ABOS Part I Orthopedic Surgery Review: Trauma, Foot & Ankle, & Oncology MCQs | Part 22213
Key Takeaway
This ABOS Part I Orthopedic Review module offers 32 advanced multiple-choice questions covering high-yield topics in orthopedic trauma and oncology. It delves into fracture management, Lisfranc injuries, compartment syndrome, and various liposarcoma types, including diagnosis, treatment strategies, and prognosis, essential for board exam preparation.
ABOS Part I Orthopedic Surgery Review: Trauma, Foot & Ankle, & Oncology MCQs | Part 22213
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 45-year-old male presents after a high-energy fall, sustaining a posterior wall acetabular fracture with a congruent reduction after closed hip dislocation. Post-reduction radiographs show no incarcerated fragments. Which of the following is the most appropriate management strategy?
Explanation
Correct Answer: C
For isolated posterior wall acetabular fractures that are congruent and stable after closed reduction of a hip dislocation, non-operative management with protected weight-bearing and restricted range of motion is a recognized option. Instability is typically assessed with stress radiographs or dynamic fluoroscopy after reduction. If stable, close monitoring for secondary displacement or late instability is crucial. Surgical indications usually include persistent instability, incarcerated fragments, or significant displacement. Immediate ORIF is typically reserved for unstable fractures or those with incarcerated fragments. Skeletal traction is less commonly used for these stable fracture patterns. Hip arthroplasty is not indicated primarily for this injury pattern without pre-existing arthritis or severe head damage. A CT scan is usually performed initially to assess the fracture pattern and rule out incarcerated fragments, but repeating it in 24 hours without clinical change is not the primary management.
Question 2
A 68-year-old female with osteoporosis falls at home, sustaining a displaced intertrochanteric hip fracture. She is otherwise healthy. What is the most appropriate definitive management for this fracture?
Explanation
Correct Answer: B
Displaced intertrochanteric hip fractures in elderly patients are typically managed surgically. A dynamic hip screw (DHS) is the gold standard for stable and reducible intertrochanteric fractures, providing controlled collapse at the fracture site which promotes impaction and healing. While intramedullary nailing (IMN) is often preferred for unstable intertrochanteric fractures (e.g., reverse obliquity, comminuted), a DHS remains a very viable option for many stable patterns, especially in the context of osteoporosis where load sharing is beneficial. Non-operative management is associated with high mortality and morbidity in this patient population. THA or hemiarthroplasty are generally reserved for displaced femoral neck fractures or failed previous fixation, not primarily for intertrochanteric fractures. External fixation is rarely used for these fractures due to high rates of complications and poor stability.
Question 3
A 32-year-old male sustains a Gustilo Type IIIB open tibia fracture with significant soft tissue loss and exposed bone. After initial debridement and stabilization, what is the most appropriate timing and method for definitive soft tissue coverage?
Explanation
Correct Answer: C
Gustilo Type IIIB open tibia fractures involve extensive soft tissue damage and often require specialized soft tissue coverage. The 'golden period' for these injuries extends beyond primary closure, which is typically reserved for clean, smaller wounds without significant contamination or tissue loss. For Type IIIB injuries, early and definitive soft tissue coverage, usually within 72 hours of injury, is critical to reduce infection rates and promote fracture healing. This often involves local rotational flaps or free tissue transfer, depending on the size and location of the defect. Delayed primary closure is not appropriate for large defects with exposed bone. Split-thickness skin grafts require a well-vascularized bed and are usually insufficient to cover exposed bone or deep structures. Leaving the wound open for weeks increases infection risk and prolongs hospitalization.
Question 4
Which of the following Salter-Harris fracture types has the highest risk of growth arrest?
Explanation
Correct Answer: E
Salter-Harris Type V fractures, which involve a crush injury to the growth plate, have the highest risk of growth arrest due to direct damage to the germinal cells. While relatively rare, the prognosis for future growth is poor. Type IV fractures (fracture through metaphysis, physis, and epiphysis) also carry a high risk if not anatomically reduced, as a cartilaginous bridge can form across the physis. Type I (separation of physis) and Type II (physis and metaphysis) generally have good prognoses if reduced. Type III (physis and epiphysis) have a better prognosis than Type IV or V but still require anatomical reduction, especially if intra-articular.
Question 5
A 35-year-old male sustains a high-energy rotational injury to his ankle, resulting in a Maisonneuve fracture. What is the key to appropriate diagnosis and management of this injury?
Explanation
Correct Answer: C
A Maisonneuve fracture is a specific type of ankle injury characterized by a fracture of the proximal fibula, rupture of the syndesmosis (anterior inferior tibiofibular ligament, posterior inferior tibiofibular ligament, interosseous membrane), and often a deltoid ligament rupture or medial malleolus fracture. The key to diagnosis is recognizing the proximal fibula fracture in the context of an ankle injury, which often appears innocuous on standard ankle views. The critical aspect for management is assessing and restoring syndesmotic integrity, as disruption of the syndesmosis leads to ankle instability. Fixation of the medial malleolus is only done if it is fractured and significantly displaced. Calcaneal fractures are not directly associated. Vascular injury is rare unless there's a significant open injury or dislocation. Non-weight bearing cast immobilization alone is insufficient if the syndesmosis is unstable, which it typically is.
Question 6
Which of the following findings is most concerning for impending compartment syndrome in a patient with a closed tibial shaft fracture?
Explanation
Correct Answer: E
While all listed options are potential signs of compartment syndrome, 'pain with passive stretching of the toes' (for the deep posterior and anterior compartments) and 'severe pain unresponsive to increasing doses of opioids' (pain out of proportion to injury) are considered the most sensitive and earliest signs of evolving compartment syndrome. Paresthesia can be an early sign but may also indicate nerve injury unrelated to compartment syndrome. Diminished pulses and pallor are late signs, often indicating irreversible muscle ischemia and nerve damage, and are less reliable early indicators because compartment pressure often exceeds venous pressure long before arterial flow is compromised.
Question 7
What is the most common serious complication following posterior hip dislocation, even after successful reduction?
Explanation
Correct Answer: B
Avascular necrosis (AVN) of the femoral head is the most common serious long-term complication following posterior hip dislocation, with incidence increasing with prolonged dislocation time. Sciatic nerve injury is common acutely but usually resolves partially or completely. Post-traumatic osteoarthritis is also a long-term sequela but AVN is more directly linked to the initial insult. Heterotopic ossification can occur but is less common and less debilitating than AVN or severe osteoarthritis. Recurrent dislocation is rare after a single, well-reduced dislocation without associated bony injury.
Question 8
A 60-year-old male falls from a height and sustains a Pilon fracture (distal tibial plafond fracture). He presents with significant swelling and skin blistering. What is the most appropriate initial management strategy?
