ABOS Orthopedic Board Review: Bone Neoplasms, Chondromas, & Sarcoma Metastasis | Part 9
Key Takeaway
This ABOS board review focuses on orthopedic oncology, covering primary bone neoplasms, their incidence, malignancy, clinical features, and metastatic pathways. It also details benign cartilaginous lesions like periosteal chondromas and enchondromas, including Ollier's disease. This resource helps master complex musculoskeletal tumor concepts for board preparation.
ABOS Orthopedic Board Review: Bone Neoplasms, Chondromas, & Sarcoma Metastasis | Part 9
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 45-year-old female presents with persistent, deep right shoulder pain. Radiographs reveal a 5 cm radiolucent lesion with stippled calcifications in the proximal humerus. MRI shows endosteal scalloping involving 80% of the cortical thickness. What is the most likely diagnosis?
Explanation
Question 2
A 22-year-old man presents with a painless lump on his proximal humerus. Radiographs show a surface lesion with underlying cortical saucerization and a sclerotic margin.
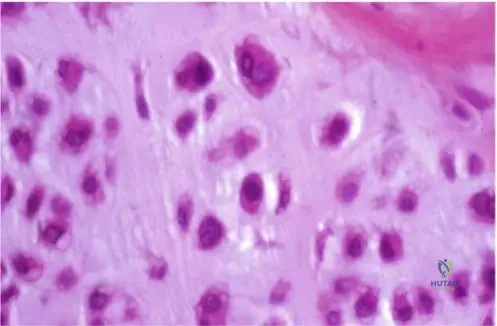
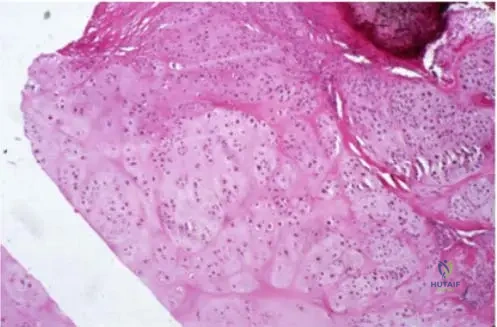
Histology shows lobules of hyaline cartilage. What is the most appropriate management?
Explanation
Question 3
A 30-year-old mechanic sustains a closed fracture of the proximal phalanx of the index finger after a minor trauma. Radiographs reveal a central, lytic lesion with thin cortices and a non-displaced pathologic fracture.
What is the recommended treatment plan?
Explanation
Question 4
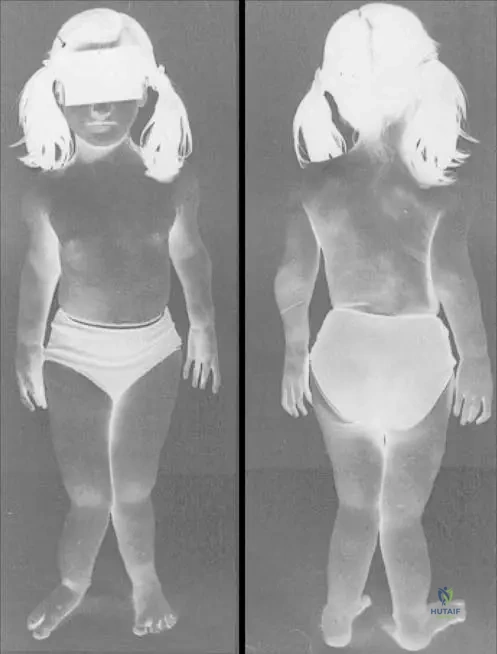
A 15-year-old female presents with multiple asymmetrical bone deformities and several soft-tissue hemangiomas with phleboliths. Which of the following gene mutations is most strongly associated with this patient's underlying condition?
Explanation
Question 5
A 16-year-old male is diagnosed with an osteoblastic osteosarcoma of the distal femur. What is the most sensitive imaging modality for detecting 'skip metastases' within the same bone?
Explanation
Question 6
A 40-year-old male presents with hip pain. Radiographs demonstrate a lytic lesion in the proximal femoral epiphysis. Biopsy reveals abundant cells with distinct borders, clear cytoplasm, and central nuclei scattered among hyaline cartilage. What is the most appropriate treatment?
