ABOS Orthopedic Board Review: Psoriatic Arthritis, Lipoma Arborescens, Down Syndrome, Scoliosis | Part 30
Key Takeaway
This ABOS Orthopedic Board Review provides challenging multiple-choice questions on key topics. Master your knowledge of psoriatic arthritis, lipoma arborescens, Down syndrome orthopedic abnormalities, and various scoliosis types. Enhance your exam preparation with detailed rationales and explanations for comprehensive understanding.
ABOS Orthopedic Board Review: Psoriatic Arthritis, Lipoma Arborescens, Down Syndrome, Scoliosis | Part 30
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 45-year-old female with a history of scaly skin plaques presents with asymmetric oligoarthritis and dactylitis of her right hand. Radiographs demonstrate central erosions of the proximal phalanx with distal bone proliferation creating a "pencil-in-cup" appearance. Which joint is classically most affected in this condition?
Explanation
Question 2
A 52-year-old male with severe psoriatic arthritis on adalimumab (Humira) is scheduled for an elective total knee arthroplasty. According to current ACR/AAHKS guidelines, how should his biologic therapy be managed perioperatively?
Explanation
Question 3
Which of the following radiographic findings is most characteristic of psoriatic arthritis as opposed to rheumatoid arthritis?
Explanation
Question 4
A patient with a long-standing history of psoriasis presents with severe, deforming joint destruction of the hands resulting in "telescoping" fingers. Which severe subtype of psoriatic arthritis does this clinical picture represent?
Explanation
Question 5
A 35-year-old male with known psoriatic arthritis develops severe, progressive axial spine pain and asymmetric sacroiliitis. Which human leukocyte antigen (HLA) is most strongly associated with this specific axial presentation?
Explanation
Question 6
A 40-year-old male complains of a chronic, painless, swollen right knee. MRI demonstrates a frond-like synovial mass.
What is the characteristic MRI finding that confirms this diagnosis?

Explanation
Question 7
Which histologic description best characterizes the lesion known as lipoma arborescens?
Explanation
Question 8
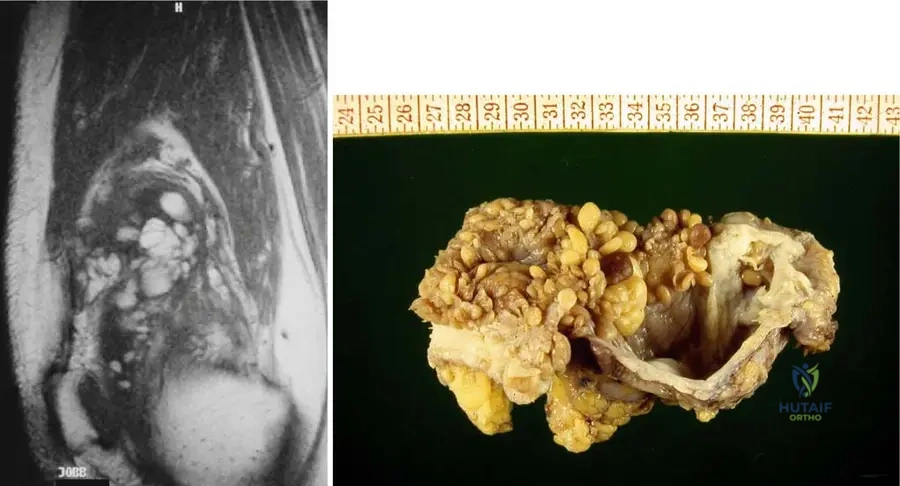
A 38-year-old female presents with mechanical catching and recurrent effusions in her knee. Imaging and gross pathology are shown.
What is the definitive treatment for this symptomatic primary lesion?
Explanation
Question 9
When attempting to differentiate lipoma arborescens from pigmented villonodular synovitis (PVNS) on MRI, which feature is highly specific for PVNS?
Explanation
Question 10
Which of the following joint conditions is most commonly associated with the development of secondary lipoma arborescens?
