ABOS Part I Orthopedic Surgery Review: Spine, Shoulder, Infections & Tumors | Part 22223
Key Takeaway
This ABOS Part I Comprehensive Review covers essential orthopedic topics including lumbar spinal stenosis, spinal infections like epidural abscess, and various spinal tumors. It also delves into rotator cuff tear arthropathy and advanced shoulder arthroplasty techniques like RSA. Prepare for your board exams by mastering critical diagnoses, imaging, and surgical management strategies.
ABOS Part I Orthopedic Surgery Review: Spine, Shoulder, Infections & Tumors | Part 22223
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 72-year-old male presents with a 6-month history of bilateral lower extremity pain, numbness, and weakness that is consistently worse with prolonged standing and walking, and significantly relieved by sitting or leaning forward (the 'shopping cart sign'). Peripheral pulses are palpable and symmetric. Which of the following is the most definitive diagnostic characteristic of neurogenic claudication in this patient?
Explanation
Correct Answer: B
The most definitive characteristic distinguishing neurogenic claudication from vascular claudication is the relief of symptoms by squatting, sitting, or bending forward (flexion of the lumbar spine). This position increases the sagittal diameter of the spinal canal, reducing compression on the neural elements. Options A, D, and E are more typical of vascular claudication (fixed distance, bruits, worse with uphill walking due to increased calf muscle demand). Diminished peripheral pulses (Option C) are a sign of vascular disease, not neurogenic claudication.
Question 2
Which of the following physical examination findings is LEAST likely to be associated with typical degenerative lumbar spinal stenosis?
Explanation
Correct Answer: C
Lumbar spinal stenosis primarily affects the cauda equina nerve roots, which are part of the peripheral nervous system. Therefore, it causes lower motor neuron signs (e.g., weakness, hyporeflexia, atrophy). Widespread upper motor neuron signs like hyperreflexia, spasticity, and a positive Babinski sign are characteristic of spinal cord myelopathy (which occurs above the conus medullaris, typically T12-L1 in adults) or brain lesions, and are NOT expected in isolated lumbar spinal stenosis. Options A, B, D, and E are all consistent with lumbar spinal stenosis (extension aggravates, normal ABI rules out vascular claudication, LMN signs are expected).
Question 3
A 65-year-old patient presents with classic symptoms of neurogenic claudication. What is the most appropriate initial imaging study to confirm the diagnosis and assess the severity of lumbar spinal stenosis?
Explanation
Correct Answer: C
MRI of the lumbar spine is the gold standard imaging study for diagnosing lumbar spinal stenosis. It provides excellent visualization of soft tissues, including the neural elements, ligamentum flavum, disc bulges, and allows for accurate assessment of the spinal canal and neural foramina narrowing. Plain radiographs (Option A) can show degenerative changes but not soft tissue compression. CT (Option B) is good for bone but inferior to MRI for neural structures unless MRI is contraindicated. EMG/NCS (Option D) and epidural injections (Option E) are diagnostic/therapeutic adjuncts, not primary imaging modalities for initial diagnosis.
Question 4
When differentiating neurogenic claudication from vascular claudication, which of the following statements is most accurate?
Explanation
Correct Answer: B
Neurogenic claudication pain is characteristically exacerbated by lumbar extension (standing still or walking upright) and relieved by lumbar flexion (sitting, bending forward, leaning over a shopping cart). Vascular claudication is relieved by rest (not necessarily flexion) and exacerbated by activity. Absent pedal pulses (Option C) are a sign of vascular claudication. Option D is incorrect as both can vary. Option E is incorrect; walking uphill typically reduces lumbar lordosis, which can be more tolerable for neurogenic claudication, while downhill walking (extension) is often worse.
Question 5
A 68-year-old female has mild to moderate lumbar spinal stenosis with neurogenic claudication symptoms. She has no significant neurological deficits. Which of the following conservative treatments has the strongest evidence base for initial management?
Explanation
Correct Answer: C
Structured physical therapy, particularly focusing on core strengthening, flexibility, and flexion-based exercises, has the strongest evidence for initial conservative management of lumbar spinal stenosis. It aims to improve spinal mechanics, reduce pain, and improve walking tolerance. Opioids (Option A) are not recommended for long-term management due to dependency risks. Bed rest (Option B) is generally detrimental. While epidural steroid injections (Option D) can provide short-term relief, indefinite, frequent injections are not recommended due to potential side effects and diminishing returns. TENS (Option E) may offer symptomatic relief but is typically used as an adjunct, not as a standalone primary treatment.
Question 6
What is the primary indication for surgical intervention in patients with lumbar spinal stenosis?
Explanation
Correct Answer: B
The primary indication for surgical intervention in lumbar spinal stenosis is the failure of extensive conservative management (typically 3-6 months) to relieve debilitating symptoms that significantly impair a patient's quality of life. Radiographic stenosis alone (Option A) is not an indication. Patient request (Option C) without conservative trials is generally not appropriate. Mild symptoms (Option D) usually respond to conservative care. Disc degeneration (Option E) is a common finding but not an indication for surgery unless it contributes to instability or stenosis causing symptoms.
Question 7
Regarding lumbar laminectomy for spinal stenosis, what is the primary goal of the decompression?