Explanation
Question 7
A 35-year-old female presents with a painless, palpable mass on her right index finger. Radiographs reveal a centrally located lytic lesion with stippled calcifications and mild cortical expansion in the proximal phalanx.
What is the most likely diagnosis?
Explanation
Question 8
A 24-year-old male presents with localized, dull ache over his proximal humerus. Imaging demonstrates a surface-based lesion with a sclerotic margin and 'saucerization' of the underlying outer cortex, with no medullary extension.
What is the most likely diagnosis?
Explanation
Question 9
A 16-year-old boy who underwent wide resection and chemotherapy for distal femoral osteosarcoma 2 years ago now presents with two new, isolated 1.5 cm nodules in the right lung base. Staging shows no other sites of disease. What is the standard of care for these lesions?
Explanation
Question 10
A 12-year-old girl is evaluated for multiple bony deformities. Radiographs reveal numerous enchondromas throughout the appendicular skeleton. Physical examination shows multiple bluish, soft-tissue masses on her limbs consistent with hemangiomas. Which syndrome does this patient have?
Explanation
Question 11
Recent genomic profiling has identified specific somatic mutations that are highly prevalent in solitary enchondromas, central chondrosarcomas, and syndromic enchondromatosis. Which of the following mutations is most characteristically involved?
Explanation
Question 12
A 55-year-old male presents with deep, progressive shoulder pain. Radiographs show a cartilaginous lesion in the proximal humerus. Which of the following MRI findings most strongly supports a diagnosis of high-grade chondrosarcoma over a benign enchondroma?
Explanation
Question 13
A 15-year-old male complains of chronic knee pain. Radiographs reveal an eccentric, lytic lesion in the distal femoral epiphysis that crosses an open physis. Histology shows polygonal cells with grooved nuclei and fine, pericellular calcifications. What is the diagnosis?
Explanation
Question 14
A 22-year-old male presents with a localized, painful swelling on the distal humerus. Imaging confirms a surface cartilaginous lesion.
Biopsy confirms a benign hyaline cartilage tumor. What is the most appropriate management?

Explanation
Question 15
A 40-year-old male presents with a lytic lesion in the proximal femoral epiphysis. Biopsy reveals cells with abundant clear cytoplasm and distinct boundaries in a background of hyaline cartilage and reactive bone. What is the recommended treatment for this lesion?
Explanation
Question 16
A 30-year-old male is diagnosed with synovial sarcoma of the distal thigh. Following wide local excision, he is monitored for distant metastasis. What is the most common site of metastasis for this tumor?
Explanation
Question 17
Which histologic feature is the hallmark of dedifferentiated chondrosarcoma?
Explanation
Question 18
A 20-year-old female presents with an eccentric, multiloculated, lytic lesion with a sclerotic rim in the proximal tibial metaphysis. Biopsy shows stellate and spindle cells in a myxoid background with scattered osteoclast-like giant cells. What is the most likely diagnosis?
Explanation
Question 19
A 30-year-old patient presents with acute finger pain after minor trauma. Imaging shows a pathologic fracture through a central, lytic lesion with faint calcification.
What is the most appropriate initial management?
Explanation
Question 20
A 14-year-old girl is diagnosed with a conventional high-grade intramedullary osteosarcoma of the distal femur. What is the standard neoadjuvant chemotherapy regimen utilized to improve survival and prevent metastasis?
Explanation
Question 21
A 10-year-old boy presents with a permeative lesion in the femoral diaphysis and an 'onion-skin' periosteal reaction. Molecular testing of the biopsy specimen is most likely to reveal which of the following chromosomal translocations?
Explanation
Question 22
Mesenchymal chondrosarcoma is a rare, aggressive bone tumor. Which of the following characteristics is true regarding its clinical behavior?
Explanation
Question 23
A 60-year-old man had a wide local excision and radiation for a high-grade undifferentiated pleomorphic sarcoma of the thigh 18 months ago. Routine surveillance CT reveals an isolated 2 cm metastasis in the left lower pulmonary lobe. What is the most appropriate treatment recommendation?
Explanation
Question 24
A 26-year-old woman is evaluated for a localized mass on the surface of her proximal tibia. Radiographs reveal saucerization of the underlying cortex and a sclerotic margin.