Explanation
Correct Answer: B
Pilon fractures are high-energy injuries often associated with severe soft tissue damage. Significant swelling and blistering indicate compromised soft tissue envelope, making immediate ORIF risky due to high rates of wound complications and infection. The preferred initial management is to apply a spanning external fixator across the ankle to restore length, alignment, and indirectly reduce the fracture, which allows the soft tissues to recover. Definitive ORIF is then performed in a delayed fashion (often 7-14 days) once the swelling has subsided, and the skin wrinkles ('wrinkle sign'). A cast is insufficient to stabilize such a complex fracture. Percutaneous screws alone are usually inadequate. Amputation is a last resort.
Question 9
In the management of a stress fracture of the femoral neck, which of the following is an absolute indication for surgical fixation?
Explanation
Correct Answer: A
Tension-side stress fractures of the femoral neck (typically posterior-medial) are inherently unstable and have a high risk of progression to complete fracture and displacement, and a higher risk of avascular necrosis. Therefore, they are considered an absolute indication for surgical fixation (e.g., with cannulated screws). Compression-side fractures (anterior-superior) are generally more stable and can often be managed non-operatively with activity modification and protected weight-bearing, unless displacement occurs. While military recruits and athletes may benefit from surgical fixation to expedite return to activity, it's not an absolute indication for all stress fractures unless instability or displacement is present. Minimally displaced fractures would fall under the category of compression or tension-side and the management depends on that distinction.
Question 10
A 30-year-old patient with a transverse fracture of the tibial shaft presents with severe pain, swelling, and tense compartments in the lower leg. Compartment pressures are elevated. What is the most appropriate immediate intervention?
Explanation
Correct Answer: C
Elevated compartment pressures in the setting of severe pain, swelling, and tense compartments indicate acute compartment syndrome, which is a surgical emergency. The definitive treatment is an emergency fasciotomy to decompress the involved compartments and prevent irreversible muscle and nerve ischemia. Delay can lead to permanent disability (Volkmann's contracture), nerve damage, and even limb loss. All other options are inappropriate or cause critical delays.
Question 11
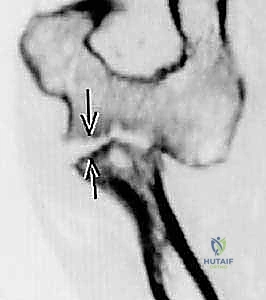
A 49-year-old female presents to the emergency department after falling down stairs, complaining of severe left foot pain, bruising, and swelling, with an inability to bear weight. Initial AP and oblique radiographs are obtained.
Based on the provided image, which of the following findings is MOST indicative of a Lisfranc injury?

Explanation
Correct Answer: C
Explanation:
The case explicitly states that the candidate identifies "diastasis of > 2 mm between the base of the first and second metatarsals" as a key feature suggestive of Lisfranc tarsometatarsal fracture dislocation. This finding, along with the presence of a 'fleck sign' (an avulsed fragment from the Lisfranc ligament insertion), is pathognomonic for a Lisfranc injury. The Lisfranc ligament connects the medial cuneiform to the base of the second metatarsal, and its disruption leads to instability and widening of the interval between the first and second metatarsal bases.
- Option A (Diastasis of 1 mm): While diastasis is a key sign, a 1 mm widening is often considered within normal limits or equivocal. A threshold of 2 mm or more is generally accepted as significant for Lisfranc injury, especially when compared to the contralateral foot or with stress views.
- Option B (Avulsed fragment lateral to the third metatarsal base): The 'fleck sign' specifically refers to an avulsion fracture from the insertion of the Lisfranc ligament, which is typically at the base of the second metatarsal, not the third.
- Option D (Fracture of the cuboid bone): While cuboid fractures can occur in foot trauma, they are not the primary diagnostic feature of a Lisfranc injury, which involves the tarsometatarsal joint complex.
- Option E (Subluxation of the navicular-cuneiform joint): This describes a Chopart joint injury, which is distinct from a Lisfranc injury involving the tarsometatarsal joints.
Question 12
Following initial radiographs, the emergency department physician is still uncertain about the diagnosis of a Lisfranc injury. The patient continues to experience severe pain and swelling. According to the case discussion, what would be the MOST appropriate next step in imaging to confirm or rule out a Lisfranc injury?
Explanation
Correct Answer: C
Explanation:
The case explicitly states the candidate's response to inconclusive radiographs: "I would consider further radiographic imaging, oblique and lateral view, stress views and a CT scan or may opt for an MRI scan." This indicates a clear progression of imaging modalities to definitively diagnose a Lisfranc injury when initial views are insufficient.
- Option A (Immediate MRI of the foot): While MRI is excellent for soft tissue and ligamentous injuries, it is often reserved for cases where CT is inconclusive or for assessing ligamentous integrity more precisely. The immediate next step typically involves further plain radiographs and CT.
- Option B (Repeat AP and oblique radiographs with increased exposure): Simply repeating the same views with different exposure is unlikely to provide new diagnostic information if the initial views were inconclusive for a structural injury like a Lisfranc dislocation. Additional views and advanced imaging are needed.
- Option C (Obtain lateral view, stress views, and a CT scan): This aligns perfectly with the candidate's recommended approach. A lateral view is crucial for assessing dorsal/plantar displacement, stress views can reveal instability not apparent on static films, and a CT scan provides detailed bony anatomy, crucial for identifying subtle fractures, displacement, and comminution within the complex tarsometatarsal joint.
- Option D (Order a bone scan): A bone scan is highly sensitive but non-specific for fractures and can take hours to days for results, making it unsuitable for acute diagnosis in the emergency setting for a potentially unstable injury.
- Option E (Discharge with a walking boot): Discharging a patient with a suspected Lisfranc injury, especially if radiographs are inconclusive, is inappropriate and carries a high risk of missed diagnosis and poor outcome, as up to 20% of these injuries are initially missed.
Question 13
A 49-year-old female is diagnosed with a Lisfranc tarsometatarsal fracture dislocation after falling down stairs. The CT scan confirms significant subluxation of the tarsometatarsal joints with a comminuted fracture at the base of the second metatarsal. Based on the case discussion, what is the MOST appropriate definitive management strategy for this patient?
Explanation
Correct Answer: B
Explanation:
The case outlines the treatment strategy based on the severity of the injury. For subluxation or dislocation, "accurate reduction and stable fixation is essential." The candidate specifically states, "In this case, I would consider open reduction and internal fixation with screws and possible plating, as required."
- Option A (Non-weightbearing cast for 6 weeks): This is indicated only for "undisplaced stable injury or sprain." The patient's CT scan shows "significant subluxation" and a "comminuted fracture," which clearly indicates an unstable, displaced injury requiring surgical intervention.
- Option B (Open reduction and internal fixation (ORIF) with screws and possible plating): This is the primary treatment for displaced Lisfranc injuries, as described in the case. The goal is accurate anatomical reduction and stable fixation to restore joint congruity and prevent post-traumatic osteoarthritis.
- Option C (Primary arthrodesis of the tarsometatarsal joints): Primary arthrodesis is reserved for "severely comminuted fracture" where anatomical reduction and stable fixation are not achievable, or in cases of chronic instability or severe arthritis. While the patient has a comminuted fracture, the primary approach for acute subluxation/dislocation is typically ORIF unless the comminution is so severe that reconstruction is impossible.
