ABOS Part I & AAOS OITE Orthopaedic Surgery Review: AC Joint, Greater Tuberosity & Humeral Shaft Fractures | Part 21542

Key Takeaway
This module offers a comprehensive ABOS Part I and AAOS OITE orthopaedic surgery review. It features 30 advanced multiple-choice questions derived from high-yield clinical cases, focusing on AC joint injuries, greater tuberosity fractures, and Holstein-Lewis fractures. It covers diagnosis, Rockwood classification, surgical management, and post-operative rehabilitation protocols.
ABOS Part I & AAOS OITE Orthopaedic Surgery Review: AC Joint, Greater Tuberosity & Humeral Shaft Fractures | Part 21542
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 28-year-old male rugby player sustains a direct blow to the superior aspect of his right shoulder with his arm adducted during a tackle. He presents with significant pain and a visible deformity. Radiographs show superior displacement of the distal clavicle, with the coracoclavicular distance measured at 20 mm on the injured side compared to 10 mm on the contralateral uninjured side. The deltotrapezial fascia appears intact. Which Rockwood classification best describes this injury?
Explanation
Correct Answer: C
The case describes a Rockwood Type III injury. According to the Rockwood classification system, a Type III injury involves complete tears of both the acromioclavicular and coracoclavicular ligaments. The clavicle is significantly displaced superiorly, typically demonstrating a 25 to 100 percent increased coracoclavicular distance. In this patient, the coracoclavicular distance increased from 10 mm to 20 mm, representing a 100% increase, which falls within the Type III criteria. Furthermore, the deltotrapezial fascia remaining intact is a key distinguishing feature of Type III compared to Type V, where it is extensively stripped. Type II involves a complete tear of the acromioclavicular ligaments with intact coracoclavicular ligaments and less than 25% increase in coracoclavicular distance. Type IV involves posterior displacement of the clavicle into the trapezius, requiring an axillary lateral radiograph for diagnosis, which is not indicated here. Type V involves severe superior displacement exceeding 100% of the normal coracoclavicular distance and extensive stripping of the deltoid and trapezius fascia, which is not described as stripped in this case.
Question 2
A surgeon is performing an open reduction and internal fixation of a chronic acromioclavicular joint separation. During the procedure, they note significant horizontal instability of the clavicle on the acromion, even after initial reduction. Based on the provided case, which ligamentous structure is the primary restraint to this specific type of instability?
Explanation
Correct Answer: C
The case explicitly states under the 'Static Stabilizers' section: 'Biomechanically, the acromioclavicular ligaments provide the primary restraint to anterior-posterior horizontal translation of the clavicle on the acromion. Sectioning the superior acromioclavicular ligament results in profound horizontal instability.' The conoid and trapezoid ligaments (coracoclavicular ligaments) are crucial for vertical stability. The coracoacromial ligament is not a primary stabilizer of the AC joint itself, and the articular disc's role in stability is minimal, especially given its degeneration with age.
Question 3
A 35-year-old construction worker presents with a Rockwood Type III acromioclavicular joint injury after a fall from scaffolding. He reports significant pain and difficulty performing overhead tasks required for his job. On physical exam, he has dynamic overriding of the clavicle on the acromion during cross-body adduction. Based on the ISAKOS guidelines mentioned in the case, what is the most appropriate management strategy?
Explanation
Correct Answer: B
The case highlights the ISAKOS Upper Extremity Committee's subclassification of Type III injuries into Type IIIA (vertically unstable but horizontally stable) and Type IIIB (vertically and horizontally unstable). The consensus suggests that Type IIIA injuries are best managed non-operatively, while Type IIIB injuries, characterized by dynamic overriding of the clavicle on the acromion during cross-body adduction, often experience poor functional outcomes with conservative care and may benefit from early surgical stabilization. This patient is a manual laborer (overhead athlete/manual laborer are indications for surgery in Type III) and presents with dynamic overriding during cross-body adduction, which is characteristic of a Type IIIB injury. Since the injury is acute (implied by 'after a fall' and not stated as chronic), acute suspensory cortical button fixation is the appropriate surgical technique. Chronic biologic reconstruction is for injuries presenting after six weeks. Distal clavicle excision is typically for chronic osteolysis or arthrosis, not acute instability. Non-operative management is generally for Type IIIA or less demanding patients with Type III.
Question 4
A 40-year-old male presents to the emergency department after a cycling accident, complaining of severe right shoulder pain. Physical examination reveals a prominent distal clavicle. To accurately assess the acromioclavicular joint and rule out a Rockwood Type IV injury, which radiographic views are most critical, and what specific modification is recommended for optimal visualization of the AC joint itself?
Explanation
Correct Answer: B
The case states that a 'Standard trauma series of the shoulder should be obtained, including a true anteroposterior view, a scapular Y view, and an axillary lateral view.' It further emphasizes that 'The axillary lateral is absolutely critical for identifying the posterior clavicular displacement characteristic of a Rockwood Type IV injury.' For optimal visualization of the AC joint itself, the 'most sensitive imaging modality for evaluating the acromioclavicular joint is the Zanca view. This is obtained by tilting the X-ray beam 10 to 15 degrees cephalad and reducing the penetrance by 50 percent compared to a standard shoulder anteroposterior radiograph.'
Question 5
A 22-year-old collegiate football player undergoes arthroscopically assisted suspensory cortical button fixation for an acute Rockwood Type V acromioclavicular joint separation. During the procedure, the surgeon is preparing to drill the coracoid tunnel. Based on the case, what is a critical technical consideration to minimize the risk of iatrogenic coracoid fracture?