Which radiographic feature best differentiates this lesion from a periosteal osteosarcoma?
Explanation
Question 25
A 45-year-old asymptomatic woman undergoes knee radiography for mild osteoarthritis. An incidental 3-cm lobulated, calcified metaphyseal lesion is found in the distal femur. MRI demonstrates lobular hyperintensity on T2-weighted images without cortical breakthrough or soft tissue extension. Which genetic mutation is most commonly associated with this specific tumor's pathogenesis?
Explanation
Question 26
A 16-year-old boy presents with a painless lump on his proximal humerus. Radiographs reveal a surface lesion causing 'saucerization' of the underlying cortex with a well-defined sclerotic margin and stippled calcifications.
What is the most appropriate initial management for this lesion if it remains asymptomatic?
Explanation
Question 27
A 30-year-old male with Maffucci syndrome presents with increasing pain in his distal femur. Radiographs show a previously calcified enchondroma that now exhibits cortical destruction and a soft-tissue mass. Which of the following systemic malignancies is this patient at highest risk for compared to a patient with Ollier disease?
Explanation
Question 28
A 14-year-old girl is diagnosed with high-grade conventional osteosarcoma of the distal femur. She completes neoadjuvant chemotherapy and undergoes surgical resection. Pathological analysis of the resected specimen reveals 95% tumor necrosis. What is the most significant clinical implication of this finding?
Explanation
Question 29
A 22-year-old man presents with acute pain and swelling in his index finger after a minor fall. Radiographs demonstrate a pathologic fracture through a central, lytic, expansile lesion with stippled calcification in the proximal phalanx.
What is the recommended management?
Explanation
Question 30
Which of the following radiographic features best differentiates a low-grade chondrosarcoma from a benign enchondroma in a long bone?
Explanation
Question 31
A 17-year-old male with classic Ewing sarcoma of the diaphyseal femur undergoes initial staging. Which of the following sites is the most common location for metastasis in this disease, and what specific staging test is uniquely mandatory compared to osteosarcoma?
Explanation
Question 32
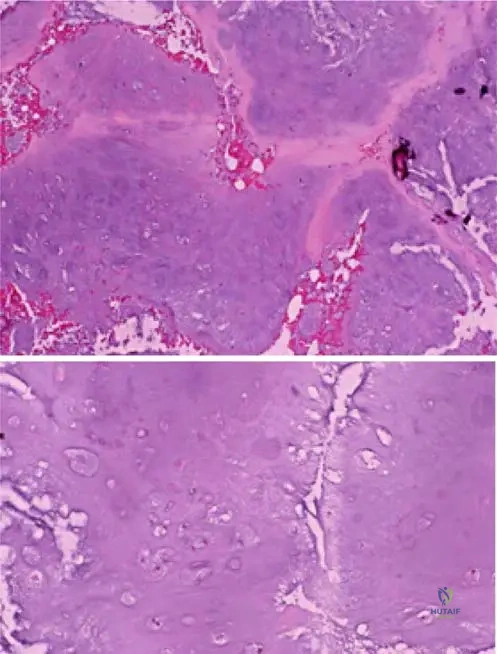
A 65-year-old male with a long-standing, stable calcified lesion in his proximal humerus presents with sudden, rapidly progressive pain and a palpable soft tissue mass. Biopsy reveals a biphasic tumor with regions of low-grade hyaline cartilage adjacent to a high-grade undifferentiated spindle cell sarcoma. What is the diagnosis?
Explanation
Question 33
A 40-year-old female presents with shoulder pain. Radiographs reveal a purely lytic lesion confined to the epiphysis of the proximal humerus. Histology demonstrates cells with abundant clear cytoplasm, distinct borders, and scattered multinucleated giant cells within a cartilaginous background. What is the most likely diagnosis?
Explanation
Question 34
During the surgical planning for a patient with high-grade osteosarcoma of the distal femur, an MRI of the entire femur is obtained. The primary purpose of imaging the entire bone is to evaluate for which of the following?
Explanation
Question 35
A 21-year-old patient who underwent distal femoral replacement for osteosarcoma 2 years ago presents for follow-up. A routine chest CT shows a solitary 1.5 cm peripheral nodule in the right lower lobe. The primary tumor site is free of recurrence, and no other lesions are noted. What is the most appropriate next step in management?
