Orthopedic Board Review: Lipoma, Osteochondroma, AS, Synovial Chondromatosis MCQs | Part 15
Key Takeaway
This ABOS Orthopedic Board Review covers essential topics including atypical lipoma, osteochondroma, ankylosing spondylitis, and synovial chondromatosis. It provides multiple-choice questions and detailed rationales to help orthopedic specialists master musculoskeletal oncology, rheumatology, and joint pathology for board certification. Key areas include diagnosis, imaging, pathology, and management strategies.
Orthopedic Board Review: Lipoma, Osteochondroma, AS, Synovial Chondromatosis MCQs | Part 15
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
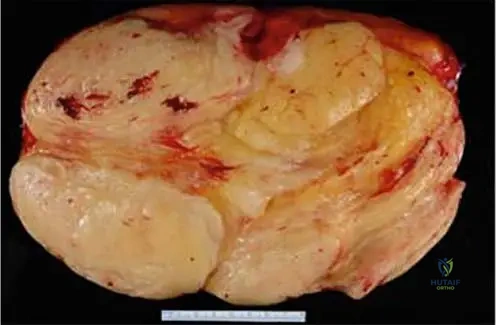
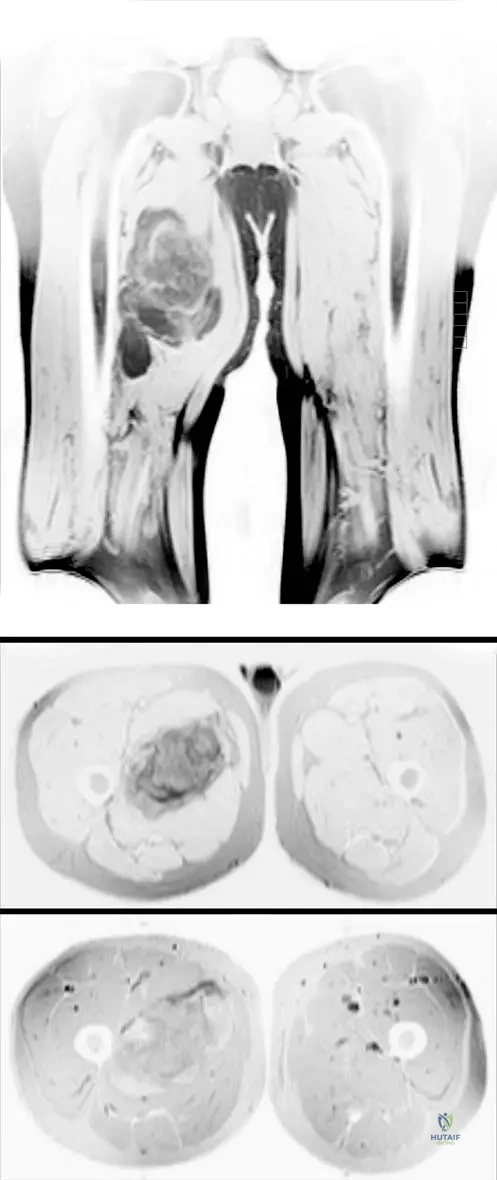
A 55-year-old male presents with a large, deep-seated painless mass in his thigh. MRI shows a predominantly lipomatous tumor with thickened septa. Histopathology shows mature adipocytes with focal nuclear atypia.
Which genetic alteration is most specific to confirm the diagnosis of an atypical lipomatous tumor?
