Open Reduction and Internal Fixation of Peritrochanteric Hip Fractures: An Intraoperative Masterclass
Key Takeaway
Welcome to the OR, fellows. Today, we're tackling peritrochanteric hip fractures. This masterclass will guide you through comprehensive surgical anatomy, meticulous preoperative planning, and a granular, real-time intraoperative execution of Open Reduction and Internal Fixation. We'll cover critical pearls, potential pitfalls, and essential postoperative management to ensure optimal patient outcomes and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
Definition and Natural History
Peritrochanteric hip fractures represent a critical, high-volume challenge in the daily practice of an orthopedic surgeon. By strict anatomic definition, these are extracapsular fractures occurring in the proximal femur, definitively involving the trochanteric region and frequently extending distally into the subtrochanteric area. This extracapsular designation is of paramount clinical importance; unlike intracapsular femoral neck fractures, the peritrochanteric region boasts a robust, redundant vascular supply derived from the extracapsular arterial ring. Consequently, osteonecrosis of the femoral head is an exceptionally rare complication, and the primary biological challenge is not achieving union, but rather achieving union in an anatomically and biomechanically stable alignment.
Without operative intervention, the natural history of a peritrochanteric fracture is characterized by universal healing, albeit with profound and debilitating malunion. The proximal femur is subject to massive deforming forces from the surrounding pelvic and thigh musculature. Left unchecked, these forces invariably drive the fracture into severe varus, profound shortening, and fixed external rotation. Historically, before the advent of modern internal fixation, this resulted in a permanently shortened, mechanically disadvantaged limb, relegating patients to severe functional limitations, chronic pain, and a drastically diminished quality of life.

Today, the overarching goal of early operative intervention—specifically open reduction and internal fixation (ORIF) or cephalomedullary nailing—is to neutralize these deforming forces, restore the native neck-shaft angle, and re-establish the mechanical axis of the lower extremity. By achieving stable anatomic or near-anatomic reduction, we facilitate immediate postoperative weight-bearing. This early mobilization is the linchpin of modern geriatric fracture care, drastically reducing the catastrophic systemic complications associated with prolonged recumbency, such as deep vein thrombosis, pulmonary embolism, decubitus ulcers, and hypostatic pneumonia.
Furthermore, the evolution of modern implant design has shifted the paradigm from rigid anatomic fixation to dynamic, load-sharing constructs. The sliding hip screw and the modern cephalomedullary nail both allow for controlled impaction of the fracture fragments along the axis of the femoral neck. This dynamic compression harnesses the physiological loading of weight-bearing to promote secondary bone healing, effectively utilizing the patient's own body weight to enhance the mechanical stability of the bone-implant construct over time.
Clinical Presentation and Initial Assessment
The classic clinical presentation of a patient sustaining a peritrochanteric hip fracture is unmistakable to the trained eye: the affected lower extremity lies in a shortened and excessively externally rotated position. This pathognomonic deformity is a direct biomechanical consequence of the unopposed muscle forces acting upon the uncoupled proximal and distal femoral fragments. The iliopsoas violently flexes and externally rotates the proximal fragment, while the adductor magnus, longus, and brevis pull the distal femoral shaft proximally and medially, exacerbating the varus collapse and limb shortening.

Initial assessment must extend far beyond the obvious orthopedic deformity. The vast majority of these patients are elderly, frail, and harbor a multitude of complex medical comorbidities. It is imperative to ascertain the precise etiology of the fall. A mechanical trip is common, but one must maintain a high index of suspicion for syncopal episodes, acute arrhythmias, cerebrovascular accidents, or severe orthostatic hypotension. A multidisciplinary approach, immediately involving geriatricians or hospitalists, is critical to optimize the patient for surgical intervention within the strongly recommended 24 to 48-hour window.
A comprehensive secondary musculoskeletal survey is absolutely mandatory in this patient population. The severe, distracting pain emanating from the fractured hip can easily mask concomitant injuries. Elderly patients frequently sustain associated distal radius fractures, proximal humerus fractures, or occult cervical spine trauma during the index fall. Missing these injuries can severely complicate postoperative rehabilitation protocols that rely heavily on upper extremity weight-bearing for walker or crutch use.
Meticulous inspection of the soft tissue envelope, particularly over the greater trochanter, sacrum, and heels, is necessary to identify impending pressure necrosis or traumatic abrasions. Any compromise to the integument overlying the proposed surgical incision could dictate an alternative surgical approach or elevate the risk of postoperative surgical site infection. Furthermore, a thorough neurovascular examination of the affected extremity must be documented prior to any reduction maneuvers or application of skin traction, establishing a baseline for postoperative comparison.
Pathogenesis and Etiology
The pathogenesis of peritrochanteric fractures is fundamentally bimodal, dictated primarily by the patient's age and intrinsic bone quality. In the geriatric population, these fractures are overwhelmingly the result of low-energy trauma, typically a simple fall from a standing height directly onto the lateral aspect of the greater trochanter. The underlying culprit is osteoporosis, which critically thins the primary compressive trabeculae and weakens the calcar femorale. Combined with age-related sarcopenia, diminished protective reflexes, and decreased subcutaneous adipose padding, the proximal femur is rendered highly susceptible to failure under relatively minor torsional or compressive loads.