Explanation
Question 11
An 8-year-old boy with Down syndrome presents with hyperreflexia, a new wide-based gait, and neck pain.
Dynamic flexion-extension radiographs reveal an atlanto-dens interval (ADI) of 11 mm. What is the most appropriate management?
Explanation
Question 12
A 45-year-old male with a history of psoriasis presents with asymmetric oligoarthritis and dactylitis. Radiographs of the hands reveal periarticular erosions and bone proliferation at the distal interphalangeal (DIP) joints. According to the CASPAR criteria, which of the following clinical findings is most specific to the diagnosis of Psoriatic Arthritis?
Explanation
Question 13
A 50-year-old female with severe psoriatic arthritis is scheduled for a total knee arthroplasty (TKA). She is currently managed with secukinumab. What is the mechanism of action of this biologic agent?
Explanation
Question 14
A patient with advanced psoriatic arthritis presents with a 'telescoping' digit resulting from severe osteolysis of the phalanges. Which of the following terms correctly describes this classic deformity?
Explanation
Question 15
When comparing outcomes of total joint arthroplasty in patients with psoriatic arthritis to those with primary osteoarthritis, patients with psoriatic arthritis are at an increased risk for which of the following complications?
Explanation
Question 16
A 38-year-old male presents with characteristic 'pencil-in-cup' deformities on hand radiographs. Which pathophysiologic process best explains this radiographic appearance in psoriatic arthritis?
Explanation
Question 17
A 45-year-old male presents with chronic, painless, boggy swelling of the left knee. An MRI is obtained. Based on the likely diagnosis of Lipoma Arborescens, what is the classic MRI finding?
Explanation
Question 18
Which of the following histological descriptions is diagnostic for Lipoma Arborescens?
Explanation
Question 19
Lipoma arborescens is most frequently associated with which of the following underlying conditions?
Explanation
Question 20
A 52-year-old female diagnosed with Lipoma Arborescens of the suprapatellar pouch continues to have mechanical symptoms and massive effusions despite intra-articular corticosteroid injections. What is the recommended treatment?
Explanation
Question 21
Which anatomic location is most commonly affected by Lipoma Arborescens?
Explanation
Question 22
A 7-year-old boy with Down syndrome presents for cervical spine screening. Radiographs demonstrate an atlanto-dens interval (ADI) of 6 mm and a Space Available for Cord (SAC) of 16 mm. He is neurologically intact. According to AAOS guidelines, what is the most appropriate management?
Explanation
Question 23
What is the critical Space Available for the Cord (SAC) threshold at the C1-C2 level that signifies an absolute indication for surgical stabilization in a patient with Down syndrome, regardless of symptoms?
Explanation
Question 24
A 12-year-old girl with Down syndrome presents with habitual bilateral patellar dislocations. Which underlying anatomic abnormalities primarily drive patellofemoral instability in this population?
Explanation
Question 25
A newborn with Down syndrome undergoes a pelvic radiograph for hip screening. Which of the following classic radiographic findings is typically seen in the pelvis of infants with Trisomy 21?
Explanation
Question 26
When performing an atlantoaxial fusion for severe instability in a patient with Down syndrome, what is the most commonly reported significant postoperative complication?
Explanation
Question 27
In an adolescent with idiopathic scoliosis, which of the following combinations of congenital vertebral anomalies carries the highest risk for rapid curve progression and often requires early surgical intervention?
Explanation
Question 28
A 13-year-old female is 5 days post-operative from a posterior spinal fusion for adolescent idiopathic scoliosis. She complains of postprandial bilious vomiting and epigastric pain. An upper GI series shows delayed gastric emptying and an abrupt cut-off of contrast in the duodenum. What anatomic structure is responsible for compressing the duodenum?
Explanation
Question 29
According to the Lenke Classification system for Adolescent Idiopathic Scoliosis, what defines a structural proximal thoracic (PT) curve?
Explanation
Question 30
A 14-year-old male with severe spastic cerebral palsy (GMFCS Level V) is undergoing posterior spinal fusion for a 75-degree neuromuscular scoliosis. He has a pelvic obliquity of 25 degrees. What is the primary functional indication for extending the fusion to the pelvis in this patient?