- Option D (Closed reduction and percutaneous pinning): While sometimes used for less severe or purely ligamentous injuries, the presence of a comminuted fracture and significant subluxation often necessitates open reduction to achieve anatomical alignment and more robust fixation than percutaneous pinning can provide.
- Option E (Below-knee backslab for pain control and delayed definitive treatment): A backslab is appropriate for initial stabilization and pain control, as mentioned in the case, but it is not the definitive treatment for a displaced Lisfranc injury. Definitive treatment should not be unduly delayed.
Question 14
A 49-year-old female with a Lisfranc injury is undergoing initial management. The orthopedic resident is performing a physical examination of the injured foot. Which of the following clinical findings, if present, would raise the MOST immediate concern for a developing compartment syndrome?
Explanation
Correct Answer: C
Explanation:
The case specifically highlights the importance of assessing neurovascular status and excluding compartment syndrome. The candidate states, "Neurovascular status, dorsalis pedis pulse" and "Compartment syndrome must be excluded." The classic signs of compartment syndrome include the '6 Ps': Pain (out of proportion), Pallor, Paresthesia, Pulselessness, Paralysis, and Poikilothermia. Among the options, a diminished pulse combined with severe pain out of proportion is a critical red flag.
- Option A (Painful passive abduction/pronation): This is a classic clinical sign of a Lisfranc injury itself, indicating instability and pain at the tarsometatarsal joints, but not specifically indicative of compartment syndrome.
- Option B (Ecchymosis and swelling around the midfoot): These are common findings in any significant foot trauma, including a Lisfranc injury, and while they can contribute to compartment syndrome, they are not direct signs of it.
- Option C (Diminished dorsalis pedis pulse with severe pain out of proportion to injury): "Pain out of proportion" is the hallmark symptom of compartment syndrome. A diminished dorsalis pedis pulse indicates compromised arterial flow, which is a late and ominous sign of severe compartment syndrome, suggesting significant tissue ischemia. This combination warrants immediate concern and intervention.
- Option D (Tenderness over the tarsometatarsal joints): This is a direct sign of a Lisfranc injury, indicating localized trauma and fracture/dislocation, but not specific to compartment syndrome.
- Option E (Inability to bear weight): This is a general symptom of severe lower limb injury and is expected with a Lisfranc injury, but it does not specifically point to compartment syndrome.
Question 15
A 49-year-old female with a Lisfranc injury is being counseled regarding her prognosis. Based on the information provided in the case, which of the following statements should the orthopedic surgeon include in the discussion with the patient?
Explanation
Correct Answer: D
Explanation:
The case explicitly addresses the prognosis for Lisfranc injuries, stating, "This is a serious injury with potentially a poor outcome. Post-traumatic osteoarthritis may occur in more than 50% of cases despite surgical intervention. Residual pain and stiff foot are not uncommon complications of this injury." This information is crucial for informed consent and realistic patient expectations.
- Option A (Full return to pre-injury activity within 3 months): This is overly optimistic for a serious injury like a Lisfranc fracture-dislocation, which often requires a prolonged recovery period, sometimes up to a year or more, and may not result in a full return to pre-injury activity.
- Option B (Post-traumatic osteoarthritis is a rare complication, occurring in less than 10% of cases): This contradicts the case, which states it may occur in "more than 50% of cases."
- Option C (Residual pain and a stiff foot are uncommon): This also contradicts the case, which states they "are not uncommon complications."
- Option D (This is a serious injury with a potentially poor outcome, and post-traumatic osteoarthritis may occur in more than 50% of cases despite surgery): This statement directly reflects the prognosis provided in the case, emphasizing the severity and potential long-term complications.
- Option E (Recovery period is generally short, and patients can expect to resume full weight-bearing within 6 weeks): This is incorrect. Even for stable injuries, non-weightbearing is typically for 6 weeks, and for surgical cases, the recovery and return to full weight-bearing are much longer.
Question 16
A 49-year-old female presents with a Lisfranc injury. During the initial assessment, the orthopedic team is vigilant for the development of compartment syndrome. If compartment syndrome is clinically diagnosed in the foot, what is the MOST appropriate immediate management step?
Explanation
Correct Answer: C
Explanation:
The case clearly states, "Once compartment syndrome has been diagnosed clinically, emergency decompression is required." This highlights the urgency and definitive nature of surgical intervention for this limb-threatening condition.
- Option A (Administer high-dose corticosteroids): Corticosteroids are not indicated for the treatment of acute compartment syndrome and may even be detrimental.
- Option B (Apply ice packs and elevate the limb): While elevation is generally good for swelling, in compartment syndrome, excessive elevation can further compromise blood flow. Ice packs are not a treatment for compartment syndrome. These measures are insufficient to reduce dangerously elevated compartment pressures.
- Option C (Perform emergency surgical decompression (fasciotomy) of the foot compartments): This is the definitive and emergency treatment for acute compartment syndrome. The case describes the specific technique of decompressing the nine compartments of the foot through three incisions.
- Option D (Monitor compartment pressures hourly and reassess clinical signs): While compartment pressures can be monitored, once the clinical diagnosis of compartment syndrome is made, surgical decompression should not be delayed by prolonged monitoring. Clinical diagnosis is paramount.
- Option E (Order an urgent MRI): MRI is not the primary diagnostic tool for acute compartment syndrome and would cause an unacceptable delay in treatment. Clinical diagnosis and immediate surgical intervention are critical to prevent irreversible tissue damage.
Question 17
A 49-year-old female sustains a Lisfranc injury. The candidate in the case mentions the importance of the 'fleck sign'. What does the 'fleck sign' specifically represent in the context of a Lisfranc injury?
Explanation
Correct Answer: A
Explanation:
The case explicitly defines the 'fleck sign': "There is a small avulsed fragment of bone in that interval. This avulsion fracture could be from the insertion of the Lisfranc ligament into the base of the second metatarsal, called a ‘fleck sign’." This is a classic radiographic indicator of a Lisfranc ligament injury.
- Option A (A small avulsion fracture from the insertion of the Lisfranc ligament into the base of the second metatarsal): This is the correct definition of the 'fleck sign' as described in the case and in orthopedic literature. It signifies disruption of the Lisfranc ligament complex.
- Option B (A small intra-articular fracture within the talonavicular joint): This describes an injury to the Chopart joint, not the Lisfranc joint.
- Option C (A displaced fracture of the cuboid bone): While cuboid fractures can occur, they are not referred to as a 'fleck sign' in the context of Lisfranc injuries.
- Option D (A comminuted fracture of the medial cuneiform): Fractures of the cuneiforms can be part of a Lisfranc injury, but the 'fleck sign' specifically refers to the avulsion from the second metatarsal base.
- Option E (A small osteochondral defect on the talar dome): This is an ankle injury, unrelated to the Lisfranc joint.
Question 18
A 49-year-old female presents with a Lisfranc injury. The initial management includes analgesia, elevation, and splinting with a below-knee backslab. The candidate emphasizes the importance of regular clinical examinations and monitoring. What is the primary reason for this vigilant monitoring in the acute phase?