Conversely, peritrochanteric fractures in young, healthy adults are almost exclusively the domain of high-energy trauma. Motor vehicle collisions, motorcycle accidents, and falls from significant heights generate the massive kinetic energy required to shatter healthy, dense cortical bone. These high-energy injuries are frequently associated with severe soft tissue trauma, extensive comminution, and a high incidence of concomitant life-threatening injuries, necessitating rigorous adherence to Advanced Trauma Life Support (ATLS) protocols prior to definitive orthopedic management.
Additionally, the orthopedic surgeon must remain vigilant for pathologic fractures. Metastatic disease (commonly from breast, prostate, lung, thyroid, or renal primary tumors), multiple myeloma, or primary bone sarcomas frequently target the highly vascularized proximal femur. A fracture pattern that appears unusually transverse, occurs with trivial trauma, or is preceded by a history of insidious, deep thigh pain should immediately raise suspicion for a pathologic etiology.
This pathologic suspicion necessitates a vastly different preoperative workup, including advanced cross-sectional imaging, whole-body bone scintigraphy, and potentially prophylactic stabilization of the entire femur. Biopsy of the lesion prior to or concurrent with fixation is often required. The surgical strategy in pathologic fractures shifts from achieving bony union (which may never occur) to providing a durable, life-long mechanical construct that allows immediate, unrestricted weight-bearing, often requiring longer cephalomedullary nails or the augmentation of fixation with polymethylmethacrylate (PMMA) bone cement.
Detailed Surgical Anatomy and Biomechanics
Osteology and Trabecular Architecture
The intertrochanteric region serves as the critical biomechanical junction where the femoral neck transitions into the diaphyseal shaft. Understanding its complex osteology is the foundation of successful internal fixation. The native neck-shaft angle, subtended by the axis of the femoral neck and the anatomical axis of the femoral shaft in the coronal plane, typically ranges from 125 to 135 degrees. Restoration of this angle is paramount; failure to do so, particularly leaving the fracture in varus, exponentially increases the bending moment on the implant, drastically elevating the risk of hardware cutout and catastrophic mechanical failure.

Equally important is the concept of femoral anteversion. The femoral neck projects anteriorly relative to the transcondylar axis of the distal femur, averaging 10 to 15 degrees of anteversion. Recognizing this three-dimensional anatomy is essential during the placement of guide pins for sliding hip screws or cephalomedullary nails. The surgeon must meticulously direct the hardware perfectly into the center-center position of the femoral head, respecting this native anteversion to avoid eccentric placement that predisposes to implant cutout.
The internal architecture of the peritrochanteric region is characterized by distinct, predictable patterns of trabecular bone designed to withstand complex physiological loads. The most structurally vital of these is the primary compressive trabecular group, which condenses along the posteromedial aspect of the femoral neck to form the calcar femorale. This dense column of bone acts as the primary buttress against varus collapse. When a fracture disrupts the calcar (an "unstable" fracture pattern), the surgeon must rely heavily on the implant to bear the load until bony union occurs.

