Masterclass: Open Reduction and Internal Fixation of Bicondylar Tibial Plateau Fractures

Key Takeaway
This masterclass guides fellows through open reduction and internal fixation of bicondylar tibial plateau fractures. We cover essential surgical anatomy, meticulous preoperative planning, and a granular, real-time intraoperative execution from the surgeon's perspective. Learn precise dissection, reduction techniques, hardware application, and critical pearls to optimize outcomes and manage potential complications for these complex injuries.
Comprehensive Introduction and Patho-Epidemiology
The management of bicondylar tibial plateau fractures remains one of the most formidable challenges in orthopedic traumatology. These injuries, representing a catastrophic failure of the proximal tibial articular surface and metaphyseal bone, demand an uncompromising understanding of knee biomechanics, spatial anatomy, and advanced osteosynthesis techniques. As orthopedic surgeons, our primary mandate when confronting these fractures is the absolute restoration of articular congruity, the re-establishment of the mechanical axis, and the provision of absolute stability to permit early, aggressive rehabilitation. Failure to achieve these tenets invariably condemns the patient to rapid post-traumatic arthrosis, profound joint stiffness, and severe functional disability.
Epidemiologically, bicondylar tibial plateau fractures exhibit a classic bimodal distribution. In the younger demographic, particularly males in their third and fourth decades, these fractures are almost exclusively the sequelae of high-energy mechanisms, such as motor vehicle collisions, motorcycle accidents, or falls from significant heights. These high-velocity impacts impart massive axial loading and shearing forces to the proximal tibia, resulting in severe osseous comminution and devastating soft tissue injury. Conversely, in the elderly, osteopenic or osteoporotic population, we increasingly encounter these complex fracture patterns following low-energy trauma, such as a simple fall from a standing height. In these instances, the compromised structural integrity of the subchondral bone fails under minimal physiologic loads, creating complex fracture geometries that are notoriously difficult to secure with standard internal fixation constructs.


Pathogenesis and Biomechanical Mechanisms
The pathogenesis of a bicondylar tibial plateau fracture is inextricably linked to the vector, magnitude, and duration of the applied force, as well as the position of the knee joint at the precise moment of impact. The primary deforming force is an overwhelming axial load. When the knee is in full extension, this axial force drives the femoral condyles squarely into the articular surface of the tibia, often resulting in a severe, symmetric bicondylar split-depression pattern. However, pure axial loading is rarely isolated; it is frequently coupled with significant varus or valgus moments. A valgus moment applied during axial loading preferentially drives the lateral femoral condyle into the lateral tibial plateau like a wedge, creating a classic lateral split and central depression, while simultaneously placing the medial collateral ligament (MCL) and medial plateau under extreme tensile and shear stress, ultimately culminating in a bicondylar failure.
Crucially, the modern orthopedic surgeon must possess a heightened awareness of the posteromedial shear fragment. Historically underappreciated, this specific fracture morphology occurs when the knee is subjected to an axial load while in a flexed and varus position. The medial femoral condyle shears off the posteromedial aspect of the tibial plateau. This is not merely a radiologic curiosity; it represents a highly unstable fracture-dislocation variant. The posteromedial fragment often encompasses the insertion of the posterior cruciate ligament (PCL) and the meniscotibial ligaments. Failure to recognize and independently stabilize this fragment with dedicated posterior or posteromedial buttress plating will inevitably lead to catastrophic posterior subluxation of the femur and rapid varus collapse of the mechanical axis, regardless of the robustness of the lateral fixation.
Furthermore, the resultant size, location, and degree of comminution of the fracture fragments are heavily dictated by the patient's intrinsic bone density. In young patients with dense, resilient cancellous bone, the energy is frequently dissipated through the creation of large, discrete fracture wedges and significant ligamentous avulsions. In contrast, osteoporotic bone tends to undergo severe, microscopic crushing and impaction, resulting in profound central articular depression with a thin, fragile subchondral shell that offers minimal purchase for standard screw fixation, necessitating the use of locked plating technology and extensive bone grafting.
Classification Systems and Clinical Relevance
To effectively communicate and formulate operative strategies, a rigorous application of classification systems is mandatory. The Schatzker classification remains the most universally utilized framework in clinical practice. Within this system, bicondylar injuries are categorized as Types V and VI. A Schatzker Type V fracture denotes a bicondylar injury where the medial and lateral articular segments are fractured, but crucially, there remains a continuity between the articular block and the tibial diaphysis. These fractures, while severe, often preserve a central pillar of intact bone, which can be leveraged during reduction.