Explanation
Question 2
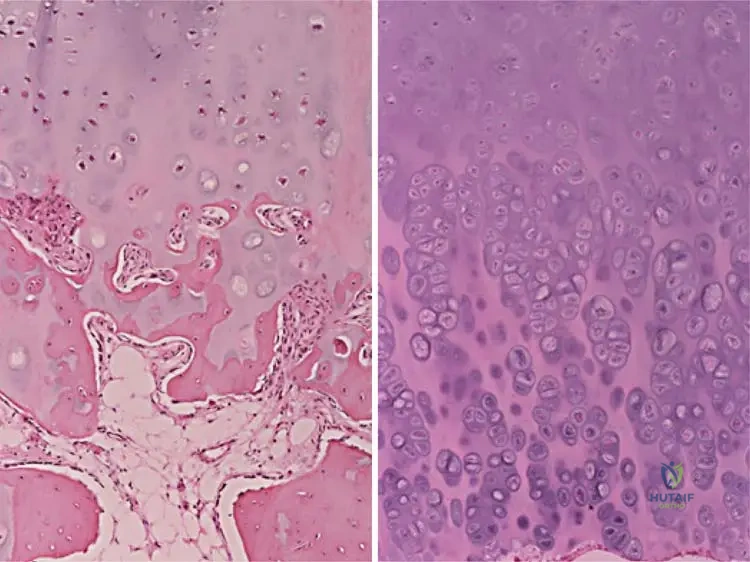
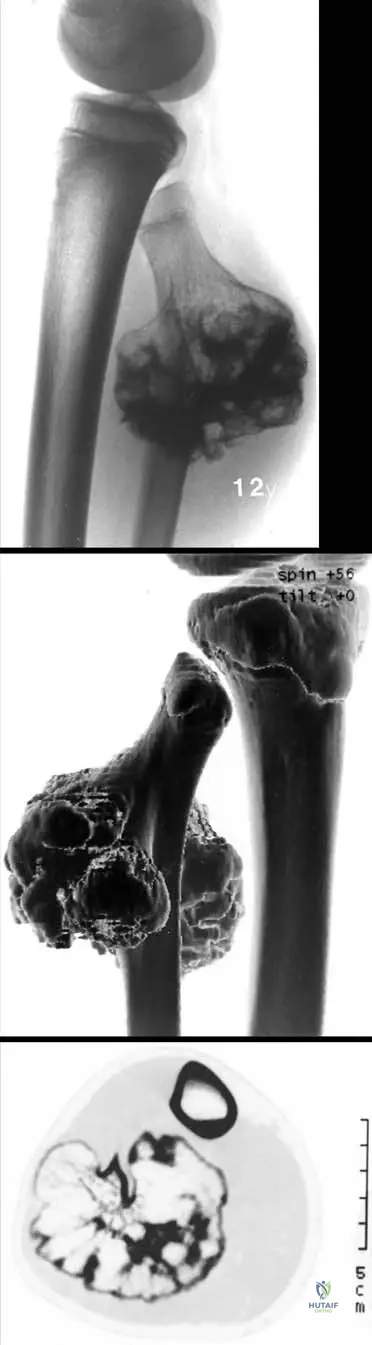
A 28-year-old male with Multiple Hereditary Exostoses presents with recent growth and pain in a distal femur lesion. MRI shows a cartilage cap thickness of 25 mm.
What is the most likely pathological finding in this growing lesion?
Explanation
Question 3
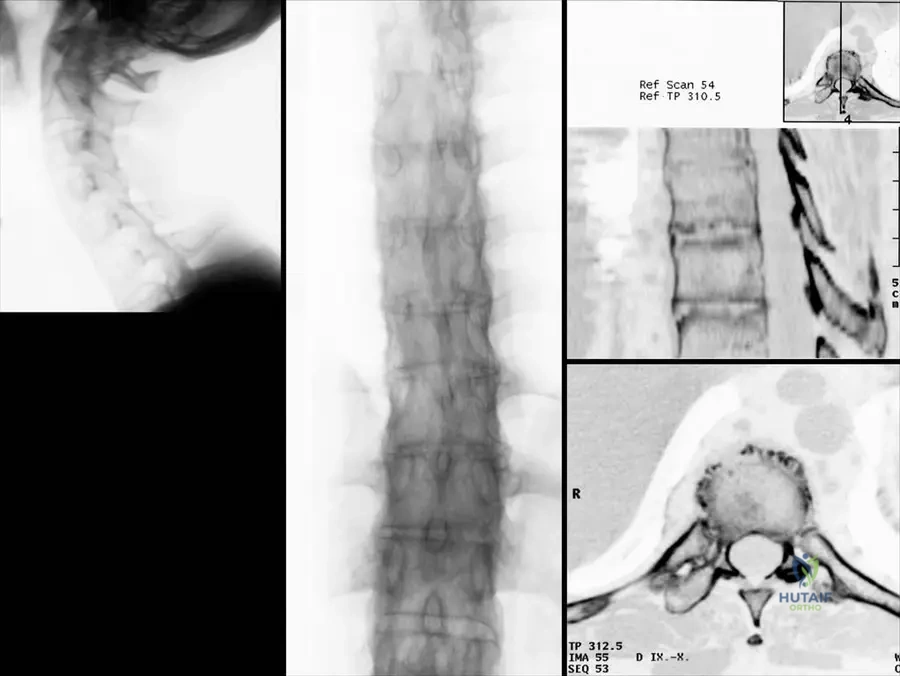
A 65-year-old male with long-standing ankylosing spondylitis presents to the ED after a minor fall. He complains of severe neck pain but has no neurological deficits. Radiographs demonstrate a fracture through the C6-C7 intervertebral disc space extending into the posterior elements.
