Mastering Adult Scoliosis: Intraoperative Techniques for Deformity Correction

Key Takeaway
This masterclass guides fellows through the complex surgical management of adult scoliosis. We cover detailed anatomy, meticulous preoperative planning, and step-by-step intraoperative execution of posterior spinal fusion and instrumentation. Learn to address coronal, sagittal, and axial deformities, manage neurovascular risks, and navigate potential pitfalls, ensuring optimal patient outcomes for degenerative and progressive scoliosis.
Comprehensive Introduction and Patho-Epidemiology
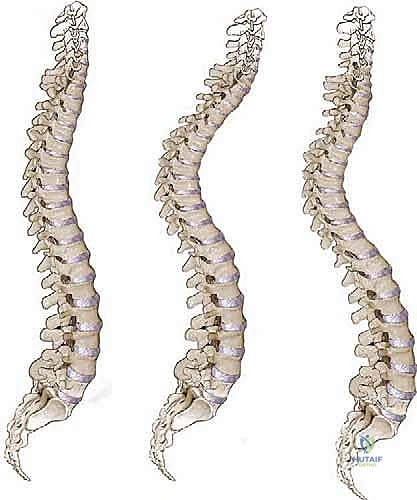
Welcome, colleagues and fellows, to the definitive discourse on one of the most formidable challenges in modern spine surgery: Adult Spinal Deformity (ASD), with a specific focus on Adult Scoliosis. This pathology represents a highly complex, multidimensional biomechanical failure of the axial skeleton that extends far beyond a simple coronal deviation. It is a profound disruption of the patient's center of gravity, leading to a cascade of compensatory mechanisms that ultimately fail, resulting in debilitating pain, neurological compromise, and a severe deterioration in health-related quality of life (HRQOL). The surgical management of ASD is not merely an exercise in skeletal realignment; it is a meticulously orchestrated reconstruction aimed at restoring global spinopelvic harmony, alleviating neural compression, and ensuring long-term biomechanical stability.
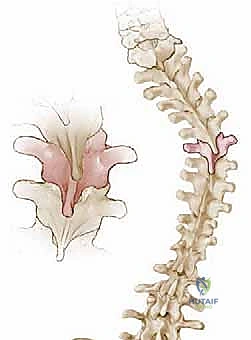
The pathophysiology of adult scoliosis is fundamentally heterogeneous, broadly categorized into two distinct etiologic pathways. The first is de novo degenerative scoliosis, which arises primarily in the lumbar spine due to asymmetric intervertebral disc degeneration and subsequent facet joint arthropathy. This asymmetric collapse initiates a vicious cycle of altered load distribution, leading to progressive coronal wedging, rotary subluxation, and, critically, a loss of lumbar lordosis. The second pathway involves the progression of pre-existing adolescent idiopathic scoliosis (AIS) into adulthood. While AIS is traditionally considered a stable entity after skeletal maturity, curves exceeding 30 to 50 degrees can progress at a rate of 1 to 2 degrees per year, exacerbated by superimposed degenerative changes.
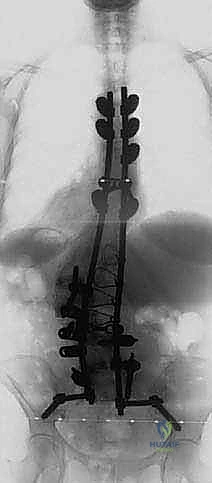
Clinically, we stratify these patients into distinct cohorts to guide our surgical rationale. Group 1 predominantly presents with symptoms of lumbar spinal stenosis—specifically, neurogenic claudication and radiculopathy—driven by the degenerative hypertrophy of the ligamentum flavum and facet joints within the concavity of the curve. These patients may have mild to moderate deformity, but their primary complaint is neural compression. Group 2 presents with progressive, globally decompensated deformity. These patients suffer from severe axial back pain due to paraspinal muscle fatigue as they constantly struggle to maintain an upright posture against a positive sagittal vertical axis (SVA). They often exhibit combined anterior, posterior, and lateral listhesis, necessitating extensive, multi-level reconstructive procedures that frequently extend into the thoracic spine and down to the pelvis.