Explanation
Question 36
A 35-year-old male undergoes a radiograph for knee pain. A surface lesion is noted on the distal femur. Biopsy reveals intermediate-grade malignant cells producing a predominantly cartilaginous matrix with some osteoid, situated on the cortical surface without medullary involvement. The radiographic appearance shows a 'sunburst' periosteal reaction. What is the diagnosis?
Explanation
Question 37
A 50-year-old male presents with a destructive bone lesion in the pelvis. A biopsy is planned. Before performing a biopsy on a suspected metastatic lesion of unknown primary origin, what is the most critical initial diagnostic step?
Explanation
Question 38
An MRI of the knee in a 40-year-old woman shows a medullary lesion in the distal femur. The radiologist notes a 'double-line sign' on T2-weighted images and a serpiginous border, distinguishing it from an enchondroma. What is the most likely diagnosis?
Explanation
Question 39
A 28-year-old man presents with a small, palpable mass on his proximal tibia. Radiographs show a well-circumscribed, saucer-like cortical depression with a sclerotic rim.
Histology shows benign hyaline cartilage. Which characteristic best differentiates this from an osteochondroma?
Explanation
Question 40
A 30-year-old woman presents with jaw pain. Imaging reveals a destructive lesion in the mandible. Histology displays a biphasic pattern with islands of well-differentiated hyaline cartilage surrounded by sheets of small, undifferentiated round blue cells in a hemangiopericytoma-like vascular pattern. What is the diagnosis?
Explanation
Question 41
In a 15-year-old male with osteosarcoma of the proximal tibia, which of the following findings would upstage the patient to Stage III according to the Enneking Surgical Staging System?
Explanation
Question 42
Which of the following bone tumors characteristically expresses the t(11;22)(q24;q12) chromosomal translocation resulting in the EWS-FLI1 fusion protein?
Explanation
Question 43
A patient with multiple hereditary exostoses (MHE) is monitored for malignant transformation. Which clinical or radiographic sign is the most reliable indicator of secondary chondrosarcoma arising from an osteochondroma in an adult?
Explanation
Question 44
A 20-year-old male undergoes curettage of a lytic lesion in the proximal phalanx of the hand.
Pathological examination shows lobules of mature hyaline cartilage. Which of the following best describes the recurrence risk and malignant potential of this solitary hand lesion?
Explanation
Question 45
A 25-year-old female presents with multiple enchondromas and soft-tissue hemangiomas. Which genetic mutation is most strongly associated with her underlying syndrome?
Explanation
Question 46
A 16-year-old boy presents with a painless lump on his proximal humerus. Imaging demonstrates a surface lesion causing saucerization of the underlying cortex with a sclerotic margin and cartilaginous matrix.
What is the most appropriate management for a growing, symptomatic lesion of this type?
Explanation
Question 47
Which of the following radiographic features is the most reliable indicator differentiating a low-grade central chondrosarcoma from a benign enchondroma in a long bone?
Explanation
Question 48
A 14-year-old boy with conventional osteosarcoma of the distal femur completes neoadjuvant chemotherapy. Restaging scans show two new 1 cm peripheral lung nodules. His primary tumor is resectable. What is the most appropriate management?
Explanation
Question 49
A 35-year-old man sustains a closed, minimally displaced fracture through a lytic lesion in the proximal phalanx of his ring finger. Radiographs show a well-circumscribed, expansile lucency with stippled calcifications.
What is the most appropriate initial management?
Explanation
Question 50
A 28-year-old female presents with a solitary enchondroma of the distal femur discovered incidentally on an MRI for a knee sprain. Which of the following statements regarding solitary enchondromas is true?
Explanation
Question 51
In a patient with Ewing sarcoma, what is the most common site of metastasis at the time of initial presentation?
Explanation
Question 52
A 45-year-old man undergoes resection of a large pelvic mass. Histopathology reveals a biphasic tumor with islands of well-differentiated, low-grade hyaline cartilage adjacent to a high-grade, non-cartilaginous spindle cell sarcoma. What is the diagnosis?
Explanation
Question 53
A 22-year-old male with Ollier disease presents with worsening pain and a rapidly enlarging mass in his proximal tibia. Which of the following is the most likely secondary malignancy to develop in this patient?