What is the most appropriate management?

Explanation
Question 4
A 45-year-old male presents with chronic knee pain, catching, and restricted range of motion. Radiographs reveal multiple uniform, calcified intra-articular loose bodies.
Primary synovial chondromatosis is currently best described as:
Explanation
Question 5
Deep lipomas of the extremities are classified as intramuscular or intermuscular. Which of the following statements regarding intramuscular lipomas is true compared to their subcutaneous counterparts?
Explanation
Question 6
A 12-year-old boy with multiple bony bumps around his knees and wrists is diagnosed with Multiple Hereditary Exostoses (MHE).
The pathogenesis of this condition involves a mutation in EXT1 or EXT2 genes, which leads to a defect in the synthesis of what molecular component?
Explanation
Question 7
A 50-year-old patient with known ankylosing spondylitis presents with localized, worsening back pain. Radiographs reveal a destructive disco-vertebral lesion with reactive sclerosis.
What is the primary etiology of this specific lesion?
Explanation
Question 8
A 38-year-old female undergoes arthroscopic removal of numerous loose bodies from her shoulder joint. Pathology confirms primary synovial chondromatosis. Which of the following features most reliably differentiates primary from secondary synovial chondromatosis?
Explanation
Question 9
An atypical lipomatous tumor (well-differentiated liposarcoma) located in which of the following anatomic areas carries the highest risk for disease-specific mortality and dedifferentiation?
Explanation
Question 10
An 18-year-old presents with a painless mass at the proximal medial tibia.
Which of the following radiographic or MRI findings is the absolute sine qua non for diagnosing a true osteochondroma?
Explanation
Question 11
A 55-year-old male presents with a deep, painless, slow-growing mass in his thigh.
Biopsy reveals mature adipocytes with focal nuclear atypia. To differentiate an atypical lipomatous tumor from a benign lipoma, which molecular finding is most diagnostic?
Explanation
Question 12
A 25-year-old male with Multiple Hereditary Exostoses (MHE) reports rapid growth of a previously stable mass on his proximal tibia.
MRI is obtained. Which of the following MRI findings is the most concerning indicator of malignant transformation to secondary chondrosarcoma?
Explanation
Question 13
A 60-year-old male with a 20-year history of ankylosing spondylitis presents after a ground-level fall. He has severe neck pain. Radiographs reveal a displaced C6-C7 discovertebral fracture.
What is the most appropriate definitive management?
Explanation
Question 14
A 40-year-old male presents with chronic knee catching and swelling. Imaging shows multiple intra-articular calcific loose bodies.
Which histopathologic feature most reliably differentiates primary synovial chondromatosis from secondary osteochondromatosis?
Explanation
Question 15
Which of the following MRI sequences is most useful for confirming that a well-circumscribed soft tissue mass is a benign lipoma rather than a fluid-filled cyst?
Explanation
Question 16
Multiple hereditary exostoses (MHE) is an autosomal dominant condition linked to mutations in the EXT1 and EXT2 genes. What is the primary function of the proteins encoded by these genes?
Explanation
Question 17
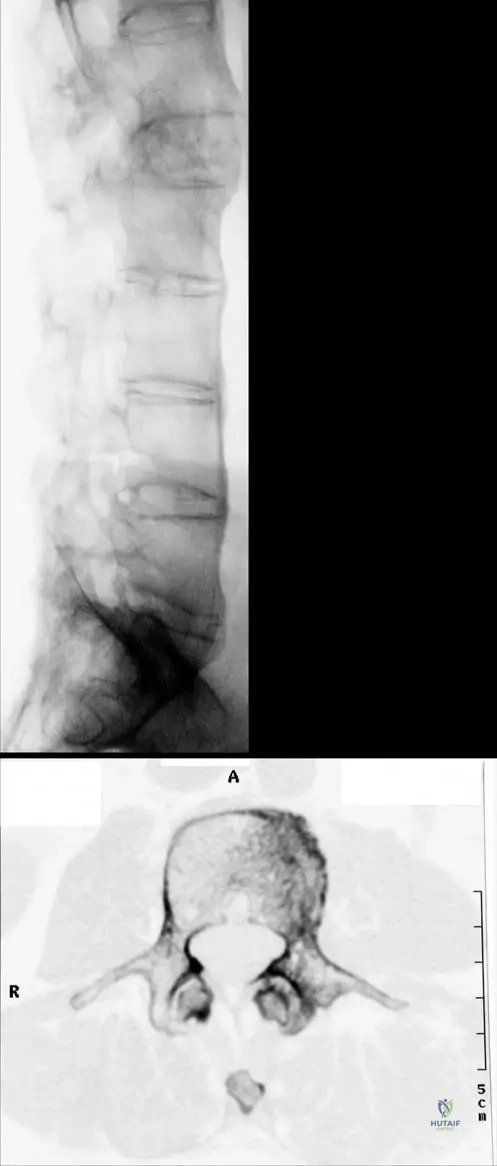
A 45-year-old male with advanced Ankylosing Spondylitis develops progressive lower back pain. Radiographs reveal a destructive, radiolucent lesion at the T12-L1 discovertebral junction with sclerotic margins.