Explanation
Question 31
Which of the following Sanders skeletal maturity stages correlates most closely with the peak height velocity (PHV) and the highest risk of curve progression in Adolescent Idiopathic Scoliosis?
Explanation
Question 32
A 45-year-old female with a history of scaly plaques on her extensor surfaces presents with chronic hand pain. Radiographs demonstrate erosive changes at the distal interphalangeal (DIP) joints, characterized by proximal phalanx tapering and distal phalanx base expansion. Which of the following is the most likely diagnosis?
Explanation
Question 33
A 52-year-old male with psoriatic arthritis is scheduled for a total hip arthroplasty. He is currently well-controlled on adalimumab (a TNF-alpha inhibitor). According to current ACR/AAHKS guidelines, what is the most appropriate perioperative management of his biologic medication?
Explanation
Question 34
Which of the following clinical or radiographic features most reliably distinguishes psoriatic arthritis from rheumatoid arthritis?
Explanation
Question 35
What is the primary early pathologic target of inflammation in psoriatic arthritis that leads to joint destruction, differentiating it from the primary target in rheumatoid arthritis?
Explanation
Question 36
Compared to patients with primary osteoarthritis, patients with psoriatic arthritis undergoing primary total knee arthroplasty have a significantly higher risk of which of the following postoperative complications?
Explanation
Question 37
A 35-year-old male presents with chronic, painless swelling of the right knee. MRI demonstrates a frond-like mass in the suprapatellar pouch.
Which of the following MRI characteristics is pathognomonic for this condition?
Explanation
Question 38
Which of the following is the most definitive surgical management for symptomatic lipoma arborescens of the knee that has failed conservative treatment?
Explanation
Question 39
Histologic examination of a specimen retrieved from a patient with lipoma arborescens will classically demonstrate which of the following?
Explanation
Question 40
In which anatomic location is lipoma arborescens most frequently identified?
Explanation
Question 41
Which of the following underlying conditions is most frequently associated with the development of secondary lipoma arborescens?
Explanation
Question 42
An 8-year-old child with Down syndrome presents for clearance to participate in the Special Olympics.
They are completely asymptomatic. Flexion-extension cervical radiographs reveal an atlantodens interval (ADI) of 6 mm. What is the most appropriate next step in management?
Explanation
Question 43
The myriad of orthopedic manifestations seen in Down syndrome, including patellofemoral instability, pes planus, and hip subluxation, are primarily attributed to which underlying pathophysiology?
Explanation
Question 44
A 10-year-old male with Down syndrome presents with a 3-week history of a limp and poorly localized knee pain. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Compared to an idiopathic SCFE in a neurotypical child, this patient is at an increased risk for which of the following?
Explanation
Question 45
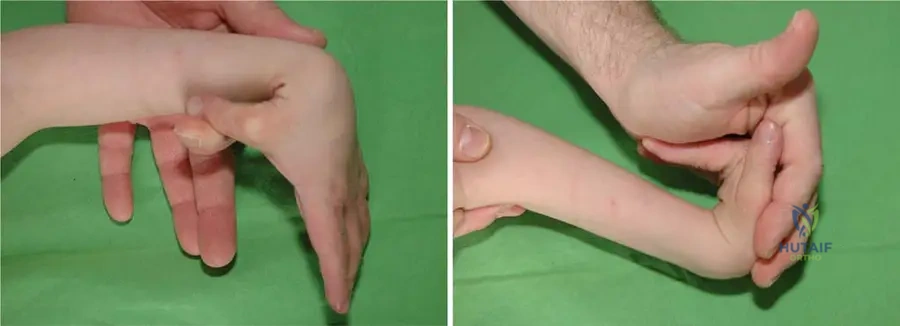
A child with Down syndrome presents with a characteristic hand anomaly.
What is the specific anatomic basis of the clinodactyly commonly observed in these patients?