Conversely, the lateral femoral wall plays a critical role in resisting lateral translation of the proximal fragment. Recent biomechanical literature has heavily emphasized the integrity of the lateral wall in determining fracture stability. If the lateral wall is deficient or fractured during the insertion of a sliding hip screw, the proximal fragment can slide laterally unchecked, leading to profound medialization of the femoral shaft and construct failure. In such lateral wall-deficient patterns, a cephalomedullary nail is biomechanically superior, acting as an intramedullary buttress to prevent this lateral translation.
Muscular Attachments and Deforming Forces
The proximal femur is the anchor point for some of the most powerful musculature in the human body, and understanding these attachments is crucial for deciphering fracture displacement and executing closed reduction maneuvers. The lesser trochanter serves as the sole insertion site for the iliopsoas tendon. When the lesser trochanter is avulsed or remains attached to the proximal fragment, the unopposed pull of the iliopsoas violently flexes and externally rotates the proximal segment, making anatomical reduction incredibly challenging without specific counter-maneuvers.

The greater trochanter is the confluence of the hip abductors and short external rotators. The gluteus medius and minimus insert onto the lateral and anterior facets, respectively, while the piriformis, obturator internus, and gemelli insert more posteriorly. In a displaced fracture, these muscles exert a strong abducting and externally rotating force on the proximal fragment. If the greater trochanter is highly comminuted, the abductor mechanism is compromised, leading to a profound postoperative Trendelenburg gait and significant functional impairment even if the bony fracture heals perfectly.

Distally, the massive adductor muscle group (adductor longus, brevis, and magnus) originates from the pubis and ischium and inserts along the linea aspera of the posterior femoral shaft. In the setting of a peritrochanteric fracture, these muscles act as powerful deforming forces, pulling the distal femoral shaft proximally and medially. This unopposed adductor pull is the primary driver of the profound shortening and varus deformity characteristic of these injuries, requiring significant longitudinal traction and lateral translation to overcome during the reduction process.
Understanding these vectors is not merely an academic exercise; it dictates the intraoperative reduction strategy. To counteract the iliopsoas, the leg is often placed in slight extension. To counteract the external rotators, internal rotation is applied to the distal fragment via the traction boot. Overcoming the adductors requires sustained longitudinal traction. Mastery of these muscular deforming forces allows the surgeon to perform a "tissue-sparing" closed reduction on the fracture table prior to ever making an incision.
Neurovascular Considerations
While the robust blood supply to the peritrochanteric region ensures a high rate of fracture union, it also presents specific intraoperative challenges regarding hemostasis. The primary arterial supply is derived from the medial and lateral femoral circumflex arteries, branches of the profunda femoris. The lateral femoral circumflex artery sends transverse branches that wrap around the anterior base of the femoral neck, supplying the vastus lateralis origin and the anterior capsule. Surgical approaches inevitably encounter these vessels, requiring meticulous electrocautery to prevent significant postoperative hematoma.

Furthermore, as the surgeon incises and elevates or splits the vastus lateralis to expose the lateral femoral cortex, multiple perforating branches from the profunda femoris artery will be encountered. These perforators pierce the lateral intermuscular septum and enter the vastus lateralis. Failure to systematically identify, isolate, and ligate or coagulate these perforators can lead to torrential bleeding, obscuring the surgical field and leading to significant, preventable blood loss in an already physiologically fragile patient population.
Neurologically, the standard lateral approach to the proximal femur is exceptionally safe, keeping the surgeon well clear of major nerve trunks. The femoral nerve lies far anteriorly within the femoral triangle, protected by the iliopsoas and rectus femoris. The sciatic nerve courses posteriorly, deep to the gluteus maximus and short external rotators.

However, extreme caution must be exercised during deep posterior retraction or if the fracture pattern necessitates a more posterior dissection. Aggressive placement of Hohmann retractors behind the posterior rim of the acetabulum or proximal femur can inadvertently compress or stretch the sciatic nerve, leading to devastating postoperative neuropraxia. Additionally, prolonged use of a hard perineal post on the fracture table can result in pudendal nerve palsy, emphasizing the need for adequate padding and minimizing the duration of extreme traction.
Exhaustive Indications and Contraindications
Operative Indications and Timing
The operative stabilization of peritrochanteric hip fractures is universally recognized as the gold standard of care. The primary indication for surgery is the diagnosis of the fracture itself in any patient who was ambulatory prior to the injury. The physiological rationale is irrefutable: early surgical stabilization allows for immediate mobilization, effectively mitigating the lethal cascade of complications associated with prolonged bed rest in the elderly. Extensive literature demonstrates that operative intervention significantly reduces one-year mortality rates, decreases the incidence of deep vein thrombosis, and dramatically improves the likelihood of returning to pre-injury functional status.