What is the most likely diagnosis?
Explanation
Question 18
A 55-year-old female with a long history of primary synovial chondromatosis of the hip presents with new, rapidly worsening rest pain and progressive joint destruction on radiographs. What is the most likely complication?
Explanation
Question 19
An atypical lipomatous tumor (ALT) and a well-differentiated liposarcoma (WDLS) are histologically identical. The terminology differs based purely on anatomical location. In which location is the term "well-differentiated liposarcoma" utilized due to the high risk of unresectability and mortality from local recurrence?
Explanation
Question 20
Which of the following is a strict diagnostic requirement for the radiographic identification of a benign osteochondroma?
Explanation
Question 21
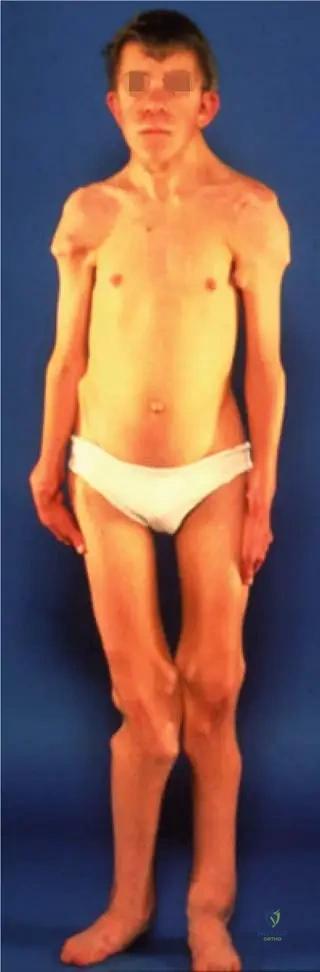
A 35-year-old male with Ankylosing Spondylitis presents for a total hip arthroplasty (THA) due to severe bilateral hip autofusion.
Compared to patients undergoing THA for primary osteoarthritis, this patient is at significantly higher risk for which of the following postoperative complications?
Explanation
Question 22
Primary synovial chondromatosis typically involves which of the following pathophysiological processes?
Explanation
Question 23
A 40-year-old male notes a slowly enlarging mass in his trapezius muscle. MRI reveals a well-defined mass with signal intensity identical to subcutaneous fat, interspersed with distinct, thick striations of skeletal muscle fibers. What is the most likely diagnosis?
Explanation
Question 24
A 14-year-old female with Multiple Hereditary Exostoses (MHE) presents with a visible forearm deformity. Which of the following descriptions represents the most common sequence of forearm deformity in this condition?
Explanation
Question 25
A 24-year-old male with chronic back pain and stiffness is suspected of having Ankylosing Spondylitis. During the physical examination, the physician makes a mark at the level of the posterior superior iliac spines (dimples of Venus) and another mark 10 cm above it, then asks the patient to flex forward. This test is known as the:
Explanation
Question 26
Which major articulation is overwhelmingly the most common site of involvement for primary synovial chondromatosis?
Explanation
Question 27
A 55-year-old male presents with a large, deep intramuscular mass in his right thigh. Biopsy reveals mature adipocytes with focal areas of hyperchromatic, atypical stromal cells.
Which of the following molecular or genetic findings is diagnostic for distinguishing this lesion from a benign lipoma?
Explanation
Question 28
A 45-year-old male with long-standing ankylosing spondylitis presents to the emergency department after a minor fall. He complains of severe neck pain. Radiographs show a fracture extending through the C5-C6 disc space and involving the posterior elements.
What is the most appropriate definitive management?