The epidemiology of ASD highlights a growing public health challenge. As the global population ages, the prevalence of degenerative scoliosis is rising exponentially, with some studies indicating a radiographic prevalence of up to 68% in asymptomatic individuals over the age of 60. However, the symptomatic cohort demands significant healthcare resources. The socioeconomic impact is profound, as untreated ASD correlates with disability scores (such as the Oswestry Disability Index) that rival or exceed those of chronic conditions like congestive heart failure or severe pulmonary disease. Understanding this patho-epidemiological landscape is the prerequisite for any spine surgeon attempting to master the intricacies of deformity correction.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Anatomy
Navigating the osteology of the dysplastic and degenerated spine requires a profound three-dimensional spatial awareness. The posterior elements—spinous processes, laminae, transverse processes, and facet joints—are the primary landmarks and anchor points for our instrumentation. However, in the setting of adult scoliosis, normal anatomical relationships are grossly distorted. Pedicle morphology varies drastically; thoracic pedicles are naturally narrower and exhibit a more medial trajectory, while lumbar pedicles are larger but frequently distorted by severe rotational deformity. Furthermore, chronic asymmetric loading induces subchondral sclerosis and massive osteophyte formation, which can obliterate standard entry points and complicate pedicle screw cannulation.

The facet joints play a pivotal role in the pathogenesis and surgical management of ASD. In degenerative scoliosis, facet arthropathy leads to joint hypertrophy, capsular laxity, and eventual subluxation. This facet incompetence is the primary driver of rotary listhesis, a hallmark of the adult scoliotic curve that significantly narrows the neuroforamen on the concavity. Intraoperatively, extensive facetectomies (such as Ponte or Smith-Petersen osteotomies) are often mandatory not only to decompress the traversing and exiting nerve roots but also to mobilize the rigid segments, allowing for posterior column shortening and lordosis restoration.

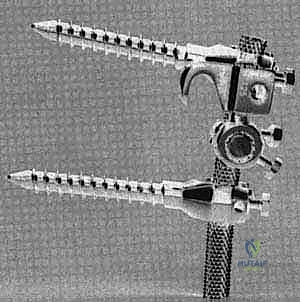
The biomechanics of the anterior column must be intimately understood, even when performing a strictly posterior approach. The intervertebral disc and vertebral bodies bear approximately 80% of the axial load in a healthy spine. In ASD, the loss of anterior column support due to advanced disc degeneration necessitates robust posterior instrumentation and, frequently, anterior or lateral interbody fusion (ALIF/LLIF) to share the load, restore disc height, and prevent hardware failure. Furthermore, the pelvic anatomy is critical for anchoring long constructs. The ilium and sacrum must be meticulously evaluated for bone density and morphology to accommodate S2-Alar-Iliac (S2AI) or traditional iliac screws, which are essential to prevent distal junctional failure in fusions crossing the cervicothoracic or thoracolumbar junctions down to the sacrum.

Muscular Intervals and Soft Tissue Envelopes
The posterior muscular envelope is not merely an obstacle to the spine; it is a vital dynamic stabilizer that must be respected and preserved. The standard posterior midline approach requires the subperiosteal dissection of the erector spinae muscle group (multifidus, longissimus, iliocostalis) off the spinous processes, laminae, and out to the tips of the transverse processes. This dissection must be meticulous, staying strictly within the subperiosteal plane to minimize disruption of the dorsal rami innervation and segmental vascular supply. Aggressive or careless retraction leads to ischemic necrosis and denervation of the multifidus, resulting in postoperative paraspinal muscle atrophy, intractable axial pain, and loss of dynamic sagittal support.
For surgeons utilizing lateral or anterior approaches (LLIF/ALIF) as part of a staged deformity correction, the anatomy of the psoas major and the lumbar plexus is of paramount importance. The lumbar plexus courses through the posterior third of the psoas muscle, with significant individual variation. Retraction of the psoas during lateral interbody placement carries a high risk of transient or permanent femoral nerve or genitofemoral nerve neurapraxia. Thorough knowledge of the safe working zones—typically the anterior third of the disc space—and the use of directional electromyography (EMG) are non-negotiable requirements for these approaches.