In stark contrast, the Schatzker Type VI fracture is defined by complete metaphyseal-diaphyseal dissociation. In this catastrophic injury, the entire articular block is completely severed from the tibial shaft, effectively rendering the knee joint floating. This pattern implies a significantly higher energy transfer, massive soft tissue stripping, and profound instability. The surgical approach to a Type VI injury is inherently more complex, often requiring extensive dual plating to bridge the metaphyseal-diaphyseal defect and restore the mechanical axis.
While the Schatzker system is invaluable, the AO/OTA classification provides a more granular, alphanumeric categorization that is essential for academic research and precise surgical auditing. Bicondylar fractures fall under the 41-C category (complete articular fractures). These are further subdivided into C1 (articular simple, metaphyseal simple), C2 (articular simple, metaphyseal multifragmentary), and C3 (articular multifragmentary). The C3 variant, representing the most complex morphology with extreme articular comminution, tests the limits of surgical reconstruction. Furthermore, modern CT-based classifications, such as the Luo three-column concept, have revolutionized our understanding by dividing the plateau into medial, lateral, and posterior columns. This three-dimensional conceptualization is critical, as it mandates that each fractured column must be independently addressed and stabilized to prevent multi-planar collapse.
Detailed Surgical Anatomy and Biomechanics
A profound, almost instinctual mastery of the regional anatomy of the proximal tibia is the absolute prerequisite for any surgeon undertaking the open reduction and internal fixation of a bicondylar plateau fracture. The surgical theater in this region is a densely packed, highly unforgiving anatomical crossroad where critical neurovascular structures, complex ligamentous restraints, and intricate osseous architecture converge. Navigating this terrain requires meticulous dissection, precise retractor placement, and an unwavering respect for the soft tissue envelope.


Osteology and Articular Architecture
The proximal tibia is an asymmetric osseous expansion designed to receive and dissipate the massive loads transmitted across the knee joint. The medial tibial plateau is the primary load-bearing surface. It is anatomically larger, concave in both the sagittal and coronal planes, and supported by bone that is significantly denser and stronger than its lateral counterpart. During the normal gait cycle, the medial plateau sustains approximately 60% to 75% of the total compressive force. This inherent concavity and dense subchondral architecture make it relatively resistant to pure depression fractures; instead, it typically fails in a shear-split pattern.
Conversely, the lateral tibial plateau is smaller, sits slightly higher anatomically, and is distinctly convex in the sagittal plane. The subchondral bone here is notably thinner and more porous. Consequently, the lateral plateau is highly susceptible to depression and impaction injuries when struck by the convex lateral femoral condyle. Understanding these morphological differences is critical during surgical reconstruction. Elevation of the lateral plateau often leaves a massive cavitary void that mandates structural bone grafting to prevent post-operative subsidence, whereas the medial plateau often requires robust anti-glide plating to resist shear forces.
The restoration of the native angular relationships of the proximal tibia is non-negotiable. The medial proximal tibial angle (MPTA), typically measuring 87 degrees (range 85-90 degrees) relative to the anatomical axis of the tibia, dictates the coronal plane alignment. Failure to restore the MPTA results in mechanical axis deviation, leading to asymmetric joint loading and accelerated unicompartmental arthrosis. Equally critical is the proximal posterior tibial angle (PPTA), which defines the posterior slope of the articular surface, averaging 81 degrees (range 77-84 degrees). This posterior slope is a fundamental determinant of knee kinematics, particularly sagittal plane stability and cruciate ligament tension. An iatrogenic alteration of the PPTA can result in profound anterior or posterior instability, severely compromising the functional outcome.

Ligamentous Restraints and Meniscal Integration
The osseous structures of the knee are intrinsically unstable without the complex network of ligamentous restraints and meniscal cushions. In the context of bicondylar fractures, concomitant soft tissue injuries are extraordinarily common, with incidences reported between 20% and 77%. The Anterior Cruciate Ligament (ACL), inserting adjacent to the medial anterior aspect of the tibial eminence, is frequently avulsed with a bony fragment in high-energy trauma. Recognizing and securing this eminence fragment is paramount to restoring anterior translational stability. The Posterior Cruciate Ligament (PCL) inserts on the posterior tibial sulcus, approximately 1 cm distal to the joint line. As previously noted, the PCL insertion is frequently compromised in posteromedial shear fractures, and failure to stabilize this region leads to catastrophic posterior sag and varus instability.