Explanation
Question 29
A 25-year-old male with a known distal femur osteochondroma reports newly onset pain and a palpable increase in the size of the mass. MRI reveals a cartilage cap thickness of 2.8 cm with soft tissue edema. What is the next best step in management?
Explanation
Question 30
A 40-year-old male presents with chronic knee catching and pain. Radiographs reveal numerous uniformly sized, calcified loose bodies within the joint space.
What is the primary pathophysiologic mechanism for this condition?
Explanation
Question 31
A 14-year-old boy presents with multiple bony prominences around his knees and ankles. Family history is positive for a similar condition. Which of the following statements regarding his diagnosis is most accurate?
Explanation
Question 32
A 35-year-old male with ankylosing spondylitis has a severe chin-on-chest deformity, rendering him unable to look straight ahead.
If surgical correction is planned, at which spinal level is an extension osteotomy most safely and commonly performed to correct the cervicothoracic kyphosis?
Explanation
Question 33
A 50-year-old female presents with a soft, painless, mobile mass on her upper back. On MRI, the mass is well-circumscribed, hyperintense on T1-weighted images, and demonstrates complete signal loss on Short Tau Inversion Recovery (STIR) sequences. What is the most likely diagnosis?
Explanation
Question 34
An 18-year-old male presents with a painless, hard bony mass extending from the proximal lateral fibula. He recently developed a foot drop and decreased sensation over the dorsum of his foot. Compression of which nerve is most likely responsible for his symptoms?
Explanation
Question 35
A 38-year-old male with a history of primary synovial chondromatosis of the hip, treated with arthroscopic synovectomy 4 years ago, presents with rapidly worsening pain. Radiographs show a destructive, lytic lesion invading the acetabulum with an associated soft tissue mass. What is the most likely diagnosis?
Explanation
Question 36
A 50-year-old male with long-standing ankylosing spondylitis presents with localized, non-radiating thoracolumbar back pain. Radiographs reveal a destructive, irregular discovertebral lesion at T12-L1 with reactive sclerosis, mimicking discitis. His CRP is only mildly elevated. What is this lesion called?
Explanation
Question 37
A 12-year-old boy presents with a hard, painless bump on his distal femur. Radiographs show a pedunculated bony exostosis pointing away from the joint.
What is the pathognomonic radiographic feature required to confirm an osteochondroma?
Explanation
Question 38
A 60-year-old male is diagnosed with an atypical lipomatous tumor (well-differentiated liposarcoma) located deep in the retroperitoneum. Why is the prognosis for this retroperitoneal lesion poorer than for a histologically identical lesion in the deep soft tissues of the thigh?
Explanation
Question 39
Primary synovial chondromatosis is a benign neoplasm characterized by synovial metaplasia. Which specific genetic fusion is most frequently implicated in the pathogenesis of this disease?
Explanation
Question 40
A 28-year-old male with HLA-B27 positive ankylosing spondylitis presents for a routine follow-up. He complains of chronic, inflammatory lower back pain. Which of the following is the most common extra-articular manifestation associated with his underlying condition?
Explanation
Question 41
A 10-year-old boy presents with an incidentally discovered sessile osteochondroma of the proximal humerus. Over the next several years of skeletal growth, how will the relative position of this lesion change?
Explanation
Question 42
A 32-year-old male with active ankylosing spondylitis has persistent axial disease (sacroiliitis and spondylitis) despite maximally tolerated doses of two different NSAIDs. He has no peripheral joint involvement. What is the most appropriate next step in his medical management?
Explanation
Question 43
A 45-year-old female presents with a deep intramuscular lipoma in the proximal anterior forearm near the supinator muscle. She reports insidious, progressive weakness in extending her thumb and fingers, without any sensory deficits. Which nerve is most likely compressed by this mass?
Explanation
Question 44
A 65-year-old female with severe, end-stage osteoarthritis of the knee undergoes arthroplasty. Intraoperatively, multiple calcified loose bodies are found in the joint. Pathologic evaluation confirms secondary synovial chondromatosis. How does this condition characteristically differ from primary synovial chondromatosis?
Explanation
Question 45
A 55-year-old man presents with a deep 12 cm thigh mass. Biopsy shows mature adipose tissue with focal nuclear atypia. Molecular testing reveals MDM2 gene amplification. What is the most appropriate management?