Explanation
Correct Answer: C
The primary goal of a lumbar laminectomy for spinal stenosis is direct decompression of the neural elements (cauda equina nerve roots). This involves removing hypertrophied ligamentum flavum, osteophytes, and sometimes portions of the lamina and facet joints to enlarge the spinal canal and neuroforamina, thereby alleviating compression. Stabilization (Option A), disc removal (Option B, though sometimes done concurrently for associated disc herniation, it's not the primary goal of laminectomy itself for stenosis), deformity correction (Option D), and preventing degeneration (Option E) are not the main objectives of a standalone decompression.
Question 8
In which of the following scenarios is adjunctive spinal fusion most strongly indicated alongside decompression for lumbar spinal stenosis?
Explanation
Correct Answer: D
Adjunctive fusion is most strongly indicated when there is significant preoperative instability or when decompression itself is likely to destabilize the segment. A concurrent degenerative spondylolisthesis (Grade I or II) with clinical instability (e.g., dynamic pain, progressive slip) or radiographic instability (increased translation or angulation on dynamic X-rays) is a common indication for fusion alongside decompression. Options A and B are typically treated with decompression alone. Multilevel stenosis (Option C) does not automatically require fusion unless instability is present. Prior microdiscectomy (Option E) doesn't inherently indicate fusion for stenosis unless instability or significant facetectomy is required for decompression.
Question 9
Which of the following is the most common immediate complication following lumbar decompression for spinal stenosis?
Explanation
Correct Answer: C
Incidental durotomy (dural tear) is the most common immediate complication during or after lumbar decompression surgery, with reported rates ranging from 3% to 17%. While other complications listed can occur, dural tears are particularly frequent due to the close proximity of the dura to the compressed structures being removed (e.g., hypertrophied ligamentum flavum, osteophytes). DVT/PE (Options A, D) are less common with appropriate prophylaxis. Surgical site infection (Option B) is a serious but less frequent immediate complication. New-onset foot drop (Option E) could occur due to nerve root injury, but dural tear is generally more common.
Question 10
A patient presents with sudden onset of bilateral leg weakness, saddle anesthesia, and acute urinary retention. This constellation of symptoms most strongly suggests which of the following?
Explanation
Correct Answer: D
The triad of bilateral lower extremity weakness, saddle anesthesia (sensory loss in the perineum, buttocks, and inner thighs), and urinary retention (or incontinence) is the classic presentation of Cauda Equina Syndrome (CES). CES is a surgical emergency requiring urgent decompression. Options A, B, C, and E do not typically present with this specific combination of severe, acute neurological deficits affecting bowel and bladder function.
Question 11
A 65-year-old diabetic male presents with insidious onset of back pain, low-grade fever, and progressive bilateral leg weakness over 2 weeks. On examination, he has a T10 sensory level and 3/5 motor strength in both lower extremities. Initial plain radiographs of the thoracic spine are unremarkable. Which of the following is the most appropriate initial diagnostic step?
Explanation
Correct Answer: D
MRI with gadolinium is the gold standard for diagnosing spinal epidural abscess (SEA), demonstrating the collection, degree of spinal cord compression, and identifying associated osteomyelitis or discitis. Given the progressive neurological deficit and suspicion of infection, urgent definitive imaging is crucial. Plain radiographs are insensitive in early disease. CT myelogram is less sensitive for soft tissue detail than MRI and involves radiation and contrast injection into the CSF. Lumbar puncture is generally contraindicated in suspected SEA due to the risk of neurological deterioration or meningitis. EMG is for peripheral nerve pathology. Corticosteroids are contraindicated before definitive diagnosis and debridement in bacterial infections.
Question 12
A patient undergoing hemodialysis develops severe cervical spine pain, fevers, and rapidly progressive quadriparesis. Blood cultures are pending. Given the patient's history, which organism is most likely responsible for a presumed spinal epidural abscess?
Explanation
Correct Answer: C
Staphylococcus aureus is the most common pathogen responsible for spinal epidural abscesses (SEA), accounting for 60-90% of cases. Methicillin-resistant S. aureus (MRSA) is particularly prevalent in patients with healthcare-associated risk factors such as hemodialysis, IV drug use, recent surgery, or indwelling catheters. While E. coli and Pseudomonas can occur, and Candida in immunocompromised hosts, S. aureus remains the dominant pathogen, especially in the context of healthcare exposure. Mycobacterium tuberculosis typically presents with a more chronic course.
Question 13
A 70-year-old male with a known C6-C7 spinal epidural abscess presents with acute urinary retention and rapidly progressive weakness in his lower extremities (motor strength 2/5). He has been on intravenous antibiotics for 48 hours without clinical improvement. What is the most appropriate next step?
Explanation
Correct Answer: B
Urgent surgical decompression is indicated for spinal epidural abscesses with progressive neurological deficits (such as new-onset urinary retention, rapidly worsening weakness) or failure of appropriate medical management to prevent irreversible neurological damage. Continuing antibiotics alone is insufficient. Adding rifampin may be part of an antibiotic strategy but does not address acute mechanical compression. Percutaneous aspiration may be considered for diagnosis or small, stable collections but not for acute, progressive deficits with neurological compromise. Steroids are generally contraindicated as they can mask symptoms, impair host immunity in bacterial infections, and are not a definitive treatment for pus collection.
