Chronic Achilles Tendon Reconstruction: V-Y Advancement with FHL Transfer Masterclass

Key Takeaway
Join us in the OR for an immersive masterclass on chronic Achilles tendon rupture repair. This guide details V-Y advancement and FHL transfer techniques, covering comprehensive anatomy, precise intraoperative steps, neurovascular precautions, and essential pearls for successful outcomes. Learn to manage critical steps from incision to hardware application, ensuring robust reconstruction and optimal patient recovery.
Comprehensive Introduction and Patho-Epidemiology
The management of a chronic Achilles tendon rupture represents one of the most formidable challenges in orthopedic foot and ankle surgery. Distinct from acute ruptures, a chronic tear—universally defined in the literature as a rupture presenting more than four to eight weeks post-injury—initiates a complex cascade of biomechanical and histological deterioration. The proximal gastroc-soleus complex undergoes rapid retraction, followed by progressive muscle atrophy and fibrofatty infiltration. Simultaneously, the rupture void fills with an unorganized, mechanically inferior fibrous scar tissue, often termed a "pseudotendon." This pseudotendon lacks the highly organized Type I collagen architecture necessary to transmit the immense forces generated during the terminal stance phase of the gait cycle.
Epidemiologically, chronic Achilles ruptures account for up to 20% to 25% of all Achilles tendon injuries, a staggering statistic that underscores the frequency of missed initial diagnoses. These injuries are frequently mischaracterized in primary care or emergency settings as severe ankle sprains, deep vein thromboses, or simple calf strains. The typical patient demographic mirrors that of acute ruptures—predominantly males in their fourth to sixth decades of life, often engaging in episodic, high-intensity athletic activities ("weekend warriors"). However, chronic presentations are also highly correlated with systemic risk factors that impair tendon vascularity and healing, including long-term fluoroquinolone use, systemic or local corticosteroid administration, diabetes mellitus, and inflammatory arthropathies.
Clinically, the patient with a chronic Achilles rupture presents with a profound, debilitating loss of the "check rein" mechanism of the ankle. The gastroc-soleus-Achilles (GSA) complex is the primary plantarflexor of the foot, responsible for generating the explosive push-off power required for normal ambulation. When this continuity is disrupted chronically, patients exhibit a characteristic calcaneal gait, characterized by a prolonged heel strike, absent toe-off, and a noticeable forward lurch. They will universally complain of an inability to walk up inclines, ascend stairs normally, or perform a single-leg heel raise. While some weak, active plantarflexion may remain due to the compensatory hypertrophy of the secondary plantarflexors (flexor hallucis longus, flexor digitorum longus, posterior tibialis, and peroneals), this is vastly insufficient for normal biomechanical function.
The surgical rationale for addressing these chronic defects mandates more than simple end-to-end apposition, which is typically impossible due to fixed tissue retraction. For defects measuring between 3 and 7 centimeters, the gold standard reconstruction involves a synergistic approach: a V-Y tendinous advancement of the proximal aponeurosis to bridge the gap, augmented by a flexor hallucis longus (FHL) tendon transfer. The V-Y advancement restores the resting length and tension of the GSA complex, while the FHL transfer provides robust vascularity to the relatively avascular watershed zone, acts as an internal splint, and contributes an "in-phase" active contractile force to augment compromised plantarflexion power.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the regional anatomy is the cornerstone of successful chronic Achilles reconstruction. The gastroc-soleus-Achilles (GSA) complex is a massive, bipennate musculotendinous structure. The gastrocnemius, originating from the posterior aspects of the medial and lateral femoral condyles, crosses three distinct articulations: the knee, the tibiotalar (ankle), and the subtalar joints. The soleus, originating from the posterior tibia and fibula, joins the gastrocnemius aponeurosis to form the Achilles tendon proper. This tendon rotates exactly 90 degrees externally as it descends, causing the gastrocnemius fibers to insert laterally and the soleus fibers to insert medially on the posterior calcaneal tuberosity. This spiraling architecture maximizes the tendon's elastic recoil and force transmission capabilities.
The vascular supply to the Achilles tendon is notoriously precarious, dictating both its propensity for rupture and its recalcitrance to healing. The tendon receives its blood supply from three main sources: the musculotendinous junction proximally, the osseous insertion distally, and the surrounding paratenon circumferentially. The paratenon is a highly vascularized, multi-layered sleeve of loose connective tissue that not only supplies intrinsic epitenon vessels but also facilitates up to 1.5 cm of frictionless tendon excursion during terminal dorsiflexion. However, a critical "watershed area" exists approximately 2 to 6 centimeters proximal to the calcaneal insertion. In this zone, the proximal and distal vascular networks anastomose poorly, rendering the tissue relatively ischemic and highly susceptible to degenerative tendinosis and subsequent rupture.