Explanation
Question 46
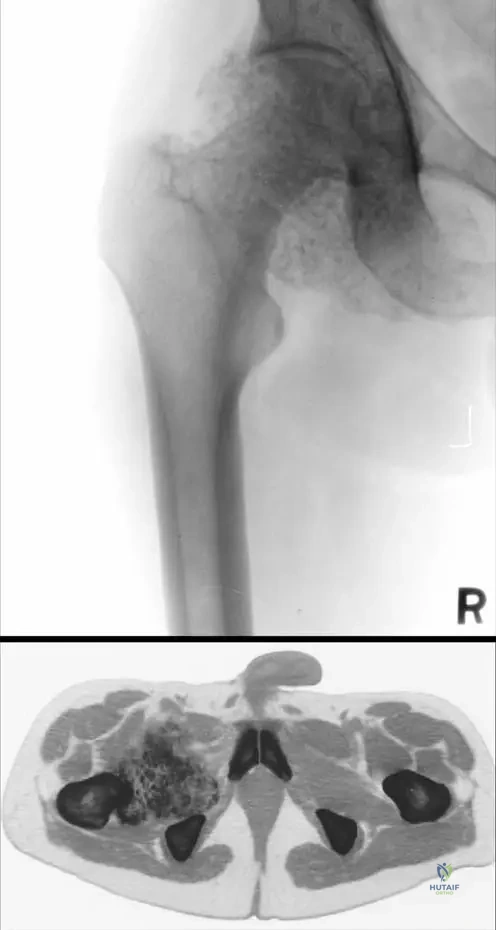
A 22-year-old male with multiple hereditary exostoses (MHE) reports new-onset, enlarging mass and pain around his right proximal femur. Which of the following is the strongest indicator of malignant transformation on imaging?
Explanation
Question 47
A 65-year-old man with advanced Ankylosing Spondylitis presents after a minor fall with severe neck pain. Radiographs are inconclusive. What is the most appropriate next step in management?
Explanation
Question 48
A 45-year-old woman complains of chronic right knee pain and locking. Imaging reveals multiple intra-articular calcified loose bodies of uniform size. What is the classic pathophysiologic mechanism of this condition?
Explanation
Question 49
A 12-year-old boy is diagnosed with Multiple Hereditary Exostoses (MHE). Genetic testing is likely to show a mutation in genes responsible for which of the following cellular processes?
Explanation
Question 50
A 50-year-old man with severe bilateral hip pain and a known history of Ankylosing Spondylitis is scheduled for a total hip arthroplasty (THA). He is at significantly increased risk for which of the following postoperative complications?
Explanation
Question 51
A 45-year-old woman presents with weakness in wrist extension and finger extension. MRI demonstrates a large mass composed uniformly of fat sitting intimately on the periosteum of the proximal radius. What is the most likely diagnosis?
Explanation
Question 52
A 30-year-old male with a history of primary synovial chondromatosis of the hip undergoes arthroscopic synovectomy. Ten years later, he presents with sudden, rapidly progressive hip pain and an enlarging mass. Radiographs show aggressive bone destruction. What is the most likely diagnosis?
Explanation
Question 53
An osteochondroma is generally considered to stop growing at skeletal maturity. If an osteochondroma-like lesion originates within the epiphysis rather than the metaphysis, leading to joint deformity and restricted motion, what is this condition termed?
Explanation
Question 54
A 68-year-old man with long-standing Ankylosing Spondylitis presents with a severe chin-on-chest deformity. Which cervical level is most commonly chosen for a closing wedge extension osteotomy to correct this deformity?
Explanation
Question 55
A painless soft tissue mass in the posterior neck of a 55-year-old man is biopsied. Histology reveals mature adipocytes, uniform spindle cells, and thick, rope-like collagen bundles without lipoblasts. Immunohistochemistry is strongly positive for CD34. What is the diagnosis?
Explanation
Question 56
A 55-year-old male with long-standing Ankylosing Spondylitis (AS) presents to the emergency department with severe neck pain following a minor fall from standing height. A CT scan of the cervical spine demonstrates a through-and-through chalk-stick fracture at the C5-C6 level. What is the most appropriate surgical management for this patient?
Explanation
Question 57
A 35-year-old male presents with a slowly enlarging, painless mass over the distal femur. Radiographs reveal a sessile bony exostosis pointing away from the joint. An MRI is obtained to evaluate the cartilage cap. Which of the following cartilage cap thicknesses is most indicative of malignant transformation to secondary chondrosarcoma in an adult?
Explanation
Question 58
A 40-year-old female presents with progressive knee pain and mechanical catching. Imaging reveals multiple intra-articular calcified loose bodies with relative preservation of the joint space. A diagnosis of primary synovial chondromatosis is suspected. What is the underlying pathogenesis of this condition?