The ligamentous structures of the spine act as tension bands that must be strategically released to achieve correction. The ligamentum flavum, often hypertrophied in degenerative scoliosis, contributes significantly to central and lateral recess stenosis. Resection of the ligamentum flavum is a fundamental step in decompression. Conversely, the anterior longitudinal ligament (ALL) may act as a tether in severe kyphotic deformities. In cases requiring massive sagittal realignment, an anterior longitudinal ligament release (ALLR) via a lateral approach, or a posterior three-column osteotomy (such as a Pedicle Subtraction Osteotomy), is required to disrupt this tether and allow for adequate lordotic reconstruction.

Neurovascular Topography and At-Risk Structures
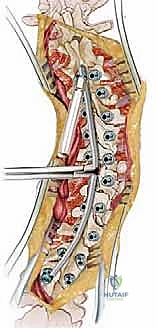
The catastrophic potential of neurovascular injury during ASD surgery cannot be overstated. The spinal cord, conus medullaris, and cauda equina are at constant risk during decompression, osteotomy execution, and deformity correction maneuvers. The spinal cord is particularly vulnerable to ischemic injury from over-distraction or direct mechanical trauma during thoracic pedicle screw placement. Continuous intraoperative neuromonitoring (IONM), encompassing somatosensory evoked potentials (SSEPs), motor evoked potentials (MEPs), and spontaneous electromyography (sEMG), is the standard of care. Any degradation in signals demands immediate cessation of the maneuver, elevation of mean arterial pressure (MAP), and critical reassessment of the hardware and neural elements.
The exiting and traversing nerve roots are highly susceptible to injury, particularly in the setting of severe foraminal stenosis and rotary subluxation. The dorsal root ganglion (DRG), located within the neural foramen, is exquisitely sensitive to stretch and compression. Aggressive correction of a coronal curve without adequate foraminal release can lead to iatrogenic compression of the nerve root on the concavity. Furthermore, the dura mater in elderly patients with chronic stenosis is often attenuated, friable, and densely adherent to the overlying ligamentum flavum or prior epidural scar tissue. Incidental durotomies are a known complication, and surgeons must be adept at primary dural repair and the use of dural sealants to prevent postoperative cerebrospinal fluid (CSF) fistulas.

Vascular anatomy presents another layer of profound risk. The segmental arteries and veins, branching from the aorta and inferior vena cava, course intimately over the vertebral bodies and near the base of the transverse processes. Uncontrolled hemorrhage from a lacerated segmental vessel during posterior exposure or osteotomy can rapidly become life-threatening. Anteriorly, the bifurcation of the aorta and IVC, typically around the L4-L5 level, dictates the approach for ALIF procedures. The left common iliac vein is particularly vulnerable during L4-L5 anterior exposures. Meticulous preoperative assessment of vascular anatomy using MRI or CT angiography is essential to mitigate these catastrophic risks.

Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in the adult scoliotic patient is among the most complex in orthopedic surgery. It requires a delicate balance between the patient's physiological age, symptom severity, curve progression, and the inherent, massive risks of major reconstructive surgery. The primary indication for surgery is the failure of exhaustive, well-documented conservative management. This includes a minimum of six months of structured physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs), neuropathic modulators (e.g., gabapentin), and targeted fluoroscopically guided epidural steroid or facet injections. When these modalities fail to provide durable relief, and the patient's HRQOL continues to decline, surgical intervention is warranted.
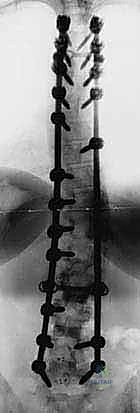
Specific indications dictate the magnitude of the surgical intervention. For patients in Group 1, whose primary pathology is neurogenic claudication secondary to focal stenosis within a relatively stable, non-progressive curve, a limited decompression with or without a short-segment fusion may suffice. However, for patients in Group 2, characterized by global sagittal imbalance (SVA > 5cm), severe pelvic incidence-lumbar lordosis (PI-LL) mismatch (>10 degrees), progressive coronal deformity (>30 degrees with documented progression), or intractable axial back pain secondary to muscular fatigue, a comprehensive, multi-level deformity correction is absolutely indicated. The goal here is not merely decompression, but the complete restoration of spinopelvic harmony to prevent adjacent segment disease and hardware failure.