The neurovascular topography of the posterior leg demands meticulous attention during surgical dissection. The sural nerve, a purely sensory branch formed by the confluence of the medial sural cutaneous nerve (from the tibial nerve) and the lateral sural cutaneous nerve (from the common peroneal nerve), courses superficially in the posterior calf. It transitions from the posterolateral midline proximally to run intimately alongside the lateral border of the Achilles tendon distally, typically lying just 5 to 7 millimeters lateral to the tendon's insertion. Injury to the sural nerve is the most common major complication of Achilles surgery, leading to debilitating neuromas or profound lateral foot dysesthesia. Furthermore, the medial neurovascular bundle—comprising the tibial nerve and posterior tibial artery—resides deep to the transverse intermuscular septum, lying immediately medial to the FHL muscle belly.
The flexor hallucis longus (FHL) is uniquely suited for Achilles augmentation. Anatomically, its muscle belly is the most distal and posterior of the deep posterior compartment muscles, extending inferiorly almost to the level of the tibiotalar joint. This low-lying muscle belly provides highly vascularized tissue directly to the site of the Achilles repair. Biomechanically, the FHL is the second strongest plantarflexor of the ankle, possessing an axis of contractility that closely parallels that of the Achilles tendon. Crucially, the FHL is an "in-phase" muscle, meaning it naturally fires synchronously with the gastroc-soleus complex during the push-off phase of the gait cycle, allowing for seamless neuromuscular integration post-transfer without the need for complex cortical retraining.
Exhaustive Indications and Contraindications
The decision to proceed with a V-Y advancement combined with an FHL transfer is dictated primarily by the size of the intraoperative tendon defect after thorough debridement of all non-viable pseudotendon. Accurate preoperative and intraoperative measurement is paramount. The V-Y advancement is mathematically and biomechanically limited in the amount of length it can generate without compromising the proximal muscle-tendon architecture. Therefore, this specific combined technique is strictly indicated for chronic, neglected ruptures exhibiting a true gap of 3 to 7 centimeters. Defects smaller than 3 centimeters can often be managed with a V-Y advancement alone or an end-to-end repair with aggressive mobilization. Conversely, massive defects exceeding 7 centimeters typically require free tissue transfer, Achilles allografts, or synthetic mesh reconstructions, as a V-Y advancement would require an unacceptably long proximal incision and risk devascularizing the aponeurosis.
Patient selection is equally as critical as gap measurement. The ideal candidate is a physiologically active individual who complains of significant functional impairment, gait instability, and weakness that has failed to improve with conservative measures (such as custom ankle-foot orthoses). The patient must possess the cognitive and psychological fortitude to adhere to a rigorous, prolonged, and highly restrictive postoperative rehabilitation protocol. The surgeon must carefully evaluate the patient's baseline functional demands; an elite athlete may require a different reconstructive algorithm or expectation management compared to a sedentary, elderly patient who simply desires a brace-free, plantigrade foot for household ambulation.
Contraindications to this extensive reconstructive procedure must be strictly respected to avoid catastrophic limb-threatening complications. Absolute contraindications include the presence of active local or systemic infection, severe peripheral arterial disease with compromised distal perfusion (ABI < 0.5), and profound peripheral neuropathy (such as advanced Charcot neuroarthropathy). Relative contraindications encompass heavy tobacco use, poorly controlled diabetes mellitus (HbA1c > 8.0%), chronic immunosuppression, and significant soft tissue compromise or previous radiation therapy to the posterior ankle. In these high-risk populations, the risk of profound wound dehiscence and deep infection often outweighs the functional benefits of reconstruction, making chronic bracing the preferred management strategy.
| Factor | Indications for V-Y + FHL Transfer | Contraindications (Absolute & Relative) |