Explanation
Question 59
A 60-year-old male presents with a large, deep-seated fatty mass in the thigh. Biopsy shows mature adipose tissue with focal atypia and hyperchromatic stromal cells. Cytogenetic analysis is ordered to differentiate an Atypical Lipomatous Tumor (ALT) from a benign lipoma. Which of the following genetic markers is characteristic of an ALT?
Explanation
Question 60
A 45-year-old male with advanced Ankylosing Spondylitis presents with fixed global positive sagittal imbalance. Surgical correction using a pedicle subtraction osteotomy (PSO) is planned. To maximize lordosis restoration and minimize the risk of spinal cord injury, what is the ideal spinal level for the PSO?
Explanation
Question 61
A 10-year-old boy presents with multiple bony bumps around his knees, ankles, and shoulders. He is short in stature and exhibits a mild forearm deformity. A diagnosis of Multiple Hereditary Exostoses (MHE) is made. What is the inheritance pattern and the most common genetic mutation associated with this condition?
Explanation
Question 62
A 60-year-old male presents with a deep intramuscular mass in the thigh. MRI reveals a large lipomatous lesion with thick septations.
Core needle biopsy shows adipocytes with variation in cell size and hyperchromatic stromal cells. Which of the following cytogenetic abnormalities is diagnostic for this tumor?
Explanation
Question 63
A 45-year-old male complains of chronic knee pain, swelling, and catching. Radiographs and MRI are shown.
What is the primary pathophysiological mechanism underlying this condition?
Explanation
Question 64
A 72-year-old male with a known history of ankylosing spondylitis presents with severe back pain after minor trauma. Imaging reveals a transvertebral fracture.
Which of the following is the most appropriate definitive management for this patient?
Explanation
Question 65
A 14-year-old boy is diagnosed with multiple hereditary exostoses (MHE). What is the normal physiological function of the proteins encoded by the genes most commonly mutated in this condition?
Explanation
Question 66
A 50-year-old male with long-standing ankylosing spondylitis presents with localized, worsening back pain without a history of trauma. Radiographs show a destructive discovertebral lesion with reactive sclerosis.
What is the most likely diagnosis?
Explanation
Question 67
A 40-year-old female presents with a painless, slow-growing mass on her proximal forearm. Radiographs demonstrate focal cortical hyperostosis of the proximal radius adjacent to a radiolucent soft-tissue mass. What is the most likely diagnosis?
Explanation
Question 68
A 25-year-old male with a known distal femur osteochondroma presents with a rapidly enlarging, pulsatile popliteal mass and calf pain.
What is the most likely etiology of the new mass?
Explanation
Question 69
Which of the following features best distinguishes primary synovial chondromatosis from secondary synovial chondromatosis?
Explanation
Question 70
A 45-year-old male incidentally undergoes a radiograph of his foot after a mild sprain. The lateral view shows a well-defined lytic lesion in the calcaneus with central calcification creating a target sign. What is the appropriate management?
Explanation
Question 71
A 32-year-old male with human leukocyte antigen (HLA)-B27 positive ankylosing spondylitis presents with acute unilateral eye pain, photophobia, and blurred vision. What is the most likely extra-articular manifestation he is experiencing?
Explanation
Question 72
A 15-year-old boy presents with a hard mass on his proximal tibia. Radiographs show a sessile bony exostosis pointing away from the joint space.
Which radiographic finding is required to definitively classify this lesion as an osteochondroma?
Explanation
Question 73
A 45-year-old male with severe ankylosing spondylitis presents with a fixed chin-on-chest deformity causing difficulty swallowing and impaired horizontal gaze. He is scheduled for an extension osteotomy. Which level is most appropriate for the osteotomy to correct the cervical deformity?
Explanation
Question 74
A 16-year-old boy with a known history of multiple hereditary exostoses (MHE) presents with worsening deformity of his left forearm and decreased range of motion. Radiographs reveal a characteristic forearm deformity associated with this condition. Which of the following best describes the typical pathoanatomy of the forearm in MHE?
Explanation
Question 75
A 35-year-old male is evaluated for a large, deep intramuscular thigh mass. Core needle biopsy confirms the presence of well-differentiated adipocytes, but the pathologist requests fluorescence in situ hybridization (FISH) to differentiate between a benign lipoma and an atypical lipomatous tumor (ALT). Amplification of which of the following gene loci is pathognomonic for ALT?
