Open Reduction and Internal Fixation of the Pubic Symphysis: An Intraoperative Masterclass
Key Takeaway
This masterclass details open reduction and internal fixation of the pubic symphysis, crucial for pelvic ring stabilization. We cover comprehensive anatomy, meticulous preoperative planning, and step-by-step intraoperative execution. Fellows will learn precise dissection, hardware application, and critical pearls to manage complex pelvic trauma, ensuring optimal patient outcomes and avoiding common pitfalls.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we are executing a highly critical and biomechanically demanding procedure: the open reduction and internal fixation (ORIF) of the pubic symphysis. This intervention transcends the mere mechanical reapproximation of osseous structures; it represents the definitive restoration of the anterior tension band of the pelvic ring. The pelvic ring is a true osteoligamentous vault, a structure that is absolutely vital for bipedal ambulation, the transmission of axial loads from the spine to the lower extremities, and the protection of the delicate genitourinary, gastrointestinal, and neurovascular viscera. Pay meticulous attention to the ensuing discourse, as the surgical nuances and anatomical mastery required here will unequivocally dictate your patient’s long-term functional outcome and survivability.
High-energy pelvic ring disruptions represent some of the most devastating injuries encountered in orthopedic traumatology, carrying a historically high mortality rate primarily driven by acute hemorrhagic shock and associated multisystem trauma. The epidemiology of these injuries demonstrates a classic bimodal distribution: high-energy mechanisms such as motor vehicle collisions, motorcycle crashes, and falls from significant heights predominantly affect the younger, physiologically robust population, whereas low-energy falls represent an increasing burden in the geriatric, osteoporotic demographic. In the context of symphyseal diastasis, we are primarily addressing the former—high-energy, anterior-posterior compression (APC) vectors that violently disrupt the anterior pelvic structures before propagating posteriorly.
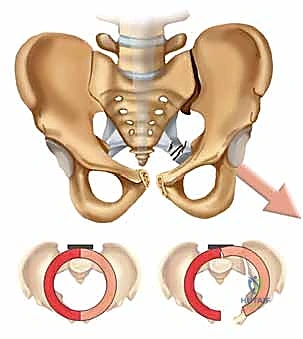
The pathogenesis of symphyseal disruption is intrinsically linked to the failure of the pelvic ring under immense external forces. A diastasis of the pubic symphysis unequivocally indicates a gross disruption of the pelvic ring and, by definition, denotes a mechanically unstable pelvis if the displacement exceeds physiological parameters. When the anterior tension band fails, the pelvis behaves analogously to an "open book," a term coined to describe the external rotation of the hemipelvis. This external rotation exponentially increases the intrapelvic volume, stripping the highly vascularized presacral venous plexus and potentially tearing major arterial branches, thereby precipitating catastrophic retroperitoneal hemorrhage.
Understanding the patho-epidemiology also requires an appreciation for the concomitant injuries that frequently accompany symphyseal diastasis. Urological injuries, particularly to the posterior urethra and extraperitoneal bladder, are highly correlated with anterior ring disruptions. Furthermore, the immense energy required to disrupt the symphysis often results in associated closed head injuries, blunt thoracic trauma, and intra-abdominal visceral damage. Therefore, the orthopedic surgeon must operate not in isolation, but as a crucial component of a multidisciplinary trauma team, balancing the urgent need for mechanical pelvic stability with the patient's overall physiological envelope.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, a profound, three-dimensional understanding of the anterior pelvic anatomy and its biomechanical behavior is non-negotiable. The pubic symphysis is an amphiarthrodial joint, characterized by a central fibrocartilaginous disc interposed between the hyaline cartilage-covered articular surfaces of the two pubic bodies. This joint is not designed for significant excursion; rather, it functions to absorb and dissipate shear and tensile forces during the gait cycle. Its stability is not inherent to its bony architecture but is entirely dependent on a robust ligamentous envelope. The primary soft tissue stabilizers are the superior and inferior arcuate ligaments. The inferior arcuate ligament, in particular, is a thick, dense fibrous band that sweeps across the inferior border of the pubic rami, acting as the primary restraint against superior translation and rotational shear.