Explanation
Correct Answer: C
Explanation:
The case explicitly states, "On admission to hospital I would arrange for regular clinical examinations and monitoring in order not to miss an early developing compartment syndrome." This highlights the critical importance of vigilance for this potentially devastating complication.
- Option A (To assess for signs of infection): While infection is a concern with any injury, especially open ones, it is not the primary acute concern driving immediate, regular monitoring in the context of a closed Lisfranc injury.
- Option B (To ensure proper alignment of the fracture within the backslab): While important, alignment is typically assessed radiographically. Clinical monitoring is more focused on physiological changes.
- Option C (To detect early signs of developing compartment syndrome): This is the most critical reason for vigilant monitoring in the acute phase of a significant foot injury. Compartment syndrome can lead to irreversible tissue damage if not promptly diagnosed and treated.
- Option D (To evaluate the patient's pain tolerance and adjust analgesia): Pain management is important, but it is a secondary goal compared to detecting a limb-threatening condition like compartment syndrome.
- Option E (To prepare the patient for immediate weight-bearing): Patients with Lisfranc injuries, especially those requiring surgery, are typically non-weightbearing for an extended period, not immediately after swelling subsides.
Question 19
A 49-year-old female with a Lisfranc injury is being prepared for surgical intervention due to significant displacement. The surgeon plans to perform open reduction and internal fixation. Which of the following is a critical step that must be completed prior to taking the patient to the operating theatre, as emphasized in the case?
Explanation
Correct Answer: C
Explanation:
The case explicitly states, "Informed consent should be taken. The management options, postoperative rehabilitation, outcome and potential complications should be discussed in detail with the patient and documented in medical records." This is a fundamental ethical and legal requirement before any surgical procedure.
- Option A (Obtain a second opinion): While sometimes helpful, a second opinion is not a mandatory critical step before every surgical case, especially when the diagnosis and treatment plan are clear.
- Option B (Administer prophylactic antibiotics 24 hours prior): Prophylactic antibiotics are typically given within 60 minutes prior to incision, not 24 hours prior, to be most effective.
- Option C (Discuss management options, postoperative rehabilitation, outcome, and potential complications with the patient and obtain informed consent): This is a crucial step for patient autonomy and shared decision-making, as highlighted in the case.
- Option D (Ensure the patient has been non-weightbearing for at least 72 hours): While non-weightbearing is part of initial management, a specific 72-hour non-weightbearing period is not a universal prerequisite for surgery, especially if the soft tissue envelope is acceptable.
- Option E (Perform a diagnostic arthroscopy): Diagnostic arthroscopy of the tarsometatarsal joints is not a standard or necessary step prior to ORIF for a Lisfranc injury. The diagnosis is typically made with radiographs and CT.
Question 20
A 49-year-old female with a Lisfranc injury is being managed. The case mentions that for an undisplaced stable injury or sprain, non-operative management is an option. What does this non-operative management typically entail?
Explanation
Correct Answer: B
Explanation:
The case clearly outlines the non-operative management for undisplaced stable injuries: "There is a role for non-operative management of an undisplaced stable injury or sprain which includes a non-weightbearing cast for 6 weeks and regular clinical and radiological review."
- Option A (Immediate weight-bearing in a walking boot): This is inappropriate for any Lisfranc injury, even stable ones, as it risks displacement and further damage.
- Option B (Non-weightbearing cast for 6 weeks with regular clinical and radiological review): This directly matches the description in the case for stable, undisplaced injuries. The non-weightbearing period allows for ligamentous healing.
- Option C (Physical therapy focusing on early range of motion and strengthening): Early range of motion and strengthening would be contraindicated during the initial non-weightbearing phase for a Lisfranc injury, as it could disrupt healing.
- Option D (Pain management with NSAIDs and activity modification only): This is insufficient for a Lisfranc injury, even a stable sprain, which requires immobilization and protection from weight-bearing.
- Option E (Custom orthotics and gradual return to activity): Orthotics may be used later in rehabilitation, but they are not the primary initial non-operative management for a Lisfranc injury.
Question 21
A 49-year-old female presents with a Lisfranc injury. The provided radiographs show the characteristic findings.
Considering the anatomy of the Lisfranc joint complex, which of the following statements accurately describes the primary stabilizing structure that is typically disrupted in this type of injury?

Explanation
Correct Answer: C
Explanation:
The case explicitly mentions the Lisfranc ligament and its insertion. The Lisfranc joint complex is stabilized by a network of ligaments, but the Lisfranc ligament itself is the key structure connecting the medial cuneiform to the base of the second metatarsal. Its disruption is central to the instability seen in Lisfranc injuries.
- Option A (The plantar fascia): The plantar fascia is a strong aponeurosis on the sole of the foot, crucial for arch support, but not the primary stabilizer of the tarsometatarsal joints.
- Option B (The spring ligament): The spring ligament (plantar calcaneonavicular ligament) supports the talar head and the medial longitudinal arch, primarily stabilizing the talonavicular joint, which is part of the Chopart joint, not the Lisfranc joint.
- Option C (The Lisfranc ligament, connecting the medial cuneiform to the base of the second metatarsal): This is the correct anatomical description of the Lisfranc ligament, which is the primary stabilizer preventing dorsal and lateral displacement of the metatarsals relative to the tarsus. Its disruption is the hallmark of a Lisfranc injury.
- Option D (The deltoid ligament): The deltoid ligament is a strong ligament on the medial side of the ankle, stabilizing the tibiotalar joint, not the midfoot.
- Option E (The calcaneocuboid ligament): This ligament stabilizes the calcaneocuboid joint, part of the Chopart joint, and is not the primary stabilizer of the Lisfranc joint complex.
Question 22
A 58-year-old male presents with a 12 cm, firm, deep-seated mass in his posterior thigh that has been slowly growing over the past 18 months. He reports occasional dull ache but no specific neurological symptoms. Physical examination reveals a non-mobile, firm mass. Which of the following clinical characteristics is the MOST concerning for a potential liposarcoma rather than a benign lipoma?
Explanation
Correct Answer: D
Academic Rationale
The most concerning clinical features for a potential liposarcoma, as opposed to a benign lipoma, are its deep-seated location and size greater than 5 cm. While benign lipomas can be large, a deep location (e.g., intramuscular or subfascial) significantly increases the suspicion for malignancy. A size greater than 5 cm is a commonly cited threshold that warrants further investigation for soft tissue masses. Progressive growth, even if slow, is also a red flag.
- A. The presence of occasional dull ache: While pain can be a symptom of malignancy, it is not a specific or highly sensitive indicator. Benign lipomas, especially angiolipomas or those causing mass effect on nerves, can also be painful.
- B. The mass being non-mobile on physical examination: Non-mobility or fixation to deeper structures is concerning, as it suggests infiltration, which is more characteristic of malignancy. However, a deep-seated mass, even if benign, might feel less mobile than a superficial one. The combination with size and depth is more critical.
- C. Slow growth over 18 months: Slow growth can occur with low-grade sarcomas, such as well-differentiated liposarcomas. However, any progressive growth, especially in a deep and large mass, is concerning. Rapid growth is a stronger indicator of high-grade malignancy, but slow growth does not rule out a low-grade sarcoma.