Explanation
Question 76
A 60-year-old male with long-standing ankylosing spondylitis presents with increasing difficulty looking forward due to a severe rigid cervicothoracic kyphosis. A cervical extension osteotomy is planned to correct his chin-on-chest deformity. At which anatomic level is this osteotomy most safely and classically performed?
Explanation
Question 77
A 45-year-old male presents with recurrent catching and locking in his left knee. Imaging reveals numerous uniformly sized, small calcified bodies confined within the joint capsule.
What is the most definitive histological hallmark distinguishing this condition from secondary osteochondromatosis?
Explanation
Question 78
A 14-year-old girl is evaluated for a painless, hard mass about the medial aspect of the proximal tibia.
Radiographs and MRI confirm the diagnosis of an osteochondroma. Which of the following imaging features is an absolute requirement to confidently make this diagnosis?
Explanation
Question 79
A 68-year-old male with a 30-year history of ankylosing spondylitis presents to the emergency department after a minor ground-level fall. He complains of moderate neck pain. Neurological examination is completely normal. Lateral cervical radiographs are largely obscured by his shoulders but show a fused spine. What is the most appropriate next step in management?
Explanation
Question 80
A 35-year-old male with long-standing primary synovial chondromatosis of the hip presents with rapid worsening of pain and joint swelling over the last three months. MRI reveals permeative destruction of the femoral neck with marrow replacement and a large soft tissue mass breaking through the joint capsule. What complication has most likely occurred?
Explanation
Question 81
Which of the following genetic mechanisms is fundamentally responsible for the pathogenesis of multiple hereditary exostoses (MHE)?
Explanation
Question 82
A 52-year-old male is referred for a painless, slow-growing soft tissue mass in his proximal forearm. MRI reveals a well-defined lipomatous mass located entirely within the belly of the brachioradialis muscle. Biopsy demonstrates mature adipocytes interdigitating with normal skeletal muscle fibers, without cytological atypia or lipoblasts. Which of the following statements regarding this lesion is true?
Explanation
Question 83
A 45-year-old male with a 20-year history of ankylosing spondylitis presents with severe bilateral hip pain and stiffness. Bilateral total hip arthroplasty (THA) is planned. Which of the following prophylactic measures is highly recommended postoperatively for this specific patient population?
Explanation
Question 84
An 18-year-old male presents with a pulsatile mass and a palpable thrill in the popliteal fossa of his right knee. He has a known history of a distal femur osteochondroma in the same leg. What is the most likely etiology of this vascular presentation?
Explanation
Question 85
A 65-year-old male presents with a slowly enlarging, painless soft tissue mass in the posterior subcutaneous neck. Excisional biopsy is performed. Histology demonstrates a mixture of mature adipocytes, uniform spindle cells, and thick, ropey collagen bundles in a myxoid background. Immunohistochemistry is positive for CD34. What is the most likely diagnosis?
Explanation
Question 86
A patient with long-standing ankylosing spondylitis sustains a cervical spine fracture extending through the C5-C6 intervertebral disc space and posterior elements.
Several hours after admission, he develops progressive bilateral lower extremity weakness and urinary retention. What is the most critical immediate diagnostic or therapeutic step?
Explanation
Question 87
During the surgical excision of a symptomatic solitary osteochondroma of the distal femur in a 20-year-old patient, which of the following oncologic principles is most critical to minimize the risk of local recurrence?
Explanation
Question 88
A 55-year-old woman is evaluated for a large mass deep in her thigh.
MRI reveals a predominantly high T1-signal mass with thick, nodular, enhancing septations (>2 mm). Biopsy confirms an Atypical Lipomatous Tumor (ALT). Which of the following statements best describes the biological behavior and appropriate treatment for this specific tumor?
Explanation
Question 89
Which of the following is the primary histological and pathophysiological initial event in the development of spinal ankylosis in ankylosing spondylitis?
Explanation
Question 90
A 30-year-old male with an established diagnosis of multiple hereditary exostoses presents with a newly enlarging, painful osteochondroma on his right iliac wing. He reached skeletal maturity 12 years ago. Imaging shows a cartilage cap measuring 3.5 cm in thickness. What is the most appropriate management?
Explanation
Question 91
Which of the following extraskeletal manifestations is most frequently associated with the HLA-B27 positive condition ankylosing spondylitis?
Explanation
Question 92
A patient is undergoing arthroscopy for primary synovial chondromatosis of the shoulder. During the procedure, the surgeon removes dozens of loose bodies. To minimize the rate of local recurrence of the condition, what additional intraoperative step is required?
Explanation
None