Lateral to the symphyseal articulation, residing on the superior pubic rami, is the pubic tubercle. This prominent bony landmark is critical for two reasons: it serves as the tendinous insertion for the inguinal ligament and the rectus abdominis pillars, and it dictates the contouring of your symphyseal plates. Anatomical dimorphism must be recognized here. In female patients, the pelvis is inherently wider and more capacious to accommodate parturition. Consequently, the anterior pelvic ring presents a more pronounced concavity, and the pubic arch is significantly more rounded due to shallower pubic bodies compared to the male osteology. Failure to account for this dimorphism during hardware selection and plate contouring will inevitably lead to malreduction or prominent, symptomatic hardware.
The Posterior Stabilizers and Injury Mechanics
The anterior ring does not fail in isolation without profound implications for the posterior pelvic stabilizers. The sacrospinous and sacrotuberous ligaments are paramount to the rotational and vertical stability of the hemipelvis. The sacrospinous ligament, extending from the lateral sacrum and coccyx to the ischial spine, is the primary restraint against external rotational forces. The sacrotuberous ligament, coursing from the posterior iliac spines and sacrum down to the ischial tuberosity, resists both rotational shear and vertical translation. When an anterior-posterior force is applied, the symphysis typically fails first. If the force continues, the energy propagates posteriorly, sequentially tearing the sacrospinous and anterior sacroiliac ligaments.


The Young and Burgess classification system elegantly maps this mechanical progression. In Anterior-Posterior Compression (APC) injuries:
* APC Type I: Represents a stable injury (Tile type A). There is minor widening of the symphysis (typically <2.5 cm) without disruption of the posterior pelvic floor or the sacrospinous ligaments. These are generally managed non-operatively.
* APC Type II and III: These are mechanically unstable injuries. Classic cadaveric biomechanical studies have demonstrated that isolated sectioning of the symphysis rarely yields more than 2.5 cm of diastasis. Therefore, a diastasis exceeding 2.5 cm is the pathognomonic threshold indicating that the sacrospinous ligaments have failed. In an APC II injury, the anterior sacroiliac ligaments are torn, allowing the hemipelvis to externally rotate "down and out," hinging on the intact posterior sacroiliac ligaments. If the energy continues, the posterior sacroiliac ligaments fail (APC III), resulting in complete global instability (rotationally and vertically unstable).


Neurovascular Risks: The Corona Mortis
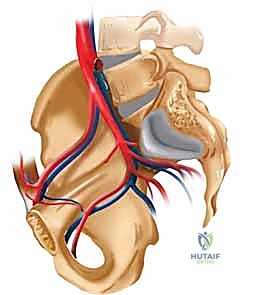
Intraoperatively, the most feared anatomical hazard during the anterior approach to the pelvis is the corona mortis (the "crown of death"). This is a highly variable but frequently present vascular anastomosis connecting the obturator circulation (branching from the internal iliac system) with the external iliac or inferior epigastric vessels. It is typically located approximately 4 to 6 centimeters lateral to the symphysis, coursing along the posterior aspect of the superior pubic ramus.
Iatrogenic laceration or avulsion of the corona mortis during subperiosteal dissection or retractor placement can result in torrential, life-threatening hemorrhage that is notoriously difficult to control due to the vessel's tendency to retract into the true pelvis. Meticulous, blunt dissection utilizing a "sponge stick" or careful periosteal elevation when working laterally along the superior rami is absolutely critical. If identified, it should be preemptively ligated or clipped.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a disrupted pubic symphysis hinges on restoring mechanical stability, minimizing pelvic volume to aid in hemostasis, and preventing long-term pain and gait dysfunction. The classical indication for ORIF is a symphyseal diastasis exceeding 2.5 centimeters. As previously detailed, this degree of displacement is the biomechanical proxy for disruption of the posterior ligamentous complex (specifically the sacrospinous ligaments), rendering the hemipelvis rotationally unstable. Leaving such an injury unreduced leads to chronic posterior pelvic pain, leg length discrepancy, and severe gait abnormalities.
Another critical indication involves specific lateral compression (LC) injury patterns. While LC injuries classically result in rami fractures, severe compressive forces can cause a "tilt fracture," where the contralateral pubic body fractures and tilts inferiorly, significantly disrupting the symphyseal articulation. If this displaced osseous fragment impinges upon the bladder, entraps the urethra, or significantly alters the dimensions of the pelvic ring (particularly relevant in females of childbearing age to prevent cephalopelvic disproportion during future parturition), anatomical reduction and rigid internal fixation are mandated.
Furthermore, we must address the unique pathology of post-partum symphyseal diastasis. During late-stage pregnancy, hormonally induced ligamentous laxity (mediated by relaxin) prepares the pelvis for childbirth. While mild widening is physiological, traumatic diastasis during parturition can result in severe displacements (up to 10-12 cm). The vast majority of these resolve spontaneously with conservative management and pelvic binding. However, if a patient exhibits persistent, debilitating pain and mechanical instability lasting 4 to 6 months postpartum, despite aggressive physical therapy, operative stabilization becomes a highly effective salvage procedure.
| Category | Specific Criteria | Rationale / Clinical Context |
|---|---|---|
| Absolute Indications | Symphyseal Diastasis > 2.5 cm | Indicates failure of the sacrospinous ligaments; rotationally unstable pelvis (APC II/III). |
| Open Pelvic Fractures (Anterior) | Requires immediate debridement; internal fixation may be used if tissue coverage is viable, otherwise external fixation. | |
| Concomitant Urologic Injury | Facilitates urological repair; prevents osseous impingement on the bladder/urethra. | |
| Impinging "Tilt" Fractures | Prevents visceral compromise and restores the birth canal dimensions in females. | |
| Relative Indications | Diastasis < 2.5 cm with Intractable Pain | May indicate occult instability; dynamic stress fluoroscopy can aid in decision-making. |
| Chronic Post-Partum Diastasis | Pain and instability persisting > 4-6 months despite maximum conservative therapy. | |
| Absolute Contraindications | Hemodynamic Instability (Extremis) | Patient cannot tolerate a prolonged procedure; requires damage control (binder/ex-fix/packing). |
| Active Local Infection / Gross Contamination | High risk of deep hardware infection; utilize external fixation instead. | |
| Severe Soft Tissue Compromise | Presence of an anterior Morel-Lavallee lesion or severe degloving precludes safe surgical incisions. | |
| Relative Contraindications | Severe Medical Comorbidities | Extreme surgical risk; non-operative management or minimally invasive external fixation preferred. |
Pre-Operative Planning, Templating, and Patient Positioning
Our journey to a successful, complication-free outcome begins long before the patient crosses the threshold of the operating room. Pre-operative planning in pelvic trauma is an exhaustive process that demands a systematic approach, beginning with adherence to Advanced Trauma Life Support (ATLS) protocols. These patients often present in profound hemorrhagic shock. Hemodynamic stabilization is the absolute first priority.
Initial Assessment and Resuscitation
If a patient requires massive transfusion protocols (e.g., >4 units of packed red blood cells) to maintain a permissive blood pressure, a mechanically unstable pelvis must be suspected as the source of retroperitoneal bleeding. Acute management dictates immediate reduction of the pelvic volume. This is best achieved in the trauma bay by internally rotating the lower extremities and placing a pelvic binder or a tightly wrapped sheet. It is a common and dangerous pitfall to place the binder over the iliac crests; it must be centered directly over the greater trochanters to effectively close the symphyseal book. Affix the sheet with heavy towel clips under tension—do not tie a knot, as knots slip and lose their compressive force.