- E. Absence of specific neurological symptoms: The absence of neurological symptoms does not rule out malignancy. Many sarcomas, especially in early stages or in locations not directly impinging on nerves, are asymptomatic or cause only vague discomfort.
Therefore, the combination of deep location and large size is the most critical alarm bell in this scenario.
Question 23
A 48-year-old female presents with a 9 cm fatty mass in her anterior thigh. MRI reveals a well-circumscribed lesion with uniform high signal intensity on T1-weighted images, identical to subcutaneous fat. However, there are also several internal septations, some measuring 3 mm in thickness, which show mild enhancement after gadolinium administration. There are no discrete non-adipose nodules. What is the most appropriate interpretation of these MRI findings?
Explanation
Correct Answer: C
Academic Rationale
While uniform fat signal is characteristic of a benign lipoma, the presence of internal septations, particularly if they are thick (>2mm) and enhancing, significantly raises suspicion for atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS). Benign lipomas typically have thin (<2mm), non-enhancing septa or no septa at all. The size of the lesion (9 cm) also adds to the concern, as larger fatty masses are more likely to be liposarcomas.
- A. Consistent with a benign lipoma, requiring no further action: This is incorrect. The enhancing thick septa are a red flag that differentiates this from a classic benign lipoma.
- B. Suggestive of a necrotic lipoma, requiring observation: Necrotic lipomas are rare and would typically show different imaging characteristics, such as fluid collections or gas, and observation is not appropriate for a suspicious mass.
- D. Indeterminate, but most likely a benign lipoma with atypical features: While it is technically indeterminate without biopsy, the imaging features are strong enough to classify it as 'highly suspicious' for ALT/WDLPS, necessitating further workup (biopsy).
- E. Characteristic of a myxoid liposarcoma: Myxoid liposarcomas typically have a significant non-fatty, myxoid component that appears as high signal on T2-weighted images and shows enhancement, often with a characteristic plexiform vascular pattern. While they can contain fat, the primary description here of a predominantly fatty mass with enhancing septa points more towards WDLPS/ALT.
Therefore, the combination of size, deep location (implied by thigh mass), and especially the thick, enhancing septa makes ALT/WDLPS the most likely diagnosis.
Question 24
A core needle biopsy of a deep-seated fatty mass in the retroperitoneum reveals mature adipocytes with mild nuclear atypia and scattered atypical stromal cells. Immunohistochemical staining shows strong nuclear positivity for MDM2 and CDK4. These findings are most consistent with which diagnosis?
Explanation
Correct Answer: D
Academic Rationale
The histological findings of mature adipocytes with mild nuclear atypia and scattered atypical stromal cells are characteristic of a well-differentiated liposarcoma (WDLPS). The key diagnostic confirmation comes from the strong nuclear positivity for MDM2 and CDK4. Amplification of the MDM2 and CDK4 genes, located on chromosome 12q13-15, is the hallmark genetic alteration found in WDLPS and atypical lipomatous tumor (ALT). This genetic marker is critical for distinguishing WDLPS/ALT from benign lipomas, which lack these amplifications.
- A. Benign lipoma with reactive changes: Benign lipomas do not exhibit significant nuclear atypia or atypical stromal cells, nor do they show MDM2/CDK4 amplification.
- B. Hibernoma: Hibernomas are benign tumors of brown fat, characterized by multivacuolated adipocytes with granular eosinophilic cytoplasm, and do not show MDM2/CDK4 amplification.
- C. Myxoid liposarcoma: Myxoid liposarcomas are characterized by a prominent myxoid matrix, a delicate plexiform capillary network, and primitive round/spindle cells, often with FUS-DDIT3 fusion gene, not MDM2/CDK4 amplification.
- E. Dedifferentiated liposarcoma (DDLPS): DDLPS is defined by the coexistence of a WDLPS component with a distinct, non-lipogenic, high-grade sarcomatous component. While it originates from WDLPS and would therefore also show MDM2/CDK4 amplification, the biopsy description does not mention a high-grade non-lipogenic component. The findings described are purely those of the well-differentiated component.
Given the specific histological and immunohistochemical findings, WDLPS is the most accurate diagnosis.
Question 25
A 65-year-old male is diagnosed with a large, retroperitoneal well-differentiated liposarcoma (WDLPS) after an extensive workup. What is the primary concern regarding the behavior and prognosis of this tumor, specifically due to its retroperitoneal location?
Explanation
Correct Answer: C
Academic Rationale
Retroperitoneal liposarcomas, even those histologically classified as well-differentiated (WDLPS), have a significantly different biological behavior and prognosis compared to their extremity counterparts (where they are termed Atypical Lipomatous Tumors, ALT). In the retroperitoneum, WDLPS has a high propensity for local recurrence and, more significantly, for dedifferentiation into a higher-grade sarcoma. This dedifferentiation confers metastatic potential and significantly worsens prognosis. The anatomical constraints of the retroperitoneum also make achieving wide, negative surgical margins challenging, further contributing to high local recurrence rates.
- A. High risk of distant metastasis to the lungs: While dedifferentiated liposarcomas (DDLPS) do have metastatic potential, WDLPS itself does not metastasize unless it dedifferentiates. The primary concern for retroperitoneal WDLPS is dedifferentiation, which then leads to metastatic risk.
- B. Low risk of local recurrence after complete excision: This is incorrect. Retroperitoneal WDLPS has a very high local recurrence rate due to its infiltrative nature and the difficulty of achieving wide margins in this anatomical space.
- D. High sensitivity to systemic chemotherapy, making it the primary treatment: WDLPS is generally not highly sensitive to conventional chemotherapy. Aggressive surgical resection is the cornerstone of treatment.
- E. Rapid growth leading to early symptoms and easy detection: Retroperitoneal sarcomas often grow to very large sizes before causing symptoms due to the expansive nature of the retroperitoneal space, making early detection challenging.
Therefore, the potential for dedifferentiation and high local recurrence are the primary concerns for retroperitoneal WDLPS.
Question 26
A 35-year-old patient presents with a 7 cm, deep-seated, firm mass in the popliteal fossa. A core needle biopsy reveals a tumor composed of primitive round and spindle cells within an abundant myxoid stroma, associated with a delicate plexiform capillary network. Lipoblasts are present. Which of the following is the most appropriate initial treatment strategy for this patient?
Explanation
Correct Answer: C
Academic Rationale
The histological description (primitive round/spindle cells, myxoid stroma, plexiform capillary network, lipoblasts) is classic for myxoid liposarcoma. Myxoid liposarcoma, particularly when deep-seated and large (7 cm), is a high-grade sarcoma that is recognized for its relative sensitivity to both chemotherapy and radiotherapy. Therefore, a multidisciplinary approach involving neoadjuvant (pre-operative) chemotherapy and/or radiotherapy followed by wide local excision is the most appropriate initial treatment strategy.
- A. Observation with serial imaging due to its low-grade nature: This is incorrect. Myxoid liposarcoma is a malignant tumor with metastatic potential, and observation is not appropriate.