Question 14
On MRI, a spinal epidural abscess typically appears as what on T2-weighted images?
Explanation
Correct Answer: C
Spinal epidural abscesses typically appear hyperintense on T2-weighted images due to the high fluid content of pus. They are often surrounded by a peripheral hypointense rim (representing granulation tissue or inflammatory changes) that shows significant enhancement after gadolinium administration. Homogenously hypointense or isointense to CSF are incorrect. Hyperintense without significant contrast enhancement would be atypical for an active abscess, which typically enhances due to inflammation and vascularity of the capsule.
Question 15
Which of the following conditions is LEAST likely to mimic a spinal epidural abscess on initial presentation, considering its typical clinical picture?
Explanation
Correct Answer: E
A spinal epidural abscess (SEA) commonly presents with back pain, fever, and neurological deficits. Acute disc herniation, spinal cord tumors, and transverse myelitis can all present with similar neurological deficits and pain, making them strong mimics. Guillain-Barré Syndrome (GBS) can cause rapidly ascending paralysis, mimicking severe neurological compromise, though fever, focal spinal pain, and a distinct sensory level are less typical for GBS, which presents with areflexia. A simple osteoporotic vertebral compression fracture, while causing back pain, typically does not present with fever or progressive neurological deficits unless there's associated cord compression from retropulsion or epidural hematoma, which would be atypical for the initial presentation of an uncomplicated osteoporotic fracture. Thus, a simple compression fracture is the least likely to mimic the full clinical picture of an SEA.
Question 16
What is the typical recommended duration of intravenous antibiotic therapy for an uncomplicated pyogenic spinal epidural abscess managed non-surgically, assuming cultures are positive for a sensitive organism?
Explanation
Correct Answer: C
For pyogenic spinal epidural abscesses (SEA), especially those managed non-surgically or those that have undergone successful debridement, a prolonged course of antibiotics is crucial to prevent recurrence and ensure eradication. A typical duration is 6-8 weeks of intravenous antibiotics, often followed by a transition to oral antibiotics for a similar duration, or sometimes 8-12 weeks total with IV transitioning to oral. The total duration depends on the pathogen, host factors, and resolution of inflammatory markers, but 6-8 weeks IV is a standard starting point for uncomplicated cases. 2-4 weeks is generally too short for eradication of established spinal infection, while 3-6 months is more typical for complicated osteomyelitis or prosthetic joint infections.
Question 17
A 45-year-old male presents with right flank pain, limping, and an inability to fully extend his right hip. He has a history of Crohn's disease. On examination, he has tenderness in the right iliac fossa and a positive psoas sign. What is the most appropriate imaging study to confirm the diagnosis and assess for a potential spinal origin?
Explanation
Correct Answer: C
While CT abdomen/pelvis with IV contrast is excellent for visualizing psoas abscesses, MRI of the lumbar spine and pelvis with contrast offers superior soft tissue resolution, allowing for better identification of the primary source (e.g., discitis, vertebral osteomyelitis), the extent of the abscess, and any intraspinal involvement. Given that psoas abscesses can often originate from spinal infections (or in Crohn's disease, directly from the bowel), MRI provides a more comprehensive assessment of both spinal and psoas pathology. The psoas sign is classic for psoas irritation/abscess.
Question 18
A patient from an endemic area presents with chronic back pain, night sweats, and weight loss. Imaging reveals destruction of multiple contiguous vertebral bodies with associated large paraspinal abscesses and severe kyphotic deformity. Which pathogen is most likely responsible?
Explanation
Correct Answer: C
This clinical presentation, including chronic symptoms, systemic signs (night sweats, weight loss), destruction of multiple contiguous vertebral bodies (often with relative disc sparing initially but progressing to disc and multiple levels), large paraspinal 'cold' abscesses, and progressive kyphotic deformity (Pott's kyphosis), is classic for spinal tuberculosis (Pott's disease). It is more common in endemic areas and immunocompromised individuals. The other pathogens typically cause pyogenic infections with a more acute course.
Question 19
A 50-year-old IV drug user presents with fever, severe T12 back pain, and new-onset paraparesis. Pending blood cultures and biopsy results, what is the most appropriate empiric intravenous antibiotic regimen?
Explanation
Correct Answer: A
In a patient with risk factors for both MRSA (IV drug user) and Gram-negative bacteria (potentially via hematogenous spread or urinary source), empiric broad-spectrum coverage is essential. Vancomycin provides excellent coverage against MRSA, while a third-generation cephalosporin like Ceftriaxone provides good coverage against Gram-negative organisms, making this a common and appropriate empiric combination. Ciprofloxacin and Rifampin would be used for specific organisms (e.g., Cipro for Pseudomonas, Rifampin in combo for S. aureus after susceptibility). Penicillin G is too narrow. Doxycycline/Metronidazole targets anaerobic and atypical bacteria. Fluconazole/Amphotericin B are for fungal infections.
Question 20
Which of the following criteria would NOT typically favor non-operative management of a spinal epidural abscess?