Simultaneously, a thorough secondary survey is conducted. Examine the perineum, flanks, and lower back for ecchymosis. The presence of a fluctuant, boggy mass indicates a Morel-Lavallee lesion—a closed degloving injury where the subcutaneous tissue is sheared from the underlying fascia, creating a potential space filled with hematoma and necrotic fat. Operating through such compromised tissue invites catastrophic infection. Urological evaluation is equally critical. In males, a high-riding prostate, scrotal hematoma, or blood at the urethral meatus mandates a retrograde urethrogram prior to any attempt at Foley catheter insertion.
Advanced Imaging and Templating
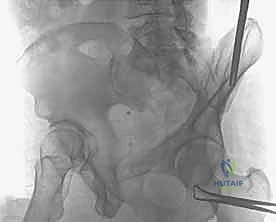
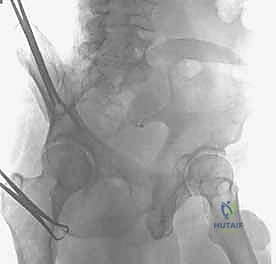
Radiographic evaluation begins with the standard AP pelvis, but this is insufficient for operative planning. We require orthogonal views: the Inlet view (x-ray beam directed 45 degrees caudad) perfectly visualizes the true pelvic brim, demonstrating anterior-posterior translation and internal/external rotation of the hemipelvis. The Outlet view (x-ray beam directed 45 degrees cephalad) elongates the pelvis, allowing for precise assessment of superior-inferior vertical translation and subtle rami fractures.


A fine-cut Computed Tomography (CT) scan with 2D multi-planar and 3D volume-rendered reconstructions is the gold standard. The CT scan allows for exact measurement of the diastasis, identification of intra-articular incarcerated fragments, and assessment of the posterior sacroiliac complex. During the templating phase, we anticipate the need for multi-hole, low-profile pelvic reconstruction plates. Typically, a 4-hole or 6-hole 3.5mm or 4.5mm plate is selected. In highly unstable patterns, orthogonal plating (one plate superiorly, one anteriorly) may be templated to enhance construct rigidity.
Patient Positioning and Setup
The patient is positioned absolutely supine on a fully radiolucent Jackson table or a flat trauma table. A small bump may be placed under the sacrum to slightly elevate the pelvis, facilitating access to the retropubic space. The lower extremities must be draped free to allow for intraoperative manipulation (internal rotation helps close the symphysis).
The abdomen and bilateral lower extremities are prepped and draped from the costal margins down to the distal thighs. This extensive prep allows for extension into a formal laparotomy if required by general surgery, and permits access to the iliac crests if percutaneous posterior fixation is concurrently planned. A Foley catheter must be in place and sterilely prepped into the field; it is a vital tactile landmark to identify the bladder neck and urethra during deep dissection.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the pubic symphysis is demanding, requiring respect for both the abdominal musculature and the delicate pelvic viscera. We predominantly utilize the Pfannenstiel approach, a transverse lower abdominal incision that provides excellent cosmesis and robust closure, though a lower midline laparotomy incision is utilized if general surgery is simultaneously addressing intra-abdominal trauma.
The Approach and Deep Dissection
The Pfannenstiel incision is made approximately two fingerbreadths (3-4 cm) superior to the palpable pubic symphysis, extending 10 to 12 centimeters transversely within the Langer lines. Dissection is carried sharply through the subcutaneous fat down to the glistening anterior rectus sheath. Hemostasis of the superficial epigastric vessels is achieved with electrocautery.


