Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures

Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Comprehensive Introduction and Patho-Epidemiology
The distal ulna serves as the fundamental, immobile keystone of the forearm's kinematic chain. It is the fixed point around which the radius, and consequently the entire hand, articulates and functions during complex rotational movements. Despite its critical biomechanical role, fractures of the distal ulna have historically been underappreciated, inadequately characterized, and frequently undertreated, particularly when juxtaposed with the exhaustive attention given to its larger counterpart, the distal radius. This historical neglect has led to a legacy of chronic wrist pain, distal radioulnar joint (DRUJ) instability, and diminished grip strength in patients who received suboptimal management of their ulnar-sided pathology.

The pathogenesis of distal ulnar fractures is intimately tied to the mechanism of injury and the position of the forearm at the moment of impact. It is a well-established orthopedic axiom that ulnar-sided injuries are predominantly generated by falls backward. In this scenario, the forearm is typically forced into hyper-supination, effectively loading the ulnar column of the distal forearm and wrist. This specific vector of force transmission results in a predictable constellation of injuries, including distal ulnar fractures, triquetral chip fractures, and avulsions or complex tears of the triangular fibrocartilage complex (TFCC). Conversely, forward falls typically force the forearm into pronation, preferentially loading the radial column and resulting in scaphoid and distal radius fractures.
Isolated fractures of the ulnar diaphysis and metadiaphysis possess their own unique patho-epidemiology. These injuries most frequently occur as a result of direct, high-energy blunt trauma to the ulnar border of the forearm. This mechanism perfectly explains the classic eponym "nightstick fracture," as the patient reflexively raises their forearm in a defensive posture to shield the face or head from an incoming blow. While isolated, these fractures can still disrupt the delicate tension-band effect of the interosseous membrane and alter the load-sharing biomechanics of the DRUJ, necessitating careful evaluation of the entire forearm axis.
The current orthopedic literature has historically provided highly variable and often contradictory guidance regarding the management of these fractures and their associated soft-tissue injuries. However, modern surgical philosophy dictates that the outcome of distal forearm fractures is intrinsically linked to the anatomic restoration of the distal ulna. If the fixed point of the forearm is left malaligned or unstable, the surgical reconstruction of the radius is fundamentally compromised. Therefore, a paradigm shift is currently underway, advocating for the simultaneous, aggressive surgical management of the distal ulna whenever the distal radius is addressed operatively.
Detailed Surgical Anatomy and Biomechanics
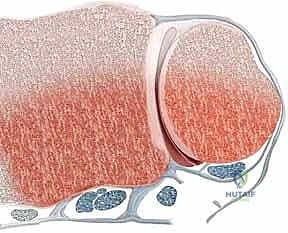
A profound understanding of the osseous and ligamentous anatomy of the distal ulna is paramount for executing successful surgical interventions. The ulnar head acts as the fixed, stable fulcrum upon which the radius and hand rest and rotate. During the arc of forearm pronation and supination, the radius translates and rotates around the ulnar head via the DRUJ. This articulation is not a simple hinge but a complex, multi-planar joint that relies on a delicate interplay between osseous congruity and ligamentous tethering to maintain stability throughout a nearly 180-degree arc of motion.


The osseous stability of the DRUJ is achieved through the articulation between the convex ulnar head and the concave sigmoid notch of the distal radius. Crucially, the spheres of these two articular surfaces differ significantly in their geometry. The curvature of the ulnar head possesses a shorter radius, whereas the curvature of the sigmoid notch has a greater radius. This geometric mismatch means that the joint is not perfectly congruent in all positions. In a neutral forearm position, approximately 60% of the joint surfaces are in contact. However, at the extreme limits of full pronation and full supination, bony contact drastically decreases to a mere 10%.
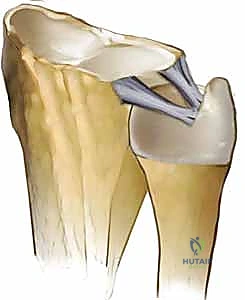
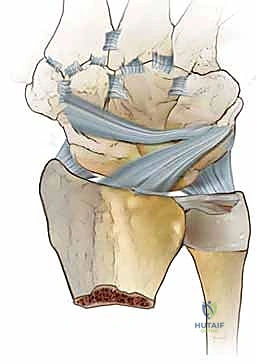
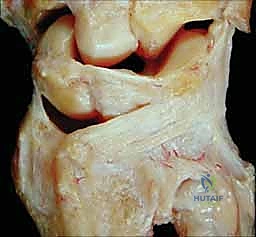
Because of this inherent osseous incongruity at the extremes of motion, the DRUJ is highly dependent on its soft-tissue envelope for stability. This joint is inextricably connected to the carpus and the radius by a highly sophisticated ligamentous apparatus known as the triangular fibrocartilage complex (TFCC). The primary stabilizers of the DRUJ are the dorsal and palmar radioulnar ligaments. These critical structures originate from the dorsal and palmar edges of the sigmoid notch on the distal radius and converge to insert firmly onto the distal ulna.
The exact insertion footprint of these ulnoradial ligaments is of paramount surgical importance. They possess both superficial and deep components that insert into the fovea (the depression at the base of the ulnar styloid) and partly attach to the base of the ulnar styloid itself. They function as dynamic reins, tightening and relaxing in an alternating fashion to control pronation and supination. Consequently, an osseous fracture at the base of the ulnar styloid frequently represents a bony avulsion of the primary DRUJ-stabilizing ligaments, leading to profound joint dissociation if left unaddressed.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for ulnar-sided injuries requires a nuanced synthesis of radiographic parameters, clinical stability assessments, and patient-specific functional demands. Not all ulnar styloid fractures require fixation; in fact, the precise anatomic location of the fracture line dictates the integrity of the TFCC and drives the surgical indication. Ulnar styloid fractures occurring at the extreme tip are generally benign. These represent isolated avulsion fractures of the ulnotriquetral collateral ligament. Because the critical ulnoradial ligaments remain securely attached to the fovea at the base of the styloid, the DRUJ remains stable, and these tip fractures demand no further surgical treatment.