Explanation
Question 54
An MRI of a patient with distal femoral osteosarcoma reveals a distinct, separate tumor focus within the proximal medullary canal of the same bone. What term best describes this finding, and how does it affect surgical planning?
Explanation
Question 55
A 19-year-old female presents with a small (< 2 cm), painless cartilaginous lesion on the surface of the proximal humerus cortex.
Histologically, it shows hypercellularity and binucleate cells. What clinical or radiographic feature distinguishes this periosteal chondroma from a periosteal chondrosarcoma?
Explanation
Question 56
Which of the following characteristics is most suggestive of clear cell chondrosarcoma?
Explanation
Question 57
A 60-year-old man presents with a painful lesion in the diaphysis of the femur. Biopsy reveals small blue round cells mixed with islands of benign-appearing cartilage and a hemangiopericytoma-like vascular pattern (staghorn vessels). What is the most likely diagnosis?
Explanation
Question 58
A 55-year-old woman is incidentally found to have a 3 cm enchondroma in her proximal humerus. Radiographs show classic rings and arcs calcification. She is completely asymptomatic. What is the most appropriate management?
Explanation
Question 59
Regarding survival in patients with osteosarcoma who develop pulmonary metastases, which factor is most strongly associated with improved long-term outcomes?
Explanation
Question 60
A 30-year-old male has an expansile lucent lesion in the proximal phalanx of the index finger.
A biopsy confirms enchondroma. During surgical treatment, what is the most important intraoperative step to minimize the risk of local recurrence?
Explanation
Question 61
What is the primary role of whole-lung irradiation in the treatment of Ewing sarcoma?
Explanation
Question 62
A 35-year-old male presents with a painless lump in his hand after a minor bump. Radiographs show a well-circumscribed, lytic lesion in the proximal phalanx with stippled calcifications.
What is the most appropriate management for a confirmed non-pathologic, asymptomatic enchondroma in this location?
Explanation
Question 63
A 22-year-old female presents with multiple asymmetrical cartilaginous lesions in her long bones and hands, associated with soft-tissue hemangiomas. Which of the following genetic mutations is most characteristic of her underlying syndrome?
Explanation
Question 64
A 24-year-old male presents with a mildly painful palpable mass on the proximal humerus. Radiographs reveal a surface lesion with cortical saucerization and a sclerotic periosteal reaction at the proximal and distal margins.
What is the most likely diagnosis?
Explanation
Question 65
In a 15-year-old male diagnosed with high-grade intramedullary osteosarcoma of the distal femur, what is the most significant prognostic factor for overall survival at the time of presentation?
Explanation
Question 66
A 45-year-old patient with a known distal femur enchondroma presents with new-onset, deep, dull aching pain at night. Radiographs show increased endosteal scalloping.
Which radiographic feature is most indicative of malignant transformation to a low-grade chondrosarcoma?
Explanation
Question 67
A 28-year-old female presents with a growing, tender mass on her anterior tibia. Biopsy confirms a periosteal chondroma. The lesion measures 2.5 cm. What is the recommended treatment?
Explanation
Question 68
A 17-year-old male with a history of distal femur osteosarcoma, treated with wide resection and chemotherapy two years ago, presents with a solitary 1.5 cm pulmonary metastasis. The primary site has no local recurrence. What is the most appropriate management?
Explanation
Question 69
A 40-year-old male complains of chronic hip pain. Radiographs reveal an epiphyseal lytic lesion in the proximal femur with a sclerotic margin and central calcifications. What is the most likely diagnosis, considering this distinct epiphyseal location in an adult?
Explanation
Question 70
A 12-year-old boy presents with multiple cartilaginous lesions in the hands and long bones, accompanied by distinct soft-tissue masses with phleboliths noted on radiographs. What is the most significant long-term risk associated with his underlying syndrome?
Explanation
Question 71
An asymptomatic 35-year-old woman has a hand radiograph taken after a minor sprain, revealing the lesion shown.
Recent molecular studies show that solitary lesions of this type are most strongly associated with somatic mutations in which of the following genes?