Timing of the surgical intervention is a critical metric of quality care. Current evidence-based guidelines strongly advocate for surgical fixation within 24 to 48 hours of admission. Delays beyond 48 hours are independently associated with exponentially increased rates of major complications, including pneumonia, urinary tract infections, pressure ulcers, and overall mortality. However, this urgency must be carefully balanced against the need for adequate medical optimization. "Rush to the OR" should not supersede the correction of life-threatening coagulopathies, severe electrolyte derangements, or acute heart failure exacerbations.
In younger patients with high-energy peritrochanteric fractures, the indications remain the same, but the biological goals shift slightly. While early mobilization is still important, the paramount goal in this demographic is achieving absolute anatomical reduction and rigid fixation to ensure perfect restoration of limb length, alignment, and rotation, thereby preventing post-traumatic arthritis and maximizing long-term athletic and occupational function. In these cases, open reduction techniques are more frequently utilized to guarantee anatomic restoration.
Nonoperative Management and Relative Contraindications
While exceedingly rare in modern orthopedic practice, there are highly specific, narrow clinical scenarios where nonoperative management of a peritrochanteric fracture is the most appropriate, humane course of action. The primary indication for nonoperative care is a patient who is actively dying or has a life expectancy measured in days to weeks due to end-stage systemic disease. In these palliative scenarios, the trauma of surgery and anesthesia outweighs any theoretical benefit, and management focuses entirely on aggressive pain control and comfort care.

Another relative contraindication is a patient with an unacceptably high anesthetic risk, such as those with recent massive myocardial infarction, severe uncorrectable coagulopathy, or acute florid sepsis. In these instances, surgery must be delayed until the acute medical crisis is resolved. If the medical condition is permanently uncorrectable, nonoperative management may be forced upon the surgical team. This involves skeletal traction or prolonged bed rest, accepting the exceptionally high morbidity and mortality associated with this path.

Interestingly, non-ambulatory status prior to the fracture (e.g., a bed-bound patient with severe advanced dementia) is not an absolute contraindication to surgery. Many orthopedic surgeons advocate for operative fixation even in non-ambulators, as stabilizing the fracture drastically reduces pain, facilitates easier nursing care (turning, hygiene), and allows the patient to sit up in a chair, thereby improving pulmonary toilet and overall quality of remaining life.
| Operative Indications | Relative Contraindications | Absolute Contraindications |
|---|---|---|
| Any ambulatory patient with a displaced or nondisplaced peritrochanteric fracture | Severe, uncorrectable medical comorbidities (e.g., acute MI, florid heart failure) | Active, untreated infection in the surgical field |
| Bed-bound patients requiring pain control and facilitation of nursing care | Life expectancy < 4 weeks (palliative care pathway preferred) | Patient actively dying / comfort measures only |
| Pathologic fractures requiring stabilization | Extreme uncorrectable coagulopathy | Refusal of surgery by a competent patient or proxy |
| High-energy fractures in young adults | Pre-existing overwhelming systemic sepsis |
Pre-Operative Planning, Templating, and Patient Positioning
Imaging and Digital Templating
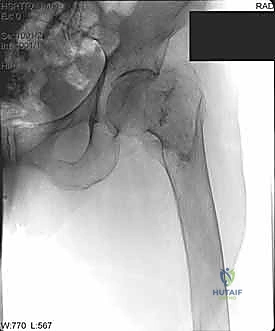
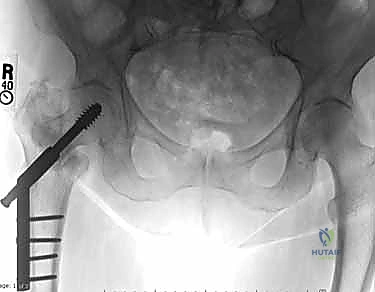
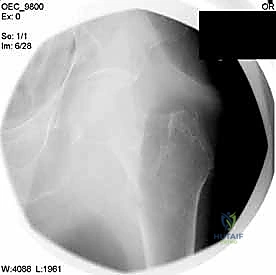
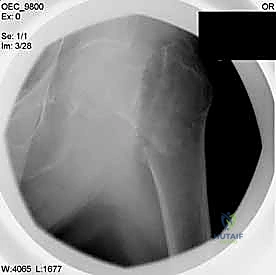
Meticulous preoperative planning is the hallmark of the master orthopedic surgeon. The standard imaging series includes an anteroposterior (AP) view of the pelvis to allow comparison with the contralateral, uninjured hip, and a cross-table lateral view of the affected proximal femur. In cases of high-energy trauma or suspected pathologic lesions, full-length orthogonal radiographs of the entire femur are mandatory to rule out synchronous diaphyseal or distal femoral lesions that would completely alter the implant choice (e.g., necessitating a long cephalomedullary nail instead of a short nail or sliding hip screw).