Conversely, fractures occurring at the base of the ulnar styloid represent a severe threat to DRUJ kinematics. The general consensus dictates that basilar ulnar styloid fractures should be treated with open reduction and internal fixation (ORIF) if they are displaced by more than 2 millimeters. Furthermore, the vector of displacement is highly prognostic. Radial translation of the fractured ulnar styloid is a pathognomonic sign of complete detachment of the ulnoradial ligament from its foveal footprint. This radial translation represents a much stronger indication for surgical intervention than simple axial or distal displacement, which primarily detaches the less critical ulnotriquetral collateral ligament.
Ulnar head fractures, which are most frequently associated with complex distal radius fractures, present another absolute indication for surgery when displaced. The pattern and severity of the distal radius fracture heavily influence the functional outcome, but an incongruent ulnar head will inevitably lead to early post-traumatic arthrosis and blocked forearm rotation. Similarly, distal ulnar neck and metadiaphyseal shaft fractures—defined strictly as fractures occurring within 4 centimeters of the distal dome of the ulnar head—must be scrutinized. While some may spontaneously realign following the reduction of an associated radius fracture, those that remain displaced or result in DRUJ instability require rigid internal fixation.
Indications and Contraindications Summary Table
| Parameter | Indications for Surgical Intervention (ORIF) | Absolute or Relative Contraindications |
|---|---|---|
| Ulnar Styloid | Basilar fracture with > 2mm displacement; Radial translation of fragment; Clinical DRUJ instability post-radius fixation. | Tip avulsion fractures; Stable DRUJ on intra-operative stress testing; Asymptomatic chronic nonunions. |
| Ulnar Head | Intra-articular step-off > 1-2mm; Comminution causing mechanical block to rotation; DRUJ incongruency. | Undisplaced fractures; Severe, non-reconstructable comminution in low-demand elderly patients (consider salvage instead). |
| Metadiaphysis | Fractures within 4cm of the dome that are angulated, shortened, or irreducible; Failure of closed reduction. | Active local soft-tissue infection; Medically unstable patient; Acceptable alignment in a stable closed kinetic chain. |
| Soft Tissue | DRUJ dissociation without fracture (foveal avulsion); TFCC tears causing gross clinical laxity. | Asymptomatic degenerative TFCC tears; Fixed, chronic DRUJ subluxation requiring salvage rather than acute repair. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful distal ulnar reconstruction. Standard orthogonal imaging, including true posteroanterior (PA), lateral, and oblique radiographs, is mandatory. The true lateral radiograph is particularly critical for assessing the dorsal-palmar translation of the ulnar head relative to the radius. However, standard radiography often underestimates the complexity of ulnar-sided injuries. Radiographs occasionally reveal DRUJ dissociation in the complete absence of an ulnar-sided fracture, a phenomenon resulting from a purely ligamentous detachment of the ulnoradial ligament from the fovea.



Advanced imaging modalities are frequently required to delineate complex pathology. Computed Tomography (CT) with 2D and 3D reconstructions is invaluable for examining comminuted, intra-articular fractures of the ulnar head. It allows the surgeon to map the articular fragments, plan the trajectory of mini-fragment screws, and assess the exact geometry of the sigmoid notch. Magnetic Resonance Imaging (MRI) is occasionally indicated, particularly in subacute or chronic settings, to evaluate the structural integrity of the TFCC, the presence of marrow edema indicative of occult fractures, and the condition of the extensor carpi ulnaris (ECU) tendon subsheath.



Patient positioning and operating room setup must facilitate unhindered access to the entire forearm and utilize intra-operative fluoroscopy efficiently. The patient is placed supine with the operative extremity extended onto a radiolucent hand table. A well-padded proximal arm tourniquet is applied. The surgeon should be seated, with the fluoroscopy monitor positioned directly across the table to allow for real-time, ergonomic viewing. Intra-operative stress testing of the DRUJ—performed by translating the ulna dorsal and palmar relative to the radius in neutral, full pronation, and full supination—is a mandatory step after the fixation of any associated radius fracture to determine if the ulnar side requires immediate intervention.