Explanation
Correct Answer: C
Under the 'Acute Injury Management' section, the case states: 'Coracoid Preparation: The base of the coracoid is exposed. Using fluoroscopic guidance or arthroscopic visualization, a guide pin is placed centrally at the base of the coracoid. It is critical to place this pin centrally to avoid eccentric drilling, which drastically increases the risk of iatrogenic coracoid fracture.' Eccentric drilling, multiple drill holes, or drill holes exceeding 4mm in diameter are all identified as etiologies for coracoid fracture in the 'Complications' table. Avoiding fluoroscopy would increase the risk of malposition, and drilling before exposure would be unsafe.
Question 6
A 48-year-old patient presents with a chronic, symptomatic Rockwood Type V acromioclavicular joint separation sustained 8 months prior. He has failed conservative management. The surgeon plans an anatomic coracoclavicular ligament reconstruction. Which of the following statements accurately reflects the principles of chronic AC joint reconstruction as outlined in the case?
Explanation
Correct Answer: C
The case clearly differentiates between acute and chronic injury management. For chronic injuries, it states: 'Chronic injuries, presenting after six weeks, lack this healing potential and require biologic augmentation, typically in the form of autograft or allograft tendon reconstruction.' It further specifies: 'Because biologic grafts require months to incorporate, they must be protected with concurrent mechanical fixation.' The Weaver-Dunn procedure is described as providing only 20-30% of native load to failure, making it inferior to anatomic reconstructions. Meticulous deltotrapezial fascial closure is highlighted as 'arguably the most critical step of the procedure' regardless of technique. Distal clavicle excision is typically for osteolysis or arthrosis, not the primary goal of chronic instability reconstruction.
Question 7
A 30-year-old patient undergoes surgical stabilization for a Rockwood Type V AC joint injury. Six months postoperatively, he presents with persistent pain localized to the distal clavicle, particularly with overhead activities. Radiographs show lucency and erosion at the distal clavicle. Based on the case, what is the most likely complication and its appropriate management?
Explanation
Correct Answer: C
The patient's symptoms of persistent pain localized to the distal clavicle with lucency and erosion on radiographs six months postoperatively are classic signs of distal clavicle osteolysis. The 'Complications and Management' table in the case describes 'Distal Clavicle Osteolysis' with an etiology of 'Micro-motion, rigid fixation (hook plates), or unrecognized intra-articular damage.' The recommended salvage strategy is 'Arthroscopic or open distal clavicle excision (Mumford procedure) once the coracoclavicular ligaments have fully healed.' The other options describe different complications with distinct presentations and management strategies.
Question 8
A patient is 3 weeks post-operative following an acute AC joint reconstruction. During their physical therapy session, the therapist instructs them on pendulum exercises. Which of the following activities, if performed by the patient at this stage, would be considered a violation of the typical Phase One rehabilitation protocol described in the case?
Explanation
Correct Answer: C
The 'Post Operative Rehabilitation Protocols' section outlines Phase One (Immobilization) from postoperative day zero to four weeks. During this phase, 'The patient is placed in a shoulder sling with an abduction pillow. The sling must support the weight of the arm to prevent inferior traction on the scapula... Active range of motion of the elbow, wrist, and hand is encouraged immediately... Pendulum exercises may be initiated at two weeks, but active shoulder elevation and reaching across the body are strictly prohibited.' Therefore, initiating active shoulder elevation at 3 weeks would be a violation of the protocol.
Question 9
A surgeon is performing an open coracoclavicular ligament reconstruction. During the exposure of the coracoid process, the clavipectoral fascia is incised lateral to the conjoint tendon. Referring to the provided image and the neurovascular anatomy described in the case, which critical neurovascular structure is at risk if dissection extends too far distally and medially from the coracoid tip?

Explanation
Correct Answer: C
Under the 'Neurovascular Anatomy' section, the case states: 'When performing coracoid dissection, surgeons must remain acutely aware of the musculocutaneous nerve, which enters the conjoint tendon approximately 3 to 5 centimeters distal to the coracoid tip, and the underlying brachial plexus, which sits posteromedial to the coracoid base.' Dissection extending too far distally and medially from the coracoid tip would directly endanger the musculocutaneous nerve as it enters the conjoint tendon. The axillary and suprascapular nerves are typically at risk more posteriorly or superiorly, respectively. The lateral pectoral nerve innervates the pectoralis major and is generally more superior and medial. The thoracoacromial artery is a vascular structure, not a nerve, and while important for hemostasis, the question specifically asks for a neurovascular structure at risk in this specific location, with the musculocutaneous nerve being the most prominent neural structure in that immediate vicinity.
Question 10
The ISAKOS Upper Extremity Committee has provided consensus guidelines for the management of Rockwood Type III acromioclavicular joint injuries. According to these guidelines, which of the following patient presentations would most likely benefit from early surgical stabilization?
Explanation
Correct Answer: C
The 'Summary of Key Literature and Guidelines' section discusses the ISAKOS consensus guidelines for Type III injuries: 'The committee subclassified Type III injuries into Type IIIA (vertically unstable but horizontally stable) and Type IIIB (vertically and horizontally unstable). The current consensus suggests that Type IIIA injuries are best managed non-operatively, while Type IIIB injuries, characterized by dynamic overriding of the clavicle on the acromion during cross-body adduction, often experience poor functional outcomes with conservative care and may benefit from early surgical stabilization.' Option C describes a manual laborer (high-demand patient) with a Type IIIB injury (dynamic overriding), which is the specific indication for early surgical stabilization according to ISAKOS. Options A, B, D, and E either describe Type IIIA injuries, patients with contraindications to surgery, or patients with less demanding lifestyles where non-operative management is preferred.