The anterior rectus sheath is incised transversely. We then elevate the fascial flaps superiorly and inferiorly off the underlying rectus abdominis muscle bellies. The linea alba is identified and split longitudinally. It is critical to preserve the tendinous insertions of the rectus abdominis on the pubic crests; do not completely detach them, as this will lead to severe postoperative core weakness and potential herniation. Instead, elevate them subperiosteally or split the fibers longitudinally to access the symphysis.
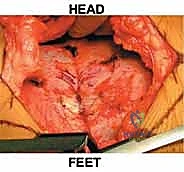

Retracting the rectus muscles laterally reveals the transversalis fascia. Bluntly sweeping this fascia posteriorly opens the Space of Retzius (the retropubic space). This space is heavily populated by the retropubic venous plexus. Expect immediate, dark venous bleeding upon entering this space. Do not attempt to chase these veins with cautery; rather, tightly pack the retropubic space with laparotomy sponges and wait several minutes. The tamponade effect is highly effective. The Foley catheter bulb is palpated to positively identify and protect the dome of the bladder, sweeping it posteriorly and cephalad with a malleable retractor.
Reduction Maneuvers
Once the pubic bodies and superior rami are exposed, the hematoma and torn remnants of the symphyseal disc are meticulously debrided to allow for a congruent bony reduction. Reduction of a widened symphysis can be technically frustrating. We employ several techniques.
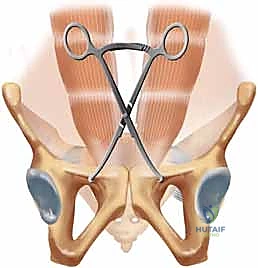
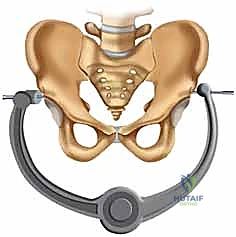
First, the patient's legs are internally rotated by an assistant to relax the external rotators and close the book. For direct mechanical reduction, a Jungbluth articulated reduction clamp is invaluable. We drill 2.5mm or 3.2mm osseous tunnels into the superior pubic rami, approximately 1-2 cm lateral to the symphysis on each side. The tines of the Jungbluth clamp are inserted into these holes. The clamp allows for powerful, controlled compression. If there is superior-inferior translation, the clamp can be applied asymmetrically (one hole more anterior/superior than the other) to dial in the vertical reduction as the clamp is closed.


Alternatively, large pointed Weber reduction forceps can be applied directly to the pubic tubercles. Care must be taken not to crush the bone or inadvertently capture the spermatic cord or round ligament, which exit the superficial inguinal ring just lateral to the pubic tubercles.
Internal Fixation
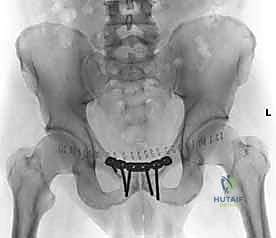
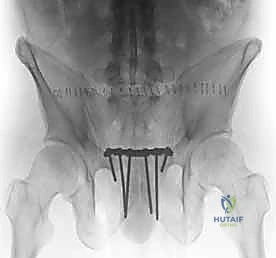
Once anatomical reduction is confirmed visually and via fluoroscopy (Inlet and Outlet views), definitive fixation is applied. The current gold standard is multi-hole plating. A pre-contoured symphyseal plate or a standard 3.5mm/4.5mm pelvic reconstruction plate is selected. The plate must be meticulously contoured to match the convexity of the superior pubic rami and sit flush against the bone to prevent prominent hardware.
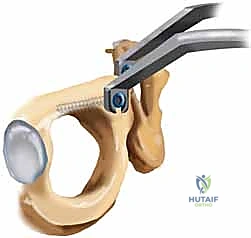

The plate is typically positioned superiorly. We aim for at least two, preferably three, fully threaded bi-cortical screws on each side of the symphysis
Clinical & Radiographic Imaging Archive