- B. Primary amputation due to the critical location: While the popliteal fossa is a critical anatomical area, limb salvage is the goal for most sarcomas. Neoadjuvant therapy can often shrink the tumor and facilitate a limb-sparing wide local excision. Amputation is reserved for cases where limb salvage is not feasible or would result in a non-functional limb.
- D. Marginal excision with careful follow-up: Marginal excision is inadequate for a sarcoma and would lead to a very high local recurrence rate. Wide local excision with negative margins is required.
- E. Intralesional corticosteroid injection for symptomatic relief: This is an inappropriate treatment for a malignant tumor.
Neoadjuvant therapy aims to improve resectability, achieve better margins, and potentially address micrometastatic disease, making it the preferred initial approach for this type of tumor.
Question 27
A 50-year-old patient undergoes resection of a large retroperitoneal fatty tumor. Histopathological examination reveals areas of well-differentiated liposarcoma (WDLPS) alongside a distinct, high-grade, non-lipogenic sarcomatous component resembling an undifferentiated pleomorphic sarcoma. What is the most accurate statement regarding the prognosis and metastatic potential of this specific tumor subtype?
Explanation
Correct Answer: C
Academic Rationale
The description of a well-differentiated liposarcoma (WDLPS) component coexisting with a distinct, high-grade, non-lipogenic sarcomatous component (e.g., undifferentiated pleomorphic sarcoma-like) is the definition of a dedifferentiated liposarcoma (DDLPS). DDLPS is an aggressive subtype of liposarcoma, particularly common in the retroperitoneum. It carries a high risk of local recurrence due to its infiltrative nature and the difficulty of achieving wide margins in the retroperitoneum. Crucially, the dedifferentiated component confers significant distant metastatic potential, primarily to the lungs, but also to other sites. This makes its prognosis considerably worse than that of WDLPS/ALT.
- A. It has a low risk of local recurrence and no metastatic potential: This describes a well-excised ALT in an extremity, not DDLPS.
- B. It is a benign tumor with a high chance of spontaneous regression: This is entirely incorrect; DDLPS is a high-grade malignancy.
- D. It is highly sensitive to chemotherapy, which is curative as a monotherapy: DDLPS is generally resistant to conventional chemotherapy as a monotherapy, though chemotherapy may be used in a neoadjuvant or adjuvant setting. Aggressive surgical resection is the cornerstone of treatment.
- E. Its prognosis is similar to a benign lipoma, regardless of size: This is incorrect. DDLPS is a high-grade malignancy with a guarded prognosis.
Therefore, the presence of dedifferentiation significantly worsens the prognosis, primarily due to increased local recurrence and metastatic risk.
Question 28
A 40-year-old patient presents with a small (2 cm), firm, tender subcutaneous nodule on her forearm that has been present for several months and is mildly painful to palpation. MRI shows a well-circumscribed fatty lesion with a prominent vascular component. Which benign fatty tumor variant is most consistent with this presentation?
Explanation
Correct Answer: D
Academic Rationale
The key distinguishing feature in this clinical vignette is the painful and tender nature of the subcutaneous fatty nodule, combined with the MRI finding of a prominent vascular component. This presentation is classic for an angiolipoma. Angiolipomas are benign lipomatous tumors characterized by a significant proliferation of mature capillary-sized vessels within the adipose tissue, which is thought to contribute to their characteristic tenderness or pain.
- A. Conventional lipoma: These are typically soft, mobile, and painless.
- B. Hibernoma: These are rare tumors of brown fat, usually painless, and found in specific locations like the neck, axilla, or mediastinum.
- C. Spindle cell lipoma: These are benign tumors characterized by mature adipocytes and uniform spindle cells. They are typically painless and found in the posterior neck, shoulder, and back of older men.
- E. Pleomorphic lipoma: These are benign tumors characterized by mature adipocytes, spindle cells, and characteristic 'floret-type' giant cells. They are typically painless and found in similar locations to spindle cell lipomas.
Therefore, the combination of pain/tenderness and a prominent vascular component on imaging strongly points to angiolipoma.
Question 29
A 68-year-old male is diagnosed with a 10 cm high-grade pleomorphic liposarcoma of the proximal thigh. He has no palpable lymphadenopathy. Which of the following imaging modalities is most crucial for initial systemic staging to detect potential distant metastases?
Explanation
Correct Answer: C
Academic Rationale
For a newly diagnosed high-grade soft tissue sarcoma, such as a pleomorphic liposarcoma, the most common site of distant metastasis is the lungs. Therefore, a CT scan of the chest is crucial for detecting pulmonary metastases. Given the size and high-grade nature, a CT scan of the abdomen and pelvis is also typically included to screen for other potential visceral metastases, especially if the primary tumor is large or located in the trunk. This comprehensive cross-sectional imaging provides the most critical information for systemic staging.
- A. Regional lymph node ultrasound: Lymph node metastases are uncommon in most soft tissue sarcomas, including liposarcoma (with the exception of epithelioid sarcoma and rhabdomyosarcoma). Therefore, routine regional lymph node dissection or extensive imaging is not typically indicated unless there is palpable lymphadenopathy.
- B. Bone scan (Technetium-99m): Bone scans are primarily used to detect bone metastases. While some sarcomas (e.g., myxoid liposarcoma) can metastasize to bone, it is less common than lung metastasis, and a bone scan is usually reserved for cases with bone pain or suspicious findings on other imaging.
- D. Comprehensive blood work including tumor markers: Tumor markers are generally not reliable or specific for the diagnosis or staging of soft tissue sarcomas.
- E. MRI of the brain: Brain metastases are rare for most soft tissue sarcomas, except for specific subtypes like high-grade myxoid liposarcoma. It is not part of routine initial staging for pleomorphic liposarcoma unless there are neurological symptoms.
Thus, CT of the chest, abdomen, and pelvis is the most appropriate and crucial initial systemic staging modality.
Question 30
A patient undergoes wide local excision for a high-grade liposarcoma of the thigh. The final pathology report indicates a positive surgical margin (R1 resection). What is the most significant implication of this finding for the patient's prognosis?
Explanation
Correct Answer: C
Academic Rationale
Margin status is consistently the most critical factor influencing local recurrence rates for all types of soft tissue sarcomas, including liposarcomas. A positive surgical margin (R1 resection), meaning microscopic tumor cells are present at the edge of the resected specimen, is a strong predictor of significantly increased risk of local recurrence. Achieving negative surgical margins (R0 resection) is paramount for local disease control.
- A. Increased risk of distant metastasis: While positive margins can be associated with a worse overall prognosis, their primary impact is on local control. Distant metastasis is more strongly correlated with tumor grade, size, and histological subtype.
- B. Necessity for immediate primary amputation: Amputation is a drastic measure and is not automatically indicated for a positive margin. Re-excision to achieve negative margins, often combined with adjuvant radiotherapy, is the standard approach.