Explanation
Correct Answer: E
Progressive neurological deficit, especially despite appropriate antibiotic therapy, is a strong absolute indication for urgent surgical decompression of a spinal epidural abscess. This represents failure of medical management and an increasing threat of irreversible neurological damage. The other options (no or minimal neurological deficit, small abscess, responsive infection, and severe comorbidities precluding surgery) are factors that would favor an attempt at non-operative management with close monitoring.
Question 21
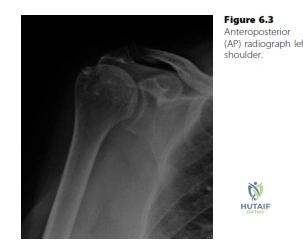
A 76-year-old left-handed fit gentleman presents with difficulties in overhead activities. An anteroposterior shoulder X-ray is obtained.
Which of the following findings is MOST indicative of rotator cuff arthropathy on this radiograph?
Explanation
Correct Answer: C
Proximal migration of the humeral head is the hallmark radiographic sign of rotator cuff tear arthropathy (RCAT). It indicates the loss of the superior stabilizing force of the rotator cuff, allowing the deltoid to pull the humeral head superiorly. This superior migration leads to abnormal articulation between the humeral head and the acromion, causing characteristic degenerative changes. While subacromial narrowing and sclerosis of the undersurface of the acromion (Option B) are often present due to impingement and chronic cuff pathology, they are not as specific for established arthropathy as proximal migration. Normal glenohumeral joint space (Option A) and absence of AC joint arthritis (Option D) are findings that rule out other pathologies but do not specifically point to RCAT. Osteophytes on the humeral head (Option E) are more characteristic of primary glenohumeral osteoarthritis, which typically presents with concentric joint space narrowing, rather than the superior erosion seen in RCAT.
Question 22
A 76-year-old left-handed fit gentleman presents with difficulties in overhead activities. The anteroposterior shoulder X-ray shows proximal migration of the humeral head and narrowing of the subacromial space. An ultrasound reveals torn subscapularis and supraspinatus with massive retraction. Given these findings, what is the MOST appropriate initial diagnosis?
Explanation
Correct Answer: C
The combination of proximal humeral migration on X-ray, massive rotator cuff tears (subscapularis and supraspinatus) with retraction on ultrasound, and difficulties with overhead activities in a 76-year-old gentleman strongly points to Rotator Cuff Tear Arthropathy (RCAT). RCAT is a specific form of degenerative arthritis characterized by superior migration of the humeral head due to a massive, irreparable rotator cuff tear, leading to erosion of the glenoid and humeral head. Primary glenohumeral osteoarthritis (Option A) typically involves concentric joint space narrowing and osteophyte formation, without significant proximal migration. Calcific tendinitis (Option B) is a distinct entity involving calcium deposits within tendons. Adhesive capsulitis (Option D) presents with global loss of range of motion, often without significant radiographic changes or massive cuff tears. While subacromial impingement syndrome (Option E) is often a precursor, the presence of massive tears and proximal migration indicates a more advanced stage, specifically RCAT.
Question 23
Following the initial AP shoulder X-ray showing proximal humeral migration and subacromial narrowing, the candidate requests an axillary view. What specific finding is the candidate MOST likely looking for on the axillary view in this clinical context?
Explanation
Correct Answer: C
In the context of suspected rotator cuff tear arthropathy (RCAT) with proximal migration seen on the AP view, an axillary view is crucial to assess for anteroposterior stability and subluxation of the humeral head relative to the glenoid. Specifically, anterior subluxation of the humeral head is a common finding in RCAT, often associated with a deficient subscapularis tendon, as noted by the second candidate in the case. Glenohumeral joint space narrowing (Option A) is better assessed on the AP view for superior migration, and while it can be seen, subluxation is more specific to cuff deficiency. AC joint osteophytes (Option B) are relevant for AC joint pathology, not directly for RCAT diagnosis. A Hill-Sachs lesion (Option D) is associated with anterior shoulder instability (dislocation), not typically RCAT. Scapular notching (Option E) is a complication seen after reverse shoulder arthroplasty, not a diagnostic feature on pre-operative plain radiographs for RCAT.
Question 24
The 76-year-old gentleman is diagnosed with rotator cuff tear arthropathy. Which of the following is the primary pathophysiological mechanism leading to the characteristic radiographic findings and symptoms in RCAT?
Explanation
Correct Answer: C
The primary pathophysiology of RCAT is the loss of the superior stabilizing force of the rotator cuff due to a massive, irreparable tear. This allows the deltoid muscle to pull the humeral head superiorly, leading to proximal migration. This superior migration causes abnormal articulation between the humeral head and the acromion/coracoacromial arch, resulting in erosion of the articular cartilage of both the humeral head and the glenoid, and eventually arthritic changes. Chronic inflammation (Option A) and primary osteoarthritis (Option B) are not the initiating factors for RCAT. Biceps tendinopathy (Option D) can be associated but is not the primary mechanism of arthropathy. While impingement (Option E) can be a precursor to rotator cuff tears, RCAT represents a more advanced stage where the cuff is massively torn, and the primary issue is the loss of humeral head depression and centering.
Question 25
If this 76-year-old gentleman had a massive rotator cuff tear but without radiographic evidence of proximal humeral migration or established arthropathy, what would be the MOST appropriate initial non-operative management strategy?