|---|---|---|
| Defect Size | 3.0 cm to 7.0 cm true gap (post-debridement) | < 3.0 cm (V-Y alone) or > 7.0 cm (Allograft required) |
| Chronicity | > 4 to 8 weeks post-injury (Chronic) | Acute injuries (< 3 weeks) without retraction |
| Patient Profile | Active, compliant, symptomatic weakness | Non-ambulatory, severe medical non-compliance |
| Vascular Status | Intact pedal pulses, ABI > 0.9 | Severe Peripheral Arterial Disease (ABI < 0.5) |
| Soft Tissue | Pliable, intact posterior skin envelope | Active infection, severe compromised skin, prior radiation |
| Neurologic | Intact sensation and motor control | Advanced Charcot arthropathy, severe neuropathy |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning begins with a comprehensive clinical examination designed to elucidate the extent of the pathology and the patient's baseline compensatory mechanics. The hallmark of a chronic rupture is a palpable, often visually obvious, defect in the posterior contour of the ankle.
The Thompson squeeze test will typically be weakly positive or equivocal; while squeezing the calf may elicit slight plantarflexion due to the intact FHL and deep compartment muscles, it will lack the crisp, robust excursion seen on the contralateral normal side. The most sensitive clinical indicator is the Matles test, evaluating the resting tension of the ankle. With the patient prone and knees flexed to 90 degrees, the affected ankle will fall into a neutral or dorsiflexed position, starkly contrasting with the 20 to 30 degrees of resting plantarflexion maintained by the intact GSA complex on the normal side.
Advanced imaging is an indispensable component of the preoperative workup for chronic ruptures. While weight-bearing radiographs are obtained to rule out calcaneal avulsion fractures or Haglund's deformity, Magnetic Resonance Imaging (MRI) is the gold standard. A non-contrast MRI in sagittal, axial, and coronal planes allows the surgeon to precisely quantify the gap between the retracted tendon ends, assess the volume and quality of the intervening scar tissue, and evaluate the degree of fatty infiltration and muscle atrophy within the gastrocnemius and soleus bellies (utilizing the Goutallier classification). This imaging directly dictates the surgical algorithm; if the MRI demonstrates a 5 cm gap, the surgical team can definitively plan for the V-Y advancement and FHL transfer, ensuring all necessary specialized equipment (e.g., bio-tenodesis screws, specialized tendon passers) is available in the operating theater.
On the day of surgery, anesthesia and patient positioning must be executed flawlessly. The procedure is typically performed under general endotracheal anesthesia to ensure absolute muscle relaxation, which is critical during the tensioning phase of the tendon transfer. A well-padded thigh tourniquet is applied; it is an absolute surgical axiom that a calf tourniquet must never be used for Achilles reconstruction, as it physically compresses the gastroc-soleus complex, preventing the proximal mobilization required for the V-Y advancement. The patient is then meticulously transitioned to the prone position onto a specialized padded frame. Chest rolls are placed longitudinally to facilitate unrestricted diaphragmatic excursion and prevent increased intra-abdominal pressure, which could lead to epidural venous engorgement and increased intraoperative bleeding.
Crucially, both lower extremities must be prepped and draped into the sterile field, extending from the mid-thigh down to the tips of the toes. This bilateral exposure is not merely a preference; it is a technical necessity. It allows the surgeon to dynamically compare the resting equinus and tension of the reconstructed ankle against the contralateral, normal limb throughout the procedure. Achieving symmetrical resting tension is the single most important intraoperative variable in restoring normal gait kinematics and preventing postoperative overlengthening or excessive stiffness.
Step-by-Step Surgical Approach and Fixation Technique
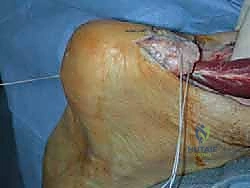
The surgical execution demands a meticulous, layered approach, prioritizing soft tissue handling and anatomic restoration. After exsanguination and tourniquet inflation to approximately 300-350 mmHg, a long, extensile posteromedial incision is mapped out.