Explanation
Question 72
A 24-year-old male presents with a painless palpable mass on the proximal humerus. Radiographs show a surface-based radiolucent lesion with a well-defined sclerotic border and overhanging cortical edges. Which of the following radiographic features best differentiates this lesion from a juxtacortical (periosteal) chondrosarcoma?
Explanation
Question 73
A 15-year-old girl is undergoing post-treatment surveillance following wide resection and neoadjuvant chemotherapy for conventional osteosarcoma of the distal femur. What is the most common site of metastasis for this tumor and the primary imaging modality for surveillance?
Explanation
Question 74
A 55-year-old man undergoes a biopsy of a large destructive pelvic mass. Histopathology reveals Grade 2 conventional chondrosarcoma. Staging studies are negative for metastasis. What is the most appropriate primary treatment?
Explanation
Question 75
A 40-year-old man with Multiple Hereditary Exostoses presents with a newly enlarging mass on his right posterior distal femur. MRI reveals an exophytic bone lesion with an overlying hyperintense cartilaginous cap on T2-weighted images. What cartilage cap thickness is highly suspicious for secondary malignant transformation?
Explanation
Question 76
A 42-year-old woman presents with persistent hip pain. Radiographs demonstrate an expansile, lytic epiphyseal lesion in the proximal femur with sharp margins. Histologic evaluation shows cells with abundant clear cytoplasm and distinct cell membranes intermixed with areas of reactive bone formation. What is the most likely diagnosis?
Explanation
Question 77
A 14-year-old boy is diagnosed with Ewing sarcoma of the femoral diaphysis. Staging is performed. The presence of metastasis at diagnosis is the most significant negative prognostic factor. Which of the following are the two most common sites of metastasis for this disease?
Explanation
Question 78
A 65-year-old male presents with a pathologic fracture of the humerus through a purely lytic, highly destructive lesion. Staging reveals an unknown primary tumor. Before planning an open biopsy, standard practice requires a CT of the chest, abdomen, and pelvis. Which primary carcinoma is notorious for producing highly vascular lytic metastases that may require pre-operative embolization?
Explanation
Question 79
A 60-year-old woman presents with thigh pain. Radiographs show a centrally located lesion in the distal femur with rings and arcs of calcification, alongside a large, destructive, purely lytic unmineralized mass breaching the cortex. Biopsy confirms a bimorphic histologic pattern. What is this entity?
Explanation
Question 80
A 20-year-old male presents with chronic knee pain. Imaging reveals an eccentric, purely lytic lesion in the proximal tibial metaphysis with a well-demarcated sclerotic margin. Histology shows lobules of stellate and spindle-shaped cells in a myxoid background, with an increased concentration of cells at the periphery of the lobules. What is the diagnosis?
Explanation
Question 81
A 16-year-old female is diagnosed with osteosarcoma of the distal femur. A full-length MRI of the entire femur is ordered prior to finalizing surgical planning. What is the primary purpose of imaging the entire involved bone?
Explanation
Question 82
A 32-year-old female presents with a surface-based lesion on the posterior distal femur measuring 6 cm. It lacks a sunburst appearance or medullary involvement. Biopsy reveals Grade 2 cartilaginous tissue without malignant osteoid. How does the management of this periosteal chondrosarcoma differ from that of periosteal osteosarcoma?
Explanation
Question 83
A 48-year-old man presents with right shoulder pain worsened by overhead activity. Radiographs reveal an incidental 3 cm medullary lesion with stippled calcifications in the proximal humerus without cortical scalloping. A subacromial corticosteroid injection provides 100% relief of his shoulder pain. What is the next best step in management of the bone lesion?
Explanation
Question 84
A 35-year-old man undergoes knee arthroscopy for mechanical catching. The surgeon finds dozens of white, cartilaginous loose bodies of similar size within the joint space, and the synovium appears thickened. What is the estimated risk of malignant transformation of this condition?
Explanation
Question 85
Which of the following histologic factors correlates most strongly with long-term survival in a patient undergoing treatment for localized conventional osteosarcoma?
Explanation
Question 86
A 22-year-old patient presents with a painful mass on the proximal phalanx. Radiographs show a small saucerized surface lesion with a sclerotic margin.
Biopsy confirms a periosteal chondroma. The pain persists despite conservative measures. What is the definitive management?