Explanation
Correct Answer: B
For a massive rotator cuff tear without established arthropathy, initial management often involves non-operative approaches to alleviate symptoms and improve function. A subacromial steroid injection (Option B) can help reduce inflammation and pain, facilitating participation in physical therapy to strengthen remaining cuff muscles and periscapular stabilizers. Immediate surgical repair (Option A) is often considered for younger, active patients or those who fail non-operative management, but it's not always the initial step, especially in older patients or those with lower demands. Glenohumeral steroid injection (Option C) is less commonly used for cuff tears and more for primary glenohumeral arthritis. Activity modification and observation (Option D) alone may not be sufficient for symptomatic relief or functional improvement. Shoulder fusion (Option E) is a salvage procedure for severe, painful, irreparable conditions, not an initial management for a massive tear without arthropathy.
Question 26
The first candidate suggests a subacromial steroid injection, followed by arthroscopic debridement and subacromial decompression after 8 weeks of failed conservative treatment. Why is this management plan inappropriate for a patient with established rotator cuff tear arthropathy?
Explanation
Correct Answer: C
The first candidate's plan is inappropriate because subacromial steroid injections, arthroscopic debridement, and subacromial decompression primarily address impingement and inflammation, or debride torn tissue. In established rotator cuff tear arthropathy (RCAT), the underlying problem is a massive, irreparable rotator cuff tear leading to superior migration of the humeral head and subsequent degenerative changes. These procedures do not restore the lost superior stability or the function of the massively torn cuff, and therefore will not significantly improve the patient's symptoms or function. Subacromial decompression is not contraindicated by age alone (Option A). Steroid injections can be effective for some shoulder pain (Option B), but not for the underlying structural problem of RCAT. While infection risk is a concern in any surgery, it's not the primary reason this plan is inappropriate (Option D). The patient's symptoms are amenable to surgical intervention, but a different type (Option E).
Question 27
Given the diagnosis of rotator cuff tear arthropathy in this 76-year-old fit gentleman who desires reasonable ability to abduct his shoulder for painting and has failed conservative management, what is the MOST appropriate surgical intervention?
Explanation
Correct Answer: D
For a 76-year-old fit gentleman with established rotator cuff tear arthropathy (RCAT), failed conservative management, and a desire for improved abduction, a reverse shoulder arthroplasty (RSA) is the most appropriate surgical intervention. Rotator cuff repair (Option A) is not possible due to the established arthropathy and likely irreparable nature of the massive tear. Hemiarthroplasty (Option B) would replace only the humeral head, but without a functional rotator cuff, the superior migration would persist, leading to poor outcomes and continued glenoid erosion. Total shoulder arthroplasty (TSA) (Option C) relies on an intact rotator cuff for stability and function, making it contraindicated in RCAT. Arthrodesis (Option E) is a salvage procedure that sacrifices motion for pain relief and stability, which would not meet the patient's desire for abduction for painting. RSA, by medializing and distalizing the center of rotation, allows the deltoid to function as the primary abductor, providing predictable pain relief and improved active range of motion, especially abduction.
Question 28
The candidate correctly explains that reverse shoulder arthroplasty (RSA) brings the center of rotation of the glenohumeral joint medially and increases the moment arm of the deltoid. How does this biomechanical change primarily contribute to improved shoulder function in patients with rotator cuff tear arthropathy?
Explanation
Correct Answer: C
The key biomechanical advantage of reverse shoulder arthroplasty (RSA) in rotator cuff tear arthropathy (RCAT) is its ability to restore active elevation (abduction and forward flexion) in the absence of a functional rotator cuff. By medializing and distalizing the center of rotation, the RSA effectively lengthens the deltoid muscle and increases its moment arm. This allows the deltoid to become the primary abductor and elevator of the arm, compensating for the deficient rotator cuff. It does not directly repair the cuff (Option A). While it can reduce glenoid erosion by providing a stable articulation, this is a secondary effect, not the primary mechanism for improved function (Option B). It typically improves abduction and flexion but may compromise rotation (Option D). Pain relief is a major goal, but it's achieved through restoring stability and function, not denervation (Option E).
Question 29
While reverse shoulder arthroplasty is indicated for rotator cuff tear arthropathy, which of the following conditions would generally be considered a contraindication or a significant relative contraindication for RSA?
Explanation
Correct Answer: C
An intact and functional rotator cuff (Option C) is a contraindication for reverse shoulder arthroplasty (RSA). RSA is specifically designed for patients with a deficient rotator cuff (e.g., massive irreparable tears, rotator cuff tear arthropathy) where a conventional total shoulder arthroplasty (TSA) would fail due to lack of cuff function. If the rotator cuff is intact and functional, a TSA or hemiarthroplasty would typically be preferred for primary glenohumeral osteoarthritis. Advanced age (Option A) is generally not a contraindication if the patient is otherwise fit for surgery. A history of previous shoulder surgery (Option B) is common and not a contraindication. Mild glenohumeral osteoarthritis (Option D) with an intact cuff would be better treated with TSA or hemiarthroplasty. Patient expectation for only pain relief (Option E) is a reasonable goal for RSA, although improved motion is also expected.