Explanation
Question 46
An adult with Down syndrome presents with progressive clumsiness, hyperreflexia, and a positive Babinski sign. Cervical radiographs are obtained. Which radiographic measurement is the strongest indicator of neurologic compromise and risk of spinal cord compression?
Explanation
Question 47
A 12-year-old female presents with a 32-degree right thoracic curve. She has not reached menarche. Radiographs demonstrate open triradiate cartilages and a Risser stage of 0. What is the most appropriate management?
Explanation
Question 48
In a 9-month-old infant diagnosed with infantile idiopathic scoliosis, which of the following radiographic parameters is the most reliable predictor of curve progression requiring intervention?
Explanation
Question 49
A 13-year-old boy presents for school scoliosis screening. Radiographs demonstrate a 38-degree left-sided thoracic scoliosis. His neurologic examination is entirely normal. What is the most appropriate next step in his evaluation?
Explanation
Question 50
In a patient with Adolescent Idiopathic Scoliosis, which of the following clinical milestones corresponds with the period of greatest risk for rapid curve progression?
Explanation
Question 51
During a posterior spinal fusion for a 55-degree thoracic scoliosis, the neuromonitoring technician reports a sudden, bilateral 60% decrease in amplitude and a 15% increase in latency of the somatosensory evoked potentials (SSEPs). Which of the following is the best initial step?
Explanation
Question 52
A 45-year-old female with a history of scaly plaques on her extensor surfaces and nail pitting presents with hand pain. Radiographs demonstrate a "pencil-in-cup" deformity of the distal interphalangeal joints. Which of the following is the most likely diagnosis?
Explanation
Question 53
A 45-year-old male presents with worsening pain and stiffness in his fingers. Exam shows nail pitting and dactylitis. Radiographs reveal osteolysis of the proximal phalanx with bony proliferation of the distal phalanx base. What is the most likely diagnosis?
Explanation
Question 54
Which of the following immunogenetic markers is most strongly associated with the axial spine manifestations of psoriatic arthritis?
Explanation
Question 55
A patient with severe psoriatic arthritis is started on secukinumab after failing methotrexate therapy. What is the precise mechanism of action of this biological medication?
Explanation
Question 56
When planning total knee arthroplasty for a patient with advanced psoriatic arthritis, the surgeon must counsel the patient on which of the following elevated post-operative risks compared to primary osteoarthritis?
Explanation
Question 57
Which radiographic feature in the hand is characteristic of psoriatic arthritis and helps distinguish it from rheumatoid arthritis?
Explanation
Question 58
A 50-year-old male presents with a painless, slowly enlarging, boggy swelling of the left knee. MRI demonstrates a frond-like synovial mass with signal intensity identical to subcutaneous fat on all sequences.
What is the best initial definitive surgical treatment for a highly symptomatic patient?
Explanation
Question 59
Lipoma arborescens is a rare, benign intra-articular lesion. Which of the following underlying joint conditions is most frequently associated with its development?
Explanation
Question 60
A 45-year-old woman presents with recurrent knee effusions. MRI reveals a villous, lipomatous synovial proliferation.
Which MRI sequence change will confirm the diagnosis of lipoma arborescens by extinguishing the high signal of the lesion?
Explanation
Question 61
Histological examination of a specimen retrieved from a knee synovectomy in a patient with suspected lipoma arborescens will most likely demonstrate which of the following?
Explanation
Question 62
What is the most common anatomical location for the development of lipoma arborescens?
Explanation
Question 63
A 7-year-old child with Down syndrome presents for routine orthopedic evaluation.
Cervical spine flexion-extension radiographs are obtained. Which of the following radiographic measurements is the most reliable indicator of impending neurologic compromise and an absolute indication for posterior cervical fusion?
Explanation
Question 64
A 10-year-old boy with Down syndrome presents with a 2-month history of a limp and poorly localized thigh pain. Exam reveals obligate external rotation of the hip during passive flexion. Which of the following is the most likely diagnosis?
Explanation
Question 65
Which of the following lower extremity orthopedic conditions is most prevalent in the Down syndrome population due to underlying collagen defects and generalized ligamentous laxity?