Contraindications must be rigorously evaluated to prevent disastrous outcomes. Absolute contraindications include active systemic or surgical site infections, severe medical comorbidities precluding general anesthesia (e.g., recent myocardial infarction, severe restrictive lung disease), and profound, uncorrectable coagulopathies. Relative contraindications are numerous and require nuanced judgment. Severe osteoporosis (T-score < -2.5) significantly increases the risk of screw pullout, proximal junctional kyphosis (PJK), and pseudarthrosis. In such cases, preoperative optimization with anabolic agents (e.g., teriparatide, romosozumab) for 3 to 6 months is often mandatory. Furthermore, severe psychosocial instability, active smoking, and chronic high-dose opioid use are strong relative contraindications that correlate with poor postoperative outcomes and high complication rates.

| Category | Indications for Surgery | Contraindications (Absolute & Relative) |
|---|---|---|
| Neurological | Progressive motor deficit; Intractable radiculopathy; Cauda equina syndrome. | Severe, fixed neurological deficits unlikely to improve (Relative). |
| Biomechanical | Global sagittal imbalance (SVA > 5cm); PI-LL mismatch > 10°; Documented curve progression. | Severe, untreated osteoporosis (Relative); Inability to tolerate extensive rehab. |
| Clinical | Failure of >6 months conservative care; Intractable axial/leg pain; Severe decline in HRQOL. | Active infection (Absolute); Unstable cardiopulmonary disease (Absolute). |
| Psychosocial | Highly motivated patient; Good support system; Realistic expectations. | Active smoking (Relative); Chronic high-dose opioid dependency (Relative). |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical and Radiographic Assessment
The foundation of a successful deformity correction is laid weeks, if not months, before the patient enters the operating theater. The clinical assessment must be exhaustive. We begin with a detailed history, focusing on the character, radiation, and exacerbating factors of the pain. Is the pain primarily mechanical (worse with standing/walking, relieved by sitting) or neurogenic? A meticulous neurological examination is performed to identify subtle deficits, such as a mild foot drop or asymmetric reflex depression, which pinpoint specific levels of compression. Gait analysis is critical; patients with severe sagittal imbalance often exhibit a characteristic "crouch gait," utilizing hip and knee flexion to artificially retrovert the pelvis and maintain a horizontal gaze.

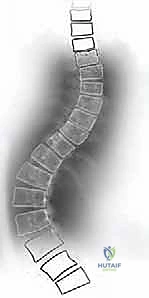
Radiographic templating is the cornerstone of our preoperative strategy. The absolute minimum requirement is high-quality, standing 36-inch posteroanterior (PA) and lateral radiographs. On the PA film, we meticulously measure the Cobb angles of the primary and compensatory curves, identifying the apical vertebra (most laterally deviated) and the stable vertebra (bisected by the center sacral vertical line). Coronal balance is assessed by dropping a plumb line from the C7 vertebral body; a deviation of more than 4 cm from the central sacral vertical line (CSVL) indicates significant coronal decompensation. We also evaluate for lateral listhesis, which frequently correlates with severe, localized foraminal stenosis on the concavity.

Sagittal plane analysis is arguably the most critical component of modern deformity planning. We measure the Sagittal Vertical Axis (SVA), the distance from the C7 plumb line to the posterior superior corner of S1. An SVA greater than 5 cm is highly correlated with poor clinical outcomes. We must calculate the spinopelvic parameters: Pelvic Incidence (PI), Pelvic Tilt (PT), and Sacral Slope (SS). The Schwab criteria dictate that our surgical goal must be to achieve a Lumbar Lordosis (LL) that is within 10 degrees of the patient's fixed Pelvic Incidence (PI-LL < 10°). Failure to restore this relationship virtually guarantees postoperative postural decompensation, hardware failure, and proximal junctional kyphosis. Advanced imaging, including MRI for evaluating neural elements and CT scanning for assessing bone stock, facet ankylosis, and planning osteotomy trajectories, completes the radiographic workup.