- D. Indication for systemic chemotherapy as the sole adjuvant treatment: Chemotherapy is generally used for systemic disease or to improve resectability, but it is not a substitute for local control measures like re-excision or radiotherapy for positive margins. Adjuvant radiotherapy is often indicated for positive margins.
- E. No significant impact on long-term survival if the tumor was small: Even for smaller tumors, positive margins significantly increase the risk of local recurrence, which can compromise limb function and potentially lead to further morbidity or mortality if subsequent recurrences are more aggressive or difficult to treat.
Therefore, a positive surgical margin is primarily a predictor of local failure.
Question 31
A 30-year-old male presents with chronic, painless knee swelling. MRI reveals a diffuse, villous, frond-like proliferation of the synovial membrane within the joint, particularly prominent in the suprapatellar pouch. The proliferating tissue demonstrates signal characteristics identical to subcutaneous fat on all sequences. What is the most likely diagnosis?
Explanation
Correct Answer: C
Academic Rationale
The MRI findings of a diffuse, villous, frond-like proliferation of the synovial membrane with signal characteristics identical to subcutaneous fat are pathognomonic for lipoma arborescens. This is a rare, benign condition characterized by a diffuse lipomatous (fatty) infiltration of the synovial membrane, most commonly affecting the knee joint, particularly the suprapatellar pouch.
- A. Synovial chondromatosis: This involves cartilaginous metaplasia of the synovium, leading to loose bodies that are typically low signal on T1 and T2 (unless calcified) and do not demonstrate fat signal.
- B. Pigmented villonodular synovitis (PVNS): PVNS is characterized by synovial proliferation with hemosiderin deposition, which typically appears as very low signal intensity on all MRI sequences (especially T2* gradient echo) due to susceptibility artifact, not fat signal.
- D. Rheumatoid arthritis: This is an inflammatory arthritis characterized by synovial hypertrophy, pannus formation, and joint effusions, but the synovial tissue itself does not show fat signal intensity.
- E. Intra-articular lipoma: An intra-articular lipoma is a benign, circumscribed collection of mature adipose tissue located within the joint capsule but typically external to the synovium, or as a localized mass within the synovium, not a diffuse villous proliferation of the entire synovial membrane.
The diffuse villous fatty proliferation of the synovium is the key to diagnosing lipoma arborescens.
Question 32
A 55-year-old patient is undergoing workup for a soft tissue mass. The orthopedic oncologist emphasizes the importance of performing a core needle biopsy rather than an excisional biopsy for any suspicious lesion. What is the primary reason for this recommendation?
Explanation
Correct Answer: C
Academic Rationale
The primary reason for preferring a core needle biopsy over an excisional biopsy for a suspicious soft tissue mass is to minimize contamination of tissue planes and preserve options for definitive limb-salvage surgery. An excisional biopsy, if performed without oncologic principles, can spread tumor cells into surrounding healthy tissues, creating a contaminated field that makes subsequent wide local excision more challenging and potentially compromises the ability to achieve clear margins or even necessitates a more extensive resection (e.g., amputation).
- A. Core needle biopsy provides a larger tissue sample for diagnosis: While core needle biopsy provides sufficient tissue for diagnosis, excisional biopsy typically provides a larger sample. However, the quality and strategic placement of the biopsy are more important than sheer volume.
- B. Excisional biopsy is more painful and requires general anesthesia: While excisional biopsy is a more invasive procedure and often requires more robust anesthesia, this is not the primary oncologic reason for avoiding it.
- D. Core needle biopsy offers real-time pathological diagnosis during the procedure: Real-time diagnosis (frozen section) can be performed with either biopsy type, but it's not a unique advantage of core needle biopsy. Definitive diagnosis often requires permanent sections and ancillary studies.
- E. Excisional biopsy has a higher risk of infection compared to core needle biopsy: While any surgical procedure carries infection risk, the difference in infection rates between the two, while present, is not the main oncologic driver for the preference.
The strategic placement of a core needle biopsy tract, along the axis of the planned definitive incision, is crucial for minimizing the impact on future surgical fields.
Question 33
A 15-year-old boy presents with progressive knee pain. Radiographs reveal a mixed lytic and sclerotic lesion in the distal femur metaphysis with a 'sunburst' periosteal reaction. Core needle biopsy confirms high-grade, intramedullary osteosarcoma without evidence of metastasis. What is the most appropriate management strategy?
Explanation
Question 34
A 28-year-old male is involved in a high-speed motor vehicle collision and sustains a displaced Pauwels type III femoral neck fracture and an ipsilateral comminuted midshaft femur fracture. He is hemodynamically stable. What is the most appropriate sequence and strategy for operative fixation?
Explanation
Question 35
A 22-year-old collegiate football player presents with midfoot pain after a severe axial load was applied to his plantarflexed foot. Non-weight-bearing radiographs appear largely unremarkable, but he has severe pain with passive pronation of the forefoot. What is the most appropriate next step in imaging to evaluate for a subtle Lisfranc injury?
Explanation
Question 36
A 12-year-old girl presents with a destructive diaphyseal lesion in her fibula with an 'onion-skin' periosteal reaction. A biopsy is performed, and molecular studies are requested. Which of the following chromosomal translocations is diagnostic for this patient's most likely condition?
Explanation
Question 37
A 45-year-old male sustains a severe closed Schatzker VI tibial plateau fracture. On presentation, the leg is significantly swollen with hemorrhagic fracture blisters over the proximal lateral tibia. What is the most appropriate initial management?
Explanation
Question 38
A 55-year-old male with poorly controlled type 2 diabetes presents with a unilaterally swollen, red, and warm left foot. He denies trauma. Pedal pulses are bounding, and he has profound peripheral neuropathy. Radiographs reveal fragmentation and subluxation at the tarsometatarsal joints without soft tissue gas. What is the most appropriate initial management?
Explanation
Question 39
A 60-year-old male presents with deep groin pain. Radiographs reveal a large destructive lesion in the right ilium with stippled 'popcorn' calcifications extending into the soft tissues. Biopsy confirms a grade II (intermediate grade) conventional chondrosarcoma. What is the recommended definitive treatment?
Explanation
Question 40
A 35-year-old male is brought to the trauma bay in hemorrhagic shock after a motorcycle accident. Pelvic radiographs show a severely displaced anteroposterior compression type III (APC-III) pelvic ring injury. The trauma team decides to apply a non-invasive commercial pelvic binder. To be maximally effective in reducing pelvic volume, where must the binder be centered?
Explanation
Question 41
A 38-year-old male undergoes open repair of an acute Achilles tendon rupture using a posteromedial approach. During the dissection, the surgeon must be cautious to protect the sural nerve. What is the classic anatomic course of the sural nerve relative to the Achilles tendon?
Explanation
Question 42
A 68-year-old female presents with persistent back pain and generalized fatigue. Laboratory tests show hypercalcemia and mild anemia. Radiographs demonstrate multiple 'punched-out' lytic lesions in her skull and pelvis. Which of the following laboratory tests is the most sensitive initial screening tool for her most likely diagnosis?