Explanation
Question 87
A 10-year-old child presents with a permeative lesion in the diaphysis of the fibula with an 'onion-skin' periosteal reaction. A core needle biopsy demonstrates sheets of small round blue cells. Which chromosomal translocation is the diagnostic hallmark for the most likely tumor?
Explanation
Question 88
A 45-year-old woman is evaluated for a large, purely lytic sacral lesion. Biopsy shows large cells with abundant clear cytoplasm and distinct borders. Immunohistochemistry is strongly positive for cytokeratin and EMA. What is the most likely diagnosis?
Explanation
Question 89
A 50-year-old male is being treated for a low-grade central chondrosarcoma of the proximal femur. Which of the following imaging features on MRI is most characteristic of high-grade transformation or dedifferentiation within a pre-existing low-grade cartilage tumor?
Explanation
Question 90
A 15-year-old female presents with multiple hard bony swellings on her hands and bluish, compressible soft tissue nodules on her forearms. Which of the following describes the underlying genetic abnormality and the estimated lifetime risk of malignant transformation in this patient?
Explanation
Question 91
A 14-year-old boy completes neoadjuvant chemotherapy and wide resection for a distal femur osteosarcoma. Two years later, a surveillance chest CT reveals three new, unilateral peripheral lung nodules (largest 1.5 cm) with no other evidence of disease. What is the most appropriate next step in management?
Explanation
Question 92
A 35-year-old male presents with chronic hip pain. Radiographs reveal a lytic lesion in the femoral head epiphysis with a sclerotic margin and central calcification. Histology shows cells with abundant clear cytoplasm and distinct cell membranes interspersed with hyaline cartilage. What is the most appropriate definitive surgical treatment?
Explanation
Question 93
A 42-year-old woman undergoes radiographs for a knee sprain, revealing an incidental finding in the distal femur:
She denies thigh pain. MRI confirms a well-circumscribed, lobulated cartilaginous lesion without endosteal scalloping or cortical breakthrough. What is the next best step in management?
Explanation
Question 94
A 60-year-old man presents with severe proximal thigh pain. Radiographs show a large, purely osteolytic, expansile lesion in the proximal femur with an impending subtrochanteric fracture. Biopsy confirms metastatic clear cell renal carcinoma. Before proceeding with prophylactic cephalomedullary nailing, which of the following is highly recommended?
Explanation
Question 95
A 28-year-old man with Hereditary Multiple Exostoses (HME) reports a rapidly enlarging, painful mass on his posterior thigh. MRI reveals a sessile osteochondroma with a newly thickened cartilage cap measuring 3.5 cm. Which of the following histological features most strongly suggests malignant transformation to secondary chondrosarcoma?
Explanation
Question 96
A 19-year-old male presents with a hard, painless mass on his proximal humerus. Radiographs are shown:
Imaging confirms a surface lesion causing saucerization of the underlying cortex with a sclerotic rim, but no medullary extension. Biopsy shows mature hyaline cartilage without atypia. What is the most likely diagnosis?
Explanation
Question 97
A 65-year-old man sustains a pathologic fracture of the proximal humerus. Imaging shows a heavily calcified medullary lesion bordered by a highly aggressive, purely radiolucent area destroying the cortex. Histology reveals low-grade hyaline cartilage sharply juxtaposed next to a high-grade, non-cartilaginous spindle cell sarcoma. What is the diagnosis?
Explanation
Question 98
A 24-year-old female presents with a destructive rib lesion. Biopsy reveals a highly cellular tumor composed of sheets of primitive, undifferentiated small round blue cells interspersed with distinct islands of well-differentiated, benign-appearing hyaline cartilage. What is the most likely diagnosis?
Explanation
Question 99
A 45-year-old male has deep thigh pain at night. Imaging shows a 6 cm cartilaginous lesion in the femoral diaphysis with focal endosteal scalloping involving 75% of the cortex. Core biopsy returns 'Atypical Cartilaginous Tumor / Grade 1 Chondrosarcoma'. What is the most appropriate joint-preserving surgical approach for this lesion?
Explanation
Question 100
A 12-year-old boy is diagnosed with Ewing sarcoma of the left ilium. During the initial staging workup, which of the following represents the single most significant prognostic factor for his overall survival?
Explanation
None