Question 11
A 32-year-old male presents to the emergency department after a high-energy fall onto an outstretched hand, complaining of severe right shoulder pain and inability to move his arm. Radiographs confirm a displaced greater tuberosity fracture. Which of the following associated injuries is most commonly observed with greater tuberosity fractures?
Explanation
Correct Answer: C
The case explicitly states that greater tuberosity fractures are frequently associated with other shoulder injuries, most notably anterior glenohumeral dislocations, occurring in 20-30% of cases. This makes anterior glenohumeral dislocation the most commonly observed associated injury among the options provided. While rotator cuff tears can be concomitant or cause the avulsion, and brachial plexus injuries can occur, they are not as frequently noted as anterior dislocations in the context of GT fractures. Humeral shaft fractures and posterior glenohumeral dislocations are less common associations.
Question 12
A 68-year-old osteopenic female sustains a fall onto her shoulder, resulting in a displaced greater tuberosity fracture with significant superior retraction. During surgical planning, the surgeon considers the primary muscle responsible for this displacement. Which rotator cuff tendon primarily inserts on the superior facet of the greater tuberosity and is the main driver of superior displacement?
Explanation
Correct Answer: D
The case details the surgical anatomy of the greater tuberosity, stating that the supraspinatus inserts on the superior facet. Its primary action is abduction of the humerus, and its unopposed pull is the main driver of superior displacement in greater tuberosity fractures. The infraspinatus inserts on the middle facet and the teres minor on the inferior facet, both contributing to external rotation. The subscapularis inserts on the lesser tuberosity, and the deltoid is not a rotator cuff muscle, inserting more distally on the humerus.
Question 13
A 48-year-old construction worker undergoes open reduction and internal fixation for a 7mm superiorly displaced greater tuberosity fracture. If this fracture had been missed and allowed to heal in its displaced position, what would be the most likely long-term functional consequence?
Explanation
Correct Answer: C
The case explains that a superiorly displaced greater tuberosity fragment can lead to mechanical impingement against the acromion during abduction, causing pain and limiting range of motion. This is a direct biomechanical consequence of the superior migration. While avascular necrosis (AVN) is a concern with humeral head fractures, it is rare for isolated greater tuberosity fractures. Chronic anterior glenohumeral instability is more associated with anterior displacement or recurrent dislocations. Isolated external rotation weakness would be more likely with significant posterior displacement. Accelerated glenohumeral osteoarthritis can be a long-term sequela of chronic impingement and altered kinematics, but mechanical impingement and reduced abduction are the more immediate and direct functional consequences of a superiorly malunited fragment.
Question 14
A 55-year-old active tennis player presents with a greater tuberosity fracture after a fall. CT imaging reveals a single, non-comminuted fragment with 4mm of superior displacement and 2mm of posterior displacement. The patient has no associated glenohumeral dislocation. Based on current guidelines and the patient's activity level, what is the most appropriate management?
Explanation
Correct Answer: C
The case states that operative management is indicated for displaced fractures, specifically mentioning superior displacement greater than 3-5 mm. With 4mm of superior displacement, this fracture falls within the surgical indication range. Furthermore, the patient is described as an 'active tennis player' with 'high functional demands,' for whom optimal restoration of shoulder mechanics is paramount. Non-operative management is typically reserved for minimally displaced fractures (<3-5mm). Arthroscopic debridement and capsular release are treatments for adhesive capsulitis, not acute fractures. Hemiarthroplasty is an extreme measure for severe, complex fractures or arthrosis, not an isolated GT fracture. Delayed ORIF is generally not recommended as early anatomical reduction is crucial for optimal outcomes.
Question 15
A 40-year-old male sustains a fall and presents with a suspected displaced greater tuberosity fracture. Initial radiographs (AP, scapular Y, axillary views) show a possible fracture, but the exact degree of displacement and comminution is unclear. Which of the following imaging modalities is considered essential for detailed pre-operative planning of a displaced greater tuberosity fracture?
Explanation
Correct Answer: C
The case explicitly states that a Computed Tomography (CT) scan with 3D reconstructions is 'essential' for displaced greater tuberosity fractures. It provides detailed information regarding fragment size, shape, number, precise degree and direction of displacement, articular involvement, and comminution, which is critical for surgical planning. While MRI is indicated if there is suspicion of concomitant rotator cuff pathology or labral tears, it is not considered the primary essential imaging for characterizing the bony fracture itself. Ultrasound, arthrography, and dynamic fluoroscopy have more limited roles in initial detailed fracture assessment.
Question 16
A surgeon is performing an anterolateral (deltoid-splitting) approach for a greater tuberosity fracture. To minimize the risk of iatrogenic injury to the axillary nerve, the surgeon must limit the deltoid split to a specific distance distal to the acromial border. What is the approximate safe limit for the deltoid split?
Explanation
Correct Answer: C
The case specifically highlights the importance of limiting the deltoid split to approximately 5 cm distal to the acromial border when using the anterolateral approach. This is because the axillary nerve typically courses horizontally around the humerus at this level, and extending the split beyond this limit significantly increases the risk of iatrogenic nerve injury, which could lead to deltoid weakness or paralysis.
Question 17
A 42-year-old patient undergoes ORIF for a greater tuberosity fracture. Intraoperatively, the surgeon uses the technique shown in the image below to achieve stable fixation of a large, single fragment.
Which of the following principles is best demonstrated by the fixation method depicted, and what is its primary advantage for this type of fracture?