Explanation
Question 66
According to the American Academy of Pediatrics (AAP), what is the current recommendation regarding routine cervical spine radiographic screening for asymptomatic children with Down syndrome prior to participation in sports?
Explanation
Question 67
A 12-year-old girl with Down syndrome presents with a 45-degree thoracic scoliotic curve.
Compared to adolescent idiopathic scoliosis (AIS), how does the management and prognosis of scoliosis in patients with Down syndrome typically differ?
Explanation
Question 68
In a 13-year-old female with adolescent idiopathic scoliosis, which of the following combinations of factors represents the highest risk for curve progression?
Explanation
Question 69
In the Lenke classification system for adolescent idiopathic scoliosis, a proximal thoracic curve is considered "structural" and must be included in the fusion construct if the curve bends out to what minimum Cobb angle on side-bending radiographs?
Explanation
Question 70
A 6-month-old infant is diagnosed with infantile idiopathic scoliosis. The rib-vertebral angle difference (RVAD) is calculated at the apical vertebra. An RVAD greater than what threshold suggests a high probability of curve progression?
Explanation
Question 71
When evaluating the spinal radiographic manifestations of a patient with psoriatic arthritis compared to ankylosing spondylitis, psoriatic arthritis is more characteristically associated with which of the following findings?
Explanation
Question 72
A 55-year-old male with long-standing psoriatic arthritis is planning to undergo a total knee arthroplasty (TKA). Compared to a patient with primary osteoarthritis, this patient is at a significantly higher risk for which of the following postoperative complications?
Explanation
Question 73
A 42-year-old male presents with a chronic, slowly enlarging, painless knee effusion. An MRI is obtained.
Based on the most likely diagnosis, what is the definitive treatment of choice?
Explanation
Question 74
A 7-year-old child with Down syndrome wishes to participate in the Special Olympics. Cervical spine flexion-extension radiographs reveal an anterior atlantodens interval (ADI) of 6 mm. The patient has no neurologic symptoms. What is the most appropriate management according to current guidelines?
Explanation
Question 75
A 2-year-old female is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra at T8. Which of the following is the most appropriate routine screening protocol to order upon making this diagnosis?
Explanation
Question 76
The pathophysiology of psoriatic arthritis distinguishes it from rheumatoid arthritis by the primary anatomic site of initial inflammation. Which of the following structures is the earliest and primary target of the inflammatory process in psoriatic arthritis?
Explanation
Question 77
Which of the following histological findings is pathognomonic for lipoma arborescens?
Explanation
Question 78
A 10-year-old boy with Down syndrome presents with a painless limp.
What is the primary underlying cause of recurrent hip instability and subluxation in this specific patient population?
Explanation
Question 79
A 12-year-old female with Adolescent Idiopathic Scoliosis (AIS) presents with a right thoracic curve. Which of the following combinations of factors indicates the highest risk for curve progression?
Explanation
Question 80
A 50-year-old patient with long-standing psoriatic arthritis develops profound osteolysis of the phalanges, resulting in redundant overlying skin and telescoping digits (arthritis mutilans). What is the primary molecular driver of the massive bone resorption seen in this condition?
Explanation
Question 81
Lipoma arborescens is most frequently observed in which of the following anatomic locations?
Explanation
Question 82
In evaluating a patient with Down syndrome for cervical spine instability, which radiographic measurement is the most reliable predictor of impending neurologic compromise?
Explanation
Question 83
In a 65-year-old female undergoing spinal deformity correction for adult degenerative scoliosis, achieving which of the following spinopelvic parameters is most strongly correlated with favorable postoperative health-related quality of life (HRQOL) outcomes?
Explanation
Question 84
Which of the following physical examination findings in the hand is highly characteristic of psoriatic arthritis but is exceptionally rare in rheumatoid arthritis?
Explanation
Question 85
A 50-year-old female has a chronically swollen knee. MRI is obtained.
Which specific MRI sequence characteristic most definitively establishes the diagnosis of lipoma arborescens?