Question 30
The examiner praises the second candidate for asking about the patient's symptoms, previous treatments, and expectations before committing to a management plan. This approach BEST exemplifies which principle of patient care?
Explanation
Correct Answer: C
The second candidate's approach of inquiring about symptoms, previous treatments, and patient expectations before recommending surgery demonstrates a strong patient-centered approach (Option C). This is crucial in orthopedic decision-making, especially for elective procedures like arthroplasty. It ensures that the chosen treatment aligns with the patient's functional goals and quality of life. Prioritizing imaging over clinical presentation (Option A) is a mistake the first candidate made. Adhering strictly to algorithms (Option B) without considering individual patient factors can lead to suboptimal outcomes. Delaying treatment (Option D) is not the intent; rather, it's about gathering relevant information to make an informed decision. Focusing solely on anatomical pathology (Option E) ignores the patient's functional limitations and desired outcomes, which is a critical component of successful treatment.
Question 31
A 55-year-old female presents with a 4-month history of progressive radiating pain in her right leg and mild foot drop. MRI of the lumbar spine reveals an intradural-extramedullary tumor at L4-L5, which is T1 isointense, T2 hyperintense, and shows strong, homogeneous enhancement with gadolinium. Erosion of the adjacent pedicle is noted. Which of the following is the most likely diagnosis?
Explanation
Correct Answer: C
The classic presentation of a slowly progressive radiculopathy combined with an intradural-extramedullary tumor that shows strong, homogeneous enhancement and associated bony erosion (enlarged neural foramen) is highly suggestive of a schwannoma. Meningiomas are also intradural-extramedullary but often show a dural tail sign and are more common in the thoracic spine in older females. Ependymomas and astrocytomas are intramedullary tumors. Neurofibromas are closely related to schwannomas but are more often associated with neurofibromatosis and can be plexiform.
Question 32
A 70-year-old male with a history of prostate cancer presents with new onset of severe mid-thoracic back pain, bilateral lower extremity weakness, and urinary retention. Neurological exam reveals a T8 sensory level and paraparesis (motor grade 2/5 bilaterally). What is the MOST appropriate initial management step?
Explanation
Correct Answer: A
This patient presents with signs and symptoms of acute spinal cord compression due to suspected metastatic disease. The priority is to prevent further neurological deterioration. High-dose IV corticosteroids (Dexamethasone) should be administered immediately to reduce edema around the spinal cord, and an emergent MRI of the entire spine is crucial to delineate the extent of compression, identify instability, and guide definitive treatment. Surgical decompression or radiation therapy will be considered after imaging and patient assessment, but steroids and imaging are the initial, most time-sensitive steps. Plain radiographs are insufficient for diagnosing spinal cord compression.
Question 33
Which of the following spinal tumor types is typically intramedullary and often associated with syringomyelia or cyst formation, particularly in the cervical spine?
Explanation
Correct Answer: C
Ependymomas are the most common intramedullary spinal cord tumors in adults, frequently found in the cervical and cervicothoracic regions. They are well-known for their association with intratumoral hemorrhage and the formation of syrinx cavities, or cysts, both rostral and caudal to the tumor, due to altered CSF flow dynamics. Meningiomas and schwannomas are typically intradural-extramedullary. Chordomas and osteosarcomas are extradural, bone-forming tumors.
Question 34
Regarding the surgical management of metastatic spinal tumors, the Spine Instability Neoplastic Score (SINS) is used to guide treatment. Which score range typically indicates overt instability requiring surgical stabilization?
Explanation
Correct Answer: E
The SINS score is a validated tool to assess spinal stability in patients with neoplastic disease. A score of 0-6 indicates stability, 7-12 indicates indeterminate stability, and 13-18 indicates overt instability. Therefore, a score above 7 (i.e., 8 or higher) typically suggests a need for surgical stabilization, although scores in the indeterminate range often warrant careful consideration and surgical consultation. A score above 12 definitely indicates overt instability, but the cutoff for considering intervention starts earlier.
Question 35
Which primary bone tumor of the spine is most commonly found in the sacrum and clivus, and is characterized by its local aggressiveness and high recurrence rates despite appearing histologically benign?
Explanation
Correct Answer: D
Chordomas are rare, slow-growing malignant tumors derived from notochordal remnants. They have a predilection for the axial skeleton, particularly the sacrum (50-60%) and the clivus (30-35%), but can occur anywhere along the spine. They are known for their local aggressiveness, high local recurrence rates, and challenging surgical resection due to their location, despite often appearing histologically benign. Osteosarcoma, chondrosarcoma, and Ewing's sarcoma can affect the spine but have different epidemiological and anatomical distributions. Giant cell tumors are benign but locally aggressive, typically affecting long bones, and less commonly the spine.
Question 36
A 45-year-old male presents with chronic back pain. Imaging reveals a lytic lesion in a vertebral body. A biopsy confirms metastatic renal cell carcinoma. The patient has no neurological deficits. Given the high vascularity of renal cell metastases, which pre-operative measure is often considered to reduce surgical blood loss?