Explanation
Correct Answer: B
The image depicts screws crossing the fracture line, which is characteristic of lag screw fixation. The case describes lag screw fixation as a technique where screws are placed across the fracture site in a lag fashion to achieve interfragmentary compression. This provides rigid fixation and excellent compression, which is advantageous for larger, single, well-corticated fragments. Tension band wiring typically involves wires, not screws. Neutralization plating uses a plate to protect screws from bending forces, which is not the primary principle shown. Suture anchor repair uses anchors and sutures, not screws, to reattach the rotator cuff footprint. Intramedullary nailing involves a rod placed within the medullary canal, which is not shown.
Question 18
A 60-year-old female undergoes ORIF for a displaced greater tuberosity fracture. Six weeks post-operatively, despite adhering to a protected rehabilitation protocol, she develops progressive, diffuse shoulder pain and a global loss of both active and passive range of motion. Radiographs show satisfactory fracture healing and no hardware issues. What is the most likely diagnosis and the primary management strategy?
Explanation
Correct Answer: C
The patient's symptoms of progressive, diffuse shoulder pain and a global loss of both active and passive range of motion, despite adherence to rehabilitation and with satisfactory fracture healing, are classic for adhesive capsulitis (frozen shoulder). The case identifies this as a common complication after shoulder trauma and surgery, with aggressive physical therapy being the cornerstone of its management. Non-union would typically present with persistent pain and possibly instability, but not necessarily global loss of passive range of motion if the fracture is healing. A rotator cuff re-tear would cause weakness and pain, but not necessarily global loss of passive motion. Axillary nerve injury would primarily cause deltoid weakness and sensory deficits. Avascular necrosis is rare for isolated GT fractures and presents with progressive pain and stiffness, but the global loss of passive motion points more strongly to adhesive capsulitis.
Question 19
A 35-year-old patient is 3 weeks post-operative following open reduction and internal fixation of a greater tuberosity fracture. The surgeon emphasizes strict adherence to the protection phase of rehabilitation. Which of the following activities is strictly restricted during this initial phase (0-6 weeks)?
Explanation
Correct Answer: D
The case outlines the 'Protection Phase (0-6 Weeks Post-Op)' of rehabilitation, explicitly stating the restriction: 'NO active shoulder range of motion (AROM).' The goal during this phase is to protect the healing fracture. Pendulum exercises, passive range of motion for adjacent joints (elbow, wrist, hand), gentle isometric scapular retractions, and limited gravity-assisted PROM are generally permitted to prevent stiffness and maintain mobility without stressing the repair. Active shoulder motion would place undue stress on the healing fracture and rotator cuff repair.
Question 20
During an orthopedic grand rounds, a debate arises regarding the optimal fixation method for a displaced greater tuberosity fracture in a 50-year-old patient with good bone quality. One surgeon advocates for suture anchors, another for lag screws, and a third for a small plate. Based on the provided case material, which statement best reflects the current consensus and controversies regarding fixation methods for greater tuberosity fractures?
Explanation
Correct Answer: D
The 'Summary of Key Literature / Guidelines' section explicitly states, 'There is no single universally accepted 'best' fixation method.' It further elaborates that the decision often comes down to surgeon preference, fragment characteristics, and bone quality. Suture fixation is often preferred for smaller avulsion fragments or osteoporotic bone, but also for broad reattachment of the rotator cuff footprint. Screw fixation is suitable for larger, sturdy fragments. Plate fixation is less common for isolated GT fractures. Therefore, options A, B, and C represent oversimplifications or incorrect statements regarding the indications or contraindications of specific methods. Option E is also incorrect, as the role of arthroscopy is still an evolving concept, and it has not been definitively proven superior in all cases, nor is it suitable for all fracture types.
Question 21
A 35-year-old male presents to the emergency department after a fall onto an outstretched arm, sustaining the injury shown in the radiograph below. He reports numbness in the dorsal first web space and inability to extend his wrist and fingers.
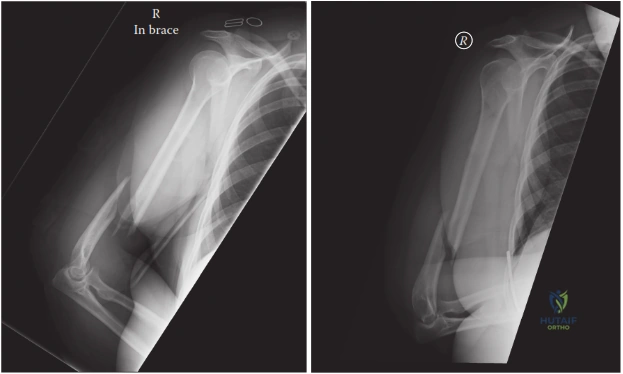
Explanation
Correct Answer: C
The radiograph depicts a spiral or oblique fracture of the distal one-third of the humerus, consistent with a Holstein–Lewis fracture. The clinical presentation of numbness in the dorsal first web space and inability to extend the wrist and fingers is characteristic of a radial nerve palsy. The case description explicitly states that the Holstein–Lewis fracture is a specific spiral or oblique fracture of the distal one-third of the humerus, characterized by its high association with radial nerve injury (10-20% incidence). The sharp, displaced proximal fracture fragment uniquely predisposes the radial nerve to entrapment or direct laceration.
Option A is incorrect because Holstein–Lewis fractures are typically spiral or oblique, not transverse, and have a significantly high risk of radial nerve injury. Option B is incorrect as Holstein–Lewis fractures are associated with radial nerve injury, not typically median nerve injury, and are not primarily supracondylar in the classic sense of pediatric supracondylar fractures. Option D is incorrect as Holstein–Lewis fractures typically spare the articular surface. Option E is incorrect as the fracture is in the distal humerus, not the proximal humerus, and is not managed with shoulder arthroplasty.