The collateral ligaments provide critical coronal plane stability. The Medial Collateral Ligament (MCL), a broad, robust structure, is the primary restraint to valgus stress. While mid-substance MCL tears can occur, we frequently observe bony avulsions or severe stretching in the setting of bicondylar injuries. The Lateral Collateral Ligament (LCL), a cord-like structure originating from the lateral femoral epicondyle and inserting on the fibular head, resists varus stress. Injury to the LCL, often part of a broader posterolateral corner (PLC) injury, significantly complicates the management of lateral plateau fractures and must be meticulously evaluated.
The menisci are vital fibrocartilaginous structures that dramatically increase the contact area between the femur and tibia, thereby reducing peak contact stresses by up to 50%. The medial meniscus is C-shaped and intimately attached to the deep fibers of the MCL, making it less mobile and more prone to tearing during shear injuries. The lateral meniscus is more circular, covers a larger portion of the articular surface, and is significantly more mobile. During the surgical approach, particularly the submeniscal arthrotomy, the menisci must be carefully elevated and protected. Peripheral meniscal detachments are common and must be meticulously repaired to the joint capsule following fracture fixation to prevent rapid chondrolysis and early osteoarthritis.
Critical Neurovascular Topography
The surgical approaches to the proximal tibia are fraught with neurovascular hazards. A deep, three-dimensional understanding of these structures is essential to prevent devastating iatrogenic complications. On the medial side, the saphenous nerve and the great saphenous vein course superficially. During the posteromedial approach, these structures must be identified early and gently retracted anteriorly. Injury to the saphenous nerve results in painful neuromas and sensory deficits along the medial aspect of the leg and foot, while damage to the vein can exacerbate post-operative edema and increase the risk of deep vein thrombosis.
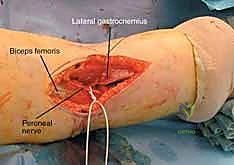
The lateral side harbors the common peroneal nerve, a structure of paramount concern. The nerve courses distally from the popliteal fossa, wrapping tightly around the fibular neck before diving into the anterior and lateral compartments of the leg. It is highly vulnerable to traction injuries during severe varus trauma and is at significant iatrogenic risk during extensive lateral dissection, retractor placement, or the application of lateral plates that extend distally. The nerve provides motor innervation for ankle dorsiflexion and foot eversion; an injury here results in a devastating foot drop. Preoperative, intraoperative, and postoperative assessment of peroneal nerve function is an absolute medicolegal and clinical imperative.
Deep within the posterior aspect of the knee lies the popliteal neurovascular bundle, comprising the popliteal artery and vein. While typically protected by the posterior joint capsule and the popliteus muscle mass, severe bicondylar fractures—particularly those with significant posterior displacement, profound comminution, or a fracture-dislocation component—can tether, lacerate, or occlude these massive vessels. The popliteal artery is rigidly tethered proximally by the adductor hiatus and distally by the soleal arch, making it highly susceptible to stretch injuries. Vascular injury occurs in approximately 2% of tibial plateau fractures, but the consequences of a missed injury are catastrophic, frequently resulting in limb amputation. A high index of suspicion and a low threshold for advanced vascular imaging are mandatory.
Exhaustive Indications and Contraindications
The decision-making process regarding the operative versus non-operative management of bicondylar tibial plateau fractures is complex and must be highly individualized. It requires a delicate balancing act between the mechanical demands of the fracture, the physiological reserve of the patient, and the condition of the surrounding soft tissue envelope. As a general principle, the vast majority of bicondylar fractures (Schatzker V and VI) represent inherently unstable, high-energy injuries that mandate surgical stabilization to achieve a functional outcome.