Digital templating software has revolutionized preoperative preparation. The surgeon must template the uninjured contralateral hip to determine the native neck-shaft angle, which dictates the angle of the implant to be chosen (commonly 125, 130, or 135 degrees). Templating also allows for the precise estimation of the lag screw length required to achieve a Tip-Apex Distance (TAD) of less than 25 millimeters, and determines the appropriate diameter of the cephalomedullary nail to ensure a secure diaphyseal fit without risking iatrogenic fracture of the anterior femoral cortex due to a mismatch in the radius of curvature.
Furthermore, the surgeon must critically analyze the fracture pattern to determine stability. The presence of a posteromedial void (calcar comminution), a fractured lateral wall, or subtrochanteric extension classifies the fracture as highly unstable. In these scenarios, the preoperative plan must pivot definitively towards a cephalomedullary device, as extramedullary sliding hip screws have an unacceptably high failure rate in lateral wall-deficient or reverse obliquity fracture patterns.
Anesthesia and Patient Optimization
The choice of anesthesia—regional (spinal) versus general—has been a subject of intense debate. Current extensive literature and large registry data suggest that while regional anesthesia may offer slight early benefits in reducing postoperative delirium and deep vein thrombosis, there is no significant difference in long-term mortality. The decision should be highly individualized, made collaboratively between the anesthesiologist, the surgeon, and the patient, factoring in the patient's cardiopulmonary reserve, coagulation status, and ability to lie flat and still during the procedure.
Blood management protocols are initiated in the preoperative phase. Peritrochanteric fractures can bleed significantly into the thigh compartments prior to surgery. A baseline hemoglobin should be assessed, and cross-matched blood should be available. The routine administration of intravenous Tranexamic Acid (TXA) at the time of incision, barring strict medical contraindications (such as active thromboembolic disease), has been proven to significantly reduce intraoperative and postoperative blood loss, thereby decreasing the need for allogeneic blood transfusions.
Optimization of medical comorbidities is a dynamic, fast-paced process. Geriatric co-management models have proven exceptionally effective. The goal is not to "clear" the patient—as a frail 85-year-old with a broken hip is never truly "cleared"—but to optimize their physiology. This includes correcting electrolyte imbalances, managing acute kidney injury from dehydration, and rapidly reversing anticoagulation if the patient is on warfarin or direct oral anticoagulants (DOACs), utilizing specific reversal agents or prothrombin complex concentrates (PCC) to safely meet the 24-48 hour surgical window.
Patient Positioning and Fluoroscopy Setup
Proper patient positioning is arguably the most critical step of the entire operation; a poor setup guarantees a difficult surgery. The vast majority of surgeons utilize a specialized orthopedic fracture table. The patient is transferred supine, and the feet are securely strapped into traction boots. A well-padded perineal post is placed between the legs to provide counter-traction. It is vital to ensure the post is resting against the ischial tuberosity and not compressing the soft tissues of the perineum to avoid devastating pudendal nerve palsies or soft tissue sloughing.