Question 22
During surgical exploration for a Holstein–Lewis fracture with complete radial nerve palsy, the surgeon identifies the radial nerve as depicted in the image below, carefully dissecting it from surrounding tissues.
Explanation
Correct Answer: C
The case study emphasizes that in Holstein–Lewis fractures, the radial nerve is particularly vulnerable at the point where it pierces the lateral intermuscular septum and more distally, where it runs intimately with the periosteum of the distal humerus. This transition point, typically 10-14 cm proximal to the lateral epicondyle, is where the nerve moves from the posterior compartment to the anterior compartment of the arm, making it susceptible to entrapment or injury by the sharp, often medially displaced, proximal fracture fragment.
Option A describes a more proximal location, not specific to Holstein–Lewis vulnerability. Option B describes the vulnerability in mid-shaft fractures, not the unique vulnerability in Holstein–Lewis fractures which are more distal. Option D describes the nerve's course after it has already passed the critical zone of injury for Holstein–Lewis fractures. Option E describes the ulnar nerve's general vicinity, not the radial nerve.
Question 23
A 48-year-old male sustains a Holstein–Lewis fracture. On initial presentation, he has an incomplete radial nerve palsy (weak wrist extension, intact sensation). After a closed reduction attempt, his radial nerve palsy progresses to a complete motor and sensory deficit.
What is the most appropriate next step in the management of this patient's radial nerve injury?
Explanation
Correct Answer: C
The case study explicitly states under 'Indications for Operative Management' that if a radial nerve palsy 'worsens or develops following closed reduction attempts,' immediate surgical exploration is mandatory. This scenario suggests iatrogenic injury or worsening entrapment of the nerve by fracture fragments. While many neuropraxias recover spontaneously, a worsening palsy after manipulation is a critical indication for immediate surgical intervention to decompress or repair the nerve and stabilize the fracture.
Option A is incorrect because worsening palsy post-reduction is an absolute indication for exploration, not observation. Option B (NCS/EMG) is not an emergent study and would delay critical intervention. Option D (functional brace and early ROM) is part of post-operative care, not the immediate management for a worsening nerve palsy. Option E (gabapentinoids for CRPS) is for a different complication and not the immediate concern.
Question 24
A 55-year-old patient with a displaced Holstein–Lewis fracture and a complete radial nerve palsy at presentation is scheduled for ORIF.
Which surgical approach is generally preferred for this fracture pattern, and what is the most critical step regarding radial nerve management during the procedure?
Explanation
Correct Answer: B
The case study states that the 'Posterior Approach (Triceps-Sparing or Triceps-Splitting)' is often the preferred approach for Holstein–Lewis fractures, particularly when radial nerve exploration is anticipated or required, as it provides excellent direct visualization of the fracture site and the radial nerve as it exits the spiral groove. The most crucial step is 'Radial Nerve Identification,' which involves identifying the nerve proximally in the spiral groove and tracking it distally to the fracture site, carefully inspecting it for injury or entrapment.
Option A (Anterolateral approach) can be used but is less preferred when direct radial nerve exploration is the primary indication. The musculocutaneous nerve is not the primary concern in Holstein–Lewis fractures. Option C (Medial approach) is not the standard for Holstein–Lewis fractures, and while ulnar nerve protection is important, it's not the primary nerve at risk in this specific fracture. Option D (Deltopectoral approach) is for proximal humerus fractures. Option E (Lateral approach) is not the primary approach, and the posterior interosseous nerve is a distal branch of the radial nerve, not the main site of vulnerability in this fracture pattern.
Question 25
During ORIF of a Holstein–Lewis fracture, the surgeon encounters an oblique fracture pattern in the distal one-third of the humerus.
Which of the following fixation principles is most strongly supported by current literature for achieving optimal biomechanical stability in this type of fracture?
Explanation
Correct Answer: C
The 'Summary of Key Literature / Guidelines' section explicitly states that 'Contemporary literature strongly supports the use of dual plating (e.g., orthogonal or parallel plate constructs) for displaced distal humeral shaft fractures, including Holstein–Lewis patterns. This provides superior biomechanical stability compared to single plating, especially against torsional and bending forces, which are critical for the oblique/spiral nature of these fractures.' It also recommends 'The use of lag screws across the oblique or spiral fracture line, prior to plate application, is highly recommended to achieve interfragmentary compression and increase construct stiffness.'
Option A (Single plate fixation) is less stable than dual plating for these fractures. Option B (Intramedullary nailing) is generally not preferred for distal humeral shaft fractures due to concerns about elbow impingement and less stable fixation in the metaphyseal region compared to plating. Option D (External fixation) is typically reserved for severe open fractures or temporary stabilization in polytrauma, not definitive fixation of closed Holstein–Lewis fractures. Option E (Tension band wiring) is more commonly used for avulsion fractures or olecranon fractures, not for diaphyseal/metaphyseal humerus fractures.
Question 26
A patient undergoes ORIF for a Holstein–Lewis fracture with an intact radial nerve. Post-operatively, the surgeon emphasizes early, protected range of motion.
In the immediate post-operative phase (0-2 weeks), which of the following rehabilitation strategies is most appropriate for this patient?
Explanation
Correct Answer: C
The 'Post-Operative Rehabilitation Protocols' section for Phase 1 (0-2 Weeks) outlines the following: 'Gentle active-assisted ROM (AAROM) and passive ROM (PROM) of the elbow, typically 30-90 degrees of flexion/extension, initiated as soon as pain allows and dictated by surgical stability.' It also specifies 'Active and passive range of motion (ROM) exercises for the wrist, hand, and fingers' and 'Pendulum exercises, active-assisted shoulder flexion, extension, abduction, and rotation (within pain limits) to prevent shoulder stiffness.' It explicitly states 'No active biceps/triceps contractions against resistance' and 'Non-weight-bearing (NWB) for the operative extremity.'