Explanation
Correct Answer: C
Metastases from renal cell carcinoma, thyroid carcinoma, and pheochromocytoma are notoriously hypervascular. Pre-operative embolization of the tumor's feeding arteries, typically performed by interventional radiology 24-72 hours before surgery, can significantly reduce intraoperative blood loss and improve the safety and feasibility of resection. Chemotherapy, corticosteroids (unless cord compression), or radiation therapy do not directly address intraoperative bleeding from hypervascular lesions. Immediate surgery without embolization carries a high risk of catastrophic hemorrhage.
Question 37
According to the Enneking staging system, modified for spinal tumors, an Enneking stage III tumor (intracapsular benign) would be managed differently from a stage IA tumor (low-grade malignant, intracompartmental). Which of the following best describes the goal of surgical treatment for an Enneking Stage II (benign, extracompartmental) lesion?
Explanation
Correct Answer: B
The Enneking staging system guides surgical margins. For an Enneking Stage I lesion (latent benign), intralesional curettage might suffice. For Stage II (active benign/extracompartmental), the goal is a marginal excision, where the tumor is removed en bloc with a minimal rim of surrounding normal tissue. This aims to remove the tumor completely while preserving vital structures. Stage III (aggressive benign) and Stage IA/IB (low-grade malignant) lesions often require a wide en bloc resection, aiming for a broader margin of healthy tissue. Radical resection is for high-grade malignancies or highly aggressive tumors where a 'dirty' margin is unacceptable. Palliative decompression is for advanced metastatic disease with neurological compromise.
Question 38
A 60-year-old patient with a known history of lung cancer develops new back pain. MRI shows an epidural mass compressing the spinal cord at T10. There is no neurological deficit beyond mild sensory changes. What is the most appropriate treatment strategy for optimal local control and quality of life?
Explanation
Correct Answer: D
For patients with good performance status, limited epidural compression, and radiosensitive tumors (like lung cancer), SBRT has emerged as a preferred treatment modality. SBRT delivers high-dose, highly conformal radiation in fewer fractions, offering excellent local control with less toxicity compared to conventional external beam radiation, and can often spare patients from extensive surgery, especially if they have mild or no neurological deficits. Emergent surgery is reserved for severe or rapidly progressing neurological deficits, spinal instability, or radioresistant tumors. Conventional radiation is an option but SBRT offers better local control. Chemotherapy is systemic, not primary for local compression, unless very chemosensitive tumor. Conservative management is inappropriate for spinal cord compression.
Question 39
Which of the following characteristics is most consistent with a diagnosis of vertebral hemangioma on MRI?
Explanation
Correct Answer: C
Vertebral hemangiomas are benign vascular tumors of the spine. On MRI, they are characteristically T1 hyperintense and T2 hyperintense due to their high fat content within the vascular channels. The 'polka dot' appearance on axial CT (due to thickened vertical trabeculae separated by fatty marrow) and the 'corduroy' sign on sagittal radiographs are classic, which correlate to high signal areas on MRI. Other options describe meningiomas (dural tail), blastic metastases (sclerotic), or aggressive malignant lesions (expansile lytic).
Question 40
What is the most common primary malignant tumor of the spine in adults?
Explanation
Correct Answer: E
Multiple Myeloma is the most common primary malignant tumor involving bone in adults, and the spine is a frequently affected site. It is a hematologic malignancy characterized by the proliferation of plasma cells. While chordoma, osteosarcoma, chondrosarcoma, and Ewing's sarcoma are also primary malignant bone tumors of the spine, they are individually much rarer than multiple myeloma. Ewing's sarcoma is more common in adolescents and young adults.
Question 41
A 68-year-old male presents with difficulty buttoning his shirt and a progressive change in his gait. Examination reveals an inverted brachioradialis reflex. This finding is most indicative of compressive pathology at which of the following spinal levels?
Explanation
Question 42
A 72-year-old female undergoes a reverse total shoulder arthroplasty (RTSA) for rotator cuff tear arthropathy. The biomechanical advantage of this prosthesis relies on medializing the center of rotation and increasing the moment arm of which of the following muscles?
Explanation
Question 43
According to the Musculoskeletal Infection Society (MSIS) criteria, which of the following is considered a definitive major criterion for diagnosing a periprosthetic joint infection?
Explanation
Question 44
A 14-year-old boy presents with knee pain and swelling. Radiographs reveal a sunburst periosteal reaction in the distal femoral metaphysis. Biopsy confirms osteosarcoma. What is the standard first-line systemic chemotherapeutic regimen for this condition?
Explanation
Question 45
A 60-year-old female presents with severe neurogenic claudication. Imaging shows a grade I degenerative spondylolisthesis at L4-L5. If conservative management fails, which nerve root is most likely compressed within the lateral recess at this level?
Explanation
Question 46
A 22-year-old rugby player has recurrent anterior shoulder instability. Computed tomography shows a 28% anterior glenoid bone loss. An open Latarjet procedure is planned. Which structure passes through the "split" of the subscapularis during this procedure?
Explanation
Question 47
A 4-year-old boy presents with acute right hip pain, fever of 39.0°C, and absolute refusal to bear weight. His ESR is 50 mm/hr and WBC is 14,000/mm³. According to the Kocher criteria, what is the approximate statistical probability that this child has septic arthritis?
