dissection must be full-thickness down to the bone or joint capsule. We strictly avoid creating subcutaneous flaps, as this devascularizes the skin and drastically increases the risk of marginal necrosis. Retraction must be gentle and intermittent; self-retaining retractors should be used with extreme caution or avoided altogether in favor of handheld retractors managed by an attentive assistant. The periosteum should only be stripped minimally, just enough to visualize the fracture lines and apply the implants.

Fibular Reconstruction and Restoring the Lateral Column
In the vast majority of cases (approximately 90%), the surgical sequence begins with the open reduction and internal fixation of the fibula. This is a critical first step, as it restores the length of the lateral column and corrects external rotation deformity. By pulling the fibula out to length, we utilize the intact anteroinferior and posteroinferior tibiofibular ligaments to indirectly reduce the attached anterolateral and posterolateral fragments of the tibial plafond.

The fibula is typically approached via a direct lateral or posterolateral incision. The fracture is reduced anatomically, utilizing reduction forceps, and stabilized with a one-third tubular plate or a specifically designed distal fibula locking plate. If the fibula is highly comminuted, a bridge plating technique may be employed to preserve the biology of the fracture site, focusing on length, alignment, and rotation rather than anatomical reduction of every intermediate fragment. Once the fibula is rigid, we have established a stable template upon which to rebuild the tibial articular surface.

Articular Reduction and Provisional Fixation Strategies
With the lateral column restored, attention turns to the tibial plafond. The joint capsule is opened to allow direct visualization of the articular surface. A femoral distractor or the existing external fixator can be utilized to apply traction across the joint, opening the space and allowing visualization of the central articular impaction. The reduction sequence generally proceeds from posterior to anterior and lateral to medial.

First, the central "die-punch" oste
Clinical & Radiographic Imaging Archive