Option A and E are incorrect as active resistance and advanced strengthening are contraindicated in the immediate post-operative phase to protect the fixation. Option B (complete immobilization for 6 weeks) is incorrect as early, protected motion is crucial to prevent elbow stiffness. Option D (unrestricted weight-bearing) is incorrect as the limb must be non-weight-bearing in this phase.
Question 27
A 60-year-old patient, 9 months after ORIF of a Holstein–Lewis fracture, presents with persistent pain, instability, and radiographic evidence of non-union. The initial fixation involved a single plate.
What is the most appropriate salvage strategy for this patient's non-union?
Explanation
Correct Answer: C
The 'Complications & Management' section, under 'Non-Union,' states that management involves 'Revision ORIF with robust fixation (dual plating), debridement of fibrous tissue, interposition bone grafting (autograft or allograft), potentially electrical stimulation.' Given the persistent pain, instability, and radiographic non-union at 9 months, a surgical revision is indicated. The initial single plate fixation may have been inadequate, making dual plating a more robust option for revision.
Option A (observation and NSAIDs) is inappropriate for an established non-union. Option B (systemic antibiotics) is incorrect without evidence of infection (e.g., elevated inflammatory markers, wound drainage, positive cultures). Option D (external fixation) is generally not the definitive treatment for a non-union of the humerus unless there are severe soft tissue issues or active infection. Option E (tendon transfers) is a salvage procedure for chronic nerve palsy, not for fracture non-union.
Question 28
A 28-year-old male presents with a Holstein–Lewis fracture after a wrestling match where his arm was twisted.
The typical mechanism of injury for a Holstein–Lewis fracture involves which of the following forces, and how does this relate to the fracture pattern's inherent instability?
Explanation
Correct Answer: B
The 'Introduction & Epidemiology' section states that the 'typical mechanism of injury involves direct trauma or a low-energy torsional force to the arm.' The 'Surgical Anatomy & Biomechanics' section further clarifies that 'The biomechanics of Holstein–Lewis fractures often involve a combination of bending and torsional forces. The oblique or spiral nature of the fracture makes it inherently unstable to rotational loads, and the smooth, often comminuted, fracture surfaces can make stable reduction challenging.'
Option A describes a different mechanism and fracture pattern. Option C describes an olecranon fracture, not a Holstein–Lewis. Option D describes a supracondylar fracture, which is distinct from a Holstein–Lewis. Option E describes a proximal humeral fracture, not a distal one-third diaphyseal fracture.
Question 29
A 40-year-old patient presents with a Holstein–Lewis fracture. On initial examination, he has no signs of radial nerve palsy. After successful closed reduction and application of a functional brace, he develops a complete radial nerve palsy 24 hours later.
This scenario represents a secondary radial nerve palsy. What is the critical implication for management compared to a primary palsy present at initial presentation?
Explanation
Correct Answer: B
The 'Summary of Key Literature / Guidelines' section, under 'Immediate vs. Delayed Exploration,' clearly states: 'If a radial nerve palsy develops or worsens after attempts at closed reduction, or post-operatively, immediate surgical exploration is mandatory. This suggests iatrogenic injury or worsening entrapment.' This is a critical distinction from primary palsy (palsy at presentation), where immediate exploration is often recommended but sometimes observation is considered for incomplete palsies, though less common for classic Holstein-Lewis patterns due to high entrapment risk.
Option A is incorrect; secondary palsies are a red flag for iatrogenic injury and require immediate exploration. Option C reverses the urgency; secondary palsies are often more concerning due to their iatrogenic nature. Option D (immediate tendon transfers) is a salvage procedure for chronic, non-recovering palsy, not acute management. Option E is incorrect as the timing of palsy onset significantly impacts the management strategy.
Question 30
A 30-year-old patient with a Holstein–Lewis fracture sustained a complete radial nerve transection that was not amenable to primary repair during initial surgery. Despite secondary nerve grafting 6 months later, there is no evidence of recovery after 18 months.
Given the persistent complete radial nerve palsy after 18 months, what is the most appropriate long-term salvage strategy to restore functional wrist and finger extension?
Explanation
Correct Answer: C
The 'Complications & Management' section, under 'Radial Nerve Palsy (Persistent/New),' states: 'If palsy persists >3-6 months post-injury: Consider secondary surgical exploration (neurolysis, repair, or grafting). Chronic palsy (>1 year): Tendon transfers (e.g., pronator teres to ECRB, FCR to EDC, palmaris longus to EPL) for functional restoration.' After 18 months with no recovery following nerve grafting, the likelihood of spontaneous or further surgical nerve recovery is very low, making tendon transfers the definitive functional salvage procedure.
Option A (repeat nerve grafting) is generally not indicated after 18 months of no recovery following a previous graft, as the window for nerve regeneration is typically considered closed or severely limited. Option B (chronic pain management) addresses symptoms but not the functional deficit. Option D (permanent immobilization) would result in a non-functional limb. Option E (electrical stimulation) is an adjunctive therapy, not a primary salvage strategy for a complete, chronic palsy.
Question 31
A 45-year-old male sustains a closed, midshaft humerus fracture and is managed non-operatively with a Sarmiento functional brace. For this treatment modality to be deemed successful and to avoid malunion, which of the following represents the widely accepted maximum limits of acceptable alignment?
Explanation
Question 32
During open reduction and internal fixation of a chronic acromioclavicular (AC) joint injury, the surgeon must address both vertical and horizontal instability. Which of the following native structures acts as the primary restraint to anteroposterior (horizontal) translation of the distal clavicle?