Operative Thresholds and Patient Selection
Operative intervention is definitively indicated to restore articular congruity, re-establish the mechanical axis, and provide sufficient stability to allow for early range of motion. The classic radiographic parameters dictating surgical intervention include an articular step-off or depression exceeding 2 to 3 millimeters, condylar widening or displacement greater than 5 millimeters, and any degree of coronal or sagittal plane instability exceeding 10 degrees when compared to the contralateral, uninjured knee. Furthermore, any fracture pattern that prevents the patient from achieving full, active knee extension due to mechanical block or severe pain is a definitive candidate for surgery.
Beyond radiographic parameters, absolute indications for immediate or urgent surgical intervention include open fractures, fractures associated with acute compartment syndrome, and injuries with concomitant vascular compromise requiring repair. In these scenarios, the orthopedic surgeon must work in tandem with trauma and vascular surgery teams to perform immediate skeletal stabilization, typically via spanning external fixation, to protect the vascular repair and allow for soft tissue management.
Patient selection is equally critical. The ideal surgical candidate is a physiologically robust individual capable of adhering to a strict, prolonged non-weight-bearing rehabilitation protocol. However, even in the elderly or physiologically compromised patient, operative intervention is often necessary, as the alternative—prolonged immobilization in a cast or brace—frequently leads to catastrophic joint stiffness, pressure ulcerations, deep vein thrombosis, and a profound loss of independent mobility. In these high-risk populations, the surgical goals may shift from perfect anatomic restoration to achieving a stable, aligned limb that permits early mobilization, often utilizing minimally invasive techniques or robust locked plating constructs designed to withstand osteoporotic bone failure.
| Category | Specific Parameters and Scenarios |
|---|---|
| Absolute Indications for Surgery | - Open fractures (requires urgent debridement/stabilization). - Acute Compartment Syndrome (requires emergent fasciotomy). - Associated vascular injury requiring repair. - Articular step-off/depression > 3mm. - Condylar widening > 5mm. - Varus/Valgus instability > 10 degrees. |
| Relative Indications | - Polytrauma patient requiring mobilization. - Floating knee injuries (ipsilateral femur fracture). - Bilateral tibial plateau fractures. |
| Absolute Contraindications | - Patient medically unfit for anesthesia (e.g., severe recent MI). - Active, severe local infection over the surgical site. - Irreversible limb ischemia (amputation indicated). |
| Relative Contraindications | - Severe soft tissue compromise (blisters, profound edema) - Indicates delay of definitive ORIF, mandates spanning ex-fix. - Non-ambulatory baseline status. - Severe, pre-existing end-stage osteoarthritis (consider primary arthroplasty). |
Non-Operative Management and Natural History
Non-operative management of true bicondylar tibial plateau fractures is exceedingly rare in modern orthopedic practice and is generally reserved for a very specific, limited patient cohort. Indications for conservative care include non-displaced or minimally displaced fractures that demonstrate absolute stability on stress examination, or patients whose profound medical comorbidities present an unacceptable risk for anesthesia and major surgery. Furthermore, non-ambulatory patients with minimal functional demands may be managed non-operatively, prioritizing pain control over anatomic restoration.
When non-operative management is elected, it typically involves a period of immobilization in a hinged knee brace locked in extension, or a long-leg cast. This is followed by a meticulously monitored, highly restrictive weight-bearing protocol. The natural history of inadequately treated or non-operatively managed displaced bicondylar fractures is uniformly poor. The inherent instability of the fracture pattern inevitably leads to progressive varus or valgus collapse under physiologic loads.
This mechanical axis deviation dramatically alters the contact stresses across the knee joint, leading to rapid, asymmetric cartilage wear and profound post-traumatic arthrosis. Furthermore, prolonged immobilization invariably results in severe arthrofibrosis, capsular contracture, and permanent loss of knee flexion and extension. The patient is often left with a painful, stiff, deformed, and highly dysfunctional limb, ultimately requiring complex, technically demanding salvage procedures such as intra-articular oste
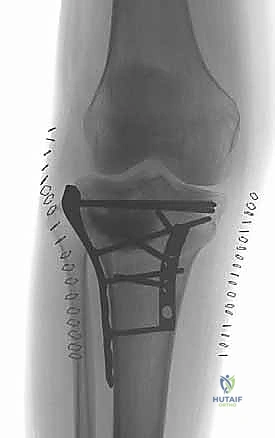
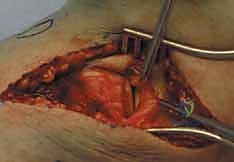
Clinical & Radiographic Imaging Archive