Explanation
Question 86
A 14-year-old girl with Down syndrome presents with recurrent, habitual patellar dislocations. Nonoperative management has failed. Operative intervention in this population is challenging due to generalized ligamentous laxity. Which approach is most often required for successful stabilization?
Explanation
Question 87
A 14-year-old non-ambulatory male with spastic quadriplegic cerebral palsy presents with a 75-degree neuromuscular scoliosis. What is the primary indication for extending the posterior spinal fusion construct to the pelvis in this patient?
Explanation
Question 88
A 35-year-old male with psoriatic arthritis has predominantly axial disease (spondylitis and sacroiliitis) that has remained highly active despite maximum doses of NSAIDs. According to current treatment guidelines, what is the preferred next step in pharmacologic management?
Explanation
Question 89
While lipoma arborescens is generally considered a benign, slow-growing neoplastic condition, it is most frequently encountered in patients with a history of which of the following underlying joint pathologies?
Explanation
Question 90
A 4-year-old child with Down syndrome presents with severe, symptomatic, flexible pes planovalgus that causes frequent tripping. Which of the following is the most appropriate initial management?
Explanation
Question 91
A 4-year-old boy presents with a 65-degree progressive early-onset scoliosis (EOS). He undergoes surgical treatment with distraction-based growth-friendly implants (growing rods). What is the most common long-term complication associated with this surgical strategy?
Explanation
Question 92
A 6-year-old boy with Down syndrome presents for a routine orthopedic evaluation prior to participating in the Special Olympics. Lateral flexion-extension cervical radiographs are obtained.
At what Atlanto-Dens Interval (ADI) threshold is surgical stabilization typically recommended in an entirely asymptomatic child with Down syndrome?
Explanation
Question 93
A 45-year-old male presents with chronic, painless swelling of the right knee without prior trauma. A sagittal T1-weighted MRI is shown below.
Which of the following is the most definitive and appropriate treatment for this condition?
Explanation
Question 94
A 50-year-old male with a long-standing history of generalized psoriasis develops progressive foreshortening of his digits, resulting in a "telescoping" phenomenon. Which of the following cytokines is most directly responsible for driving the extensive osteoclastogenesis and bone resorption seen in this specific presentation?
Explanation
Question 95
A 4-year-old girl with Down syndrome presents with a painless limp.
Radiographs demonstrate bilateral hip subluxation with an increased acetabular index. Which of the following underlying pathophysiologic factors most significantly contributes to the high rate of joint instability in this population?
Explanation
Question 96
A 12-year-old female with Down syndrome presents with a progressive 55-degree thoracic scoliotic curve. If posterior spinal fusion is performed, which of the following postoperative complications is significantly more common in this patient population compared to age-matched patients with adolescent idiopathic scoliosis?
Explanation
Question 97
A 38-year-old female presents with a slowly enlarging, boggy right knee effusion. MRI reveals a large, villous synovial mass in the suprapatellar pouch.
To reliably differentiate lipoma arborescens from Pigmented Villonodular Synovitis (PVNS) on MRI, which of the following imaging characteristics is most uniquely diagnostic of lipoma arborescens?
Explanation
Question 98
A 55-year-old male with long-standing psoriatic arthritis is evaluated for progressive cervical neck pain. He is HLA-B27 positive. Which of the following cervical spine manifestations is most characteristic of his disease compared to classical Rheumatoid Arthritis?
Explanation
Question 99
A 6-year-old boy with Down syndrome is diagnosed with a 35-degree right thoracic scoliosis. There is no evidence of atlantoaxial instability. Regarding the non-operative management of his spinal deformity, what is the expected efficacy of TLSO bracing?
Explanation
Question 100
A 42-year-old female with severe psoriatic arthritis presents with incapacitating pain, instability, and a 40-degree flexion deformity of her dominant index finger distal interphalangeal (DIP) joint. Radiographs show a classic "pencil-in-cup" deformity. If surgery is planned, which of the following is the most reliable procedure?
Explanation
None