Explanation
Question 33
When evaluating the literature regarding the operative management of humeral shaft fractures, randomized controlled trials comparing open reduction internal fixation (ORIF) with plates versus intramedullary (IM) nailing demonstrate which of the following significant differences in complications?
Explanation
Question 34
Anatomical reconstruction of the coracoclavicular (CC) ligaments requires precise knowledge of their insertions. Which of the following accurately describes the anatomy and primary biomechanical role of the conoid ligament?
Explanation
Question 35
A 25-year-old elite collegiate volleyball player sustains an isolated, displaced greater tuberosity fracture of the dominant shoulder. Radiographs show superior displacement of the fragment. What is the generally accepted threshold for surgical fixation in this specific patient demographic?
Explanation
Question 36
A 35-year-old male presents with a distal-third spiral fracture of the humerus (Holstein-Lewis fracture) following an arm-wrestling incident. He has an absent brachioradialis reflex and inability to extend his wrist. At what specific anatomic location is the radial nerve most susceptible to tethering or entrapment in this fracture pattern?
Explanation
Question 37
A 42-year-old male falls directly onto his shoulder. Clinical examination reveals a prominent acromion, but the distal clavicle is non-palpable and appears displaced posteriorly. Radiographs confirm posterior displacement of the clavicle through the trapezius muscle. What is the correct Rockwood classification for this injury?
Explanation
Question 38
A 9-year-old boy falls onto his shoulder from a bicycle and sustains what appears radiographically to be a severe acromioclavicular (AC) joint dislocation. However, based on the patient's age, what is the most likely true pathology of this "pseudodislocation"?
Explanation
Question 39
When managing a humeral shaft fracture non-operatively with a functional brace, which of the following fracture characteristics is most strongly associated with an increased risk of nonunion?
Explanation
Question 40
A surgeon is performing an open reduction and internal fixation of an isolated, displaced greater tuberosity fracture using a direct lateral (deltoid-splitting) approach. To avoid iatrogenic nerve injury, the distal extent of the deltoid split must not exceed what distance from the lateral edge of the acromion?
Explanation
Question 41
A 25-year-old male sustains a closed distal third spiral fracture of the humeral shaft (Holstein-Lewis) after an arm-wrestling match. On initial examination, he has weak wrist extension and numbness in the first dorsal web space. Closed reduction is performed, and post-reduction examination shows no change in his neurologic status. What is the most appropriate management of the radial nerve injury?
Explanation
Question 42
A 45-year-old avid tennis player sustains an isolated greater tuberosity fracture of the proximal humerus. Radiographs and CT imaging show superior displacement of the tuberosity fragment. At what threshold of superior displacement is open reduction and internal fixation generally indicated to prevent subacromial impingement in this active patient?
Explanation
Question 43
In evaluating the stability of the acromioclavicular (AC) joint, a surgeon considers the primary anatomical restraints. Which of the following accurately describes the primary ligamentous restraint to superior translation of the distal clavicle?
Explanation
Question 44
A 35-year-old male presents with a closed midshaft humerus fracture and is treated with a Sarmiento functional brace. Which of the following coronal and sagittal plane angular deformities are considered the maximum acceptable limits for non-operative management of a humeral shaft fracture?
Explanation
Question 45
A 55-year-old female dislocates her shoulder anteriorly after a fall. Post-reduction radiographs demonstrate an associated, minimally displaced greater tuberosity fracture. What is the relationship between this fracture and the risk of a concomitant rotator cuff tear?
Explanation
Question 46
A surgeon is planning a posterior approach to the humerus for internal fixation of a distal third shaft fracture. To safely identify and protect the radial nerve, the surgeon must understand its anatomical course. At what distance proximal to the radiocapitellar joint does the radial nerve typically pass from the posterior to the anterior compartment through the lateral intermuscular septum?
Explanation
Question 47
A meta-analysis comparing compression plating versus intramedullary nailing for the treatment of humeral shaft fractures demonstrates differences in complication profiles. Which of the following complications is significantly more common with intramedullary nailing compared to plating?
Explanation
Question 48
A 28-year-old cyclist sustains an injury to his shoulder. Radiographs reveal a distal clavicle fracture with severe displacement. On the axillary lateral view, the distal clavicle is displaced posteriorly into the trapezius muscle fibers. The AC joint itself appears intact. Which classification best describes the equivalent AC joint injury pattern, and what is the recommended treatment?
Explanation
Question 49
When performing surgical fixation of a comminuted, osteoporotic greater tuberosity fracture, biomechanical studies favor which of the following constructs to provide the strongest fixation and minimize construct failure?
Explanation
Question 50
A 40-year-old male sustains a proximal third transverse humeral shaft fracture. He is placed in a functional fracture brace. Which of the following fracture characteristics places him at the highest risk for developing a nonunion?
Explanation
Question 51
In the classical Weaver-Dunn procedure for chronic acromioclavicular joint instability, the coracoacromial (CA) ligament is transferred to the distal clavicle. What is a primary limitation of using the isolated CA ligament for this reconstruction?
Explanation
Question 52
A 32-year-old male presents with a severe midshaft humeral fracture between the insertions of the pectoralis major and the deltoid. Based on the muscular attachments, what are the predictable deforming forces on the proximal and distal fracture fragments?
Explanation
Question 53
During an open distal clavicle excision (Mumford procedure) for AC joint osteoarthritis, the surgeon meticulously resects the distal clavicle. Resecting more than 10-12 mm of the distal clavicle increases the risk of which iatrogenic complication?
Explanation
Question 54
A 22-year-old male is involved in a motorcycle collision and sustains a highly comminuted midshaft humerus fracture and ipsilateral displaced fractures of the radius and ulna shafts. He has a normal neurovascular exam. What is the most appropriate management for the humerus fracture?