Operating Room Setup and Patient Positioning
The execution of a massive deformity correction requires a highly choreographed operating room environment. Patient positioning on the Jackson OSI table is a critical surgical step in itself, not merely a preparatory task. The patient is carefully log-rolled onto the prone frame. The chest and hip pads must be meticulously positioned to allow the abdomen to hang completely free. This decreases intra-abdominal pressure, thereby reducing epidural venous engorgement and minimizing intraoperative blood loss. All pressure points—particularly the ulnar nerves at the cubital tunnel, the peroneal nerves at the fibular head, and the face—must be heavily padded to prevent devastating positioning neuropathies or ischemic visual loss.
The surgical table is actively utilized to achieve intraoperative lordosis before the first incision is even made. By extending the hips and utilizing the table's articulation capabilities, we can passively close mobile disc spaces and facet joints, thereby reducing the amount of active, instrumented correction required later in the case. The cervical spine is maintained in a neutral position to prevent spinal cord traction. Once positioned, a lateral fluoroscopic image or an O-arm spin is obtained to verify the baseline alignment and ensure that the planned surgical levels are adequately visualized and accessible.

Neuromonitoring setup is a complex, multidisciplinary effort. The neurophysiologist places subdermal electrodes for SSEPs, MEPs, and sEMG. The anesthesia team must employ a Total Intravenous Anesthesia (TIVA) protocol, typically utilizing propofol and remifentanil infusions, while strictly avoiding volatile inhalation agents and long-acting paralytics, which profoundly suppress motor evoked potentials. Baseline signals are acquired prior to positioning and immediately after the final prone position is achieved. A clear communication protocol between the surgeon, anesthesiologist, and neurophysiologist is established to manage any intraoperative signal degradation swiftly and effectively.

Step-by-Step Surgical Approach and Fixation Technique
Exposure and Decompression
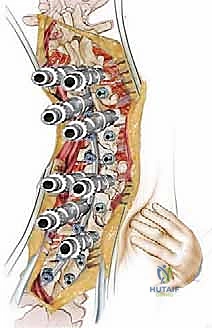
The surgical approach begins with a precise, midline longitudinal incision extending over the planned levels of instrumentation. The dissection must be meticulously maintained within the avascular subperiosteal plane to minimize blood loss and preserve the paraspinal musculature. Using Cobb elevators and electrocautery, the multifidus and longissimus muscles are swept laterally off the spinous processes, laminae, and facet joints, exposing the anatomy out to the tips of the transverse processes in the lumbar spine and the costotransverse joints in the thoracic spine. Hemostasis is rigorously maintained using bipolar electrocautery, bone wax, and hemostatic agents (e.g., Floseal, Surgiflo) packed into the bleeding epidural or cancellous bone spaces.

Once the posterior elements are cleanly exposed, attention turns to mobilization and decompression. In a rigid adult deformity, the posterior column is often foreshortened and ankylosed. Wide facetectomies (Ponte osteotomies) are performed at multiple levels. This involves complete resection of the inferior articular process of the cephalad vertebra and the superior articular process of the caudal vertebra, along with the intervening ligamentum flavum. This maneuver not only provides excellent visualization of the traversing and exiting nerve roots for decompression but also significantly increases the flexibility of the segment, allowing for 5 to 10 degrees of sagittal correction per level when compressed.

Neural decompression is tailored to the patient's specific preoperative symptomatology and advanced imaging. Central canal stenosis is addressed via wide laminectomies, while lateral recess and foraminal stenosis require meticulous undercutting of the pars interarticularis and complete foraminotomies. The exiting nerve root, particularly the L5 root beneath the sacral ala in severe lumbosacral curves, must be visually identified and completely freed from any bony or ligamentous compression. Throughout the decompression, the dura is protected with cottonoid patties. In the event of an incidental durotomy, it must be repaired primarily with 4-0 or 5-0 non-absorbable suture (e.g., Prolene or Nurolon) and reinforced with a dural sealant to prevent postoperative CSF leakage.