Templating should involve a variety of implant options. Because the distal ulna features a rapidly tapering metaphysis and complex articular geometry, standard straight plates are often inadequate. The surgeon must have access to dedicated distal ulna locking plates, mini-fragment screw sets (1.5mm and 2.0mm), headless compression screws for articular fragments, and suture anchors for ligamentous reattachment. Anticipating the need for arthroscopic assistance is also prudent, as arthroscopy should be considered if radiographs lead the physician to suspect DRUJ dissociation without obvious radiographic explanations.
Step-by-Step Surgical Approach and Fixation Technique
The Universal Dorsal Approach to the Distal Ulna
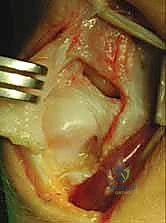
The surgical exposure of the distal ulna must be meticulously executed to preserve the delicate soft-tissue stabilizers while providing adequate visualization of the osseous anatomy. The distal ulna is approached through a dorsal longitudinal or slightly zigzag incision centered directly over the DRUJ and the ulnar head. Full-thickness fasciocutaneous flaps are elevated to protect the dorsal sensory branches of the ulnar nerve, which are highly variable and easily injured during this exposure.



Deep dissection involves elevating the ulnar retinacular flap. The interval is typically developed between the extensor retinaculum and the separate dorsal subsheath of the extensor carpi ulnaris (ECU). It is imperative to leave the ECU firmly within its subsheath whenever possible to prevent iatrogenic subluxation of the tendon post-operatively. The extensor digiti minimi (EDM) is identified and retracted radially. This approach provides a panoramic view of the distal ulna, allowing the surgeon to access an ulnar styloid fracture, address a metadiaphyseal shaft fracture, and simultaneously visualize, assess, and treat any associated TFCC pathology.
Fixation Strategies for Specific Fracture Patterns
For unstable ulnar styloid base fractures, reduction is achieved using fine pointed reduction forceps. Fixation can be accomplished utilizing a variety of techniques depending on fragment size. A tension-band construct utilizing a 0.045-inch Kirschner wire and a figure-of-eight stainless steel wire provides excellent biomechanical stability. Alternatively, a cannulated headless compression screw (typically 2.0mm or 2.4mm) can be placed antegrade from the tip of the styloid into the ulnar metaphysis, burying the head beneath the articular cartilage to prevent irritation.


Ulnar head fractures require anatomic reduction of the articular surface to restore the congruity of the DRUJ. Small, isolated articular shear fragments can be secured with countersunk mini-fragment screws or bioabsorbable pins. More complex, comminuted intra-articular fractures may require the use of a low-profile, contoured distal ulna locking plate. These plates are designed to wrap around the ulnar pole, allowing multiple locking screws to raft the articular surface while avoiding penetration into the DRUJ.
Management of the Metadiaphysis and Ligamentous Complex
Distal ulnar neck and shaft fractures (within 4 cm of the dome) are notoriously difficult to control with cast immobilization alone. Three-point fixation, even in a well-molded above-elbow cast, is generally ineffective due to the deforming forces of the pronator quadratus and the inherent instability of the cylindrical shaft. Therefore, these fractures require rigid stabilization. Standard 3.5mm limited-contact dynamic compression plates (LC-DCP) or pre-contoured locking plates are applied to the dorsal or ulnar border of the bone, ensuring at least three bicortical screws are placed proximal and distal to the fracture zone.




In scenarios where radiographs reveal DRUJ dissociation in the absence of a fracture, or when instability persists after osseous fixation, direct repair of the TFCC is mandated. Arthroscopically assisted repair or open reattachment of the ulnoradial ligament to the fovea is required to restore stability. Using suture anchors placed directly into the bleeding bone of the fovea, the deep fibers of the TFCC are tensioned and tied down, effectively recreating the critical tether that prevents dorsal-palmar translation of the radius relative to the ulna.


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following the management of distal ulnar fractures remain a significant clinical challenge. The natural history of inadequately treated distal ulnar fractures frequently leads to marginal long-term problems, but severe malunions and nonunions can be devastating to wrist function. Distal ulnar malunions frequently cause DRUJ incongruency, which manifests clinically as a mechanical block to forearm rotation, chronic pain, and accelerated post-traumatic arthrosis. This is precisely why the proactive management of these deceptive fractures is of paramount importance.



Ulnar styloid nonunions are a particularly common complication, though not all are symptomatic. The main physical findings of a symptomatic ulnar styloid nonunion include ulnar-sided wrist pain that exacerbates with loading in rotation, combined with focal point tenderness directly over the ulnar styloid. The symptomatology stems from several distinct pathophysiologic mechanisms: DRUJ instability from a malfunctioning ulnoradial ligament (peripheral TFCC detachment), abutment of the ununited fragment onto the triquetrum and ulnar carpus, impingement of the overlying ECU
Clinical & Radiographic Imaging Archive