Explanation
Question 55
The coracoclavicular (CC) ligament complex consists of the conoid and trapezoid ligaments. Which of the following statements accurately describes their respective anatomical footprints and functions?
Explanation
Question 56
A 60-year-old male with a history of alcohol abuse presents to the emergency department after a seizure. He has a locked-in internally rotated right arm and severe shoulder pain. Radiographs reveal a posterior shoulder dislocation. Which proximal humerus fracture is most commonly associated with this specific type of dislocation?
Explanation
Question 57
A 19-year-old male sustains an open distal third humeral shaft fracture after a rollover motor vehicle accident. The arm is pale, pulseless, and cool to the touch. Immediate closed reduction fails to restore the pulse. In the operating room, what is the correct sequence of management?
Explanation
Question 58
A patient is evaluated for an AC joint injury after a fall. Examination shows severe inferior displacement of the distal clavicle, resting underneath the coracoid process, posterior to the conjoint tendon. What is the Rockwood classification for this injury?
Explanation
Question 59
During open reduction and internal fixation of a proximal humerus fracture extending into the greater tuberosity, you use heavy non-absorbable sutures to secure the tuberosity fragment. Which muscle's tendon insertion are you primarily capturing to counteract the superior deforming force on the greater tuberosity?
Explanation
Question 60
A 50-year-old female presents with a nonunion of a midshaft humerus fracture 8 months after initial non-operative management in a functional brace. She is healthy and a non-smoker. Radiographs show a hypertrophic nonunion with adequate bone stock. What is the most appropriate surgical management?
Explanation
Question 61
The coracoclavicular (CC) ligaments are the primary stabilizers of the AC joint against superior-inferior translation. Which of the following accurately describes the anatomy and biomechanical function of the CC ligament complex?
Explanation
Question 62
A 25-year-old overhead athlete sustains a closed, isolated greater tuberosity fracture after a fall. To optimize return to play and avoid mechanical subacromial impingement, surgical fixation is highly recommended if superior displacement exceeds which of the following thresholds?
Explanation
Question 63
Which of the following clinical scenarios represents an absolute indication for early surgical exploration of the radial nerve in the setting of a newly sustained humeral shaft fracture?
Explanation
Question 64
A 34-year-old male sustains a closed spiral fracture of the distal third of the humeral shaft. On initial presentation in the emergency department, his neurovascular exam is completely intact. A closed reduction is performed, and a coaptation splint is applied. Immediately post-reduction, the patient is unable to actively extend his wrist or fingers, and he has decreased sensation over the dorsal first web space. What is the most appropriate next step in management?
Explanation
Question 65
A 28-year-old female sustains a midshaft humeral fracture and is being treated non-operatively with a functional brace (Sarmiento). To achieve an acceptable functional and cosmetic outcome without requiring surgical intervention, the maximum acceptable limits of radiographic deformity must not be exceeded. Which of the following represents the maximum acceptable deformity for non-operative management of a humeral shaft fracture?
Explanation
Question 66
A 45-year-old skier sustains an anterior shoulder dislocation with an associated isolated greater tuberosity fracture.
The dislocation is successfully reduced in the emergency department. Post-reduction radiographs demonstrate the greater tuberosity fragment remains displaced 7 mm superiorly. What is the most appropriate definitive management?
Explanation
Question 67
An orthopedic surgeon is performing an anatomic coracoclavicular (CC) ligament reconstruction for a chronic Type V acromioclavicular joint separation. To accurately reproduce the native anatomy and optimize biomechanical stability, where should the surgeon place the clavicular drill tunnel for the conoid ligament?
Explanation
Question 68
A 25-year-old male sustains a polytrauma including a diaphyseal humerus fracture that requires surgical stabilization. Comparing intramedullary nailing to compression plating for humeral shaft fractures, intramedullary nailing is most consistently associated with which of the following postoperative outcomes?
Explanation
Question 69
A 50-year-old female presents with a non-displaced greater tuberosity fracture after a ground-level fall. She is treated non-operatively and immobilized in a sling for 4 weeks. At her 3-month follow-up, radiographs confirm complete fracture union, but she complains of significant, globally restricted active and passive shoulder range of motion. What is the most likely diagnosis?
Explanation
Question 70
A 30-year-old cyclist falls directly onto the point of his shoulder. Clinical examination reveals an irreducible, posteriorly displaced clavicle that is firmly palpable within the trapezius muscle belly. Radiographs, including an axillary lateral view, confirm the distal clavicle is displaced posteriorly relative to the acromion. Which Rockwood classification type does this injury represent?
Explanation
Question 71
During the posterior operative approach to the humerus for internal fixation of a midshaft fracture, the radial nerve is identified to protect it from iatrogenic injury. At what approximate location does the radial nerve pierce the lateral intermuscular septum to transition from the posterior to the anterior compartment of the arm?
Explanation
Question 72
A 30-year-old man sustains a closed midshaft humeral fracture with an associated primary radial nerve palsy on the day of injury. He is treated non-operatively with a functional brace. At 3.5 months post-injury, he shows absolutely no signs of clinical or electromyographic (EMG) recovery of the radial nerve. What is the most appropriate next step in management?
Explanation
Question 73
A 65-year-old female presents with severe arm pain and mobility at the fracture site 8 months after sustaining a midshaft humerus fracture initially treated with a functional brace. Radiographs demonstrate a persistent fracture line with sclerotic, rounded bone ends and an absence of bridging callus. Laboratory inflammatory markers are normal. What is the gold standard surgical intervention for this specific complication?
Explanation
None