The incision begins distally, 1 to 2 centimeters medial to the palpable Achilles tendon, extending from the calcaneal insertion and curving gently toward the posterior midline as it ascends the calf. This medial bias is a critical strategic decision; it deliberately avoids the sural nerve (which lies laterally) and prevents the final surgical scar from rubbing against the posterior counter of the patient's shoe. The incision is carried sharply through the skin and subcutaneous fat as a single, full-thickness fasciocutaneous flap to preserve the fragile subdermal vascular plexus.
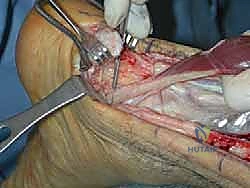
Deep dissection begins with the immediate identification and protection of the sural nerve and the lesser saphenous vein. Using blunt Metzenbaum dissection, these structures are isolated, encircled with a vessel loop, and gently retracted laterally out of the operative field. The paratenon, heavily thickened in chronic cases, is then identified and incised longitudinally. It is meticulously reflected off the underlying pseudotendon and preserved for subsequent closure. The zone of injury is now fully exposed. The surgeon systematically excises the disorganized, fibrotic pseudotendon using a scalpel and rongeurs until healthy, parallel collagen bundles with punctate bleeding are identified at both the proximal and distal tendon stumps.

With the knee flexed to 30 degrees and the ankle held in 20 degrees of plantarflexion (matching the contralateral side), the true defect is measured. For our masterclass scenario, assuming a 5 cm gap, we proceed to the V-Y advancement.


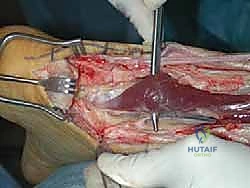
The V-Y advancement is executed at the proximal myotendinous junction. An inverted "V" is marked exclusively on the tendinous aponeurosis. The apex of the V is positioned centrally, just distal to the muscle belly. The limbs of the V are designed to be at least twice the length of the measured gap (e.g., 10 cm limbs for a 5 cm gap) and diverge to exit at the medial and lateral margins of the tendon.


Using a #15 blade, the aponeurosis is incised full-thickness, strictly avoiding any injury to the underlying red muscle fibers. This preservation of the muscle belly is paramount, as it maintains the vascular supply to the advancing tendinous flap. Gentle distal traction on the proximal Achilles stump allows the V to slide distally, converting the defect into a "Y" configuration and bridging the rupture gap.
Attention is then directed to the FHL harvest. The deep fascia over the deep posterior compartment is incised just medial to the Achilles tendon. The FHL muscle belly is easily identified by its low-lying nature.

The medial neurovascular bundle is identified and protected medially. The FHL tendon is traced as far distally as possible into the fibro-osseous tunnel beneath the sustentaculum tali. While maintaining the ankle and great toe in maximum plantarflexion to gain length, the tendon is transected just proximal to the master knot of Henry. The harvested FHL tendon is then brought into the primary operative field and prepared with a running locking whipstitch using a high-tensile strength #2 non-absorbable suture.

To anchor the FHL, a bone tunnel is drilled into the posterior calcaneal tuberosity, typically 1 to 2 centimeters anterior to the Achilles insertion, directed from dorsal-superior to plantar-inferior.


The FHL tendon is passed into this tunnel. The ankle is positioned in 15 to 20 degrees of plantarflexion (again, verifying symmetry with the prepped contralateral leg).

Maximum physiological tension is applied to the FHL tendon, and it is secured within the calcaneus using an appropriately sized bio-tenodesis interference screw.