The uninjured leg is typically placed in a "scissor" position—extended and dropped posteriorly, or flexed and abducted in a hemi-lithotomy position—to allow the C-arm fluoroscopy unit unhindered access for perfectly orthogonal lateral imaging. The C-arm is brought in from the unaffected side. The surgeon must verify that perfect AP and true lateral images of the proximal femur and femoral head can be obtained effortlessly before the patient is prepped and draped. Time spent optimizing the fluoroscopic views preoperatively saves exponential amounts of time and frustration during the critical phases of implant placement.
Once positioned, closed reduction is attempted using the mechanisms of the fracture table. Longitudinal traction is applied to restore length, overcoming the adductor pull. The leg is then internally rotated (usually 10 to 15 degrees) to overcome the external rotators and bring the anteverted femoral neck parallel to the floor, presenting a true AP profile on fluoroscopy. The reduction is critically assessed on both AP and lateral views. If an acceptable closed reduction cannot be achieved, the surgeon must be prepared to execute percutaneous or formal open reduction techniques using bone hooks, collinear reduction clamps, or elevators prior to reaming.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Approach and Initial Exposure
For both sliding hip screws and cephalomedullary nails, the standard approach is a lateral incision over the proximal femur. The length and exact starting point vary based on the chosen implant. For a cephalomedullary nail, a 3 to 5-centimeter longitudinal incision is made proximal to the tip of the greater trochanter. The fascia lata is incised in line with the skin incision. The abductor musculature (gluteus medius) is then split bluntly in line with its fibers to access the tip of the trochanter. Great care is taken not to dissect too far posteriorly to protect the vascular supply to the femoral head.

If a sliding hip screw is selected, a more distal 8 to 10-centimeter incision is utilized over the lateral aspect of the greater trochanter extending distally along the femoral shaft. After incising the fascia lata, the vastus lateralis is encountered. The surgeon can either split the vastus lateralis in line with its fibers or elevate it off the lateral intermuscular septum, reflecting it anteriorly. Elevating the muscle belly generally provides better exposure of the lateral cortex and is preferred for applying the side plate of a sliding hip screw.

During the exposure of the lateral femur, meticulous hemostasis is mandatory. As the vastus lateralis is elevated, perforating branches from the profunda femoris artery will be encountered. These must be systematically identified, clamped, and electrocoagulated or ligated. Failure to secure these perforators will result in persistent intra
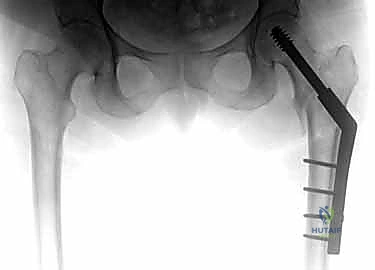
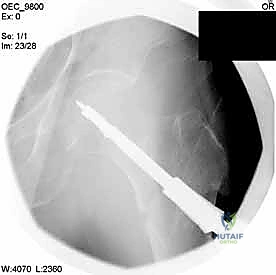
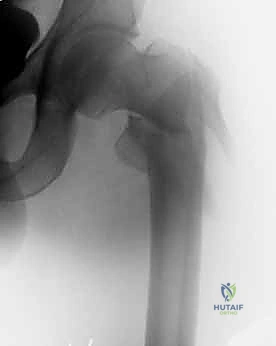
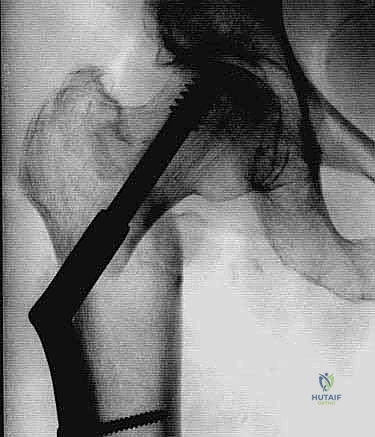
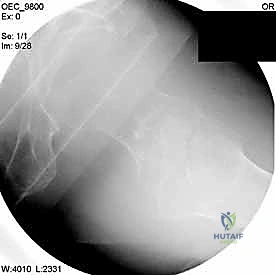
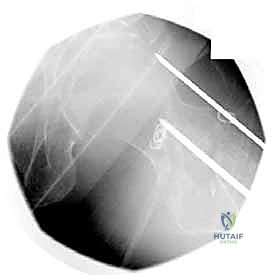
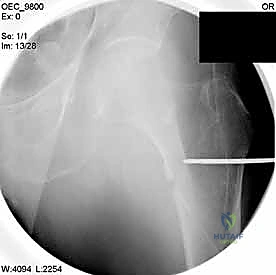
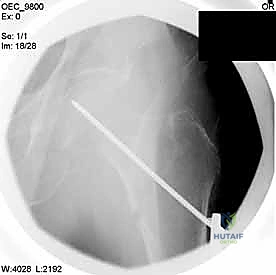
Clinical & Radiographic Imaging Archive