Explanation
Question 48
A 32-year-old woman presents with a lytic, expansile epiphyseal lesion in the proximal tibia. Histology shows mononuclear cells interspersed with multinucleated giant cells. Which of the following targeted therapies acts by binding to RANKL for the treatment of this lesion?
Explanation
Question 49
An 82-year-old male sustains a Type II odontoid fracture. He has severe medical comorbidities making surgery high risk. If treated non-operatively with a rigid cervical collar, which factor is most highly associated with an increased risk of non-union?
Explanation
Question 50
A 45-year-old diabetic female presents with global restriction of shoulder active and passive motion. She is diagnosed with adhesive capsulitis. The pathophysiology of this condition is primarily characterized by elevated levels of which of the following cytokines?
Explanation
Question 51
A 54-year-old intravenous drug user presents with mid-back pain, a low-grade fever, and progressive bilateral lower extremity weakness over the past 48 hours. MRI of the thoracic spine reveals a ventral epidural abscess spanning T6-T8 with severe anterior spinal cord compression. What is the most appropriate surgical approach for this patient?
Explanation
Question 52
A 72-year-old female presents with pseudoparalysis of her dominant right shoulder. Radiographs show superior migration of the humeral head with an acromiohumeral interval of 3 mm. She has a history of a massive, irreparable rotator cuff tear. Which of the following is an absolute contraindication to a reverse total shoulder arthroplasty (RTSA) in this patient?
Explanation
Question 53
A 45-year-old poorly controlled diabetic presents with exquisite pain in his lower leg out of proportion to exam findings, massive swelling, and advancing erythema. Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score is 8. Which of the following is the most critical next step in management?
Explanation
Question 54
An 11-year-old boy presents with progressive knee pain. Radiographs reveal a metaphyseal, mixed lytic and sclerotic lesion in the distal femur with a "sunburst" periosteal reaction.
Biopsy confirms high-grade conventional osteosarcoma. What is the standard of care for treatment?
Explanation
Question 55
In the radiographic evaluation of adult spinal deformity, which of the following spinopelvic parameters is most highly correlated with poor health-related quality of life (HRQOL) scores and serves as a primary target during surgical correction?
Explanation
Question 56
A 50-year-old female with type 1 diabetes presents with progressive, severe shoulder pain and stiffness over the past 4 months. She has lost both active and passive range of motion, particularly in external rotation. What is the most characteristic histological finding of the glenohumeral capsule in this condition?
Explanation
Question 57
A 3-year-old boy presents with a 2-day history of refusal to bear weight on his right leg. He is febrile to 39.0 degrees C. His ESR is 50 mm/hr, CRP is 4.5 mg/dL, and WBC is 14,000/mm^3. Based on the classic Kocher criteria, what is the predictive probability that this child has a septic hip?
Explanation
Question 58
A 14-year-old girl presents with deep thigh pain and a palpable soft tissue mass. Radiographs show a permeative lytic lesion in the diaphysis of the femur with a prominent "onion skin" periosteal reaction. Genetic testing of the biopsy specimen is most likely to reveal which of the following translocations?
Explanation
Question 59
A 30-year-old male falls from a height of 15 feet, sustaining a T12 burst fracture. He is neurologically intact. Which of the following radiographic findings is most specifically indicative of a posterior ligamentous complex (PLC) injury, necessitating surgical stabilization?
Explanation
Question 60
A 22-year-old collegiate wrestler sustains a traumatic anterior shoulder dislocation. After reduction, an MRI arthrogram reveals an avulsion of the anterior-inferior glenoid labrum. Which ligamentous structure, attached to this torn labral fragment, acts as the primary restraint to anterior translation at 90 degrees of shoulder abduction and maximum external rotation?
Explanation
Question 61
A 68-year-old male presents with chronic right knee pain 3 years after a total knee arthroplasty. Aspiration yields synovial fluid with a WBC count of 4,500 cells/uL and 85% polymorphonuclear neutrophils (PMNs). According to the Musculoskeletal Infection Society (MSIS) criteria for chronic PJI, what is the most appropriate interpretation and next step?
Explanation
Question 62
A 32-year-old female presents with activity-related knee pain. Radiographs reveal an eccentric, lytic lesion in the distal femoral epiphysis extending to the subchondral bone without a sclerotic margin. Histology shows multinucleated giant cells in a background of neoplastic mononuclear stromal cells. What is the standard first-line surgical treatment?
Explanation
Question 63
A 45-year-old male presents with severe right leg pain radiating to the dorsum of his foot and great toe. Neurological examination reveals 3/5 weakness in extensor hallucis longus (EHL) and decreased sensation over the first dorsal web space. A paracentral disc herniation at which lumbar level is most likely responsible?
Explanation
Question 64
A 28-year-old cyclist falls directly onto his left shoulder, sustaining a completely displaced midshaft clavicle fracture with 2.5 cm of shortening and no cortical contact. If this fracture is managed nonoperatively in a sling, what is the most commonly reported complication compared to operative fixation?
Explanation
Question 65
A 15-year-old male presents with right distal femur pain. Radiographs reveal a metaphyseal lesion with a 'sunburst' periosteal reaction and Codman's triangle. Which of the following is the most appropriate management sequence?
Explanation
None