Explanation
Question 43
A 30-year-old male sustains a closed tibia shaft fracture. Overnight, he develops excruciating leg pain requiring escalating doses of narcotics. Passive stretch of his toes reproduces severe pain. Which of the following formulas correctly defines the 'delta P' used to diagnose acute compartment syndrome, and what threshold warrants emergent fasciotomy?
Explanation
Question 44
A 26-year-old female sustains a Hawkins Type III talar neck fracture following a fall from height. Which of the following best describes the disruption of the blood supply and the associated risk of avascular necrosis (AVN) of the talar body?
Explanation
Question 45
A 32-year-old female presents with knee pain. Radiographs reveal an eccentric, expansile, lytic lesion in the epiphysis of her distal femur extending to the subchondral bone. Biopsy confirms a giant cell tumor of bone. For massive or unresectable giant cell tumors, which targeted pharmacologic therapy has shown significant efficacy in arresting tumor progression?
Explanation
Question 46
A 40-year-old farmer sustains a Gustilo-Anderson Type IIIA open tibia fracture from a tractor power take-off injury. The wound is grossly contaminated with soil and manure. In addition to a first-generation cephalosporin and an aminoglycoside, what additional prophylactic antibiotic must be initiated in the emergency department?
Explanation
Question 47
A 42-year-old roofer falls 15 feet and sustains a displaced intra-articular calcaneus fracture (Sanders Type III). During operative reconstruction via an extensile lateral approach, the surgeon must reduce the tuberosity to the 'constant fragment'. Which anatomic structure defines the constant fragment in a calcaneus fracture?
Explanation
Question 48
A 19-year-old male complains of severe, progressively worsening mid-thigh pain that awakens him at night but is dramatically relieved by ibuprofen. A CT scan reveals a 1 cm radiolucent nidus surrounded by dense reactive sclerosis in the femoral diaphysis. What is the most appropriate, minimally invasive definitive treatment?
Explanation
Question 49
A 25-year-old male unrestrained passenger is involved in a head-on motor vehicle collision. His knees strike the dashboard. In the emergency department, his right leg is severely painful and completely immobile. Which of the following postures is classic for an unreduced posterior hip dislocation?
Explanation
Question 50
A 52-year-old female presents with a progressive flatfoot deformity. On exam, she has a positive 'too many toes' sign and is entirely unable to perform a single-leg heel rise on the affected side. She has pain along the medial ankle. Dysfunction of which of the following tendons is the primary etiology of this condition?
Explanation
Question 51
A 62-year-old female with a history of breast cancer presents with increasing right thigh pain. Radiographs demonstrate a large, lytic lesion in the subtrochanteric region of the femur causing a 60% loss of cortical diameter. Her Mirels score is calculated at 10. What is the most appropriate management?
Explanation
Question 52
A 15-year-old boy presents with progressive knee pain. Radiographs reveal a destructive metaphyseal lesion in the distal femur with a "sunburst" periosteal reaction. Biopsy confirms high-grade intramedullary osteosarcoma. What is the most appropriate treatment sequence?
Explanation
Question 53
A 24-year-old male presents with a displaced femoral neck fracture (Pauwels type III). What is the primary biomechanical advantage of using a dynamic hip screw (DHS) with a derotational screw compared to three parallel cannulated screws for this injury?
Explanation
Question 54
A 12-year-old boy presents with progressive distal thigh pain. Radiographs demonstrate a permeative diaphyseal lesion with a lamellated periosteal reaction.
Biopsy reveals sheets of small round blue cells. Which of the following translocations is most characteristic of this diagnosis?
Explanation
Question 55
A 22-year-old collegiate football player sustains an axial load to a plantarflexed foot. Weight-bearing radiographs reveal widening of the interval between the first and second metatarsal bases. The primary ligament disrupted in this injury originates from and inserts into which of the following structures?
Explanation
Question 56
A 45-year-old male sustains a high-energy Schatzker IV tibial plateau fracture (medial plateau). An MRI is obtained to evaluate soft tissue injuries. Which of the following ligamentous structures is most commonly injured in association with this specific fracture pattern?
Explanation
Question 57
A 32-year-old female presents with knee pain. Radiographs show an eccentric, lytic epiphyseal lesion in the distal femur without a sclerotic rim. Biopsy confirms a Giant Cell Tumor of bone. If medical therapy is considered, denosumab acts by directly inhibiting which of the following?
Explanation
Question 58
A 58-year-old female presents with a progressive, flexible flatfoot deformity and inability to perform a single-leg heel rise. Examination reveals a 'too many toes' sign and tenderness over the medial ankle. Which of the following surgical interventions is most appropriate for a Stage IIb posterior tibial tendon dysfunction?
Explanation
Question 59
A 35-year-old male presents with a hypotensive (BP 75/40 mmHg) pelvic ring injury after a crush injury. The FAST exam is negative. A pelvic binder is applied, but he remains persistently hypotensive (BP 80/45 mmHg) after 2 liters of crystalloid. The institution lacks immediate interventional radiology capabilities. What is the most appropriate next step in management?
Explanation
Question 60
A 40-year-old laborer sustains a purely ligamentous Lisfranc injury with 3 mm of diastasis between the medial and middle cuneiforms. Based on current high-level evidence, what is the primary advantage of primary arthrodesis over open reduction and internal fixation (ORIF) for this specific injury pattern?
Explanation
Question 61
A 55-year-old male presents with deep, aching thigh pain. Radiographs reveal a lytic lesion with 'popcorn' calcifications in the proximal femur. Biopsy reveals atypical chondrocytes in a hyaline cartilage matrix with permeation into the surrounding marrow spaces. What is the most appropriate definitive treatment?
Explanation
Question 62
A 30-year-old male falls from a height. Radiographs
demonstrate a comminuted intra-articular distal femur fracture. CT scan reveals an associated coronal plane fracture of the lateral femoral condyle. What surgical approach provides the most direct and extensile access for anatomic reduction and fixation of this specific articular fragment?
Explanation
Question 63
A 45-year-old male sustains an acute Achilles tendon rupture. He is counseled on nonoperative versus operative management. Based on current high-level evidence, which of the following is true regarding nonoperative management with early functional rehabilitation compared to operative repair?
Explanation
Question 64
A 14-year-old boy presents with progressive knee pain and swelling. Imaging
reveals a permeative diaphyseal lesion with an 'onion skin' periosteal reaction. Biopsy reveals sheets of uniform small round blue cells. Cytogenetic analysis is pending. Which of the following chromosomal translocations is most pathognomonic for this suspected diagnosis?
Explanation
Question 65
During open reduction and internal fixation of a high-energy tibial plateau fracture with a posteromedial fragment, the surgeon decides to use a direct posteromedial approach. To safely expose the bone, the deep dissection utilizes an internervous plane between which of the following two structures?
Explanation
Question 66
A 62-year-old female with known metastatic breast cancer presents with severe back pain and myelopathic symptoms. Imaging reveals a lytic metastasis in the T8 vertebral body causing high-grade epidural spinal cord compression (ESCC). Her neurologic exam demonstrates 4/5 strength in the bilateral lower extremities with hyperreflexia. According to the NOMS framework, what is the most appropriate management?
Explanation
None
